
Abstract
Background
Patients with breast or prostate cancer diagnosed during the summer season have been observed to have better survival. The extent to which this is due to biological and/or health care system related factors is unclear.
Methods
Using the Swedish Cancer Register and clinical databases, we analyzed overall survival by month of diagnosis among the incident cases of breast (n = 89,630) cancer and prostate (n = 72,375) cancer diagnosed from 1960 to 2004. We retrieved data on tumor stage from 1976 for breast cancer and 1997 for prostate cancer. Cox proportional hazards models were used to calculate relative risk of survival by the season of diagnosis.
Results
There was a higher hazard ratio of death in men and women diagnosed with cancer in the summer with a relative hazard of 1.20 (95% confidence interval 1.15–1.25) for July for prostate cancer and 1.14 (95% confidence interval 1.09–1.19) for August for breast cancer when compared to being diagnosed in January. This difference coincided with a lower mean number of cases diagnosed per day, and a higher proportion of advanced cases diagnosed in the summer. This pattern of presentation was stronger in the later years.
Conclusion
The difference in stage distribution explains the seasonal variation in prognosis seen in this study. The variation may be because of structure of the health care system and a strong tradition of vacationing from mid June to mid August. Thus, the health care infrastructure and the late presentation of symptomatic disease may influence cancer survival studied by season of diagnosis substantially.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The influence of season of diagnosis on prognosis of different malignancies has been recently explored [1–7]. In general, a better prognosis was found for cancers of the breast, prostate, and colon following diagnosis or treatment initiation in the summer or fall. Increased levels of vitamin D during a period of increased sunlight exposure at the time of diagnosis have been hypothesized to be because of possible underlying cause of the seasonal effect [2, 4–7]. Theoretically, this explanation is attractive based on data relating vitamin D to decreased cancer risk in epidemiological and experimental studies [8–10]. However, there are also studies that report seasonal patterns of cancer survival that are not consistent with the hypothesis that prognosis is best following seasons with high sun exposure [11–14]. An alternative hypothesis to the biological—or a possible confounder that makes it difficult to study a biological mechanism—is that the variations in survival with season of diagnosis or treatment are associated with infrastructure of health care and management issues [12, 13]. During typical vacation seasons, most industrialized countries in the western world have lower staffing, less experienced staff, and also a less specialized health care. Training of attendant staff and organization of care influence cancer outcomes [15, 16]. During the summer month vacations, patients themselves may be less willing to make appointments for routine primary care and screening or low level symptoms.
We undertook a population-based study within two health care regions in Sweden to study the association between season of diagnosis and prognosis among women diagnosed with breast (n = 89,630) cancer and men diagnosed with prostate (n = 72,375) cancer. The Swedish results relating to season are particularly interesting to explore because of the long standing and strong tradition among a large majority of Swedes to take vacation from the last week in June until the first week of August.
Subjects and methods
The study population for the current investigation includes all residents in two health care regions in Sweden, the Stockholm–Gotland and Uppsala–Örebro health care regions, during 1960–2004. We took advantage of existing population-based databases: the Swedish Cancer Register, clinical databases for the two health care regions, the Swedish Population Register. All residents in Sweden were assigned an individually unique national registration number which allows linkage between the registry databases.
The Swedish cancer register
Information on incident of breast and prostate cancer cases in the regions came from the Swedish Cancer Register, established in 1958. All health care providers are by law mandated to report new incident cases of cancer based on laboratory and/or on clinical findings. The completeness has been estimated to be 98% for breast cancer and 94% for urological tumors [17].
The national cancer register is compiled from six regional registers, including those from the Stockholm–Gotland and Uppsala–Örebro regions. In the Swedish Cancer Registry, the date of diagnosis is set as the earliest date the cancer registry received notification of the cancer in question. For example, if a first diagnosis by cytology is verified later by a surgical specimen, the date of the first notification to the registry is kept as the date of diagnosis, but the full histopathological report is recorded as the final confirmation of diagnosis.
The registry included 89,630 incident breast cancer cases among women and 72,375 incident prostate cancer among men. Men and women with a cancer diagnosis made first at autopsy were not included.
Clinical databases
Because no information on stage was recorded in the Swedish Cancer Register prior to 2005, we cross-linked the information from the Register with clinical databases for breast and prostate cancer maintained at the Regional Oncologic Centers. The clinical databases are kept for purposes of quality assurance and clinical research and to record tumor characteristics, tumor stage, and treatment data. They are continuously updated against the Swedish Cancer Registry data for completeness of both registers. The breast cancer clinical database has been in operation since 1976 in the Stockholm–Gotland health care region and since 1992 in the Uppsala–Örebro region. The Stockholm-Gotland breast cancer register has a coverage of 95% and the Swedish Cancer Register and Uppsala–Örebro of 98%. The databases for prostate cancer have been in operation, in Stockholm, since 1998 and since 1997 in the Uppsala–Örebro Health Care Region, with a coverage of 90% and 99%, respectively.
In the clinical database for prostate cancer, patients were classified as having distant metastatic disease if bone scintigram was positive or the PSA-value at diagnosis was over 100 μg/l [18]. In the clinical data for breast cancer, we defined stage II and/or more advanced as a maximum tumor size of more than 20 mm and/or presence of metastatic lymph nodes and/or presence of a T4 tumor (UICC 1966) and/or of distant metastases at diagnosis.
The patients were followed through a linkage to the Population Register, which is continuously updated for all Swedish citizens’ vital status. If a person emigrates, the registry is notified and the record can thus be censored from further follow-up.
Diagnostic and treatment facilities
A population-based mammography screening program began in the late 1980s in the two health care regions [19]. PSA testing became more widespread in Sweden after 1996. Virtually all women with breast cancer are treated within the tax financed public health care system in Sweden. The same is true for prostate cancer patients undergoing radical surgery or radiotherapy, or being treated for advanced disease. However, especially in the Stockholm area, prostate cancer patients under active monitoring without radical treatment often see a private practitioner.
Statistical methods
Cox proportional hazard models were used to study the effect of month of diagnosis on overall survival. Likelihood ratio tests were used to investigate appearance of monthly variation in survival within time periods. Follow-up time was calculated from date of cancer diagnosis to death or censored at date of emigration from Sweden or end of follow-up (31 December 2005). We conducted analyses for each of six different time periods, comparing risk of death to cases diagnosed in the month of January. We used the Chi-square test to test the significance of difference in the mean number of cases diagnosed per month in each time period. All statistics and graphical illustrations are performed using the statistical program package R [20].
The management for both diagnoses has varied substantially over the time period studied, especially regarding screening practices. Analyses were therefore stratified on diagnosis and time period. Both our a priori hypotheses regarding the association between month of diagnosis and prognosis imply that stage of disease is an intervening variable rather than a confounder. Stage was therefore not included in models, but incidence of early and advanced stage disease over the year in different time periods was calculated. One set of the analyses included age at diagnosis, but the results were virtually the same as in those without age adjustment and results of the crude analyses are therefore shown. All the analyses were first done by health care region. However, because the pattern was virtually identical in the two regions, only the summarized data are shown.
To exclude that the seasonal variation only involves deaths from causes other than cancer, we used relative survival in one set of analyses. Excess mortality was calculated as the difference between the observed number of deaths and the expected number of deaths during the first five years from diagnosis. The expected number was calculated using the age, year, and sex specific death incidences in the general Swedish population. Finally, a model including only patients with advanced disease in the subset with stage information was done to investigate whether a delay also for patients with more advanced tumors carried over in a worse prognosis.
Results
Table 1 shows the number of incident cases of breast and prostate cancer by age, date of diagnosis, and duration of follow-up. The number of deaths by each cancer site is also shown. The analyses are based on a total of 834,645 person-years of follow-up for breast and 367,319 person-years for prostate cancer.
Relative risk of death by month of diagnosis
First, we estimated the relative risk of death by month of diagnosis, with January as the reference for every five-year period (Fig. 1). Already from 1960 and onward, we found a tendency for a higher hazard ratio of deaths among patients diagnosed in the summer, with a peak in July for prostate cancer, with a 10–24% higher hazard in the different time periods corresponding to an overall relative hazard of 1.20 (95% confidence interval 1.15–1.25) from 1960 to 2004. For breast cancer, the most marked peak appeared in August with a 5–17% higher hazard and an estimate of 1.14 (95% confidence interval 1.09–1.19) for the whole study period. The seasonal variation in prognosis became more pronounced in later years of observation. For prostate cancer, the seasonal variation in diagnosis did not differ in a statistically significant way 1960–1969 or 1970–1979, but did so (p < 0.05) in all later periods. During 1990–1999 and 2000–2004, the relative hazard was 1.25 (1.16–1.36) and 1.17 (1.00–1.37), respectively, comparing diagnosis from July to January. Also for breast cancer, the variation in prognosis became more pronounced after 1979 (p < 0.01 for a difference over the months in each following period). During 1990–1999 and 2000–2004, two periods reflecting modern screening and management practices, the relative hazard with 95% confidence interval was 1.12 (1.01–1.23) and 1.15 (0.95–1.40), respectively, comparing diagnosis from August to January. During the period of analyses we observed an overall improvement in prognosis for both cancers, yet with the same pattern of association between month of diagnosis and prognosis over the whole study period (data not shown).

Relative risk of death by month of diagnosis, January every year, as the reference by five/ten-year periods
We repeated the analyses with relative survival as endpoint and found the same pattern with a relative excess mortality in July varying between 1.2 and 1.5 for prostate cancer and in August between 1.04 and 1.3 for breast cancer for the different time periods. For prostate cancer the contrast was biggest in 1995–1999 and for breast cancer in 1980–1989.
Number of cases diagnosed per month
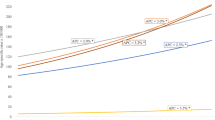
To explore further the variation in survival, by season of diagnosis, we estimated the mean number of cases diagnosed per day in a given month, by a five-year calendar period from 1960 and onward (Fig. 2). For prostate cancer, a seasonal variation in number of cases per month started to appear around 1975 and became gradually more pronounced over time (p < 0.001 within each time period), with the lowest number of cases diagnosed in July, but also with some decrease in December and January. For breast cancer the same pattern was evident, but the seasonal variation became more prominent in the mid 1970s (p < 0.001 throughout all periods). Furthermore, a pattern qualitatively similar to that found in the summer was seen also for December and January.

Mean number of cases diagnosed per month per time period for prostate and breast cancer
Incidence and proportion of cases with advanced stage cancer by month of diagnosis
We used the clinical databases in the two health care regions to estimate the proportion of prostate cancer patients diagnosed with distant metastases at the time of presentation (Fig. 3). From 1999 and onward, this proportion was consistently higher in the summer time. Likewise, among women with breast cancer, the proportion with stage II or with more advanced disease, peaked during the summer months (Fig. 3).

Proportion of prostate cancers diagnosed with metastatic disease (M1 of PSA > 100) and breast cancers diagnosed with stage II (UICC stage) or more advanced disease
Furthermore, we estimated the crude incidence rate per 100,000 men diagnosed with metastatic prostate cancer and women diagnosed with stage II or more advanced breast cancer over the year. This analysis was confined to the later time periods when stage information was available (Table 2). The incidence rate of advanced disease had less seasonal variation than that of early stage disease (Table 2), if anything, the rate of advanced disease was lower during summer, to become slightly higher immediately after. To investigate if this indicated a more severe delay also for women with stage II or more advanced breast cancer and men with metastatic prostate cancer, a survival analysis of these patient strata by month of diagnosis with January as a reference was carried out. For breast cancer the relative hazards varied between 0.86 (February) and 1.0 (July). Globally, the months were more different from each other than expected by chance (p = 0.04), but no month stood out as statistically significantly different from January on its own. For prostate cancer the estimates varied between 0.88 (December) and 1.05 (July). The estimates for the months did not differ from each other in a statistically significant way globally (p = 0.09) or individually. There was not a consistent seasonal pattern for neither of the diagnoses.
Discussion
In contrast to several other investigators [1–7], we found a worse survival for patients diagnosed with breast or prostate cancer in the summer compared with other periods of the year. The association between month of diagnosis and prognostic outlook became continuously stronger with calendar time. Supporting the time trends, the number of persons diagnosed with breast or prostate cancer in the summer relative to the other months also decreased in later time periods. Beginning in the mid 1990s, when we had stage information, the stage distribution became less favorable in the summer relative to the other months. This difference appears to be due not to so much to a shift in incidence of cases diagnosed with more advanced disease over the seasons as to the relatively fewer diagnoses of early stage cases, and therefore the total number of cases, so that the proportion of those diagnosed with advanced disease became higher in the summer.
We utilized population-based registers with nearly complete coverage of the population. The follow-up started at the earliest notification to the cancer registry of the diagnosis, so the calendar time of starting treatment may have been later, and for patients with prostate cancers, considerably later. The clinical databases have been repeatedly utilized for research (www.roc.se/publ-ref/publ_brost.asp, www.roc.se/publ_ref/publ_prostata.asp) and the data sets have thus been quality assured and cleaned on several occasions. We studied overall survival as opposed to cancer-specific survival. The hypothesis about Vitamin D as a causal agent theoretically involves deaths due to many causes as suggested by a recent meta-analysis [21]. Likewise, the alternative hypothesis about effects of quality in care and/or self referral patterns also involves deaths from other causes. Our results were not sensitive to the age distribution. If the assumption is that we address a cancer specific phenomenon, our results would rather err on the conservative side, diluting the estimates. This hypothesis was also corroborated by our analyses of relative excess mortality, which if anything showed stronger corrrelations than the overall survival pattern. A possible explanation for the seasonal variation in number of cases could be less well functioning cancer registration during the summer months. However, the high overall coverage [17] makes this a less likely explanation for the rather dramatic changes in reports and it is also difficult to accommodate that a less good reporting would pertain nearly only to patients diagnosed with early disease.
Our findings are in line with common medical practice in Sweden, where provision of most elective routine procedures in health care is substantially reduced for approximately six weeks starting in late June. For example, mammography screening does not take place during the summer months and accessibility to health care diminishes because of vacation patterns. As a corollary, people are less prone to seek medical consultations for minor symptoms or for advice on screening during vacation and may wait until symptoms develop. The differences in survival across the season of diagnosis have become greater during the later years, with the largest impact from 2000 to 2004. These time trends are in line with changing screening practices. Mammography screening for breast cancer began in the late 1980s, whereas PSA-testing for prostate cancer—with no organized program—became increasingly widespread from the mid 1990s.The absolute rate of cases diagnosed in advanced stages is nearly constant over the year, whereas the number of patients with early stage prostate or breast cancer is strongly increased in the spring and fall.
The small shift toward a lower rate of advanced cancer during the summer and an increase after, could mean that also some patients with more advanced disease, but less alarming symptoms wait until after summer to seek advice. We could not substantiate that such a delay carried over in a markedly worse survival for those diagnosed in a more advanced stage in the summer. The similar survival prospects for those with advanced cancer over the year also contradict that the treatment for a patient once diagnosed would be of substantial less quality during the summer time. However, to more firmly exclude a seasonal and clinically relevant shift in prognosis for subsets of those in the most advanced tumor stages, a more detailed stage and treatment information in combination with individual data on symptom duration would be needed.
Our study does not address the hypothesis of vitamin D as potentially beneficial for cancer [9] or that improvement in vitamin D intake can lower overall mortality [21]. Our data imply in line with the two Finnish studies [12, 13] that the health care system related factors may significantly influence the association between season of diagnosis and prognosis in cancer. Thus, these factors may confound season of diagnosis as an indicator for vitamin D exposure in a prognostic study. The great majority of studies on season of diagnosis and prognosis have so far only allowed ecological inferences for any sort of causal agent and hence they have had little possibility to control for confounding. The time of diagnosis is determined by a large range of factors that are not directly driven by tumor biology such as screening activity, screening participation, location of the tumor (influencing when it becomes palpable or otherwise symptomatic), individual response to symptoms, and availability of health care. Some of these behavioural factors may also be related to lifestyle, which may also include exposure to vitamin D and/or other possible modifiers of cancer prognosis.
It is difficult to compare studies that take date of diagnosis as a departure [1, 4, 7] with those which use date of treatment [5, 11]. Our data indicate that even for breast cancer, with a short time interval between diagnosis and treatment, using day of treatment initiation would skew the baseline date for a survival analysis about one month forward. Thus, two studies, both showing the best result with July as the indicator for exposure of either an environmental factor or circumstances related to management, may have different interpretations if date of diagnosis is used in one study and date of treatment in the other. Studies that group months into seasons as spring, summer, autumn, and winter may overlook the pattern found in our study, and different definitions of the seasons may yield different results.
We interpret the effects seen in our study as results of selection: Screened patients are “removed” from the vacation months since screening activity is low and there are no symptoms to prompt a medical consultation. Swedish patients only seek medical advice during vacation time when symptoms prevail. Patients with mild symptoms may also postpone a consultation until after vacation. Our study cannot directly address if extending screening to the vacation months or more readily available health care also during normal vacation times would improve the situation for patients with advanced disease. However, two important public health issues are illuminated by our results. Access and organization of health care will impact survival substantially—bearing in mind that some of the improvement in survival following screening will be due to added lead time. Furthermore, the results underline that it is unfavorable to postpone a medical consultation until more alarming symptoms occur. Finally, the results may prompt other investigators to take health care system factors into account in studies of season of diagnosis and prognosis in cancer.
References
Lim HS, Roychoudhuri R, Peto J, Schwartz G, Baade P, Möller H (2006) Cancer survival is dependent on season of diagnosis and sunlight exposure. Int J Cancer 119:1530–1536. doi:10.1002/ijc.22052
Porojnicu A, Robsahm TE, Berg JP, Moan J (2007) Season of diagnosis is a predictor of cancer survival. Sun-induced vitamin D may be involved: a possible role of sun-induced vitamin D. J Steroid Biochem Mol Biol 103:675–678. doi:10.1016/j.jsbmb.2006.12.031
Porojnicu AC, Lagunova Z, Robsahm TE, Berg JP, Dahlback A, Moan J (2007) Changes in risk of death from breast cancer with season and latitude: sun exposure and breast cancer survival in Norway. Breast Cancer Res Treat 102:323–38 (Epub 2006 Sept 21). doi:10.1007/s10549-006-9331-8
Robsahm TE, Tretli S, Dahlback A, Moan J (2004) Vitamin D3 from sunlight may improve the prognosis of breast-, colon- and prostate cancer (Norway). Cancer Causes Control 15:149–158. doi:10.1023/B:CACO.0000019494.34403.09
Zhou W, Suk R, Liu G, Park S, Neuberg DS, Wain JC, Lynch TJ, Giovannucci E, Christiani DC (2005) Vitamin D is associated with improved survival in early-stage non-small cell lung cancer patients. Cancer Epidemiol Biomarkers Prev 14:2303–2309. doi:10.1158/1055-9965.EPI-05-0335
Moan J, Porojnicu AC, Robsahm TE, Dahlback A, Juzeniene A, Tretli S, Grant W (2005) Solar radiation, vitamin D and survival rate of colon cancer in Norway. J Photochem Photobiol B 78:189–193. doi:10.1016/j.jphotobiol.2004.11.004
Porojnicu AC, Robsahm TE, Ree AH, Moan J (2005) Season of diagnosis is a prognostic factor in Hodgkin’s lymphoma: a possible role of sun-induced vitamin D. Br J Cancer 93:571–574. doi:10.1038/sj.bjc.6602722
Schwartz GG, Skinner HG (2007) Vitamin D status and cancer: new insights. Curr Opin Clin Nutr Metab Care 10:6–11
Giovannucci E (2005) The epidemiology of vitamin D and cancer incidence and mortality: a review (United States). Cancer Causes Control 16:83–95. doi:10.1007/s10552-004-1661-4
Bouillon R, Eelen G, Verlinden L, Mathieu C, Carmeliet G, Verstuyf A (2006) Vitamin D and cancer. J Steroid Biochem Mol Biol 102:156–162. doi:10.1016/j.jsbmb.2006.09.014
Meltzer AA, Annegers JF (1995) Survival time and season-of-treatment initiation in children with acute lymphoblastic leukaemia. Leuk Lymphoma 17:443–447. doi:10.3109/10428199509056855
Sankila R, Joensuu H, Pukkala E, Toikkanen S (1993) Does the month of diagnosis affect survival of cancer patients? Br J Cancer 67:838–841
Aaltomaa S, Lipponen P, Eskelinen M (1992) Demographic prognostic factors in breast cancer. Acta Oncol 31:635–640. doi:10.3109/02841869209083845
Porojnicu AC, Robsahm TE, Dahlback A, Berg JP, Christiani D, Bruland OS, Moan J (2007) Seasonal and geographical variations in lung cancer prognosis in Norway: does Vitamin D from the sun play a role? Lung Cancer 55:263–270. doi:10.1016/j.lungcan.2006.11.013
Hebert-Croteau N, Brisson J, Pineault R (2000) Review of organizational factors related to care offered to women with breast cancer. Epidemiol Rev 22:228–238
Purushotham AD, Pain SJ, Miles D, Hamett A (2001) Variations in treatment and survival in breast cancer. Lancet Oncol 2:719–725. doi:10.1016/S1470-2045(01)00585-X
Barlow L, Westergren K, Holmberg L, Talbäck M (2008) The completeness of the Swedish Cancer Register—a sample survey for year 1998. Acta Oncol. doi:10.1080/02841860802247664
Sandblom G, Holmberg L, Damber JE, Hugosson J, Johansson JE, Lundgren R, Mattsson E, Varenhorst E (2002) Prostate-specific antigen for prostate cancer staging in a population-based register. Scand J Urol Nephrol 36:99–105. doi:10.1080/003655902753679373
Swedish Organised Service Screening Evaluation Group (2006) Reduction in breast cancer mortality from organized service screening with mammography: 1. Further confirmation with extended data. Cancer Epidemiol Biomarkers Prev 5:45–51. doi:10.1158/1055-9965.EPI-05-0349
Ihaka R, Gentleman RR (1996) A language for data analysis and graphics. J Comput Graph Stat 5:299–314. doi:10.2307/1390807
Autier P, Gandini S (2007) Vitamin D supplementation and total mortality. A meta-analysis of randomized controlled trials. Arch Intern Med 167:1730–1737. doi:10.1001/archinte.167.16.1730
Acknowledgment
The study was supported by the Swedish Cancer Society. The clinical databases were collected and quality assured by the regional working collaborative groups for breast and prostate cancer in the Stockholm–Gotland and the Uppsala–Örebro health care regions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Holmberg, L., Adolfsson, J., Mucci, L. et al. Season of diagnosis and prognosis in breast and prostate cancer. Cancer Causes Control 20, 663–670 (2009). https://doi.org/10.1007/s10552-008-9279-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-008-9279-6