
Abstract
Metabolic syndrome (MetS) is an established risk factor for cardiovascular diseases and mortality. Limited data are available on the prevalence of MetS and its association with exercise among breast cancer survivors. The present study included 1,696 breast cancer survivors from the Shanghai Breast Cancer Survival Study, a population-based prospective cohort study conducted between April 2002 and October 2011 in Shanghai, China. All women had a physical examination taken at study clinic approximately 60 months post-diagnosis. Exercise was assessed at approximately 6, 18, 36, and 60 months post-diagnosis. Information on medical history, tumor characteristics, cancer treatment, anthropometrics, and lifestyle was collected at study enrollment. Associations between exercise and MetS at 60 months post-diagnosis were evaluated with multivariable logistic regression models. The mean age of the study population was 56.68 at 60-month survey, and the mean follow-up since cancer diagnosis was 63.66 months. The prevalence of MetS using National Cholesterol Education Program Adult Treatment Panel III criteria at approximately 60 months after diagnosis was 33.14 %. Among overweight and obesity breast cancer survivors (body mass index (BMI) ≥ 25 kg/m2 at baseline), the prevalence was 55.18 %. The most common type of exercise in this population was walking (45.40 %) at baseline. Exercise participation between 6 and 60 months post-diagnosis was inversely associated with the prevalence of MetS with the adjusted odds ratio (OR) for exercise participation of ≥3.5 h/week (30 min/day) being 0.69 (95 % confidence interval (CI) 0.48–0.98). In addition consistent exercise participation reduced the prevalence of MetS (adjusted OR 0.70 (95 % CI 0.50–1.00). Associations of exercise with MetS were not modified by baseline waist circumference, BMI, comorbidity, baseline menopausal status, TNM stage, cancer treatment, or ER/PR status (p interactions >0.05). Regular and persistent exercise after cancer diagnosis, even at low-to-moderate intensity level, decreases the prevalence of MetS among long-term breast cancer survivors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The number of breast cancer survivors has continued to grow with advances in early diagnosis and cancer treatment [1–3]. With the improvement of survival rate, the impact of comorbidity on survival and quality of life among long-term breast cancer has becoming an important issue [4].
Metabolic syndrome (MetS) is characterized as a cluster of conditions including hyperglycemia, abdominal obesity, dyslipidemia, and high blood pressure, and is associated with cardiovascular diseases and death [5, 6]. Emerging evidence implicates MetS as a long-term risk factor for cancer, but also suggests that certain cancer therapies might increase risk of developing MetS among cancer survivors [7–9]. One recent meta-analyses of cross-sectional studies found that adult cancer survivors with hematologic malignancies were at an increased risk of MetS [10]. The issue for MetS and related risk factors among breast cancer survivors has attracted growing attention [8]. Anti-estrogen hormonal therapy may be associated with the development of MetS among breast cancer survivors. Use of aromatase inhibitors (AIs) agents in women with breast cancer can worsen lipid profiles, increase hypercholesterolemia, and increase risk of adverse cardiovascular outcomes [11]. Lifestyle changes after cancer diagnosis and treatment may also play a role in the development of MetS [12]. Previous studies have shown that high levels of exercise are inversely correlated with the prevalence of MetS in the general population [13–15]. However, whether exercise participation can reduce the risk of MetS among cancer survivors have been less studied. Exercise was found to associate with the development of MetS childhood cancer survivors [16]. However, data among breast cancer survivors are scant. We only found one previous report which shown that MetS was diagnosed in 54.8 % of overweight postmenopausal breast cancer survivors [17]. To our knowledge, no study has specifically evaluated the association between exercise and MetS among breast cancer survivors. As metabolic and hormonal parameters related to MetS may affect breast cancer prognosis [18–20] and MetS is associated with increased risk of CVD disease and mortality [21, 22], it is of particular importance to identify modifiable factors related to MetS among breast cancer survivors so that proper preventive measurements can be taken.
Using data from the Shanghai Breast Cancer Survival Study (SBCSS), a prospective cohort of female breast cancer survivors, we examined the prevalence of MetS approximately 5 years after cancer diagnosis and evaluated the association of exercise after diagnosis with the risk of MetS and its components.
Materials and methods
The study was approved by the institutional review boards of all participating institutions: the Shanghai Municipal Center for Disease Control and Prevention and Vanderbilt University. Written, informed consent was obtained from all study participants.
Study participants
Study participants were female breast cancer survivors enrolled in the SBCSS, a population-based prospective cohort study conducted in Shanghai, China. Details of the study design and methods have been previously described [23, 24]. In short, a total of 6,299 women diagnosed with breast cancer between March 2002 and April 2006 were identified from the Shanghai Cancer Registry, and 5,042 were enrolled (participation rate, 80.0 %) and completed baseline interviews at approximately 6 months after cancer diagnosis. The cohort has been followed up by in-person interviews at 18, 36, and 60 months after cancer diagnosis. The 60-month interview was completed for 3,640 patients out of 4,439 surviving patients (response rate, 82.0 %). A subset of women who completed the 60-month in-person interview participated in a physical health examination at a designated study clinic, which included assessment of MetS components (n = 1,696) and they were included in the current analysis. The MetS components tested include waist circumference (WC), blood pressure (BP), fasting plasma glucose (FBG), triglycerides (TG), and high-density lipoprotein (HDL-C).
Data collection
Structured questionnaires were used to collect data during in-person survey took place at approximately at 6, 18, 36, and 60 months after cancer diagnosis. The survey questionnaire at the 6-month post-diagnosis baseline interview covered socio-demographic characteristics, disease history, menstrual and reproductive history, diet, lifestyle (such as exercise, smoking), medication use, CAM use, as well as quality of life (QOL). Clinical information collected included TNM stage at diagnosis, estrogen receptor (ER) and progesterone receptor (PR) status, type of surgery, chemotherapy, radiation therapy, chemotherapy, and hormonal therapy at baseline. Medical charts were reviewed to verify clinical and treatment information. Anthropometric measurements of height, weight, and waist and hip circumference were measured at 6 and 60 months survey. Exercise was updated at each follow-up surveys (i.e., 18, 36, and 60 months post-diagnosis). Anthropometric measurements were taken according to a standard protocol. Body mass index (BMI) at baseline and the 60-month post-diagnosis survey were calculated. A Charlson comorbidity index was created for each woman based on a validated comorbidity scoring system [25] and the diagnostic codes from the International Classification of Diseases, Ninth Revision, Clinical Modification.
Exercise assessment
Using a validated exercise questionnaire [26], participants were asked whether they participated in exercise regularly (at least twice a week) at of each the 6, 18, 36, and 60-month interview. If the woman answered “Yes,” she was further asked to report up to 5 of the most common activities in which she participated. At the baseline, 6-month post-diagnosis interview, women reported activities that took place during the 6 months preceding the interview. At subsequent interviews, women reported activities since the last interview (i.e., for the preceding 12 or 18 or 24 months). No women reported participating in more than 4 types of exercise during the first 18 months after diagnosis, and only 4 cases of women reported participating in 5 types of exercise at the 36-month post-diagnosis interview, and 1 case reported participating in 5 types of exercise at 60-month post-diagnosis interview. Patients were asked how many hours per week they spent exercise (e.g., walking, jogging, and swimming). Given that exercise during the first 6-month post-diagnosis interview may be influenced by cancer treatments, a variable combining exercise participation between 6 and 60 months (18, 36, and 60-month interview) after diagnosis among breast cancer survivors was created as a cumulative level of exercise. According to the exercise recommendation “a half-hour of exercise every day” [27], all patients were classified into one of the following categories: no exercise 0 h per week, ≤3.5 h per week, and >3.5 h per week. We derived patterns of exercise participation according to information collected at the post-diagnosis surveys as follows: (1) “never participation” refers to those with no exercise participation reported at any survey; (2) “consistent participation” refers to participants who reported exercise participation all four relevant follow-up surveys; and (3) “non-consistent participation” refers to those who reported to have exercised in some but not all surveys. The two latter patterns were included in the “ever participation” category. A variable combining exercise participation over the entire 60 months after diagnosis was also created as a cumulative level of exercise.
Furthermore, each activity was assigned a metabolic equivalent (MET) score, based on the method proposed by Ainsworth [28]. The score for MET-hours per week for each activity was calculated from the hours per week the participant reported engaging in that activity multiplied by the assigned MET score. The MET score for individual activities was summed to derive a total exercise MET score.
MetS evaluation
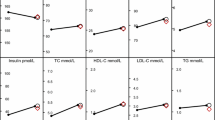
The following MetS components were assessed at the 60-month, post-diagnosis interview during a physical examination at the Health Physical Examination Center of the Shanghai Municipal Center for Disease Control and Prevention: anthropometric measurements (WC, height, weight); blood pressure; and clinical laboratory assessments, including FBG, lipids (total cholesterol (TC), TG, HDL-C, and low-density lipoprotein (LDL-C)). Blood pressure was measured using a sphygmomanometer. Abdominal circumference was evaluated at midway between the iliac crest and the last rib. Blood samples for fasting glucose, triglycerides, and cholesterol tests were obtained after overnight fasting.
Metabolic syndrome was defined using two approaches: the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATPIII) definition (modified in 2005) [27] and the International Diabetes Federation (IDF) definition (revised in 2006) [29]. According to the NCEP-ATPIII definition, participants who met at least three of the following five criteria were considered to have MetS: WC ≥ 88 cm; fasting blood glucose level ≥6.1 mmol/L; fasting TG level ≥1.7 mmol/L; fasting HDL-C <1.295 mmol/L; and blood pressure ≥130/85 mmHg. According to the 2006 IDF definition, the same five criteria were used, but the presence of central adiposity (WC ≥ 80 cm) as a required component to define MetS. The NCEP-ATPIII definition of MetS is the most widely used and clinically relevant guideline [30].
In this analyses of the association of exercise and MetS, patients who reported a diagnosis of diabetes mellitus at baseline interview were excluded (n = 80).
Statistical analysis
The primary outcome of this study was prevalence of MetS at approximately 5-years post-diagnosis. Analyses of variance (ANOVA) and χ2 tests were conducted to examine differences between women included in the present study and all women who completed the 60-month interview. Logistic regression model was used to evaluate the association of exercise participation during the 60 months post-diagnosis and the prevalence of MetS. Women reporting no exercise participation after breast cancer diagnosis served as the reference group. Odds ratios (ORs) and 95 % confidence intervals (CIs) were adjusted for age at diagnosis, education at baseline, BMI at baseline, menopausal status at baseline, TNM status, and Charlson comorbidity index at baseline. BMI was categorized as normal (BMI < 25 kg/m2), overweight (BMI ≥ 25 to <30 kg/m2), and obese (BMI ≥ 30 kg/m2). Analyses of the association of exercise and MetS were further stratified by BMI and WC at baseline, menopausal status at baseline, comorbidity at baseline, TNM stage, ER/PR status, and cancer treatment. Multiplicative interaction was tested by using the log-likelihood test in the logistic models by introducing interaction. Tests for trend were performed by entering the categorical variables as continuous parameters in the models. A p value of <0.05 was be used to define statistical significance. All tests were conducted by using SAS version 9.2 (SAS Institute, Cary, NC).
Results
Among the 1,696 study participants, the mean age at the 60-month post-diagnosis survey was 56.68 (SD = 7.79) and the mean months of follow-up after cancer diagnosis was 63.66 (range 59.04–87.89). The demographic and clinical features of the study population, and the comparison of these characteristics between women in the present study and women who completed the 60-month survey (n = 3,640) are presented in Table 1. Compared with women who completed the 60-month survey, those in the current study were younger, had higher education, were more likely to have received chemotherapy, and were less likely to be postmenopausal at study enrollment. Women in the present study also had a lower comorbidity index, BMI, and WC at the baseline survey, compared to all women who completed the 60-month interview. Regular participation in exercise was not significantly different between the study population and women who completed the 60-month interview.
At 6-month post-diagnosis survey, 65.92 % of women reported regular exercise participation. The corresponding percentages were 74.59, 74.82, and 66.75 % at 18, 36 and 60 months post-diagnosis, respectively. The major types of exercise in this population included walking (48.12 %), gentle gymnastics (15.74 %), body building using fitness equipment (6.53 %), and traditional Chinese exercises (5.72 %, including Tai Chi and Qigong) at baseline survey. Similar results were observed at 18, 36 and 60 months post-diagnosis among this study participants, but more participants were involved in the traditional Chinese exercises (20.43, 20.52, and 18.83 %, respectively).
The duration of exercise participation increased with time since diagnosis. Among women who reported exercise participation, the percent who spent longer than 3.5 h per week was 32.65, 58.18, 62.57, and 64.49 % at 6-, 18-, 36-, and 60-month survey, respectively. The mean duration of exercise participation was 3.11 h per week (median 8.87 MET-h/wk) at 6-month post-diagnosis survey and increased to 4.87 (median 16.00 MET-h/wk), 5.13 (median 18.00 MET-h/wk), and 5.18 h per week (median 18.10 MET-h/wk) at 18-, 36-, and 60-month post-diagnosis survey.
As shown in Table 2, according to NCEP-ATP III and IDF definitions, the prevalence of MetS among breast cancer survivors at 5 years post-diagnosis was 33.14 and 36.56 %, respectively. Older age at diagnosis (≥60 years) was associated with a higher prevalence of MetS. The prevalence of MetS using NCEP-ATP III criteria by BMI category was 22.27 % among normal/underweight participants, 51.43 % among overweight participants, and 80.56 % among obese participants. The prevalence of each MetS component was as follows: WC ≥ 88 cm (19.34 %), high triglycerides (42.81 %), high blood pressure (59.91 %), low HDL (36.73 %), and high blood glucose (31.60 %) (data not shown in tables).
Table 3 presents associations of cumulative exercise over the entire 60 months after diagnosis and between 6 and 60 months post-diagnosis with the prevalence of MetS among breast cancer survivors at 60 months post-diagnosis. According to the NCEP-ATP III definition, prevalence of MetS was significantly lower for survivors who reported exercise participation of at least 3.5 h/week (30 min/day) between 6 and 60 months post-diagnosis, compared to women who reported no exercise participation during this time (adjusted OR 0.69, 95 % CI 0.48–0.98, p for trend = 0.005). Consistent exercise participation reduced the risk of MetS (adjusted OR 0.70, 95 % CI 0.50–1.00, p for trend = 0.005). Similar results were found for cumulative exercise over the first 60 months after diagnosis, but the p for trend for duration of exercise was not statistically significant (p = 0.09).
Table 4 displays results for the association of cumulative exercise between 6 and 60 months post-diagnosis and each of the specific components of MetS, and the number of MetS components. We found that exercise was significantly associated with only one specific MetS component, i.e., abdominal obesity (WC ≥ 88 cm).
As Table 5 shows, associations of exercise with risk of MetS were not modified by baseline WC, BMI, menopausal status, Tamoxifen use, radiotherapy use (p for interactions >0.05 for all), although significant associations were only observed for breast cancer survivors using tamoxifen and those with BMI < 25. Vast majority of our study participants received chemotherapy (93.9 %) prevented a stratified analysis by this treatment, while the results suggested that a statistically significant inverse association was seen in that subgroup received chemotherapy. Similarly, no significant interactions were observed for associations of exercise and MetS by comorbidity, TNM stage, or ER/PR status (data not shown).
Discussion
In this longitudinal population-based cohort study of breast cancer survivors, we found that regular exercise at least 30 min a day and consistent exercise participation for approximately 5 years after diagnosis were significantly associated with reduced prevalence of MetS at 5-years post-diagnosis of breast cancer. This association varied little by WC, BMI, menopausal status, comorbidity, TNM stage, ER/PR status, and cancer treatment. Exercise was also associated with reduced WC at 5-years post-diagnosis.
Because cancer treatments may lead to lifestyle changes through physical complications or psychological stress, exercise participation of breast cancer patients receiving cancer treatments may be reduced [31, 32], and this was confirmed in the present study. Specifically, exercise participation was lowest within the first 6 months post-diagnosis, and after 6 months post-diagnosis, the median duration increased, which is consistent with exercise change patterns observed in previous studies [33, 34]. Due to the concern that exercise in the first 6 months post-diagnosis is confounded by cancer-related treatments, we focus on the discussion on results generated based on exercise participation during 6 and 60 months post-diagnosis.
The findings in the present study are consistent with previous studies conducted in the general population indicating that the regular physical activity is associated with reduces risk of MetS [35–37]. The musculoskeletal, endocrine, cardiovascular, immune, and neurological systems of the body are all influenced to some degree when a person participates in exercise [38]. A study of survivors of childhood cancer found that reduced exercise was involved in the development of metabolic syndrome [16] We identified only one study to date of the association of exercise and the risk of Mets among breast cancer survivors. This study of 29 cases showed that combination exercise training can improve metabolic syndrome parameters in postmenopausal breast cancer patients [39].
Weight gain is common among breast cancer survivors in Western countries [40] and this also has been confirmed in our study population [41]. The presence of visceral adipose tissue may directly lead to metabolic syndrome, because of its hyperlipolytic state and the contribution of excess free fatty acids to insulin resistance [5]. In our study, we found that exercise was associated with reduced WC at 5-years post-diagnosis. Similar results were reported by investigators using data from the National Health and Nutrition Examination Survey [42], which showed that increasing physical activity was negatively associated with adiposity among breast cancer survivors. An intervention study among African American breast cancer survivors reported that regular moderate exercise, such as walking, appears to improve BMI and anthropometric measurements [43]. These data suggest that the beneficial of exercise on MetS is likely to be mediated through the weight reduction and reduced central adiposity.
A working group of the American College of Sports Medicine published a major review and update on physical activity and cancer survivors in 2010 in MSSE [44]. There was consensus that exercise was safe and appropriate during and after cancer treatments and resulted in improvement in physical functioning and quality of life for cancer survivors. This review also indicated that the benefits for cancer survivors were sufficient for the recommendation to avoid inactivity following the 2008 Physical Activity Guidelines [45], which stated that physical activity can significantly reduce the risk of some cancers and benefit the quality of life for cancer survivors. The majority of women in our study participated in low-to-moderate levels of exercise, such as walking, and our results indicated that approximately 30 min of participant in low and moderate activities daily may achieve the same goal of reducing the risk of MetS among breast cancer survivors.
Our study has several strengths. To our knowledge, it is the first population-based, longitudinal study to prospectively evaluate the effect of post-diagnosis exercise on the prevalence of MetS among long-term breast cancer survivors. The population-based study design and the high response and follow-up rates largely minimized selection bias. Multiple exercise assessments were implemented, and the detailed exercise information was collected. This improved the exposure assessment. The data on socio-demographic, lifestyle, and medical factors, and anthropometrics collected using structured and/or validated questionnaires allowed a detailed adjustment for potential confounding factors and stratified analyses for evaluation of potential interactions.
Several limitations of this study should be mentioned. First, exercise information was self-reported, which can be subject to recall bias or over-reporting. However, our validation study indicated that the self-reported exercise questionnaire has high validity [26]. Second, our study included only one assessment of MetS, and MetS status at baseline was unknown. However, we had collected detailed information on disease history (including diabetes, hypertension, heart disease, and so on) at baseline. We excluded those cases with diabetes history at diagnosis when assessing the association between post-diagnosis exercise and the prevalence of MetS. We also adjusted for the baseline comorbidity index in our analysis. Nevertheless, because our study design did not allow identification of the onset of MetS, temporality between exercise participation and development of MetS cannot be determined. Lastly, the participants of current study differ from the entire cohort in several demographic and clinical characteristics which may influence the generalizability of the study results.
In conclusion, our results indicate that MetS is highly prevalent in long-term overweight breast cancer survivors, and regular exercise at least 30 min a day may decrease the risk of MetS. Given the negative health consequences of MetS, further studies are warranted to evaluate the strategies for screening, monitoring, and treating MetS, and development of exercise programs for breast cancer survivors. Addressing the healthy lifestyle practices to reduce the risk of MetS and other comorbidities should be encouraged, and it will reduce the risk for non-cancer-related mortality among breast cancer survivors.
References
Ferlay J, Shin HR, Bray F, Forman D (2010) GLOBOCAN 2008 v1.2. Cancer Incidence and Mortality Worldwide, International Agency for Research on Cancer, Lyon
Siegel R, DeSantis C, Virgo K et al (2012) Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin 62:220–241
Parkin DM, Fernandez LM (2006) Use of statistics to assess the global burden of breast cancer. Breast J 12(Suppl 1):S70–S80
Maurea N, Coppola C, Ragone G et al. (2010) Women survive breast cancer but fall victim to heart failure: the shadows and lights of targeted therapy. J Cardiovasc Med (Hagerstown)
de Haas EC, Oosting SF, Lefrandt JD, Wolffenbuttel BH, Sleijfer DT, Gietema JA (2010) The metabolic syndrome in cancer survivors. Lancet Oncol 11:193–203
Denke MA, Pasternak RC (2001) Defining and treating the metabolic syndrome: a primer from the adult treatment panel III. Curr Treat Options Cardiovasc Med 3:251–253
Nuver J, Smit AJ, Postma A, Sleijfer DT, Gietema JA (2002) The metabolic syndrome in long-term cancer survivors, an important target for secondary preventive measures. Cancer Treat Rev 28:195–214
Redig AJ, Munshi HG (2010) Care of the cancer survivor: metabolic syndrome after hormone-modifying therapy. Am J Med 123(87):e1–e6
Cowey S, Hardy RW (2006) The metabolic syndrome: a high-risk state for cancer? Am J Pathol 169:1505–1522
Jung HS, Myung SK, Kim BS, Seo HG (2012) Metabolic syndrome in adult cancer survivors: a meta-analysis. Diabetes Res Clin Pract 95:275–282
Redig AJ, Munshi HG (2010) Metabolic syndrome after hormone-modifying therapy: risks associated with antineoplastic therapy. Oncology (Williston Park) 24:839–844
Patterson RE, Flatt SW, Saquib N et al (2010) Medical comorbidities predict mortality in women with a history of early stage breast cancer. Breast Cancer Res Treat 122:859–865
Dai DF, Hwang JJ, Chen CL et al (2010) Effect of physical activity on the prevalence of metabolic syndrome and left ventricular hypertrophy in apparently healthy adults. J Formos Med Assoc 109:716–724
Nguyen TH, Tang HK, Kelly P, van der Ploeg HP, Dibley MJ (2010) Association between physical activity and metabolic syndrome: a cross sectional survey in adolescents in Ho Chi Minh City, Vietnam. BMC Public Health 10:141
Harralson TL, Uplinger N, McLaughlin M (2010) Increasing physical activity: a step toward controlling metabolic syndrome. Diabetes Educ 36:70–71
van Waas M, Neggers SJ, van der Lelij AJ, Pieters R, van den Heuvel-Eibrink MM (2010) The metabolic syndrome in adult survivors of childhood cancer, a review. J Pediatr Hematol Oncol 32:171–179
Thomson CA, Thompson PA, Wright-Bea J, Nardi E, Frey GR, Stopeck A (2009) Metabolic syndrome and elevated C-reactive protein in breast cancer survivors on adjuvant hormone therapy. J Womens Health (Larchmt) 18:2041–2047
Berrino F, Pasanisi P, Bellati C et al (2005) Serum testosterone levels and breast cancer recurrence. Int J Cancer 113:499–502
Goodwin PJ, Ennis M, Pritchard KI et al (2002) Fasting insulin and outcome in early-stage breast cancer: results of a prospective cohort study. J Clin Oncol 20:42–51
Pasanisi P, Berrino F, De Petris M, Venturelli E, Mastroianni A, Panico S (2006) Metabolic syndrome as a prognostic factor for breast cancer recurrences. Int J Cancer 119:236–238
Grundy SM (2006) Metabolic syndrome: connecting and reconciling cardiovascular and diabetes worlds. J Am Coll Cardiol 47:1093–1100
Mottillo S, Filion KB, Genest J et al (2010) The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 56:1113–1132
Shu XO, Zheng Y, Cai H et al (2009) Soy food intake and breast cancer survival. JAMA 302:2437–2443
Epplein M, Zheng Y, Zheng W et al (2011) Quality of life after breast cancer diagnosis and survival. J Clin Oncol 29:406–412
Grunau GL, Sheps S, Goldner EM, Ratner PA (2006) Specific comorbidity risk adjustment was a better predictor of 5-year acute myocardial infarction mortality than general methods. J Clin Epidemiol 59:274–280
Matthews CE, Shu XO, Yang G et al (2003) Reproducibility and validity of the Shanghai Women’s Health Study physical activity questionnaire. Am J Epidemiol 158:1114–1122
Grundy SM, Cleeman JI, Daniels SR et al (2005) Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 112:2735–2752
Ainsworth BE, Haskell WL, Whitt MC et al (2000) Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 32:S498–S504
Alberti KG, Zimmet P, Shaw J (2005) The metabolic syndrome—a new worldwide definition. Lancet 366:1059–1062
Alberti KG, Eckel RH, Grundy SM et al (2009) Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 120:1640–1645
Irwin ML, Crumley D, McTiernan A et al (2003) Physical activity levels before and after a diagnosis of breast carcinoma: the Health, Eating, Activity, and Lifestyle (HEAL) study. Cancer 97:1746–1757
Beasley JM, Kwan ML, Chen WY et al (2012) Meeting the physical activity guidelines and survival after breast cancer: findings from the after breast cancer pooling project. Breast Cancer Res Treat 131:637–643
Andrykowski MA, Beacham AO, Jacobsen PB (2007) Prospective, longitudinal study of leisure-time exercise in women with early-stage breast cancer. Cancer Epidemiol Biomarkers Prev 16:430–438
Littman AJ, Tang MT, Rossing MA (2010) Longitudinal study of recreational physical activity in breast cancer survivors. J Cancer Surviv 4:119–127
Golbidi S, Mesdaghinia A, Laher I (2012) Exercise in the metabolic syndrome. Oxid Med Cell Longev 2012:349710
Misra KB, Endemann SW, Ayer M (2005) Leisure time physical activity and metabolic syndrome in Asian Indian immigrants residing in northern California. Ethnicity Dis 15:627–634
Lakka TA, Laaksonen DE (2007) Physical activity in prevention and treatment of the metabolic syndrome. Appl Physiol Nutr Metab 32:76–88
McTiernan A (2004) Physical activity after cancer: physiologic outcomes. Cancer Invest 22:68–81
Nuri R, Kordi MR, Moghaddasi M et al (2012) Effect of combination exercise training on metabolic syndrome parameters in postmenopausal women with breast cancer. J Cancer Res Ther 8:238–242
Vance V, Mourtzakis M, McCargar L, Hanning R (2011) Weight gain in breast cancer survivors: prevalence, pattern and health consequences. Obes Rev 12:282–294
Gu K, Chen X, Zheng Y et al (2010) Weight change patterns among breast cancer survivors: results from the Shanghai Breast Cancer Survival Study. Cancer Causes Control 21:621–629
Lynch BM, Dunstan DW, Healy GN, Winkler E, Eakin E, Owen N (2010) Objectively measured physical activity and sedentary time of breast cancer survivors, and associations with adiposity: findings from NHANES (2003–2006). Cancer Causes Control 21:283–288
Wilson DB, Porter JS, Parker G, Kilpatrick J (2005) Anthropometric changes using a walking intervention in African American breast cancer survivors: a pilot study. Prev Chronic Dis 2:A16
Schmitz KH, Courneya KS, Matthews C et al (2010) American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 42:1409–1426
US Department of Health and Human Services (2008) Physical activity guidelines for Americans. Okla Nurse 53:25
Acknowledgments
The authors thank Dr. Fan Jin for her support in study implementation and the participants and staff members of the SBCSS for making this study possible. The authors also thank Ms. Bethanie Rammer for their assistance in manuscript preparation. The SBCSS was supported by grants from the Department of Defense Breast Cancer Research Program (DAMD 17-02-1-0607 to X.-O. Shu), the National Cancer Institute (R01 CA118229 to X.-O. Shu) and Shanghai Health Bureau (12GWZX0101 to W. Lu). Pingping Bao was awarded the Fogarty International Clinical Research Fellow (FICRS-F 2011–2012) and supported by the grant (5 R24 TW007988) from National Institutes of Health, Fogarty International Center through Vanderbilt University. The contents of this paper are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health, Fogarty International Center, and Vanderbilt University.
Conflict of interest
The authors declare they have no conflict interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bao, PP., Zheng, Y., Nechuta, S. et al. Exercise after diagnosis and metabolic syndrome among breast cancer survivors: a report from the Shanghai Breast Cancer Survival Study. Cancer Causes Control 24, 1747–1756 (2013). https://doi.org/10.1007/s10552-013-0252-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-013-0252-7