
Abstract
Purpose
We investigated the association between breast cancer incidence and obesity among Asian women.
Methods
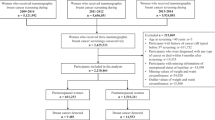
We used data from 30,109 women who had undergone medical check-ups and opportunistic breast cancer screening at least twice at the St. Luke’s International Hospital Affiliated Clinic, Center for Preventive Medicine, between April 1, 2005 and March 31, 2014. This study evaluated obesity through body mass index (BMI) at age 18–20 years (BMI18–20y), BMI at research entry (entry BMI), change of BMI from age 18–20 to research entry (ΔBMI), abdominal circumference at research entry (AC), and HbA1c [N] at research entry (HbA1c). We used a multivariate Cox proportional hazard model to evaluate hazard ratios (HRs) and 95% confidence intervals (95% CIs).
Results
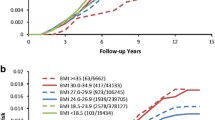
Of the 30,109 women, 325 were initially diagnosed with breast cancer over 131,657 person-years. Postmenopausal women whose BMI increased ≥+5.0 were significantly more likely to develop breast cancer (HR 1.902, 95% CI 1.202–3.009) than were the stable BMI group (ΔBMI: −2.5 to +2.5). Postmenopausal women with AC ≥90 cm were significantly likelier to develop breast cancer than were those with AC <70 cm (HR 2.500, 95% CI 1.091–5.730). Among postmenopausal women whose BMI18–20y was ≥20, those with high (≥6.5) HbA1c were more likely to develop breast cancer than those with low (<5.5) HbA1c (HR 3.325, 95% CI 1.307–8.460).
Conclusions
Breast cancer incidence and obesity are positively associated in postmenopausal Asian women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Breast cancer has a high incidence among women world-wide [1,2,3,4]. Particularly in Japan, the morbidity and mortality of breast cancer has increased for a few decades [5]. Because breast cancer had been less common in Japan than Western countries, Westernized life styles (notably, diet and the consumption of much red meat and fat) are considered to be possible causes for this increased morbidity [6,7,8,9,10,11,12,13]. To prevent increased mortality, Japan began population-based mammography screening about 17 years ago. However, we cannot clearly show decreased breast cancer mortality in Japan yet [5].
Whereas associations among obesity, metabolic factors, weight gain, and breast cancer are widely reported in Western populations [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30], Asian women tend to have lower body mass index (BMI) than Western women, and associations between breast cancer and BMI in Asian women have not been widely studied. We therefore investigated effects of obesity on breast cancer development in Asian women.
Methods
Study population
We used the data from women who had each undergone at least two medical check-ups which included opportunistic breast cancer screening (ultrasonography, mammography or both) at St. Luke’s International Hospital Affiliated Clinic, Center for Preventive Medicine between April 1, 2005 and March 31, 2014. We excluded women with histories of breast cancer, or who were diagnosed with breast cancer at their first examinations during this period. We also used written questionnaire data and measurements taken at subjects’ first visits during this period as data at research entry.
Definitions
We evaluated obesity through body mass index (BMI) at age 18–20 years (BMI18–20y), BMI at research entry (entry BMI), change of BMI from age 18–20 to research entry (ΔBMI), abdominal circumference at research entry (AC), and HbA1c [N] at research entry (HbA1c).
Height and body weight at entry were defined as their measured values at the first medical check-up during the study period.
In calculating BMI18–20y, we assumed that height does not change after adulthood. We calculated BMI18–20y using height at research entry and the weight answered to the question “Body weight at age 18–20 years old” in the questionnaire. We excluded subjects who answered that their body weight at age 18–20 years old was less than 30 kg, because it seems to be erroneous. We classified BMI18–20y into 4 categories; BMI18–20y (kg/m2): <18.5, 18.5 ≤ to < 20.0, 20.0 ≤ to < 24.0, and ≥24.0. These cut-off points were based on WHO classification and preceding studies [31, 32]. We evaluated hazard ratios (HRs) relative to the BMI18–20y: 20.0 ≤ to < 24.0 group.
We calculated entry BMI using height and body weight at entry. Entry BMI was classified into 4 categories: <20.0, 20.0 ≤ to < 22.0, 22.0 ≤ to < 24.0, 24.0≤. We evaluated HR relative to the 20.0 ≤ to < 22.0 group.
We calculated ΔBMI by subtracting BMI18–20y from entry BMI. ΔBMI was classified in 4 categories (loss: <−2.5, stable: −2.5 ≤ to < 2.5, gain: 2.5 ≤ to < 5.0, major gain: 5.0≤) as used in a preceding study [31]. We set the stable group as a reference in this analysis.
To assign abdominal circumference (AC), we used the data that were measured during medical check-up at entry. AC was classified to 3 categories: AC low: <70, AC norm: 70 ≤ to < 90, and AC high: ≥90. The cut-off point of 70 cm was based on the average measurement for Japanese women [33]; 90 cm is the reference value for metabolic syndrome screening in Japan. We calculated HR for the norm and obesity groups relative to the AC low group.
For HbA1c, we used HbA1c [N], which is used worldwide. Some women’s data were taken as HbA1c [JDS], which had previously been used only in Japan. We converted the HbA1c [JDS] to HbA1c [N] with the formula “HbA1c [NGSP] % = 1.02 × HbA1c [JDS] +0.25%” [34]. The HbA1c was classified into 3 categories (<5.5, 5.5 ≤ to < 6.5, 6.5≤). These cut-off points came from a preceding study [35, 36]. We set the <5.5 group as a reference in this analysis.
Statistical analysis
We estimated HRs and 95% confidence intervals (CIs) using multivariate Cox proportional hazards regression model. We selected the 4 covariations: age at the first medical check-up during the study period, smoking habit (Never smokers, Past smokers, and Current smokers), alcohol consumption (Never drinkers, Opportunity drinkers, and Regular drinkers), and Family history (having breast cancer or ovarian cancer among primary or secondary family members). In the initial analysis, we divided women into premenopausal and postmenopausal groups, and analyzed their breast cancer incidence with regard to BMI18–20y, baseline BMI, ΔBMI, abdominal circumference, and HbA1c. In the secondary analysis, we divided women into two groups (BMI18–20y ≥ 20 or < 20). All analyses were performed using SPSS, version 21. All statistical tests were two-sided. P < 0.05 was considered significant.
Results
The subjects’ characteristics are shown in Table 1. The average observation period was 52.5 months, which corresponded to 131,657 person-years. During the observation period, 325 initial breast cancers were identified among 30,109 women. The premenopausal group included more regular-drinkers (P < 0.001) and current-smokers (P < 0.001). Family history of breast cancer or ovarian cancer was not related to menopausal status. Premenopausal women tended to be leaner than postmenopausal women according to entry BMI (P < 0.001), BMI18–20y (P < 0.001), AC (P < 0.001), and HbA1c (P < 0.001).
In the analysis of ΔBMI, postmenopausal women in the major gain group had significantly higher risk for developing breast cancer than did the stable group (HR 1.902, 95% CI 1.202–3.009; Table 2). However, this association was observed in only women whose BMI18–20y was <20 (BMI18–20y < 20—HR 2.048, 95% CI 1.114–3.765, whereas BMI18–20y ≥ 20—HR 0.974, 95% CI 0.469–2.024; Table 3) if analyzed separately for BMI18–20y.
Similarly, in analysis of AC, postmenopausal women in the large AC group were significantly more likely to develop breast cancer than those in the small AC group (HR 2.500, 95% CI 1.091–5.730; Table 2). However, this association was observed only among women whose BMI18–20y was <20 (BMI18–20y < 20—HR 0.360, 95% CI 0.049–2.625, whereas BMI18–20y ≥ 20—HR 3.259, 95% CI 1.208–8.786; Table 3) if analyzed separately by BMI18–20y.
HbA1c was not associated with breast cancer development if only menopausal status was considered. However, among women who were both postmenopausal and whose BMI18–20y was >20, those with high HbA1c were more likely to develop breast cancer than those with low HbA1c (HR 3.325, 95% CI 1.307–8.460; Table 3).
The entry BMI groups did not show significantly difference in breast cancer incidence. However, subgroup analysis showed that, among postmenopausal women with high entry BMI (>24), those whose BMI18–20y had been <20 had a high risk of developing breast cancer (HR 1.903, 95% CI 0.966–3.751, P = 0.063), whereas those whose BMI18–20 was ≥20 had a low risk of developing breast cancer (HR 2.267, 95% CI 0.903–5.689, P = 0.081; Table 3).
By itself, BMI18–20y did not affect breast cancer development.
Discussion
In this study, we evaluated the association between obesity and development of breast cancer in Asian women. We found that factors associated with developing breast cancer were large AC (≥90 cm), increased BMI ≥5 from 18 to 20 years old, and high HbA1c among postmenopausal women whose BMI18–20y was >20.
In analyzing entry BMI, we found that premenopausal women whose entry BMI was ≥24 kg/m2 were less likely to develop breast cancer, and postmenopausal women whose entry BMI was ≥24 kg/m2 were more likely to develop breast cancer.
In the previous study, postmenopausal obesity was reported to increase risk of breast cancer regardless of race, as also found in the current study [14, 37]. However, premenopausal obesity was reported to increase the risk of breast cancer for Asian women [14] and decrease it in non-Asian women [37]. This present study found that obesity in Asian and non-Asian women did not affect differently.
High BMI at 20 years old is reported to significantly decrease likelihood of premenopausal breast cancer [17, 31]. In our study, high BMI18–20y (≥24 kg/m2) tended to decrease premenopausal breast cancer compared with average BMI18–20y (20 ≤ to < 24; HR 0.509, 95% CI 0.160–1.615; Table 2]. Therefore, high premenopausal BMI has been suggested to suppress premenopausal breast cancer.
In our study, large ΔBMI (≥5.0) increased postmenopausal breast cancer incidence. Other studies have shown similar results [17, 26, 28, 38, 39], indicating that a slender body habitus at adolescence is associated with postmenopausal breast cancer development [31]. In this study, significantly increased risks for breast cancer were associated with ΔBMI (major gain group compared with stable group) and AC (≥90 cm group compared with ≤70 cm group) were observed only among women whose BMI18–20y was <20, indicating that women who were slender or average at 18–20 years old and whose BMI or AC increased are significantly more likely to develop breast cancer. These findings also suggest that dramatic changes in lipid metabolism during menopause are associated with breast cancer. However, among women with high HbA1c, BMI18–20y ≥ 20 significantly increased breast cancer risk.
Although associations between HbA1c and cancer development have been reported [35, 36, 40], these relationships are controversial for each organ. Among studies of HbA1c and breast cancer, some support a relationship [35, 40] and some do not [36, 41, 42]. In this study, we had a new viewpoint from evaluating the relationship between breast cancer development and HbA1c with regard to BMI18–20y. A positive association between HbA1c and cancer incidence has been attributed to attenuated immunity against tumor cells caused by hyperglycemia [43]; thus, longer periods of hyperglycemia would correspond to increased risks for cancer. By considering obesity at 18–20 years old in this study, we may be able to evaluate the effect of high HbA1c on carcinogenesis more accurately.
Some studies have evaluated the relationship between waist size and breast cancer [29, 44], and found waist size to be positively associated with breast cancer risk; our results were similar to theirs. However, unlike most preceding studies, we both focused on Asian women, and used AC (which is the measurement method for Japanese figures), rather than waist measurement (which is obviously correlated, but not the same thing). The relationship between AC and breast cancer is interesting, because in recent years in Japan, AC measurement has become a standard part of medical check-ups, to help spot metabolic syndrome. Our results indicate that AC could also identify women with high breast cancer risk and thus lead to more effective breast cancer screening.
Our study has several limitations. First, all subjects had undergone opportunistic breast cancer screenings. Second, we used data from women who had at least two breast cancer screenings, which may have led to selective bias. Third, some data were obtained using questionnaires, and therefore must be affected by recall bias. Measurement error may also be included, although not inevitably.
In summary, this study showed that large BMI gain after adulthood and (among women whose BMI18–20y was greater than 20) large abdominal circumference and high HbA1c level are associated with greater postmenopausal breast cancer risk.
References
Jatoi I, Anderson WF, Rao SR, Devesa SS (2005) Breast cancer trends among black and white women in the United States. J Clin Oncol 23:7836–7841. doi:10.1200/JCO.2004.01.0421
Siegel RL, Miller KD, Jemal A (2016) Cancer statistics, 2016. CA Cancer J Clin 66:7–30. doi:10.3322/caac.21332
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136:E359–E386. doi:10.1002/ijc.29210
DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A (2016) Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA Cancer J Clin 66:31–42. doi:10.3322/caac.21320
Katanoda K, Hori M, Matsuda T, Shibata A, Nishino Y, Hattori M, Soda M, Ioka A, Sobue T, Nishimoto H (2015) An updated report on the trends in cancer incidence and mortality in Japan, 1958–2013. Jpn J Clin Oncol 45:390–401. doi:10.1093/jjco/hyv002
Shin S, Saito E, Inoue M, Sawada N, Ishihara J, Takachi R, Nanri A, Shimazu T, Yamaji T, Iwasaki M, Sasazuki S, Tsugane S (2016) Dietary pattern and breast cancer risk in Japanese women: the Japan Public Health Center-based Prospective Study (JPHC Study). Br J Nutr 115:1769–1779 doi:10.1017/S0007114516000684
De Stefani E, Deneo-Pellegrini H, Boffetta P, Ronco AL, Aune D, Acosta G, Mendilaharsu M, Brennan P, Ferro G (2009) Dietary patterns and risk of cancer: a factor analysis in Uruguay. Int J Cancer 124:1391–1397. doi:10.1002/ijc.24035
Wu AH, Yu MC, Tseng CC, Stanczyk FZ, Pike MC (2009) Dietary patterns and breast cancer risk in Asian American women. Am J Clin Nutr 89:1145–1154. doi:10.3945/ajcn.2008.26915
Zhang CX, Ho SC, Fu JH, Cheng SZ, Chen YM, Lin FY (2011) Dietary patterns and breast cancer risk among Chinese women. Cancer Causes Control 22:115–124. doi:10.1007/s10552-010-9681-8
Farvid MS, Cho E, Chen WY, Eliassen AH, Willett WC (2015) Adolescent meat intake and breast cancer risk. Int J Cancer 136:1909–1920. doi:10.1002/ijc.29218
Pouchieu C, Deschasaux M, Hercberg S, Druesne-Pecollo N, Latino-Martel P, Touvier M (2014) Prospective association between red and processed meat intakes and breast cancer risk: modulation by an antioxidant supplementation in the SU.VI.MAX randomized controlled trial. Int J Epidemiol 43:1583–1592. doi:10.1093/ije/dyu134
Cho E, Chen WY, Hunter DJ, Stampfer MJ, Colditz GA, Hankinson SE, Willett WC (2006) Red meat intake and risk of breast cancer among premenopausal women. Arch Intern Med 166:2253–2259. doi:10.1001/archinte.166.20.2253
Taylor EF, Burley VJ, Greenwood DC, Cade JE (2007) Meat consumption and risk of breast cancer in the UK Women’s Cohort Study. Br J Cancer 96:1139–1146. doi:10.1038/sj.bjc.6603689
Wada K, Nagata C, Tamakoshi A, Matsuo K, Oze I, Wakai K, Tsuji I, Sugawara Y, Mizoue T, Tanaka K, Iwasaki M, Inoue M, Tsugane S, Sasazuki S, Japan RGftDaEoCPSi (2014) Body mass index and breast cancer risk in Japan: a pooled analysis of eight population-based cohort studies. Ann Oncol 25:519–524. doi:10.1093/annonc/mdt542
Sonnenschein E, Toniolo P, Terry MB, Bruning PF, Kato I, Koenig KL, Shore RE (1999) Body fat distribution and obesity in pre- and postmenopausal breast cancer. Int J Epidemiol 28:1026–1031
Montazeri A, Sadighi J, Farzadi F, Maftoon F, Vahdaninia M, Ansari M, Sajadian A, Ebrahimi M, Haghighat S, Harirchi I (2008) Weight, height, body mass index and risk of breast cancer in postmenopausal women: a case-control study. BMC Cancer 8:278. doi:10.1186/1471-2407-8-278
Huang Z, Hankinson SE, Colditz GA, Stampfer MJ, Hunter DJ, Manson JE, Hennekens CH, Rosner B, Speizer FE, Willett WC (1997) Dual effects of weight and weight gain on breast cancer risk. JAMA 278:1407–1411
Kaaks R, Van Noord PA, Den Tonkelaar I, Peeters PH, Riboli E, Grobbee DE (1998) Breast-cancer incidence in relation to height, weight and body-fat distribution in the Dutch “DOM” cohort. Int J Cancer 76:647–651
Adebamowo CA, Ogundiran TO, Adenipekun AA, Oyesegun RA, Campbell OB, Akang EE, Rotimi CN, Olopade OI (2003) Waist-hip ratio and breast cancer risk in urbanized Nigerian women. Breast Cancer Res 5:R18–R24
Rosato V, Bosetti C, Talamini R, Levi F, Montella M, Giacosa A, Negri E, La Vecchia C (2011) Metabolic syndrome and the risk of breast cancer in postmenopausal women. Ann Oncol 22:2687–2692. doi:10.1093/annonc/mdr025
Chow LW, Lui KL, Chan JC, Chan TC, Ho PK, Lee WY, Leung LH, Sy WM, Yeung CC, Yung AK (2005) Association between body mass index and risk of formation of breast cancer in Chinese women. Asian J Surg 28:179–184. doi:10.1016/S1015-9584(09)60338-9
Suzuki S, Kojima M, Tokudome S, Mori M, Sakauchi F, Wakai K, Fujino Y, Lin Y, Kikuchi S, Tamakoshi K, Tamakoshi A (2013) Obesity/weight gain and breast cancer risk: findings from the Japan collaborative cohort study for the evaluation of cancer risk. J Epidemiol 23:139–145
Kuriyama S, Tsubono Y, Hozawa A, Shimazu T, Suzuki Y, Koizumi Y, Ohmori K, Nishino Y, Tsuji I (2005) Obesity and risk of cancer in Japan. Int J Cancer 113:148–157. doi:10.1002/ijc.20529
Ahn J, Schatzkin A, Lacey JV, Albanes D, Ballard-Barbash R, Adams KF, Kipnis V, Mouw T, Hollenbeck AR, Leitzmann MF (2007) Adiposity, adult weight change, and postmenopausal breast cancer risk. Arch Intern Med 167:2091–2102. doi:10.1001/archinte.167.19.2091
Reeves GK, Pirie K, Beral V, Green J, Spencer E, Bull D, Collaboration MWS (2007) Cancer incidence and mortality in relation to body mass index in the Million Women Study: cohort study. BMJ 335:1134. doi:10.1136/bmj.39367.495995.AE
Florath I, Sarink D, Saunders C, Heyworth J, Fritschi L (2016) Breast cancer risk and the interaction between adolescent body size and weight gain in later life: a case-control study. Cancer Epidemiol 45:135–144. doi:10.1016/j.canep.2016.10.016
Sebastiani F, Cortesi L, Sant M, Lucarini V, Cirilli C, De Matteis E, Marchi I, Negri R, Gallo E, Federico M (2016) Increased Incidence of breast cancer in postmenopausal women with high body mass index at the modena screening program. J Breast Cancer 19:283–291. doi:10.4048/jbc.2016.19.3.283
Cordina-Duverger E, Truong T, Anger A, Sanchez M, Arveux P, Kerbrat P, Guénel P (2016) Weight and weight changes throughout life and postmenopausal breast cancer risk: a case-control study in France. BMC Cancer 16:761. doi:10.1186/s12885-016-2793-0
Wang X, Li L, Gao J, Liu J, Guo M, Liu L, Wang W, Wang J, Xing Z, Yu Z (2016) The association between body size and breast cancer in han women in Northern and Eastern China. Oncologist. doi:10.1634/theoncologist.2016-0147
Chen L, Cook LS, Tang MT, Porter PL, Hill DA, Wiggins CL, Li CI (2016) Body mass index and risk of luminal, HER2-overexpressing, and triple negative breast cancer. Breast Cancer Res Treat 157:545–554. doi:10.1007/s10549-016-3825-9
Suzuki R, Iwasaki M, Inoue M, Sasazuki S, Sawada N, Yamaji T, Shimazu T, Tsugane S, Group JPHC-bPS (2011) Body weight at age 20 years, subsequent weight change and breast cancer risk defined by estrogen and progesterone receptor status–the Japan public health center-based prospective study. Int J Cancer 129:1214–1224. doi:10.1002/ijc.25744
Consultation WE (2004) Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363:157–163. doi:10.1016/S0140-6736(03)15268-3
The National Health and Nutrition Survey in Japan (2011). In: Cancer Control and Health Promotion Division. Health Service Bureau. Ministry of Health, Labour and Welfare, Japan
Kashiwagi A, Kasuga M, Araki E, Oka Y, Hanafusa T, Ito H, Tominaga M, Oikawa S, Noda M, Kawamura T, Sanke T, Namba M, Hashiramoto M, Sasahara T, Nishio Y, Kuwa K, Ueki K, Takei I, Umemoto M, Murakami M, Yamakado M, Yatomi Y, Ohashi H, Society CotSoDMRLToJD (2012) International clinical harmonization of glycated hemoglobin in Japan: From Japan Diabetes Society to National Glycohemoglobin Standardization Program values. J Diabetes Investig 3:39–40. doi:10.1111/j.2040-1124.2012.00207.x
Goto A, Noda M, Sawada N, Kato M, Hidaka A, Mizoue T, Shimazu T, Yamaji T, Iwasaki M, Sasazuki S, Inoue M, Kadowaki T, Tsugane S, Group JS (2016) High hemoglobin A1c levels within the non-diabetic range are associated with the risk of all cancers. Int J Cancer 138:1741–1753. doi:10.1002/ijc.29917
Hope C, Robertshaw A, Cheung KL, Idris I, English E (2016) Relationship between HbA1c and cancer in people with or without diabetes: a systematic review. Diabet Med 33:1013–1025. doi:10.1111/dme.13031
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371:569–578. doi:10.1016/S0140-6736(08)60269-X
Trentham-Dietz A, Newcomb PA, Egan KM, Titus-Ernstoff L, Baron JA, Storer BE, Stampfer M, Willett WC (2000) Weight change and risk of postmenopausal breast cancer (United States). Cancer Causes Control 11:533–542
Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE (2006) Adult weight change and risk of postmenopausal breast cancer. JAMA 296:193–201. doi:10.1001/jama.296.2.193
Travier N, Jeffreys M, Brewer N, Wright CS, Cunningham CW, Hornell J, Pearce N (2007) Association between glycosylated hemoglobin and cancer risk: a New Zealand linkage study. Ann Oncol 18:1414–1419. doi:10.1093/annonc/mdm135
Miao Jonasson J, Cederholm J, Eliasson B, Zethelius B, Eeg-Olofsson K, Gudbjörnsdottir S (2012) HbA1C and cancer risk in patients with type 2 diabetes—a nationwide population-based prospective cohort study in Sweden. PLoS ONE 7:e38784. doi:10.1371/journal.pone.0038784
Lin J, Ridker PM, Rifai N, Lee IM, Manson JE, Buring JE, Zhang SM (2006) A prospective study of hemoglobin A1c concentrations and risk of breast cancer in women. Cancer Res 66:2869–2875. doi:10.1158/0008-5472.CAN-05-3922
Berrou J, Fougeray S, Venot M, Chardiny V, Gautier JF, Dulphy N, Toubert A, Peraldi MN (2013) Natural killer cell function, an important target for infection and tumor protection, is impaired in type 2 diabetes. PLoS ONE 8:e62418. doi:10.1371/journal.pone.0062418
Gaudet MM, Carter BD, Patel AV, Teras LR, Jacobs EJ, Gapstur SM (2014) Waist circumference, body mass index, and postmenopausal breast cancer incidence in the Cancer Prevention Study-II Nutrition Cohort. Cancer Causes Control 25:737–745. doi:10.1007/s10552-014-0376-4
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Neither author has any disclosures to report.
Ethical standards
This study complies with the current laws of Japan.
Statement of human rights
For this type of study, formal consent was not required.
Rights and permissions
About this article

Cite this article
Suzuki, Y., Tsunoda, H., Kimura, T. et al. BMI change and abdominal circumference are risk factors for breast cancer, even in Asian women. Breast Cancer Res Treat 166, 919–925 (2017). https://doi.org/10.1007/s10549-017-4481-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-017-4481-4