
Abstract
In a prior substudy of the CAN-NCIC-MA.22 clinical trial (ClinicalTrials.gov identifier NCT00066443), we observed that neoadjuvant chemotherapy reduced tumor RNA integrity in breast cancer patients, a phenomenon we term “RNA disruption.” The purpose of the current study was to assess in the full patient cohort the relationship between mid-treatment tumor RNA disruption and both pCR post-treatment and, subsequently, disease-free survival (DFS) up to 108 months post-treatment. To meet these objectives, we developed the RNA disruption assay (RDA) to quantify RNA disruption and stratify it into 3 response zones of clinical importance. Zone 1 is a level of RNA disruption inadequate for pathologic complete response (pCR); Zone 2 is an intermediate level, while Zone 3 has high RNA disruption. The same RNA disruption cut points developed for pCR response were then utilized for DFS. Tumor RDA identified >fourfold more chemotherapy non-responders than did clinical response by calipers. pCR responders were clustered in RDA Zone 3, irrespective of tumor subtype. DFS was about 2-fold greater for patients with tumors in Zone 3 compared to Zone 1 patients. Kaplan–Meier survival curves corroborated these findings that high tumor RNA disruption was associated with increased DFS. DFS values for patients in zone 3 that did not achieve a pCR were similar to that of pCR recipients across tumor subtypes, including patients with hormone receptor positive tumors that seldom achieve a pCR. RDA appears superior to pCR as a chemotherapy response biomarker, supporting the prospect of its use in response-guided chemotherapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
For locally advanced breast cancer (LABC), neoadjuvant chemotherapy is administered prior to surgery to improve local control of disease [1, 2]. While only 30–42 % of LABC patients survive 5 years following chemotherapy, 5-year survival rates are increased up to 90 % for patients that achieve a pathologic complete response (pCR), defined as the absence of invasive cancer in the breast and axilla post-treatment [3, 4]. “Response-guided therapy,” whereby treatment is modified early in chemotherapy for patients with clinically non-responding tumors is also possible with neoadjuvant chemotherapy. Support for this approach was recently reported in the GeparTrio trial, where disease-free survival (DFS) and overall survival (OS) were significantly longer after response-guided therapy, [8 cycles of anthracycline-taxane-based chemotherapy (TAC) or 6 cycles of TAC followed by capecitabine and vinorelbine] compared to conventional chemotherapy (6 cycles of TAC) [5]. DFS improvement was observed for all hormone receptor positive (HR+) and Her2+ tumors, but not triple-negative tumors (TNBC) [5]. Interestingly, while pCR has been associated with increased patient survival post-chemotherapy [6–8], pCR rates in this study could not predict the enhanced survival benefit from response-guided chemotherapy. pCR, however, did predict improved DFS for patients with TNBC or Her2+ tumors [5]. As pCR determinations can only be made post-treatment and as few patients with hormone receptor positive tumors achieve a pCR [3, 9–12], this endpoint is not an ideal chemoresponse biomarker. High pre-treatment tumor Ki-67 levels have been associated with poor prognosis after chemotherapy for lymph node negative patients, but no cut points could be established to define clearly prognostic groups [13–15]. Ki-67 levels after neoadjuvant chemotherapy could predict prognosis for HR+ tumors, but they could not predict outcome after response-guided chemotherapy [16]. Similarly, while tumor size, volume, and apparent diffusion coefficient values by magnetic resonance imaging, have shown promise to assess treatment response [17], these studies had variable study designs, variable cut points, and were significantly underpowered [18]. Reduced tumor 18F-deoxyglucose (FDG) uptake after chemotherapy administration is also associated with the achievement of a pCR in breast cancer patients [19–21], but the sensitivity and specificity of this approach has been low [22]. FDG positron emission tomography (PET) has recently been shown to be effective in identifying non-responders to docetaxel plus trastuzumab in patients with Her2+ breast cancer who benefitted from bevacizumab treatment [23]. Nevertheless, the costs and infrastructure for PET scanning also limit this approach.
In the MA.22 LABC clinical trial, RNA was isolated from tumor core biopsies of the first 50 enrolled patients prior to, during, and after concurrent epirubicin/docetaxel chemotherapy, and RNA integrity for each sample assessed as an RNA integrity number (RIN). We observed that a low mid-treatment RIN was associated with a pCR post-treatment (pCR defined as described above) [24]. In concurrent independent biopsies, there was no association between tumor cellularity and tumor RIN values mid-treatment, nor was mid-treatment tumor cellularity correlated with a post-treatment pCR [24]. Moreover, while the RIN algorithm specifically assesses autolytic RNA degradation [25], we observed that chemotherapy treatment in highly responding tumors creates unique bands in the RNA electropherogram, which often resulted in the assignment of “n/a” values for RIN by the Agilent Bioanalyzer. To better quantify this phenomenon of “RNA disruption,” we developed the RNA disruption assay (RDA), where the magnitude of RNA disruption is expressed as an RNA disruption index (RDI). The objective of this study was to assess tumor RNA disruption during treatment as a biomarker of chemotherapy response, the reporting of which would strongly meet current reporting recommendations for tumor marker prognostic and predictive studies (REMARK guidelines) [26]. These include the purpose of our study, a CONSORT diagram, patient and specimen characteristics, assay methods, study design, statistical analysis methods, computation of hazard ratios, the plotting of Kaplan–Meier (K–M) survival curves, and multivariate discriminant analysis. We show that high tumor RNA disruption during chemotherapy is associated with markedly increased DFS post-treatment, irrespective of tumor subtype or achievement of pCR.
Methods
Preparation of tumor RNA from patients
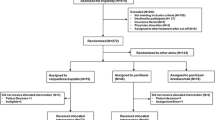
In the NCIC-CTG-MA.22 clinical trial (ClinicalTrials.gov identifier NCT00066443; for Consort Diagram, see Fig. 1), various doses of epirubicin and docetaxel were administered to 93 patients with LABC in a standard (q3 weekly) or dose dense (q2 weekly) regimen, with pegfilgrastim support. Doses for the q3 weekly regimen were 75 mg/m2 docetaxel and 75, 90, 105, or 120 mg/m2 epirubicin, while doses for both drugs in the q2 weekly regimen were 50, 60, and 70 mg/m2. At each time point, tumor volume was assessed clinically using caliper measurements. Under ultrasound guidance, six tumor core biopsies (14 gauge needle) were obtained from consenting patients at baseline, after 3 (q3 weekly) or 4 (q2 weekly) cycles of chemotherapy (mid-treatment), and after 6 (q3 weekly) or 8 (q2 weekly) cycles of chemotherapy. At each time point, three biopsies were fixed in formalin for immunohistochemical receptor expression studies, while the remaining three were quickly stored in liquid nitrogen for RNA integrity studies. Four patients in the q3 weekly schedule and one patient in the q2 weekly schedule did not yield mid-treatment biopsies, while pathology data were unavailable for 3 patients (Fig. 1). Thus, 85 patients had complete RNA integrity, receptor expression, and clinical response data. For RNA isolation, frozen biopsies were placed into 0.5 ml of RLT buffer (Qiagen), homogenized for 5 min using a Coreless pellet pestle gun, and the homogenates sheared through a 20 gauge needle. Total RNA was isolated from each homogenate using Qiagen RNeasy Mini kits.

Consolidated Standards of Reporting Trials (CONSORT) flow diagram for the MA.22 clinical trial, administered by the NCIC Clinical Trials Group (Kingston, ON, Canada)
Assessment of RNA quantity, quality, and RNA disruption
RNA quality was assessed by applying 1 μl of each RNA preparation onto Caliper™ RNA Nanochips and resolving the component RNAs by capillary electrophoresis using an Agilent 2100 Bioanalyzer, as per the manufacturer’s protocol. Using RNA standards of known mass and molecular weight (also run on the chip), the quantity of RNA in each preparation was determined. To quantify RNA disruption, a proprietary algorithm was applied, which expressed the disrupted RNA to normal RNA ratio as an RNA disruption index (RDI). To better evaluate mid-treatment RNA disruption and its relationship to pCR incidence, we stratified RDI values into three zones based on pCR response. As shown in Fig. 2, Zone 1 begins at 0 RDI and extends to the maximum level of RNA disruption in tumor biopsies that is inadequate to obtain a pCR (RDI ≤10; NPV >0.99). These patients are deemed pCR non-responders. Zone 2 contains an intermediate zone of RNA disruption (maximum RDI >10 and ≤35), which permitted the inclusion of one pCR responder in this zone. Zone 3 is a high level of RNA disruption (maximum RDI >35), containing the vast majority of pCR responders (7 of 8 pCRs in the MA.22 clinical trial). Subsequently, the same response zones with the same RDI cut points based on pCR incidence were used to assess the relationship between the extent of tumor RNA disruption and DFS.

RNA disruption indices and RNA concentration values for tumors from MA.22 patients after 3–4 cycles of epirubicin/docetaxel chemotherapy. Hormone receptor positive (HR+) tumors express ER, with or without PR and without Her2 expression. Her2+ tumors express Her2, with or without ER or PR. Triple-negative breast cancers (TNBCs) lack expression of ER, PR, and Her2. Compared to non-responders, pCR responders were clustered in regions of high RNA disruption and lower RNA content regardless of tumor subtype. No patients with HR+ tumors had a pCR
RNA disruption specificity and distinction from RNA autolytic degradation
When test core biopsies of untreated breast tumor xenografts from mice were flash frozen in liquid nitrogen or immersed in RNAlater™, their RNA banding pattern remained normal and their RDI low over time. In contrast, biopsies from identical tumors placed in gauze immersed in phosphate buffered saline and stored at room temperature for 48 h showed a large low molecular weight peak of autolytically degraded RNA in the “fast region” of the electropherogram (data not shown), which was distinct from “inter-region” bands of RNA for chemotherapy-treated tumors seen in Fig. 3. These abnormal RNA banding patterns often resulted in a RIN value of “n/a” by the Bioanalyzer. These observations indicated that differences in RDI values in patient tumors were chemotherapy-specific and unrelated to preanalytical factors. The RNA quantity and quality metrics using the Bioanalyzer were highly reproducible, with an intra-chip and inter-chip variation in the RNA concentration value for repeated same sample assessment of 3.1 and 3.7 %, respectively. The intra-chip and inter-chip variations in RDI value for repeated same sample assessment were 2.7 and 3.1 %, respectively.

The RNA disruption index (RDI) quantifies the tumor RNA banding pattern induced by chemotherapy agents. As shown in the above electropherograms of MA.22 patients, RDI increases as the intensities of the 28S and 18S rRNA bands decrease and the intensities of abnormal bands increase. The lack of relationship between RDI and Agilent Technologies’ RNA Integrity Number (RIN) for samples exhibiting high RNA degradation is depicted. Unlike RDI, RIN was developed to quantify RNA autolytic degradation
Assessment of cell surface receptors
The expression of estrogen receptor (ER), progesterone receptor (PR), and the Her2/Neu receptor (Her2)] prior to therapy in 82 MA.22 patient biopsies was assessed by immunohistochemistry as described previously [24].
Assessment of mid-treatment tumor cytology
A separate collection of mid-treatment biopsies was fixed in formalin, paraffin-embedded, sectioned, and stained with haematoxylin/eosin to determine the mean per cent tumor cellularity within each biopsy as assessed by the trial pathologist.
Results
Chemotherapy effects on the tumor RNA disruption index (RDI)
The RDI magnitude was directly proportional to the degree of departure from the normal banding pattern for tumor RNA (Fig. 3). As RDI increased, the intensities of the 28S and 18S rRNA bands decreased, while the intensities of abnormal RNA bands increased. Maximum RDI values and RNA concentration for all patients, pCR responders, and pCR non-responders prior to treatment and after 3 or 4 cycles of chemotherapy are depicted in Table 1. The mean maximum tumor RNA disruption index (RDI) for all patients increased 3.4-fold at mid-treatment from 26.0 ± 5.8 to 88.1 ± 19 (p = 3.7 × 10−8, WSR). Moreover, while pre-treatment maximum RDIs were not significantly different between pCR responders and pCR non-responders (lack of pCR), mean mid-treatment maximum RDI values were 2.2-fold higher in pCR responders (176 ± 60) than pCR non-responders (79.0 ± 20) [p = 0.005, Mann–Whitney–Wilcoxon test (MWW)]. Chemotherapy increased maximum tumor RDI values in pCR responders 5.8-fold from 30.4 ± 23 at baseline to 176 ± 60 post-treatment. The effects of treatment on maximum tumor RDI values were highly significant in both pCR responders and pCR non-responders (p values for WSR of 0.012 and 3.1 × 10−5, respectively). A twofold reduction in the mean tumor RNA concentration from 197 ± 24 to 94 ± 13 ng/μl [p = 3.4 × 10−6 Wilcoxon Signed-Rank test (WSR)] was observed between baseline and the 3rd of 4th cycle of chemotherapy.
Mid-treatment RNA disruption and clinical response to chemotherapy
Eighty per cent of pCR non-responder tumors had mid-treatment maximum RDI values in zones 2 or 3 (Table 2), suggesting that they responded partially or fully to treatment but did not achieve a pCR. In contrast, 20 % of patients had mid-treatment maximum tumor RDI values in zone 1 (Table 2). As shown in plots of tumor maximum RDI versus RNA concentration, all pCR responders mid-treatment clustered to the top (high RDI) and left (low RNA content) of these plots (Fig. 2). Only 5 % of patients exhibited no response to treatment by clinical assessment, while 75 and 20 % of patients exhibited partial and complete clinical responses, respectively (Table 2). In contrast, RDA indicated that 20 % of tumors exhibited very little RNA disruption mid-treatment (RDA zone 1)—greater than four times the number of non-responders determined by clinical response. While only nine per cent of patients achieved a pCR, RDA identified 35 % of patients as partial responders (zone 2) and 45 % of patients as strong responders (zone 3). For pCR responders, 7 had tumors in zone 3 and 1 in zone 2. Seventy-five per cent of pCR responders had a complete clinical response, while 25 % had a partial clinical response. Compared to pCR non-responders, pCR responders were clustered in regions of high RNA disruption and low RNA content (regardless of tumor subtype; see Fig. 2). No patients with hormone receptor positive (HR+) tumors [ER+, PR+ or PR−, Her2−] had a pCR.
Tumor RNA disruption and disease-free survival (DFS)
Disease-free survival (DFS) without disease progression at up to 108 months follow-up was significantly greater (by 23 months) for zone 3 patients mid-treatment compared to zone 1 patients (p = 0.009, MWW; Table 3). Even greater DFS (an additional 27.2 months) could be seen for patients with HR+ tumors in zone 3 compared to similar tumors in zone 1 (p = 0.007, MWW; Table 3). None of the above significant differences were observed when pre-treatment tumor RDI values were assessed.
Survival benefit detected by high RNA disruption is equivalent to that achieved by pCR
Table 3 also shows that the mean DFS for MA.22 patients with mid-treatment tumors in Zone 3 was 56.9 ± 5.6 months—very similar to that experienced by pCR responders (59.4 ± 12 months). Patients with mid-treatment tumors in zone 1 had considerably lower DFS (33.9 ± 6.4 months). The 38 patients (45 %) with tumors in RDA zone 3 enjoyed a DFS benefit equivalent to the 8 pCR recipients (9 % of patients). Kaplan–Meier (K–M) plots (Fig. 4) revealed that DFS was clearly greater for patients with tumors in zone 3 (RDI >35) mid-treatment than for patients with tumors in zones 1 or 2 (RDI ≤35), although this difference was of borderline statistical significance [p = 0.10, Mantel Cox test (MC)]. In addition, in exploratory K–M analyses, both the separation between the disease-free survival curves and the significance of this separation clearly changed as RDI cut points were increased from 20 (p = 0.92, hazard ratio 1.0; data not shown), to 35 (p = 0.10, hazard ratio 1.8; Fig. 4), to 50 (p = 0.05, hazard ratio 2.0; Fig. 5), and then to 100 (p = 0.04, hazard ratio 2.2). This suggests a lack of randomness in the data and a clear relationship between the extent of RNA disruption mid-treatment and patient disease-free survival.

Kaplan–Meier plots depicting differences in disease-free survival over time between MA.22 patients with mid-treatment tumor RDI values in zone 3 (RDI >35) and MA.22 patients with mid-treatment tumor RDI values in zones 1 and 2 (RDI ≤35). The significance of the differences in the Kaplan–Meier plots [as determined using a Mantel Cox (MC) test] and the hazard ratio associated with RDI values ≤35 are listed below the plots. Patients on the plots that exhibited a pCR post-treatment are indicated using black arrows

Exploratory Kaplan–Meier plots depicting differences in disease-free survival curves between MA.22 patients with tumor RDI values >50 and patients with tumor RDI values ≤50. A similar analysis was conducted where differences in disease-free survival curves were assessed for MA.22 patient tumor RDI values above or below 100. The significance of the differences in the Kaplan-Meier plots [as determined using a Mantel Cox (MC) test] and the hazard ratio associated with the lower RDI values are listed below the plots. Patients on the plots that exhibited a pCR post-treatment are indicated using black arrows
Enhanced DFS is associated with high RNA disruption across tumor subtypes
Interestingly, as shown in Table 4, the mean DFS for patients with HR+ tumors in zone 3 was 61.0 ± 7.0 months—very similar to both pCR responders and non-pCR responders in zone 3 across all subtypes (59.4 ± 12 months and 56.3 ± 6.2, respectively). Yet, no patient with a HR+ tumor achieved a pCR. While the data set is small, the mean DFS for patients in zone 3 for a particular tumor subtype appeared very similar to the mean DFS for pCR responders of that subtype. This included patients with TNBC, which had a lower DFS interval than the HR+ and Her2+ subtypes.
Discussion
In this study, patients with tumors in Zone 1 did not exhibit a pCR and had inferior DFS irrespective of subtype. RDA identified substantially more chemotherapy non-responders (20 %) compared to clinical assessment (5 %). Given that pCR has been shown to be an independent predictive factor of increased survival after neoadjuvant chemotherapy, irrespective of breast cancer subtype [27], the Food and Drug Administration USA has conditionally approved the use of pCR as a drug response biomarker for accelerated drug approval. MA.22 patients without a pCR who exhibited a zone 3 level of tumor RNA disruption had a DFS benefit from chemotherapy equivalent to pCR recipients, including those with HR+ tumors (Table 4). This suggests that pCR is inferior to RDA as a chemoresponse biomarker. In K–M plots, patients with tumor RDI values above 35 (Fig. 4) or above 50 and 100 (Fig. 5) exhibited substantially greater survival than patients with tumors below these values. While 7 of 8 pCR recipients in Fig. 4 resided on the curve representing higher tumor RNA disruption (RDI >35) and higher survival, so did a large number of patients that did not achieve a pCR. It is important to recognize that RDA zones identified patients with superior DFS even though the cut points were designed based only on pCR response. Taken together, these findings are consistent with a recent proposal [28] that pCR may only be a suitable surrogate parameter of treatment efficacy in a subset of patients with highly proliferating ER− or Her2+ breast tumors. Further support for the limited utility of pCR as an indicator of chemotherapy response stems from a recent meta-analysis of 28 clinical trials involving 13,738 patients, which revealed that only 16 % of the variability among the effects of neoadjuvant chemotherapy DFS could be attributed to the pCR rate [29]. Another recent meta-analysis of 11,955 patients in 12 clinical trials showed that pCR was prognostic only in patients with aggressive tumor subtypes (Her2+/ER− and TNBC) [30]. Concerns have been raised as to the utility of pCR as a chemoresponse biomarker for all breast tumor subtypes [31]. A recent review [32] argues that because pCR is seldom seen with endocrine therapy or chemotherapy in HR+ tumors, alternate intermediate endpoints need to be established and validated in patients with this tumor subtype. This study supports RDA as an alternate intermediate endpoint both for response and non-response to chemotherapy.
Multivariate discriminant analysis using a proportional hazard model based on a Wald test for significance (WT) revealed that neither drug dose, drug schedule, tumor subtype, tumor RNA concentration tumor cellularity, nor the magnitude of tumor RDI alone (as single variables) was significantly associated with DFS in the MA.22 clinical trial. Using a regression process, in which factors with least significance to predict DFS were singly deleted from the model until the combination of remaining factors was significant, it was found that a combination of total epirubicin dose, total docetaxel dose, and dose schedule did significantly affect DFS (Supplemental Table 1). However, as a single factor, patients with tumor RDI values >50 had significantly greater DFS than patients with RDI values ≤50 (p = 0.04, WT), consistent with the above exploratory K–M plots (Fig. 5). This indicates that, as a single factor, patients with tumor RDI values >50 have a significantly greater disease-free survival compared to those with tumor RDI values ≤50. pCR was not a significant predictor of DFS, but this is likely due to the small number of pCR responders in our study (8 in total). Note that at an RDI cut point of 50, all but one pCR responder resided on the higher survival K–M curve in Fig. 5, while at a cut point of 100, 3 pCR recipients resided on the lower survival curve (Fig. 4). Given that at an RDI cut point of 50, RDI as a single factor could predict DFS, while pCR could not, and given that at an RDI cut point of 100, 3 pCR recipients resided on the lower survival curve, these observations support our claim that RDI may be superior to pCR as a predictor of DFS.
Biopsies with low RDI values had a wide range of tumor cellularity values, as did biopsies with high RDI values. Thus, low or high RNA disruption is not surrogate for high or low tumor cellularity, respectively. This may help explain why low mid-treatment tumor cellularity values were not associated with a post-treatment pCR in an early substudy of the MA.22 clinical trial [24].
High RNA disruption was also observed in post-treatment tissues at the site of the original tumor for MA.22 patients who had a pCR post-treatment (data not shown). This indicates that RNA disruption may occur in stromal and other tissues associated with the tumor or that the highly disrupted RNA from dying tumor cells may remain within the lesion post-treatment. Moreover, these observations suggest that it is unnecessary to separate tumor tissue from surrounding stromal/inflammatory cells or normal breast tissue to utilize RNA disruption as a chemoresponse biomarker. The choice of chemotherapy agents and their order of administration may also have an impact on the magnitude of RNA disruption observed, such that regimen-specific RDI cut points may need to be established to predict response and survival after neoadjuvant chemotherapy.
We have recently observed (Narendrula et al., submitted for publication) that a variety of structurally distinct chemotherapy agents can induce tumor cell RNA disruption and death in a dose- and time-dependent manner using various cell lines in the laboratory, including breast tumor cells. This suggests that RNA disruption is commonly associated with chemotherapy-induced tumor cell death. However, the true value of RDA will be ascertained only through assessment of the relationship between tumor RNA disruption levels and both post-treatment pCR incidence and DFS in multiple independent cohorts of breast cancer patients (treated with a variety of chemotherapy regimens). Such studies are in progress. RDA would be of even greater clinical value when RNA disruption and its ability to reliably predict chemosensitivity and survival can be demonstrated early after chemotherapy administration (cycles 1 or 2). These studies are also underway. This would permit non-responding patients to be considered as early as possible for alternate treatments, such as surgery, radiation therapy, or other chemotherapy regimens, sparing these patients the toxicities of ineffective chemotherapy regimens [33–36], while possibly improving patient survival.
Conclusions
Based on the above observations, this study suggests that chemotherapy administration induces the creation of specific RNA degradation products that are distinct from those exhibited during autolytic degradation of RNA. We refer to this as “RNA disruption” and devised the RNA disruption index to quantify this phenomenon. High tumor RNA disruption is associated with both the achievement of pCR in patients and significantly improved disease-free survival. This novel biomarker could be used to assess tumor response to chemotherapy, such that non-responding patients could be spared the toxic side effects of the ineffective regimen and be moved promptly to downstream treatments such as surgery, radiation therapy, or other chemotherapy drugs.
Abbreviations
- RNA:
-
Ribonucleic acid
- RDA:
-
RNA disruption assay
- RDI:
-
RNA disruption index
- pCR:
-
Pathologic complete response
- DFS:
-
Disease-free survival
- LABC:
-
Locally advanced breast cancer advanced
- FDG:
-
Fluoro-deoxyglucose
- TNBC:
-
Triple-negative breast cancer
- PET:
-
Positron emission tomography
- RIN:
-
RNA integrity number
- ER:
-
Estrogen receptor
- PR:
-
Progesterone receptor
- HER2:
-
Human epidermal growth factor receptor 2
- HR+:
-
Hormone receptor positive
- WSR:
-
Wilcoxon Signed-Rank test
- MWW:
-
Mann–Whitney Wilcoxon
- MC:
-
Mantel Cox Test
- K-M:
-
Kaplan–Meier
- WT:
-
Wald Test
- rRNA:
-
Ribosomal RNA
References
Jacobs C, Simos D, Clemons M (2014) Treatment for locally advanced breast cancer: a global challenge, personalized medicine or both? Curr Opin Support Palliat Care 8:30–32
Sulpher J, Dent R, Dent S (2014) Neoadjuvant chemotherapy in breast cancer: what questions remain? Curr Opin Support Palliat Care 8:59–63
Kuerer HM, Newman LA, Smith TL, Ames FC, Hunt KK, Dhingra K, Theriault RL, Singh G, Binkley SM, Sneige N, Buchholz TA, Ross MI, McNeese MD, Buzdar AU, Hortobagyi GN, Singletary SE (1999) Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemotherapy. J Clin Oncol 17:460–469
Formenti SC, Dunnington G, Uzieli B, Lenz H, Keren-Rosenberg S, Silberman H, Spicer D, Denk M, Leichman G, Groshen S, Watkins K, Muggia F, Florentine B, Press M, Danenberg K, Danenberg P (1997) Original p53 status predicts for pathological response in locally advanced breast cancer patients treated preoperatively with continuous infusion 5-fluorouracil and radiation therapy. Int J Radiat Oncol Biol Phys 39:1059–1068
von Minckwitz G, Blohmer JU, Costa SD, Denkert C, Eidtmann H, Eiermann W, Gerber B, Hanusch C, Hilfrich J, Huober J, Jackisch C, Kaufmann M, Kummel S, Paepke S, Schneeweiss A, Untch M, Zahm DM, Mehta K, Loibl S (2013) Response-guided neoadjuvant chemotherapy for breast cancer. J Clin Oncol 31:3623–3630
Mieog JS, van der Hage JA, van de Velde CJ (2007) Neoadjuvant chemotherapy for operable breast cancer. Br J Surg 94:1189–1200
Specht J, Gralow JR (2009) Neoadjuvant chemotherapy for locally advanced breast cancer. Semin Radiat Oncol 19:222–228
Sinclair S, Swain SM (2010) Primary systemic chemotherapy for inflammatory breast cancer. Cancer 116:2821–2828
von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, Gerber B, Eiermann W, Hilfrich J, Huober J, Jackisch C, Kaufmann M, Konecny GE, Denkert C, Nekljudova V, Mehta K, Loibl S (2012) Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 30:1796–1804
Liu SV, Melstrom L, Yao K, Russell CA, Sener SF (2010) Neoadjuvant therapy for breast cancer. J Surg Oncol 101:283–291
Guarneri V, Broglio K, Kau SW, Cristofanilli M, Buzdar AU, Valero V, Buchholz T, Meric F, Middleton L, Hortobagyi GN, Gonzalez-Angulo AM (2006) Prognostic value of pathologic complete response after primary chemotherapy in relation to hormone receptor status and other factors. J Clin Oncol 24:1037–1044
Albain KS, Barlow WE, Ravdin PM, Farrar WB, Burton GV, Ketchel SJ, Cobau CD, Levine EG, Ingle JN, Pritchard KI, Lichter AS, Schneider DJ, Abeloff MD, Henderson IC, Muss HB, Green SJ, Lew D, Livingston RB, Martino S, Osborne CK (2009) Adjuvant chemotherapy and timing of tamoxifen in postmenopausal patients with endocrine-responsive, node-positive breast cancer: a phase 3, open-label, randomised controlled trial. Lancet 374:2055–2063
Clahsen PC, van de Velde CY, Duval C, Pallud C, Mandard AM, Obelle-Deroide A, van den Broek L, van de Vijver MJ (1999) The utility of mitotic index, oestrogen receptor and Ki-67 measurements in the creation of novel prognostic indices for node-negative breast cancer. Eur J Surg Oncol 25:356–363
Trihia H, Murray S, Price K, Gelber RD, Golouh R, Goldhirsch A, Coates AS, Collins J, Castiglione-Gertsch M, Gusterson BA (2003) Ki-67 expression in breast carcinoma: its association with grading systems, clinical parameters, and other prognostic factors—a surrogate marker? Cancer 97:1321–1331
Urruticoechea A, Smith IE, Dowsett M (2005) Proliferation marker Ki-67 in early breast cancer. J Clin Oncol 23:7212–7220
von Minckwitz G, Schmitt WD, Loibl S, Muller BM, Blohmer JU, Sinn BV, Eidtmann H, Eiermann W, Gerber B, Tesch H, Hilfrich J, Huober J, Fehm T, Barinoff J, Rudiger T, Erbstoesser E, Fasching PA, Karn T, Muller V, Jackisch C, Denkert C (2013) Ki67 measured after neoadjuvant chemotherapy for primary breast cancer. Clin Cancer Res 19:4521–4531
Prevos R, Smidt ML, Tjan-Heijnen VC, van Goethem M, Beets-Tan RG, Wildberger JE, Lobbes MB (2012) Pre-treatment differences and early response monitoring of neoadjuvant chemotherapy in breast cancer patients using magnetic resonance imaging: a systematic review. Eur Radiol 22:2607–2616
Lobbes MB, Prevos R, Smidt M, Tjan-Heijnen VC, van Goethem M, Schipper R, Beets-Tan RG, Wildberger JE (2013) The role of magnetic resonance imaging in assessing residual disease and pathologic complete response in breast cancer patients receiving neoadjuvant chemotherapy: a systematic review. Insights Imaging 4:163–175
Weber WA, Schwaiger M, Avril N (2000) Quantitative assessment of tumor metabolism using FDG-PET imaging. Nucl Med Biol 27:683–687
Kim SJ, Kim SK, Lee ES, Ro J, Kang S (2004) Predictive value of [18F]FDG PET for pathological response of breast cancer to neo-adjuvant chemotherapy. Ann Oncol 15:1352–1357
McDermott GM, Welch A, Staff RT, Gilbert FJ, Schweiger L, Semple SI, Smith TA, Hutcheon AW, Miller ID, Smith IC, Heys SD (2007) Monitoring primary breast cancer throughout chemotherapy using FDG-PET. Breast Cancer Res Treat 102:75–84
Kelloff GJ, Hoffman JM, Johnson B, Scher HI, Siegel BA, Cheng EY, Cheson BD, O’shaughnessy J, Guyton KZ, Mankoff DA, Shankar L, Larson SM, Sigman CC, Schilsky RL, Sullivan DC (2005) Progress and promise of FDG-PET imaging for cancer patient management and oncologic drug development. Clin Cancer Res 11:2785–2808
Coudert B, Pierga JY, Mouret-Reynier MA, Kerrou K, Ferrero JM, Petit T, Kerbrat P, Dupre PF, Bachelot T, Gabelle P, Giard S, Coeffic D, Bougnoux P, Prevost JB, Paintaud G, Thibault G, Hernandez J, Coudert M, Arnould L, Berriolo-Riedinger A (2014) Use of [(18)F]-FDG PET to predict response to neoadjuvant trastuzumab and docetaxel in patients with HER2-positive breast cancer, and addition of bevacizumab to neoadjuvant trastuzumab and docetaxel in [(18)F]-FDG PET-predicted non-responders (AVATAXHER): an open-label, randomised phase 2 trial. Lancet Oncol 15:1493–1502
Parissenti AM, Chapman JA, Kahn HJ, Guo B, Han L, O’Brien P, Clemons MP, Jong R, Dent R, Fitzgerald B, Pritchard KI, Shepherd LE, Trudeau ME (2010) Association of low tumor RNA integrity with response to chemotherapy in breast cancer patients. Breast Cancer Res Treat 119:347–356
Schroeder A, Mueller O, Stocker S, Salowsky R, Leiber M, Gassmann M, Lightfoot S, Menzel W, Granzow M, Ragg T (2006) The RIN: an RNA integrity number for assigning integrity values to RNA measurements. BMC Mol Biol 7:3
McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM (2005) REporting recommendations for tumor MARKer prognostic studies (REMARK). Nat Clin Pract Oncol 2:416–422
Bonnefoi H, Litiere S, Piccart M, Macgrogan G, Fumoleau P, Brain E, Petit T, Rouanet P, Jassem J, Moldovan C, Bodmer A, Zaman K, Cufer T, Campone M, Luporsi E, Malmstrom P, Werutsky G, Bogaerts J, Bergh J, Cameron DA (2014) Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann Oncol 25(6):1128–1136
Berruti A, Generali D, Brizzi MP, Ardine M, Dogliotti L, Bottini A (2005) Is pathologic complete response a valid surrogate parameter of treatment efficacy in HER2 positive breast cancer patients undergoing primary chemotherapy plus trastuzamab? J Clin Oncol 23:8130–8131
Amoroso V, Berruti A, Gallo F, Bertaglia V, Paloja E, Simoncini EL, Generali G, Bottini A, Bruzzi P, Sormani MP (2013) Pathological complete response after primary chemotherapy as a surrogate end point of treatment efficacy in breast cancer patients: a trial-based meta-analysis. In: San Antonio Breast Cancer Symposium. P3-14-03
Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L, Valagussa P, Swain SM, Prowell T, Loibl S, Wickerham DL, Bogaerts J, Baselga J, Perou C, Blumenthal G, Blohmer J, Mamounas EP, Bergh J, Semiglazov V, Justice R, Eidtmann H, Paik S, Piccart M, Sridhara R, Fasching PA, Slaets L, Tang S, Gerber B, Geyer CE Jr, Pazdur R, Ditsch N, Rastogi P, Eiermann W, von Minckwitz G (2014) Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384:164–172
Prowell TM, Pazdur R (2012) Pathological complete response and accelerated drug approval in early breast cancer. N Engl J Med 366:2438–2441
Carey LA, Winer EP (2014) Defining success in neoadjuvant breast cancer trials. Lancet 384(9938):115–116
Hurria A, Fleming MT, Baker SD, Kelly WK, Cutchall K, Panageas K, Caravelli J, Yeung H, Kris MG, Gomez J, Miller VA, D’Andrea G, Scher HI, Norton L, Hudis C (2006) Pharmacokinetics and toxicity of weekly docetaxel in older patients. Clin Cancer Res 12:6100–6105
Sparano JA, Wang M, Martino S, Jones V, Perez EA, Saphner T, Wolff AC, Sledge GW Jr, Wood WC, Davidson NE (2008) Weekly paclitaxel in the adjuvant treatment of breast cancer. N Engl J Med 358:1663–1671
Marupudi NI, Han JE, Li KW, Renard VM, Tyler BM, Brem H (2007) Paclitaxel: a review of adverse toxicities and novel delivery strategies. Expert Opin Drug Saf 6:609–621
van Dalen EC, Caron HN, Dickinson HO, Kremer LC (2011) Cardioprotective interventions for cancer patients receiving anthracyclines. Cochrane Database Syst Rev CD003917
Acknowledgments
This work was supported by funding from Sanofi-Aventis Pharmaceuticals and the Cancer Research Fund of the Ontario Institute for Cancer Research (Grant Number 02-MAY-0159) to A.M.P. Funding is also acknowledged from the Canadian Cancer Society that supports the NCIC Clinical Trials Group, and from RNA Diagnostics, Inc. We are extremely grateful to the patients who participated in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All patients involved in this study provided written consent for participation in the trial and for the provision of the tumor core biopsies. Approvals were also obtained from the research ethics board of all cancer treatment centers involved in this study. Approval for the biomarker study was also obtained from the Research Ethics Board of Health Sciences North, at which the biomarker study was conducted. We declare the clinical trial and associated biomarker study comply with the current laws governing clinical research studies in Canada.
Conflict of interest
The authors disclose financial competing interests. Drs. Parissenti and Guo are inventors of a patent owned by Laurentian University entitled “Method of using tumor RNA integrity to measure response to chemotherapy in cancer patients,” the subject of this study. The patent was based, in part, on data from patients in the MA.22 clinical trial described in this study. Dr. Maureen Trudeau was the principal investigator of the trial, and Dr. Lois Shepherd was the physician coordinator of the trial, administered by the NCIC Clinical Trials Group. Drs. Parissenti and Guo have received royalties from commercialization activities associated with this activity. This includes the creation of RNA Diagnostics, Inc., which developed the RNA disruption assay described in this study. Drs. Parissenti and Pritzker are shareholders in RNA Diagnostics, Inc. Dr. Maureen Trudeau is the Chair of the Clinical Advisory Board for RNA Diagnostics, Inc. and has received financial compensation and shares for her roles/activities in the company. Some of the analyses described in this manuscript were performed by employees of RNA Diagnostics, Inc. (Dr. L. Pritzker and Ms. Xiaohui Wang). It should be noted that Drs. Parissenti and Guo submitted tumor RNA quality data to the NCIC Clinical Trials Group in a blinded fashion. They did not have access to the clinical response data or tumor pathology data of the patients prior to this submission. This was revealed to them and to RNA Diagnostics, Inc. only upon conclusion of the trial.
Electronic supplementary material
Below is the link to the electronic supplementary material.
10549_2015_3498_MOESM1_ESM.docx
Supplemental Table 1: Multivariate discriminant analysis revealing the ability of multiple variables (total epirubicin dose, total docetaxel dose, and the dose schedule) to significantly affect disease-free survival, when used in combination (Wald test). In single factor analysis, patients with tumor RDI values >50 had significantly greater DFS than patients with RDI ≤ 50 (Wald test). Supplementary material 1 (DOCX 14 kb)
Rights and permissions
About this article

Cite this article
Parissenti, A.M., Guo, B., Pritzker, L.B. et al. Tumor RNA disruption predicts survival benefit from breast cancer chemotherapy. Breast Cancer Res Treat 153, 135–144 (2015). https://doi.org/10.1007/s10549-015-3498-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-015-3498-9