
Abstract
Background
It is believed that greater adiposity is associated with reduced risk of breast cancer in premenopausal but increased risk in postmenopausal women. However, few studies have evaluated these relationships among Black women or examined anthropometric measures other than near-diagnosis body mass index (BMI).
Purpose
This study investigated associations between measures of body size across the life course and breast cancer risk among Black and White women living in the US South.
Methods
We used data from the Carolina Breast Cancer Study, a population-based case–control study of invasive breast cancer in North Carolina women aged 20–74 years. We assessed nine body size variables, including age 10 relative weight; age 18 BMI; adult weight gain; “reference” BMI 1 year before interview; and post-diagnosis measured BMI and abdominal obesity measures.
Results
Among premenopausal Whites, heavier childhood relative weight was associated with decreased cancer risk [odds ratio (OR) 0.48 95 % confidence interval 0.33–0.70]. Among premenopausal Blacks, greater adult waist circumference and waist-to-hip ratio (WHR) were associated with increased risk [waist OR 1.40 (1.00–1.97) and high tertile WHR OR 2.03 (1.29–3.19)], with associations for WHR in a similar direction in Whites. Among postmenopausal women, recalled body size was not associated with risk, except for increased risk associated with adult weight gain among White non-hormone therapy users. ER/PR status and hormone therapy use also modified other associations.
Discussion
In this population, greater adult BMI was not associated with increased breast cancer risk, but some measures of early-life body size and abdominal obesity were associated with risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Black women have higher breast cancer mortality than the rest of the population [1]. The mortality disparity could be partially attributable to Black women’s higher rates of cancer incidence before menopause [2, 3]. One factor that is thought to influence risk of breast cancer differentially in premenopausal and postmenopausal women is adult body mass index (BMI) and adiposity. This factor may be especially salient in understanding patterns of breast cancer incidence among Black women because, in the USA, Black women have higher obesity prevalence than the rest of the population [4].
It is widely accepted that higher adult BMI and greater adiposity are associated with reduced risk of breast cancer in premenopausal women and increased risk in postmenopausal women [5]. However, the evidence for these relationships is ambiguous. A recent meta-analysis concluded that BMI around the time of diagnosis was not significantly associated with incidence of premenopausal breast cancer and only minimally associated with incidence of postmenopausal breast cancer [6]. Further, many of the studies on this topic were conducted in White populations. The few population-based studies among Black women have produced inconclusive results (reviewed in [7]). Many studies of premenopausal cancer in African American women find no association with obesity status near the time of diagnosis [7]. Among postmenopausal Black women, results have been mixed [7]: Some studies found decreased risk [8, 9], others increased risk [10, 11], and others found suggestive or null relationships [12, 13].
A major challenge in understanding the relationship between body size and breast cancer risk among African Americans is that there are few population-based studies with enough Black women to examine the relationship between body size and cancer, stratified by important modifiers, such as menopausal status, estrogen- and progesterone-receptor status, and use of hormone therapy (HT). Additionally, many studies of body size in Black women have assessed body size shortly before or after diagnosis rather than at specific ages or developmental periods in the life course. Previous studies suggest that early-life body size may be a more important predictor of risk than body size shortly before diagnosis [13–15]. For instance, the Black Women’s Health Study (BWHS), a prospective cohort study, reported that BMI shortly before diagnosis was not associated with breast cancer risk in premenopausal or postmenopausal women [13]. However, high BMI at age 18 was associated with reduced risk of premenopausal and postmenopausal cancers. Likewise, in the Nurses’ Health Study, body size in childhood and adolescence was more strongly associated with cancer risk than other measures, independent of adult BMI [14, 15].
The aim of this study was to investigate the association between diverse measures of body size across the life course with risk of premenopausal and postmenopausal breast cancer in the Carolina Breast Cancer Study (CBCS), one of the largest case–control breast cancer studies of US Black women. This analysis extends previous work from the CBCS’s Phase 1 [8], with life course measures and an additional 5 years of data. White women from the same population are studied for context and comparison.
Methods
Study population
The CBCS is a population-based, case–control study of breast cancer [16]. Women were eligible to be cases if they were identified through the North Carolina Cancer Registry as diagnosed with a first primary breast cancer 1993 and 2000, aged between 20 and 74 years, and living in a 24-county area of central and eastern North Carolina. Using randomized recruitment, Black cases and young cases (aged 20–49 years) were oversampled [17].
The CBCS was conducted in two phases (1993–1996; 1996–2001). Study procedures were similar in the phases, but phase 2 included cases of in situ cancer in addition to invasive cancer. The present analysis was restricted to invasive cancer. Of the 2,501 eligible cases of invasive breast cancer in Black and White women, physicians refused contact for 172 cases (6.9 %), 63 (2.5 %) could not be located, 447 (17.9 %) refused to participate, and 36 (1.4 %) died before being interviewed. Thus, 788 Black cases and 995 White cases were included in the present analysis. The overall response rate among eligible, living, and locatable cases was 70.9 % percent for Blacks and 77.1 % for Whites.
Controls were selected between 1993 and 2001 from the same geographic area as cases, using records from the North Carolina Division of Motor Vehicles to identify controls for cases aged <65 years and from the US Health Care Financing Administration, which oversees Medicare, to identify control women aged 65–74 years. Controls were frequency-matched to cases by race and 5-year age group [17, 18]. Of the 3,198 eligible controls who were contacted, 675 (21.1 %) could not be located, 908 (28.4 %) refused to participate, and 79 (2.5 %) had died before being interviewed. Thus, 718 Black controls and 818 White controls were included in the present analysis. The response rate for eligible, living, and locatable controls was 59.8 % for Blacks and 65.8 % for Whites.
Data collection
Participants were interviewed in person by trained nurses using a pretested, standardized questionnaire. For 94.9 % of cases (94.5 % Black, 95.2 % White), interview occurred within 1 year of the diagnosis date. The interview collected self-reported body size, race, family history of cancer, reproductive and menstrual history, hormone use, alcohol consumption, occupational exposures, and socio-demographic characteristics, among a number of other possible risk factors for breast cancer.
Measurements of height, weight, and waist and hip circumferences were taken at the time of interview using standardized scales and tape measures. Height and weight were measured twice to the nearest 0.5 cm and 0.5 kg, respectively, and the two measurements were averaged. The waist circumference measurement was taken at the natural indentation of the waist, and the hip circumference was taken at the greatest protrusion of the buttocks. Both circumferences were measured two times and averaged. A third measurement was taken if the first two differed by more than 1.0 cm, in which case the two closest values were averaged. All study participants provided written informed consent. The study was approved by the institutional review board of the University of North Carolina at Chapel Hill.
Exposure variables
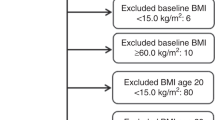
This analysis examined nine variables reflecting different anthropometric characteristics between age 10 and the interview date. Six measures of recalled body size were assessed via questionnaire. Preadolescent body size was based on an interview question about weight relative to other girls of the same age and height when the respondent was in fifth grade, or about 10 years old. “About the same” weight was chosen as a referent because it reflects participants’ perceptions of a typical or normative childhood body size in their childhood communities. Next, young adult body size was assessed by BMI (kg/m2) at age 18 years, based on conversion from recalled weight (lb) at age 18 and recalled usual adult height (feet; inches). Mid-adulthood body size was assessed by BMI at age 35 years, based on recalled weight at age 35 and usual adult height. Change in BMI between ages 18 and 35 years was grouped into tertiles based on the distribution of this variable in the control population of Blacks and Whites combined, to create a common categorization scheme for race-stratified analyses. Missingness is greater for the variables BMI at age 35, and BMI change between ages 18 and 35 years than for other variables because women who were younger than 35 years when they were diagnosed or selected into the study were not eligible to answer this question. Pre-diagnosis, or the “reference,” BMI was calculated using usual adult height and recalled weight 1 year before the interview or, if the subject was pregnant a year before the interview, before that pregnancy. Weight change between ages 18, and the reference date was the difference between reference weight and weight at age 18 years and was measured in kg/m2.
Additional body size variables were measured by trained nurses at a post-diagnosis interview (for cases) or after selection (for controls). Measured BMI at interview was calculated from measured weight (kg) divided by measured height squared (m2). BMI was classified into 4 categories: underweight to normal weight: <25.0; overweight: 25.0–29.9; class 1 obesity: 30.0–34.9; class 2 obesity and above: ≥35 [19]. Measured waist circumference was used to identify abdominal obesity (>88 cm) [20]. Waist-to-hip ratio (WHR), calculated as measured waist circumference divided by hip circumference, was categorized into tertiles based on the distribution of waist circumference in the control population of Blacks and Whites combined.
Statistical analysis and covariates
Unconditional logistic regression was used to calculate odds ratios and 95 % confidence intervals comparing cases to controls. Sampling weights (accounting for the oversampling of Black and young cases) and an offset term were incorporated into each model to account for the study’s sampling approach [17]. Positive or inverse linear trends were assessed based on [1] ordinal coding of categorical variables and [2] medians of categorical variables. Except for age 10 relative weight, whose trend was only assessed across ordinal values of the variable, in-text references to p-for-trend tests refer to two-sided p values (α = 0.05) based on category medians.
All models were stratified by race and menopausal status at the time of diagnosis (for cases) or selection into the study (for controls). Cases and controls were classified as postmenopausal if, at diagnosis or selection, respectively, [1] they were under age 50 and had undergone natural menopause (ceased menstruating in the absence of hysterectomy), bilateral oophorectomy, or irradiation to the ovaries or [2] they were aged 50 or older and had ceased menstruating [16, 21]. If women were still menstruating when diagnosed with cancer or selected for the study, they were classified as premenopausal [16]. A Nurses’ Health Study validation of two methods of classifying menopausal status, one method less precise than ours (assigning age at hysterectomy as menopausal age) and a more precise imputation method, found both methods produced similarly accurate associations between breast cancer incidence and a range of risk factors, including BMI (see Table 4 in [22]).
All models were adjusted for the age (in years) at which women were selected into the study, modeled by a continuous variable and a squared term, which was statistically significant (p ≤ 0.05) in some preliminary analyses. Additionally, multivariable-adjusted models included the following variables, identified as potential confounders, known breast cancer risk factors that may also affect body size, through analysis of a directed acyclic graph (DAG): education level (some high school or less, high school graduate, college graduate), first-degree family history of breast cancer (yes/no), smoking history (current, former, never) alcohol use of at least 12 drinks in one’s lifetime (yes/no), age at menarche (≤11, 12–13, or >13 years), lactation history (had breastfed, never breastfed), and a composite of parity and age at first full-term pregnancy (FFTP) (nulliparous, 1 child and FFTP age ≤25 years, 1 child and FFTP age >25 years, ≥2 children and FFTP age ≤25 years, ≥2 children and FFTP age >25 years). Because some potential confounders, education, parity, age at first full-term birth, and lactation history, may be intermediates on the pathway between childhood and young adult body size and incident cancer [23], we ran models with and without these variables. Results were similar. Therefore, we only present results for the age-adjusted and fully adjusted models.
Our main analyses did not mutually adjust for body size at other ages because body size measures are highly correlated, violating assumptions of statistical independence. Additionally, later measures of body size may be colliders on the causal pathway between earlier body size and cancer incidence; therefore, adjusting for older body size could induce bias [24]. We did, however, run supplemental analyses adjusting early body size for continuous reference BMI and adjusting measures of central adiposity at interview for continuous BMI measured at interview.
Results
Descriptive characteristics
Characteristics of this population have been previously reported [25] (see Supplemental Table 1). Table 1 shows the unweighted distributions of body size across the life course among Black and White cases and controls (Analyses accounting for the oversampling of Black and young cases produced similar results.). For the subjective measure of age 10 weight, Black women were more likely than White women to report being “thinner” than peers, while White women were relatively more likely to report being “about the same.” For all adult measures, body size tended to be greater in Black versus White women and to increase with age. For instance, about 20 % of control Black women reported being overweight (BMI ≥ 25.0 kg/m2) at age 18, but, by age 35, nearly half were overweight. Among White women, only 5 % reported being overweight at age 18, and about 20 % reported being overweight at age 35. At the interview, the majority of Black control women were obese, as indicated by measured BMI or waist circumference. About a quarter of White women were obese.
Premenopausal breast cancer
Among premenopausal Black and White women, most measures of body size were not associated with breast cancer risk (see Table 2). However, several measures showed associations or suggestive trends in one or both race groups: age 10 relative weight, body size at age 35, and measures of abdominal obesity near diagnosis.
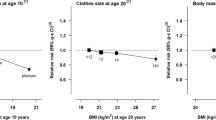
Among premenopausal Black women, being thinner than peers at age 10 was associated with greater risk of cancer [OR 1.44 (1.00, 2.07)] compared to those who reported being “about the same” weight as peers. There was not evidence of a linear trend (p = 0.29). Additionally, greater BMI at age 35 showed a positive trend with increased cancer risk among premenopausal Black women (p = 0.01). Later in life, neither reference BMI nor BMI measured at interview were associated with cancer risk among Black premenopausal women. In contrast, waist circumference and WHR measured near the diagnosis were positively associated with cancer risk (respectively, p-for-trend = 0.05 and 0.02).
Among premenopausal White women, reporting heavier weight at age 10 was strongly associated with decreased cancer risk compared to those who reported “about the same” age 10 weight (OR 0.48 [0.33, 0.70]). There was evidence of an inverse linear relationship between greater age 10 weight and cancer risk. In contrast to Black women, among White premenopausal women, greater BMI at age 35 showed a suggestive association with decreased cancer risk (p = 0.09) as did the highest tertile of BMI change between ages 18 and 35 compared to the lowest tertile (OR 0.70 [0.49, 1.02]). Later in life, greater reference BMI was not linearly associated with cancer risk. However, greater BMI measured at interview showed a suggestive trend with decreased risk (p = 0.10), e.g., OR for BMI ≥35 = 0.67 (0.41, 1.08). Finally, measured waist circumference was not associated with cancer risk, but WHR showed a suggestive trend (p = 0.07), with increased odds ratios for the second and third tertiles versus the first tertile [OR 1.41 (1.02, 1.95) and OR 1.33 (0.91, 1.96), respectively].
Adjusting measures of early-life body size for reference BMI did not materially change results among Black and White premenopausal women (see Table 2). Among Whites, high WHR’s linear trend with increased risk became more pronounced (p < 0.01), and the estimate for high waist circumference increased from 0.87 (0.63, 1.18) to 1.43 (0.88, 2.32).
Postmenopausal breast cancer
In general, among postmenopausal Black and White women, recalled measures of body size in childhood and adulthood were not associated with breast cancer risk (see Table 3). However, body size measured shortly after diagnosis, specifically BMI and WHR measured at the study interview, showed suggestive associations among Black women and stronger associations in the same directions among White women. However, the BMI and WHR associations observed were in different directions: greater measured BMI appeared to be associated with decreased risk, while greater WHR was associated with increased risk.
Among postmenopausal Black women, BMI measured at interview was not linearly associated with cancer risk (p-for-trend = 0.69), but those in the overweight (25 ≤ BMI < 30 kg/m2), class I obese (30 ≤ BMI < 35 kg/m2), and class II obese (BMI ≥ 35 kg/m2) categories appeared to have lower risk than those in the normal-weight category: OR 0.61 (0.38, 0.98), OR 0.77 (0.47, 1.28), and OR 0.58 (0.35, 0.94), respectively. Additionally, greater WHR had a suggestive association with increased cancer risk (p-for-trend = 0.08). Among postmenopausal White women, greater measured BMI at interview was associated with decreased cancer risk, but WHRs in the middle and highest tertiles were associated with increased risk versus than the lowest tertile, respectively, OR 1.53 (1.09, 2.14) and OR 1.53 (1.08, 2.18).
Adjusting recalled measures of early-life body size for reference BMI did not change results (Table 3). However, adjusting waist circumference and WHR for measured BMI did appear to increase the magnitude of their positive associations with cancer risk. For instance, among postmenopausal Black women, the OR for high waist circumference increased from 1.08 (0.77, 1.52) to 1.39 (0.92, 2.10) (p-for-trend = 0.28).
Restricting to non-users of hormone therapy
We performed additional analyses examining relationships among women who had never used HT. As expected, use of HT was uncommon in premenopausal Black or White women (<11 % of cases or controls), more common among postmenopausal Black women (30 % of cases, 38 % of controls), and most common among postmenopausal White women (58 % of cases, 61 % of controls). Among premenopausal women and postmenopausal Blacks, results were not appreciably different after excluding HT users. However, among postmenopausal Whites, excluding HT users resulted in increased point estimates for adult weight gain, measured BMI, waist circumference, and WHR. Estimates for the middle and highest tertiles of adult weight gain increased from 0.98 and 0.96 to 1.87 (1.10, 3.17) and 1.62 (0.89, 2.96), respectively. Additionally, among White premenopausal non-HT users, the association between greater measured BMI and decreased cancer risk was no longer evident. Finally, the OR for high waist circumference increased from 0.97 to 1.36 (0.86, 2.13) (p-for-trend = 0.05); for WHR, the OR for the middle tertile of WHR increased from 1.53 to 1.92 (1.04, 3.57), for the highest tertile, the OR increased from 1.53 to 2.34 (1.29, 4.24) (p-for-trend = 0.01). Adjusting adult weight gain for reference BMI and abdominal obesity measures for measured BMI did not change results substantially but tended to result in modest increases in the magnitudes of point estimates (results not shown).
Stratifying by estrogen- and progesterone-receptor status
We also estimated associations between body size and case status stratifying by estrogen- and progesterone-receptor status. Table 4 presents associations stratified by ER and PR status only among non-HT users, because HT use showed evidence of modifying associations in analyses described above.
Among Black premenopausal non-HT users, none of the results differed appreciably for cancers that were ER+ or PR+ compared to cancers that were ER− and PR− (Table 4). Among premenopausal White non-HT users, two variables that were associated with decreased cancer risk in unstratified analysis [age 10 relative weight and BMI measured at interview (see Table 2)] tended to be more strongly associated with decreased risk for ER+ or PR+ cancers than for ER− and PR− cancers. Additionally, the middle and highest tertiles of WHR tended to show associations with greater risk of ER− and PR− cancer [OR 1.89 (1.16, 3.09) and OR 1.74 (0.95, 3.18), respectively] but not ER+ or PR+ cancers. For premenopausal women, results were similar when HT users were included.
Among postmenopausal Black women, before excluding HT users, there were few associations between body size and ER+ or PR+ cancers or ER− and PR− cancers, except for suggestive relationships with reference and measured BMI (results not shown). After excluding HT users (Table 4), a suggestive trend between greater measured BMI and decreased risk of ER− and PR− cancers remained (p = 0.07), e.g., OR for BMI ≥35 = 0.26 (0.11, 0.61). Greater reference BMI and adult weight gain also showed some indications of decreased risk of ER− and PR− cancers. Among postmenopausal White women, before excluding HT users, there were not strong differences in the associations between recalled body size and ER+ or PR+ cancers or ER− and PR− cancers (results not shown). Restriction to non-HT users resulted in especially imprecise estimates among postmenopausal White women, because HT use was common in this group (Table 4). However, there were indications that a positive association between cancer risk and adult weight gain was present for ER+ or PR+ cancers (p = 0.04) but not ER− and PR− cancers (p = 0.64). Further, an association observed between measured BMI and decreased risk of cancer before excluding HT users was attenuated for ER+ or PR+ cancers after HT users were excluded. Great WHR appeared associated with increased risk for ER+ or PR+ cancer and showed an increase, though statistically non-significant ORs for ER− and PR− cancer.
Discussion
Our analyses produced two consistent findings for premenopausal breast cancer in Black and White women. First, as discussed in more detail below, larger prepubertal body size showed indications of inverse associations with breast cancer risk in premenopausal Black and White women. These associations were particularly evident for hormone-receptor positive cancers. Second, adult abdominal obesity was positively associated with premenopausal cancer. Premenopausal Black women with higher waist circumference and WHRs showed consistently higher odds ratios. Among premenopausal Whites, the higher tertiles of WHR were associated with increased cancer risk after controlling for BMI measured at interview.
Among postmenopausal Black and White women, there not were strong associations between recalled body size across the life course and breast cancer risk, except for associations between adult weight gain and risk among White non-HT users. BMI measured at interview was associated with reduced cancer risk, but the associations varied by ER/PR status as well as HT-user status.
The majority of studies of childhood body size and breast cancer risk were conducted in White populations and found that that being thinner in childhood was associated with greater risk of premenopausal breast cancer [14, 15, 26, 27]. Two studies also found similar associations with risk of postmenopausal cancer [15, 28]. The current study indicates that thin body size at age 10 is associated with increased risk of premenopausal breast cancer after taking into account racial differences in reporting peer comparisons. Specifically, Black premenopausal women who reported being “about the same” weight as peers (referent) at age 10 years were at decreased risk of breast cancer diagnosis than those who reported “thinner” weight, while Whites who reported being “heavier” were at decreased risk relative to those who reported “about the same” weight as peers. The term, “about the same,” when used by Black women likely corresponded to similar BMI as the category “heavier,” used by premenopausal White women. As evidence, 56 % of Black cases who reported being “heavier” at age 10 also reported an overweight BMI (BM ≥ 25 kg/m2) at age 18, whereas only 22 % of “heavier” White cases reported an overweight BMI at age 18. Therefore, the relevant contrast for classifying “thin” body size likely differs by race. The contrast of “heavier” versus “thinner”/“similar” among Whites is likely objectively closest to the contrast of “similar”/“heavier” versus “thinner” among Blacks. Results were robust to adjustment for later reference BMI. We did not observe an association between childhood weight and postmenopausal cancer, which has been less studied.
Leaner prepubescent body size may be associated with greater risk of breast cancer through its association with more rapid trajectories of adolescent growth, particularly greater height velocity [14, 29]. More rapid adolescent growth could increase levels of growth hormones and epithelial proliferation in the breast or decrease time for repair of DNA damage, thereby increasing risk of breast cancer [30, 31]. In the most comprehensive prospective study of childhood body size and breast cancer risk, a cohort of 2,547 British girls followed from birth to their early 50 s (1946–1999), fast height gains between ages 4 and 7 and between 11 and 15 years were the strongest childhood predictors of breast cancer risk [29]. The relationships among childhood BMI, height velocity, and breast cancer demonstrate the complex interplays in life course research on breast cancer. Although larger childhood body size is a risk factor for early puberty (which is a risk factor for breast cancer), greater childhood BMI is also independently associated with lower risk of breast cancer, particularly at premenopausal ages [29, 32]. Other theories about the association between leaner childhood body size and breast cancer risk have also been posited, including later differentiation of mammary gland cells for leaner girls [14] and greater frequency of anovulatory cycles. This second theory has not been supported by research that took into account ovulatory problems [13, 33].
Unlike other studies, we did not observe an association between greater BMI at age 18 and decreased risk of breast cancer. Cohort studies have observed strong inverse relationships between age 18 BMI and reduced risk of both premenopausal and postmenopausal breast cancer in both Black and White US women and Japanese women [13, 15, 34]. A case–control study of postmenopausal women in Sweden similarly found a suggestive protective association of high age 18 BMI but concluded it was entirely attributable to adult weight gain: women who reported being thinner at 18 age gained more weight in adulthood [28]. If, in our population, women who were thinner at age 18 tend to gain the same amount of weight or less weight in adulthood than their heavier peers, results in CBCS may differ from other populations.
Results for adult weight gain among postmenopausal White women are consistent with a recent meta-analysis that concluded that greater adult weight gain is associated with risk of postmenopausal cancer, most strongly for ER+ or PR+ cancers [35]. In CBCS, among postmenopausal White women who had never used HT, greater adult weight gain between age 18 and the reference date appeared associated with increased risk of hormone-receptor positive cancers. The associations with adult weight gain were not evident among postmenopausal Black women.
Recalled “reference” BMI was not strongly associated with cancer risk among premenopausal or postmenopausal women in our study. In contrast, BMI measured after diagnosis showed inverse associations with cancer risk that were modified by HT use. Results for recalled “reference” BMI may differ from results for measured post-diagnosis BMI for several reasons. Associations with measured BMI may be biased downward because of disease-related weight loss (cachexia) [36]. Alternatively, results for self-reported “reference” BMI may be subject to measurement bias. Consistent with previous research showing that US women systematically underreport their weight [37], control women tended to misreport their heights and weights in ways that led to underestimates of their self-reported reference BMI. For instance, among Blacks controls, 21 % reported reference date BMI <25 but only 14 % had BMI <25 when measured at the interview, when we would expect controls’ reference weights a year before interview to be similar to weights measured at the interview. The same pattern was evident among Whites: 52 % reported reference BMI <25 but only 44 % were measured at interview as under 25.
Greater WHR was associated with increased cancer risk in several subgroup analyses, with no evidence of modification by ER/PR status. Stronger relationships with increased cancer risk for measures of abdominal obesity versus BMI have been documented in other studies [13, 38, 39]. For example, in the BWHS, while higher BMI tended to be associated with decreased risk of premenopausal cancer, greater abdominal adiposity tended to be associated with increased risk [13]. Some studies of Black women, however, find that waist circumference is more predictive of increased risk than WHR [38, 40]. While waist circumference and WHR are both indicators of abdominal obesity [41, 42], WHR may be more strongly correlated with subcutaneous abdominal fat while waist circumference may be more strongly correlated with visceral adipose tissue [43–45]. Because the deep visceral fat is more specifically correlated with metabolic abnormalities, such as insulin resistance, it is possible that waist circumference and WHR may reflect distinct risk pathways associated with cancer etiology.
Several of the limitations of this work should be noted. Many of the body size measures were assessed retrospectively and are subject to recall bias. In particular, the measure of childhood body size was subjective and dependent on the normative body size norm of a woman’s family and peer group. Further, as with all case–control studies, disease- or treatment-related weight change could cause bias for measures assessed after diagnosis. Additionally, some selected controls could not be located or refused participation in the study. However, in phase 1 of CBCS, mean BMI did not differ between women who participated in the study and those agreeing only to a brief telephone survey [46]. There may be heterogeneity in the relationship between body size and breast cancer incidence by breast cancer subtype [47]. Racial differences and differences among studies may reflect differences in the mix of cancer subtypes comprising the cancer cases in each group [36]. Finally, classification of menopausal status did not take into account use of HT.
The work has unique strengths. This analysis comprehensively studied life course body size and breast cancer risk among Black American women. Additionally, we focused on a Black population in the South, the US region where the majority (55 %) of Black Americans lives [48]. The study was population-based and used a rapid ascertainment system to interview and measure 95 % of breast cancer cases within 12 months of diagnosis, limiting selection bias from mortality and measurement bias from treatment and disease-related weight gain. We also conducted supplemental analyses to evaluate whether HT affected associations. Restricting to non-users of HT changed several associations among postmenopausal White women, a group with high prevalence of HT use in our study. These findings confirm that HT is an important modifier to consider in studies of body size and cancer risk, particularly in populations with high HT usage.
This research adds further evidence that the processes by which body size influences breast cancer risk are complex, varying by period in the life course, menopausal status, HT use, and tumor subtype. Additionally, the results for the association between childhood weight and premenopausal breast cancer add further evidence that early-life body size has long-term influences on adult cancer risk. Additionally, consistent with a recent meta-analysis [6], we failed to find strong positive associations between greater BMI near the time of diagnosis and risk of breast cancer, but did find positive associations with greater WHR.
References
SEER (2011) SEER cancer statistics review, 1975–2008. National Cancer Institute, Bethesda, MD [cited 2011]. http://seer.cancer.gov/csr/1975_2008
Zaloznik AJ (1995) Breast cancer stage at diagnosis: Caucasians versus Afro-Americans. Breast Cancer Res Treat 34(3):195–198
Shinagawa SM (2000) The excess burden of breast carcinoma in minority and medically underserved communities: application, research, and redressing institutional racism. Cancer 88(5 Suppl):1217–1223
Flegal KM, Carroll MD, Kit BK, Ogden CL (2012) Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. J Am Med Assoc 307(5):491–497
World Cancer Research Fund/American Institute for Cancer Research (2010) Food, nutrition, physical activity, and the prevention of breast cancer. American Institute for Cancer Research, Washington, DC
Cheraghi Z, Poorolajal J, Hashem T, Esmailnasab N, Doosti Irani A (2012) Effect of body mass index on breast cancer during premenopausal and postmenopausal periods: a meta-analysis. PLoS One 7(12):e51446
Sexton KR, Franzini L, Day RS, Brewster A, Vernon SW, Bondy ML (2011) A review of body size and breast cancer risk in Hispanic and African American women. Cancer 117(23):5271–5281
Hall IJ, Newman B, Millikan RC, Moorman PG (2000) Body size and breast cancer risk in black women and white women: the Carolina Breast Cancer Study. Am J Epidemiol 151(8):754–764
Adams-Campbell LL, Kim KS, Dunston G, Laing AE, Bonney G, Demenais F (1996) The relationship of body mass index to reproductive factors in pre- and post-menopausal African-American women with and without breast cancer. Obes Res 4(5):451–456
Schatzkin A, Palmer JR, Rosenberg L, Helmrich SP, Miller DR, Kaufman DW et al (1987) Risk factors for breast cancer in black women. J Natl Cancer Inst 78(2):213–217
Zhu K, Caulfield J, Hunter S, Roland CL, Payne-Wilks K, Texter L (2005) Body mass index and breast cancer risk in African American women. Ann Epidemiol 15(2):123–128
Berstad P, Coates RJ, Bernstein L, Folger SG, Malone KE, Marchbanks PA et al (2012) A case–control study of body mass index and breast cancer risk in white and African-American women. Cancer Epidemiol Biomark Prev 19(6):1532–1544
Palmer JR, Adams-Campbell LL, Boggs DA, Wise LA, Rosenberg L (2007) A prospective study of body size and breast cancer in black women. Cancer Epidemiol Biomark Prev 16(9):1795–1802
Baer HJ, Colditz GA, Rosner B, Michels KB, Rich-Edwards JW, Hunter DJ et al (2005) Body fatness during childhood and adolescence and incidence of breast cancer in premenopausal women: a prospective cohort study. Breast Cancer Res 7(3):R314–R325
Harris HR, Tamimi RM, Willett WC, Hankinson SE, Michels KB (2011) Body size across the life course, mammographic density, and risk of breast cancer. Am J Epidemiol 174(8):909–918
Newman B, Moorman PG, Millikan R, Qaqish BF, Geradts J, Aldrich TE et al (1995) The Carolina Breast Cancer Study: integrating population-based epidemiology and molecular biology. Breast Cancer Res Treat 35(1):51–60
Weinberg CR, Sandler DP (1991) Randomized recruitment in case–control studies. Am J Epidemiol 134(4):421–432
Weinberg CR, Wacholder S (1990) The design and analysis of case–control studies with biased sampling. Biometrics 46(4):963–975
World Health Organization (1995). Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organization technical report series 854:1–452. PubMed PMID: 8594834. Epub 1995/01/01. eng
Expert panel on the identification, evaluation, and treatment of overweight in adults (1998) Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: executive summary. Am J Clin Nutr 68(4):899–917
Moorman PG, Kuwabara H, Millikan RC, Newman B (2000) Menopausal hormones and breast cancer in a biracial population. Am J Public Health 90(6):966–971
Rosner B, Colditz GA (2011) Age at menopause: imputing age at menopause for women with a hysterectomy with application to risk of postmenopausal breast cancer. Ann Epidemiol 21(6):450–460
Hernan MA, Hernandez-Diaz S, Robins JM (2004) A structural approach to selection bias. Epidemiology 15(5):615–625
Glymour MM, Weuve J, Berkman LF, Kawachi I, Robins JM (2005) When is baseline adjustment useful in analyses of change? An example with education and cognitive change. Am J Epidemiol 162(3):267–278
Hall IJ, Moorman PG, Millikan RC, Newman B (2005) Comparative analysis of breast cancer risk factors among African-American women and White women. Am J Epidemiol 161(1):40–51
Ahlgren M, Melbye M, Wohlfahrt J, Sorensen TI (2004) Growth patterns and the risk of breast cancer in women. N Engl J Med 351(16):1619–1626
De Stavola BL (2004) Childhood growth and breast cancer. Am J Epidemiol 159(7):671–682
Magnusson C, Baron J, Persson I, Wolk A, Bergstrom R, Trichopoulos D et al (1998) Body size in different periods of life and breast cancer risk in post-menopausal women. Int J Cancer Journal international du cancer 76(1):29–34
De Stavola BL, dos Santos Silva I, McCormack V, Hardy RJ, Kuh DJ, Wadsworth ME (2004) Childhood growth and breast cancer. Am J Epidemiol 159(7):671–682
Berkey CS, Frazier AL, Gardner JD, Colditz GA (1999) Adolescence and breast carcinoma risk. Cancer 85(11):2400–2409
Hilakivi-Clarke L, Forsen T, Eriksson JG, Luoto R, Tuomilehto J, Osmond C et al (2001) Tallness and overweight during childhood have opposing effects on breast cancer risk. Br J Cancer 85(11):1680–1684
Le Marchand L, Kolonel LN, Earle ME, Mi MP (1988) Body size at different periods of life and breast cancer risk. Am J Epidemiol 128(1):137–152
Michels KB, Terry KL, Willett WC (2006) Longitudinal study on the role of body size in premenopausal breast cancer. Arch Intern Med 166(21):2395–2402
Suzuki R, Iwasaki M, Inoue M, Sasazuki S, Sawada N, Yamaji T et al (2011) Body weight at age 20 years, subsequent weight change and breast cancer risk defined by estrogen and progesterone receptor status: the Japan public health center-based prospective study. Int J Cancer Journal international du cancer 129(5):1214–1224
Vrieling A, Buck K, Kaaks R, Chang-Claude J (2010) Adult weight gain in relation to breast cancer risk by estrogen and progesterone receptor status: a meta-analysis. Breast Cancer Res Treat 123(3):641–649
Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K et al (2006) Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 295(21):2492–2502
Jain RB (2010) Regression models to predict corrected weight, height and obesity prevalence from self-reported data: data from BRFSS 1999–2007. Int J Obes (Lond) 34(11):1655–1664
Bandera EV, Chandran U, Zirpoli G, Gong Z, McCann SE, Hong CC et al. (2013) Body fatness and breast cancer risk in women of African ancestry. BMC Cancer 13:475
Amadou A, Ferrari P, Muwonge R, Moskal A, Biessy C, Romieu I et al (2013) Overweight, obesity and risk of premenopausal breast cancer according to ethnicity: a systematic review and dose–response meta-analysis. Obes Rev 14(8):665–678
John EM, Sangaramoorthy M, Phipps AI, Koo J, Horn-Ross PL (2011) Adult body size, hormone receptor status, and premenopausal breast cancer risk in a multiethnic population: the San Francisco Bay Area breast cancer study. Am J Epidemiol 173(2):201–216
Hu FB (2008) Obesity and cancer. In: Hu FB (ed) Obesity epidemiology. Oxford University Press, New York, pp 174–195
Schapira DV, Clark RA, Wolff PA, Jarrett AR, Kumar NB, Aziz NM (1994) Visceral obesity and breast cancer risk. Cancer 74(2):632–639
Rose DP, Komninou D, Stephenson GD (2004) Obesity, adipocytokines, and insulin resistance in breast cancer. Obes Rev 5(3):153–165
Raikkonen K, Matthews KA, Kuller LH (1999) Anthropometric and psychosocial determinants of visceral obesity in healthy postmenopausal women. Int J Obes Relat Metab Disord 23(8):775–782
Bonora E, Micciolo R, Ghiatas AA, Lancaster JL, Alyassin A, Muggeo M et al (1995) Is it possible to derive a reliable estimate of human visceral and subcutaneous abdominal adipose tissue from simple anthropometric measurements? Metab Clin Exp 44(12):1617–1625
Moorman PG, Newman B, Millikan RC, Tse CK, Sandler DP (1999) Participation rates in a case-control study: the impact of age, race, and race of interviewer. Ann Epidemiol 9(3):188–195
Harris HR, Willett WC, Terry KL, Michels KB (2011) Body fat distribution and risk of premenopausal breast cancer in the Nurses’ Health Study II. J Natl Cancer Inst 103(3):273–278
Rastogi S, Johnson TD, Hoeffel EM, Drewery Jr. MP (2011) The Black population: 2010. In: Bureau USC (ed) Washington, DC: U.S. Department of Commerce
Acknowledgments
This research was funded in part by the University Cancer Research Fund of North Carolina and the National Cancer Institute Specialized Program of Research Excellence (SPORE) in Breast Cancer (NIH/NCI P50-CA58223). Dr. Robinson was supported by the National Cancer Institute (1K01CA172717-01). Dr. Troester was supported by the following grants from the National Institutes of Health: U01 ES019472; P30 ES010126; P30 DK056350; and P50 CA151135. This research was supported in part by a grant from the National Institute of Environmental Health Sciences (P30ES010126). We are grateful to the Carolina Population Center (R24 HD050924) for general support.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Robinson, W.R., Tse, C.K., Olshan, A.F. et al. Body size across the life course and risk of premenopausal and postmenopausal breast cancer in Black women, the Carolina Breast Cancer Study, 1993–2001. Cancer Causes Control 25, 1101–1117 (2014). https://doi.org/10.1007/s10552-014-0411-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-014-0411-5