
Abstract
Purpose
Colorectal cancer (CRC) incidence rates have increased among young adults and have decreased among older adults. We re-evaluated these trends using more recent data covering about 96 % of the United States population.
Methods
Colorectal cancer incidence rates were abstracted from the National Program of Cancer Registries and the Surveillance Epidemiology and End Results analytic files for diagnosis years 1998–2009. We report rates for young adults (age <50 years) and for older adults (age 50 years or older) by four race/ethnicity groupings. We examined CRC incidence rates by stage at diagnosis, tumor subsite, and state. We calculated the correlation between state-specific CRC incidence and prevalence of colonoscopy reported in the Behavioral Risk Factor Surveillance System.
Results
Rectal cancer incidence rates increased from 1998 through 2009 among young non-Hispanic white adults and young blacks. Among older adults, CRC incidence rates decreased among all four race/ethnicity groupings and in all states. The decline was apparent for all stages and for all subsites. States with greater decreases in CRC incidence rates had higher colonoscopy screening rates.
Conclusion
Rectal cancer is increasing among younger adults, for reasons largely unknown. Among older adults, CRC incidence continues to decrease, probably because of increasing uptake of colonoscopy screening. Decreases in CRC incidence are correlated with increased use of colonoscopy, indicating that CRC may be largely preventable through colonoscopy screening. Efforts to increase screening rates in underserved populations would help reduce health disparities associated with this type of cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 2008, the US Preventive Services Task Force (USPSTF) recommended screening for colorectal cancer (CRC) in adults beginning at age 50 years and continuing until age 75 using (1) annual high-sensitivity fecal occult blood testing or (2) sigmoidoscopy every five years combined with high-sensitivity fecal occult blood testing every three years or (3) colonoscopy every 10 years [1]. These recommendations represented a policy change. In 2002, the USPSTF recommended CRC screening in all adults aged 50 years or older. The updated guidelines do not include routine screening in adults age 75 through 85 and recommend against screening in adults older than 85 [1]. The reduction in mortality associated with CRC screening is due to the detection and removal of early-stage cancer or precancerous lesions [1]. Colonoscopy is a component in any CRC screening program since follow-up of positive screening tests requires colonoscopy [1].
The benefits of CRC screening have become evident in national cancer statistics. The CRC incidence rates among adults aged 50 years or older have declined in recent years [2]. In contrast, CRC incidence rates among young (ages 20–49) non-Hispanic (NH) white men and women and Hispanic men increased between 1992 and 2005, while CRC incidence rates among young NH black and Asian men and women and Hispanic women remained stable [3].
The purpose of this report is to evaluate CRC incidence trends from 1998 to 2009 stratified by age (younger than 50 years and 50 years or older), nationally, and by state using combined data from the CDC’s National Program for Cancer Registries (NPCR) and the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program. While these registries included the entire US population, the CRC incidence data included in our analysis covered about 96 % of the population between 1998 and 2009.
Materials and methods
Data were abstracted from a combined NPCR and SEER analytic file using the SEER*Stat program, version 8.0.1 [4]. We excluded from analyses data for the years a state did not meet the quality standards for publication in the United States Cancer Statistics (USCS) [5]. Data were obtained from 45 NPCR state cancer registries, the District of Columbia (DC), and from five SEER state cancer registries. The minimum number of years of state data was seven (two states), while 40 states had data for the full 12 years. The use of the term, state, henceforth refers to the 50 states and the DC. We combined the data from all states for the purpose of conducting anatomic subsite and stage-specific analyses and to obtain the overall US CRC incidence rates. We also obtained each state-specific overall CRC incidence rate for the purpose of state comparisons. Analyses were stratified by age: young adults (<50 years of age) or older adults (aged 50 years or older). These two age groups were never combined.
The rubric CRC included the cecum (International Classification of Diseases for Oncology, third edition [6] = C180), appendix (C181), ascending colon (C182), hepatic flexure (C183), transverse colon (C184), splenic flexure (C185), descending colon (C186), sigmoid colon (C187), large intestine—NOS (C188, C189, C260), rectosigmoid junction (C199), and rectum (C209). Anatomic subsite analyses included the proximal colon [cecum, ascending colon, hepatic flexure, transverse colon, and splenic flexure], the distal colon [descending colon and sigmoid colon], and rectum [rectum and rectosigmoid junction].
Colorectal cancer stage at diagnosis was classified according to the extent of disease [local, regional, distant, and unknown] using the SEER 1977 and 2000 staging schemes [7, 8]. During the study period, stage coding for cancer was affected by the publication of national guidelines for state registries (i.e., SEER 2000) and especially by the introduction of collaborative staging (CS) in 2004 [9, 10]. Thus, to maintain comparability of CRC stage coding across the study period (1998–2009), we used a “standardized” staging system we developed [11].
We classified race/ethnicity for the US analyses as non-Hispanic whites (NHWs), Hispanic whites, blacks (regardless of Hispanic ethnicity), and Asians (regardless of Hispanic ethnicity), using the classifications available in the NPCR/SEER analytic files. We did not include American Indians/Alaska Natives in this analysis because of small numbers. For state-specific analyses, we classified race/ethnicity as whites (NHWs and Hispanic whites) and blacks.
We calculated age-standardized CRC incidence rates for younger adults (age <50 years) and for older adults (age ≥ 50 years) using the 2000 standard million US age population, truncated appropriately for the younger or older age group. We calculated the annual percent change (APC) in CRC incidence rates using the formula \( {\text{APC}} = \left( {e^{{b_{1} }} \text{ - }1} \right) \times 100 \) where b 1 is the slope from the weighted regression of the logarithm of the rate on year of diagnosis using the case count as the analytic weight. We displayed a funnel plot of the state APCs in CRC incidence rates according to their standard errors to highlight states with high and low APCs [12].
We obtained information on sigmoidoscopy/colonoscopy use from the CDC’s Behavioral Risk Factor Surveillance System (BRFSS) for the years 1997, 1999, 2002, 2004, 2006, and 2008 [13]. Respondents aged 50 years or older were asked whether they ever had a sigmoidoscopy/colonoscopy. In 1997, the question pertained to sigmoidoscopy/proctoscopy, but this year is included in the BRFSS online statistics in the category sigmoidoscopy/colonoscopy. We regressed the logarithm of the odds (% Yes ÷ % No) of the response on year of survey for each state and plotted the slope from these models against the state APC in CRC incidence rates. We also obtained the overall % Yes according to state across survey years and plotted this variable against the state APC in CRC incidence rates. For brevity, sigmoidoscopy/colonoscopy is referred to as S/C endoscopy henceforth.
Statistical analyses were performed using Stata version 12 [14].
Results
Younger adults (aged <50 years):
Among young NHWs, CRC incidence rates increased during the period 1998 through 2009 (APC = 1.61 (95 % CI 1.35, 1.87) among men and 1.79 (1.46, 2.11) among women). Overall CRC incidence rates did not increase significantly from 1998 through 2009 among young blacks, Asians, and Hispanic whites (Table 1).
The increase in CRC cancer incidence from 1998 through 2009 differed by proximal colon, distal colon, or rectal subsite (Table 1). Among NHWs, the largest increase was observed for rectal cancer and the second largest increase for distal colon. The increases for these two subsites were not statistically significantly different from each other, but the increase in proximal colon was significantly smaller than was the increase for distal colon and rectal cancer. Among young black adults, rectal cancer incidence increased significantly among men and women between 1998 and 2009, while proximal colon and distal colon cancer rates were stable. The increase in CRC among young NHWs was evident for local, regional, and distant stages.
Older adults (aged 50 years or older)
The APCs in CRC incidence according to stage and subsite at diagnosis by race/ethnicity and gender are displayed in Table 2. CRC incidence rates declined from 1998 through 2009 among each of the four race/ethnicity groups. The decline is apparent for all stages, although the incidence rate of regional CRC declined most rapidly. The difference in the rate of decline of regional CRC compared with the average rate of decline of local and distal CRC was statistically significant for blacks, Asians, and Hispanic whites.
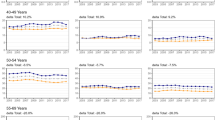
The incidence rates of proximal, distal, and rectal CRC significantly decreased from 1998 through 2009 among each of the four race/ethnicity groups (Table 2, Fig. 1). The rate of decline for proximal, distal, and rectal CRC was not statistically significantly different among blacks, Asians, and Hispanic whites. For NHWs, the rate of decline of the incidence rate of distal CRC was significantly larger than was the average rate of decline of proximal and rectal CRC. Overall CRC incidence rates are highest for blacks, followed by NHWs, then Hispanic whites, and are lowest for Asians. The decrease in CRC incidence was largest for NHWs (p < 0.0001) compared with the other three race/ethnicity groups and about equal for the other three race/ethnicity groupings (p > 0.20). From 1998 through 2009, CRC annual incidence rates among adults aged 50 years or older declined from 210.1/105 to 162.6/105 among blacks (an 23 % reduction), from 140.2/105 to 107.9/105 among Asians (a 23 % reduction), from 157.0/105 to 116.9/105 among Hispanic whites (a 26 % reduction), and from 196.5/105 to 132.9/105 among NHWs (a 32 % reduction).

Logarithm of CRC incidence rates by year (1998–2009) and tumor subsite according to race/ethnicity among adults aged 50 years or older, all states combined
State-based CRC rates among older adults
The APCs for CRC incidence for each of the 50 states and for the District of Columbia are displayed in map format for whites in Fig. 2a and for blacks in Fig. 2b. For whites, CRC incidence declined in all states, but the decline was not statistically significant for Hawaii. The mean APC for NHWs across states was −3.13 (−3.41, −2.86)95 %, while the average APC weighted by the inverse variance of the state-specific APCs was −3.02 (−3.10, −2.95)95 %.

a APCs in overall CRC incidence rates among whites aged 50 years or older by state. b APCs in overall CRC incidence rates among balcks aged 50 years or older by state
For blacks, we excluded 11 states from the analysis because they had fewer than 100 CRC cases during the study period. Of the 40 remaining states, the CRC incidence rates decreased in 38 states, of which 28 were statistically significant. The mean APC for blacks across states was −2.29 (−2.76, −1.83)95 %, while the weighted average was −1.94 (−2.12, −1.76). The state-level mean difference in the APCs for blacks versus whites was 0.87 (95 % CI 0.43, 1.31; p = 0.0003) in the 40 states with a 100 or more black CRC cases.
The findings for whites and blacks combined are displayed as a funnel plot in Fig. 3. States at the bottom of the figure provide the most precise APCs. States on the left of the figure had the largest decreases in CRC incidence. The mean APC was −3.02 (−3.28, −2.75), while the weighted average APC was −2.91 (−2.98, −2.84). The APC was below zero for all states, and the decrease in CRC incidence was statistically significant for 50 states. The smallest decreases in CRC incidence rates were in Hawaii (−0.40), Alabama (−0.54), and North Dakota (−1.35); all of their APCs are outside the pseudo 95 % CI, and the APC for Hawaii is not statistically significant. The states with the largest decreases in CRC incidence are Wisconsin (−4.55), Vermont (−4.47), and Rhode Island (−4.40). States that have better-than-average decreases in CRC incidence and are considerably outside the pseudo 95 % limits are Wisconsin (−4.55), Vermont (−4.47), Rhode Island (−4.40), Maryland (−4.17), and Florida (−4.08).

Funnel plot of state-specific APC in overall CRC among adults aged 50 years or older
CRC incidence rates and colonoscopy among older adults
The correlation between state-level annual percentage changes in CRC incidence among whites and blacks and the average BRFSS self-reported colonoscopy rates across years was −0.57 (p < 0.0001) (Fig. 4a). That is, states with greater decreases in CRC incidence rates during the study period tended to have higher colonoscopy screening rates. Additionally, states that experienced greater decreases in CRC incidence rates generally also experienced greater increases in colonoscopy screening rates in BRFSS (correlation between annual percentage change in CRC incidence and annual percentage change in colonoscopy rates = −0.43; p = 0.002) (Fig. 4b).

a Correlation between state-level change in overall CRC incidence rates and S/C endoscopy screening rates among US adults aged 50 years or older. b Correlation between state-level change in overall CRC incidence rates and change in S/C endoscopy screening rates among US adults aged 50 years or older
Discussion
Our analysis using a large nationally representative dataset shows CRC incidence increased from 1998 through 2009 among young NHW adults, extending and expanding the findings reported in the SEER 13 registries from 1992 through 2005 [2]. These data indicate that CRC incidence rates among young black, Asian, and Hispanic white men and women increased from 1998 through 2009, but the increases were small and not statistically significant. The increase in CRC incidence rates among the young NHWs was strongest for rectal cancer, but evident for distal colon cancer as well. Additionally, we found a statistically significant increase in rectal cancer among young black men and women and small and non-significant increases among Asians and Hispanic whites. An advantage of the national data compared with the SEER registries is that it is possible to evaluate trends among minority racial/ethnic groups. In addition, the NPCR data add significantly more data from regions and populations in the USA where cancer rates are higher due to differences in risk factors such as smoking [15].
The increase in distal colon cancer and rectal cancer incidence among young adults is largely unexplained. Siegel et al. [3] suggested that the increased prevalence over the last three decades of obesity and type 2 diabetes, which are risk factors for CRC, may partially account for the increased CRC incidence rates in young adults. Larsson et al. [16] estimate that the rate of CRC increases about 20 % per 5 Unit (kg/m2) increase in body mass index (BMI), a standard measure of excess weight. Among NHWs’ ages 20 through 49, mean BMI increased from 25.7 in 1998 to 28.1 kg/m2 in 2009 [17] with a corresponding APC of 1.69 for CRC incidence rates among young NHW adults. Using these statistics, we estimate that about 48 % of the increase in CRC incidence among young NHW adults may be due to increased BMI. Additionally, we allowed for a 5-year temporal lag in the population BMI measurements (25.0 in 1993 to 27.4 kg/m2 in 2004) and for a 10-year lag (24.2 in 1988 and 25.8 kg/m2 in 1999) and obtained estimates of the increase in CRC due to increased BMI of 48 % and 31 %, respectively. We note, however, that the attribution of the recent increase in CRC incidence rates among the young to increased obesity among them in this ecologic analysis is speculative. The prevalence of diabetes among NHW young adults in 1998 was 1.8 %, while in 2009, it was about 5.2 % [17]. Larsson et al. [18] estimate that the rate of CRC is about 30 % higher among diabetics compared with non-diabetics. These statistics suggest that the increase in the prevalence of diabetes among young NHWs can explain only about 5 % of the increased incidence rate of CRC. Allowance for a five- and 10-year lag periods reduces the estimates to 4 % and to 0 %, respectively, reinforcing the notion that an increasing prevalence of diabetes is not a cause of the increased rates of CRC in young adults. We did not do the corresponding calculation for blacks either for BMI or for diabetes since CRC incidence rates increased only 0.38 % per year from 1998 through 2009 among young black adults. The observation that diabetes is related both to colon and to rectal cancer [18] and the effect of obesity, if anything, is slightly stronger for colon versus rectal cancer [16] detracts from the notion that changes in obesity and diabetes are responsible for the increase in the rates of rectal cancer among young adults.
Among older adults, CRC incidence rates declined from 1998 through 2009 among each of the four race/ethnicity groups. The decline was highest among NHWs, but statistically significant declines were apparent among blacks, Asians, and Hispanic whites. The decline was about equal for proximal colon, distal colon, and rectal cancers among blacks, Asians, and Hispanic whites and was highest for distal colon cancer among NHWs. For extent of disease, the declines in CRC incidence were apparent for all stages among whites, blacks, and Hispanic whites with largest declines in regional-stage CRC for all race/ethnicity groupings.
With respect to states, it is remarkable that CRC incidence rates declined significantly from 1998 through 2009 among whites in almost all states and among blacks in 28 of the 40 states with sufficient data to analyze. APCs in CRC incidence rates were inversely correlated with colonoscopy screening rates as well as with changes in the uptake of colonoscopy screening in the period 1997 through 2008.
Naishadham et al. [19] reported a correlation of −0.65 between the percentage change in CRC mortality rates between 1990–1994 and 2003–2007 and colon cancer screening rates (fecal occult blood test (FOBT), sigmoidoscopy, or colonoscopy). Our analysis verifies this finding, although an advantage of our approach is that we use incidence rather than mortality rates, and we restricted our definition of screening to colonoscopy because it is the most commonly used CRC screening test [20]. Data from the 2010 National Health Interview Survey (NHIS) indicate that while FOBT use was high among adults with military health care insurance (17.5 %), associations with other sociodemographic and health care variables were similar as with colonoscopy [20]. Data from the BRFSS demonstrate that the use of FOBT among US adults aged 50–75 decreased from 21.1 to 11.8 % from 2002 to 2010 [21]. Results from the NHIS show that in 2000, 34 % of US adults aged 50–75 reported getting any colorectal test or procedure and 19 % reported getting a colonoscopy; in 2010, 59 % reported getting any colorectal test or procedure and 55 % reported getting a colonoscopy [22]. While FOBT is effective for the early detection of colorectal cancer and decreases colorectal cancer mortality, since the use of FOBT is declining and the use of colonscopy is increasing, decreases in colorectal cancer incidence are likely to be due to the increased use of colonoscopy. Typically, in cancer screening, it is anticipated that the beneficial effect of screening will be reflected in a decline in mortality, not incidence rates. In fact, incidence rates are likely to increase just after the initiation of a screening program since some early latent cancers will be detected by the screening program. However, colonoscopy is different in that its application leads to a reduction in incidence rates (and therefore mortality rates as well). The decrease in incidence is apparent for the entire colon/rectum and for all stages. Such a pattern probably results from excising pre-malignant lesions throughout the entire colon with a corresponding decrease in proximal and distal colon cancers and a general decrease across all stages.
Our analysis of colonoscopy screening rates and trends in CRC incidence rates has all the limitations of any ecologic analysis. In short, some other temporal factor correlated with colonoscopy rates may account for the decline in the state CRC incidence rates. Yet, it is difficult to imagine how an extraneous factor would cause a decrease in CRC incidence rates in older adults given that rectal cancer and distal colon cancer incidence rates have increased in young adults. Colonoscopy is the most likely explanation since its use is confined to those experiencing the benefit of decreased CRC rates (adults aged 50 years or older), its prevalence is sufficiently high (~50 %), and it is biologically plausible that the removal of pre-cancerous lesions would result in a decrease in the occurrence of CRC.
In summary, CRC incidence rates, especially distal colon cancer and rectal cancer, have increased in recent years among young adults for reasons largely unknown, although some of the increase may be explained by increased prevalence of obesity. Among older adults, the decline in CRC incidence rates in recent years has been large, widespread across states, evident across all race/ethnic groups, and most likely attributable to increased uptake of screening, especially colonoscopy.
References
U.S. Preventive Services Task Force (2008) Screening for colorectal cancer. Recommendation statement. Oct 2008 www.uspreventiveservicestaskforce.org
Siegel RL, Ward EM, Jemal A (2012) Trends in colorectal cancer incidence rates in the United States by tumor location and stage, 1992-2008. Cancer Epidemiol Biomarkers Prev 21:411–416
Siegel RL, Jemal A, Ward EM (2009) Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev 18:1695–1698
Surveillance Research Program, National Cancer Institute SEER*Stat software version 7.0.5. Available at: seer.cancer.gov/seerstat
National Program of Cancer Registries, United States Cancer Statistic, Centers for Disease Control and Prevention (2012) Available at http://www.cdc.gov/cancer/npcr/uscs/technical_notes/criteria.htm/ Accessed 14 Feb 2012
SEER Site Recode, ICD-O-3 (1/27/2003) Definition (2012) Available at: http://seer.cancer.gov/siterecode/icdo3_d01272003/ Accessed 19 Sept 2012
Fritz A, Ries L (eds) (2012) SEER extent of disease-1988. Codes and coding instructions, 3rd edn. National Cancer Institute 1998 available at: http://seer.cancer.gov/manuals/EOD10Dig.pub.pdf. Accessed 19 Sept 2012
Young JL Jr, Roffers SD, Ries LAG, Fritz AG, Hurlbut AA (eds) (2012) SEER summary staging manual-2000: codes and coding instructions, National Cancer Institute, NIH Pub. No. 01-4969, Bethesda, MD, 2001. Available at: http://seer.cancer.gov/tools/ssm/. Accessed 4 Jan 2012
Collaborative Staging Task Force of the American Joint Committee on Cancer. Collaborative Staging Manual and Coding Instructions, version 01.04.00: Jointly published by American Joint Committee on Cancer (Chicago, IL) and U.S. Department of Health and Human Services (Bethesda, MD), 2004. NIH Publication Number 04-5496. Incorporates updates through 8 Sept 2006
Collaborative Staging Task Force. Collaborative Stage Data Collection System, Collaborative Staging (2012) Available at: http://www.cancerstaging.org/cstage/cstageintro.html. Accessed 3 Jan 2012
Austin H, Duong LM, King J, Richardson LC, Eheman C (2012) A method to adjust for stage coding changes in the national program of cancer registries illustrated for colorectal cancer. J Regist Manag 39(2):62–68
Spiegelhalter DJ (2005) Funnel plots for comparing institutional performance. Stat Med 24:1185–1202
Centers for Disease Control and Prevention (CDC). Behavioral risk factor surveillance system survey data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 1997, 1999, 2002, 2004, 2006, and 2008. Available at http://www.cdc.gov/brfss/index.htm Accessed 16 April 2013
StataCorp. (2011) Stata: release 12. Stata Corp LP, College Station
Wingo PA, Jamison PM, Hiatt RA, Weir HK, Gargiulla PM, Hutton M, Lee NC, Hall HI (2003) Building the infrasctructure for nationwide cancer surveillance and control: a comparison between The National Program of Cancer Registries (NPCR) and The Surveillance, Epidemiology, and End Results (SEER) Program (United States). Cancer Causes Control 14:175–193
Larsson SC, Wolk A (2007) Obesity and colon and rectal cancer risk: a meta-analysis of prospective studies. Am J Clin Nutr 86:556–565
Centers for Disease Control and Prevention (CDC). Behavioral risk factor surveillance system survey data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Available at http://www.cdc.gov/brfss/index.htm Accessed 16 April 2013
Larsson SC, Orsini N, Wolk A (2005) Diabetes mellitus and risk of colorectal cancer: a meta-analysis. J Natl Cancer Inst 97:1679–1687
Naishadham D, Lansdorp-Vogelaar I, Siegel R, Cokkinides V, Jemal A (2011) State disparities in colorectal cancer mortality patterns in the United States. Cancer Epidemiol Biomarkers Prev 20(7):1296–1302
Shapiro JA, Klabunde CN, Thompson TD, Nadel MR, Seeff LC, White A (2012) Patterns of colorectal cancer test use, including CT colonography, in the 2010 National Health Interview Survey. Cancer Epidemiol Biomarkers Prev 21(6):895–904
Centers for Disease Control and Prevention (2011) Vital signs: colorectal cancer screening, incidence, and mortality-United States, 2002–2010. MMWR Morb Mortal Wkly Rep 60(26):884–889
National Center for Health Statistics (2013) Health, United States, 2012: with special feature on emergency care. Hyattsville, MD
Conflict of interest
No author has any conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
These data were provided by the central cancer registries participating in either the National Program of Cancer Registries (NPCR) (November 2011 data submission) or the Surveillance, Epidemiology, and End Results (SEER) Program (November 2011 submission).
Rights and permissions
About this article
Cite this article
Austin, H., Jane Henley, S., King, J. et al. Changes in colorectal cancer incidence rates in young and older adults in the United States: what does it tell us about screening. Cancer Causes Control 25, 191–201 (2014). https://doi.org/10.1007/s10552-013-0321-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-013-0321-y