
Abstract
Mammographic density (MD) is a strong risk factor for breast cancer, but the biological mechanism underlying this association is not clear. Current adult body mass index (BMI) is inversely associated with percent MD; however, few studies have included Hispanic women or evaluated associations with measures of body fatness earlier in life. ESMaestras was established in 2006, when 28,345 women ages ≥35 responded to a detailed questionnaire that assessed possible disease risk factors, including body fatness in childhood, adolescence, and young adulthood. In 2007, 2084 ESMaestras participants underwent a clinical examination, which included measurements of weight, height, and sitting height and a mammogram. We measured percent MD using a computer-assisted method. The current analysis includes 972 premenopausal and 559 postmenopausal women. We used multivariable linear regression to evaluate associations between measures of body size and MD, independent of current BMI. Among pre- and postmenopausal women, we observed no significant associations between body fatness during childhood, adolescence, or young adulthood and percent MD. Among postmenopausal women, we observed a modest positive association between body fatness immediately before first pregnancy and between ages 25 and 35 after adjustment for current BMI, with differences of 4.9 and 3.6 % points, respectively, in percent MD between the heaviest and leanest women (p-trend = 0.02). There were no significant associations between height, sitting height, and percent MD among pre- or postmenopausal women in multivariable models adjusting for BMI. In general, we found no clear associations between measures of body size in early life, current sitting height, or current height, and percent MD, after adjusting for current BMI, in this population of Mexican women. Our observation of a positive association between early adult body fatness (i.e., before first pregnancy and ages 25–35) and percent MD among postmenopausal women is inconsistent with prior research and requires confirmation in other studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Percent mammographic density (MD) refers to the proportion of fat and epithelial and stromal tissue in the breast and is a strong independent predictor of breast cancer risk [1]. Fat tissue is radiolucent and appears dark on a mammogram, while epithelium and stroma are both radiodense and appear light on a mammogram [2]. The mechanism by which percent MD influences cancer risk is unknown, but mammographically dense tissue may reflect epithelial proliferation and stromal fibrosis in response to growth factors [3].
Adult obesity is associated with increased risk of postmenopausal breast cancer and decreased risk of premenopausal breast cancer [4] while body fatness in childhood and adolescence has been associated with reduced risk of both pre- and postmenopausal breast cancer, independent of adult body mass index (BMI) [5–13]. These associations may be mediated, at least in part, through MD. In particular, body fatness in childhood and adolescence has been inversely associated with percent MD in adulthood [14, 15] and adjustment for percent MD attenuates associations between body fatness and breast cancer risk [16]. There is consistent epidemiologic evidence that current BMI is inversely associated with percent MD [17, 18]; however, fewer studies have focused on the role of body size earlier in life [14–16, 19–21] and none have evaluated early life body size and MD among Mexican women separately.
Given that the prevalence of overweight and obesity in Mexico has increased dramatically in recent years [22] while breast cancer mortality has risen [23], understanding the potential impact of body fatness on risk factors for breast cancer, including MD, in this population is of critical public health importance [24]. Therefore, we evaluated associations between childhood and adolescent body fatness and other anthropometric variables with MD among pre- and postmenopausal women in Mexico.
Methods
Study population
The ESMaestras cohort has been described in detail previously [25]. Briefly, ESMaestras was formed when 28,345 female teachers aged 35 years and over in the Mexican states of Jalisco and Veracruz replied to a baseline questionnaire in 2006. In 2007, a subsample of 2,084 ESMaestras teachers participated in a clinical evaluation that included an interview, anthropometry, and mammography.
For this analysis, 1,707 participants had MD measurements available. We excluded 83 women with unknown menopausal status at the time of their mammogram. We further excluded an additional 65 postmenopausal women who were on hormone replacement therapy at the time of their mammogram due to the known impact of hormone use on MD [26] as well as six women with incomplete information on BMI. Finally, we excluded 22 women who reported a prior breast cancer diagnosis. Our final analytic sample comprised 972 premenopausal and 559 postmenopausal women. Informed consent was obtained from all participants and the study was approved by the human research committee at the National Institute of Public Health in Mexico.
Body size
On the 2006 self-administered questionnaire, ESMaestras participants were asked to select the silhouette (i.e., somatotype) that best represented their body fatness at the following ages: before menarche, 2 years after menarche, between 18 and 20 years of age, just before their first pregnancy, and between 25 and 35 years of age based on a 9-level figure drawing (Fig. 1). The validity of this exposure measure has been demonstrated: among older individuals in another population of women, the correlations between recalled somatotype and BMI measured at approximately the same ages generally ranged from 0.60 to 0.75 [27]. Among pre- and postmenopausal women in this study, the correlations between the current somatotype and current BMI were high (r = 0.71 and 0.63, respectively; p < 0.01). During the clinical evaluation, trained study staff measured participants’ height, sitting height, and weight. Study personnel measured weight using an electronic digital scale (Tanita Corp, Japan) to the nearest 0.1 kg and height using a wall stadiometer (Seca Corp., Hanover, MD, USA) to the nearest centimeter. Sitting height was calculated by measuring from the head vertex to the floor and subtracting 45 cm for the height of the chair seat.

Questionnaire item on body size at various ages (ESMaestras 2006)
Mammographic density
A radiology technician performed mammography using the Giotto Image M (Internazionale Medico Scientifica, Bologna, Italy) in Jalisco and the Hologic Lorad M-III (Hologic, Bedford, MA, USA) in Veracruz. Mammograms were developed using the Agfa CP1000 (Agfa-Gevaert Group, Belgium) developer. Craniocaudal views were taken on each breast. An Astra 2400S scanner (Umax, Fremont, CA, USA) was used to digitize the mammograms. A single observer measured MD on the left craniocaudal view using Mamgr, a computer-assisted program developed at the Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine [28–30]. This thresholding software measures total area as well as total dense area on a mammogram. We calculated percent MD by dividing the dense area by the total area as well as non-dense area by subtracting the dense area from the total area. The Mamgr observer was blinded to early life body size, height, and sitting height. In a reliability study of 100 ESMaestras mammograms, the intraclass correlation coefficient between MD measurements evaluated using the Mamgr software versus the Cumulus program developed at the University of Toronto was 0.87. In 108 duplicate mammograms, the intraobserver ICC was 0.84.
Covariate data
From the 2006 self-administered questionnaire, we obtained information on age at menarche, parity, age at first birth, breastfeeding, family history of breast cancer, personal history of benign breast disease (BBD), hormonal contraceptive use, smoking status, alcohol consumption, physical activity, whether AmerIndian language was spoken by the participant or her parents, and past postmenopausal hormone (PMH) use (postmenopausal women only). Age was calculated based on the date of the clinical visit and BMI was defined as measured weight (kg) divided by measured height squared (m2) during the clinical visit or based on the 2006 self-report when clinical visit data were unavailable.
Statistical analysis
We used multivariable linear regression to estimate the associations between percent MD and height, sitting height as well as body fatness at the following ages: before menarche, 2 years after menarche, between 18 and 20 years of age, just before their first pregnancy, and between 25 and 35 years of age. In secondary analyses, we also evaluated associations of body fatness with natural logarithm-transformed absolute dense and non-dense area in separate models. For each body size measure, we categorized the exposures into four categories; extreme categories were collapsed as necessary due to small samples sizes. Separate analyses were performed for pre- and postmenopausal women. In multivariable models, we adjusted for age (continuous), state (Veracruz, Jalisco), age at menarche (<12, 12, 13, 14+), parity (nulliparous, 1, 2, 3, 4+), age at first birth (<25, 25+), breastfeeding (never, <12 months, 12+ months), family history of breast cancer (no, yes), history of BBD (no, yes), hormonal contraceptive use (never, ever), smoking status (never, past, current), alcohol consumption (none, any), physical activity (low, medium, high), whether an AmerIndian language were spoken by the participant or her parents (no, yes), and, among postmenopausal women, past PMH use (no, yes). Missing indicators were included as appropriate. In our final models, we additionally adjusted for current BMI (continuous) because our primary interest was the association of early life body size with MD, independent of current BMI. Results from multivariable models without current BMI were generally similar to those from models that adjusted for age and state alone, so age and state-adjusted models are not presented. To test for linear trend, we modeled categories of somatotype, height, and sitting height as an ordinal score variable; while current BMI was modeled continuously for tests of trend. To evaluate possible effect modification, we further stratified analyses by state and tested for statistical interaction by modeling the cross-product of state and somatotype as an ordinal variable (Wald test). In posthoc analyses, we also evaluated possible effect modification of the association between body fatness in young adulthood by current BMI (<30 vs. 30+ kg/m2) among postmenopausal women. All analyses were conducted using SAS version 9.2 (SAS Institute, Cary, NC, USA).
Results
Among premenopausal women, those with high percent MD were more likely to be younger, have a lower current BMI, drink alcohol, have a history of BBD, and to be a never smoker (Table 1). Among parous women, those with denser breasts were more likely to have ever breastfed. Among postmenopausal women, those with high percent MD were more likely to have a lower current BMI and have a history of BBD, but were less likely to ever have used oral contraceptives (Table 1). Overall, women from Jalisco had 5 % point higher percent MD compared to women from Veracruz, even after adjusting for known predictors of percent MD.
As expected, current BMI was strongly inversely associated with percent MD in both pre- and post-menopausal women in this study population (p-trend < 0.01; Tables 2 and 3). Among premenopausal women, there were no significant trends in the associations between body fatness at any earlier age, height, or sitting height and percent MD (Table 2). Women with the heaviest somatotypes 2 years after menarche had 3.5 % point higher percent MD compared to the leanest women, after adjusting for current BMI (difference between extreme categories: 3.5, 95 % CI: 0.37, 6.6); however, this difference was modest and there was no evidence of a linear trend (p = 0.11). Results from multivariable models that did not adjust for current BMI also suggested that body fatness between ages 25 and 35 was inversely associated with percent MD (difference between extreme categories: −3.4, 95 % CI: −5.8, −0.98; p-trend = 0.01); however, further adjustment for current BMI rendered this association null (p-trend = 0.97) (Table 2).
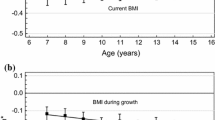
Among postmenopausal women, there was a modest positive association between body fatness immediately before first pregnancy and at ages 25–35 in multivariable models including adjustment for current BMI [difference between extreme categories: 4.9; 95 % CI: 1.1, 8.7 (p-trend = 0.02) and 3.6; 95 % CI: 0.46, 6.7 (p-trend = 0.02), respectively]. No other associations between body fatness in childhood or adolescence or current height/sitting height with percent MD were observed (Table 3).
Since the positive associations between somatotype prior to pregnancy and at ages 25–35 and percent MD among postmenopausal women were unexpected, we further stratified these analyses by current BMI to determine whether the association was modified by current body fatness. Positive associations were noted among both non-obese (i.e., BMI < 30) and obese (i.e., BMI ≥ 30 kg/m2) postmenopausal women (all p-interaction ≥ 0.05). In addition, the associations between body size at any age, height, sitting height, and percent MD did not vary significantly by state (all p-interaction ≥ 0.08).
Finally, we considered anthropometric measures in relation to absolute dense breast area and absolute non-dense breast area in separate analyses. Among premenopausal women, current BMI was positively associated with absolute dense and non-dense area (p-trend < 0.01). No associations, independent of current BMI and non-dense area, between any of the somatotype or height measures and absolute dense area were observed in premenopausal women. Similarly, in these women there were no associations between early life somatotype and absolute non-dense breast area in multivariable models that adjusted for current BMI and dense area, with the exception of somatotype at ages 25–35, for which a modest positive association was noted (p-trend = 0.04). Height was also associated with absolute non-dense area in premenopausal women (p-trend = 0.01) (Supplementary Table 1). Among postmenopausal women, current BMI was significantly positively associated with both dense and non-dense area (p-trend ≤ 0.03). Similar to our findings for percent MD, somatotype immediately before pregnancy and at ages 25–35 were positively associated with absolute dense breast area among postmenopausal women, independent of current BMI and absolute non-dense area. There were no associations between somatotype at any age, height, or sitting height and absolute non-dense area, independent of current BMI and dense area, among postmenopausal women (Supplementary Table 2).
Discussion
Consistent with the epidemiologic literature [17, 18], we observed an inverse association between current BMI and percent MD in this population of Mexican women. In addition, we did observe a modest positive association between body fatness in early adulthood (i.e., before first pregnancy and at ages 25–35) and percent MD among postmenopausal women independent of current BMI. However, there were no clear associations between measures of body size in childhood or adolescence (i.e., pre-menarche, post-menarche, or ages 18–20), current sitting height, or current height, and percent MD, after adjusting for current BMI, in pre- and postmenopausal Mexican women.
Recent evidence suggests that early life exposures may be particularly relevant for breast cancer risk [31]. Indeed, several epidemiologic studies have shown that heavier body size in childhood and adolescence is associated with reduced breast cancer risk later in life [5–13]. Several studies have also suggested that body fatness in childhood and adolescence is associated with lower percent MD later in life [14–16, 19–21]. In the US Nurses’ Health Study (NHS), for example, recalled heavier childhood body somatotype was inversely associated with percent MD in postmenopausal women [14]. The lack of association between early life body fatness and adult percent MD in EsMaestras is in contrast to most of the current literature on this topic [14–16, 19–21]; however, in a recent study of U.S. Chinese immigrant women, there also was no association between weight in childhood and adult MD [32].
There are several possible explanations for the observed null results. The majority of the previous studies included predominantly Caucasian populations and none reported associations separately for Hispanic/Mexican women. It is possible that the association between early life body size and MD differs by race/ethnicity. The well-established inverse association between current BMI and percent MD has been observed previously in Hispanic women [33, 34]; however, heavier body type in childhood and adolescence may be associated with different dietary or lifestyle factors than current BMI, which could result in different associations with adult percent MD. For example, due to secular trends and as evidenced by the rapid increase in rates of obesity in Mexico over the last 20 years [22], body fatness in early life in this study population may reflect a different composition of diet and lifestyle factors (e.g., traditional dietary habits) than current obesity in Mexico, which may reflect adoption of more Western dietary patterns, less active lifestyles, or other factors [24, 25]. Possible misclassification of body fatness in childhood and adolescence could potentially explain these results; however, correlations between recalled body shape and measured BMI were high in a prior US validation study [27] and inverse associations with childhood or adolescent somatotype and percent MD were observed among women in two prior US studies [14, 15]. Moreover, women in EsMaestras were on average younger than women in those studies, suggesting that recall, if anything, would be improved.
Our finding of a positive association between early adult body fatness (i.e., before first pregnancy and at ages 25–34) and percent MD among postmenopausal women was unexpected and, if confirmed in other studies, may suggest a possible critical period of increased susceptibility to factors that influence breast tissue composition. Alternatively, this could be a chance finding or reflect residual confounding by current BMI. Although several studies have reported inverse associations between BMI in early adulthood (e.g., ages 18–26) and percent MD later in life [14, 19, 20], we are not aware of any that have specifically assessed body fatness in the years immediately before first pregnancy. Of note, approximately half of parous women were at least 25 years of age at the time of their first pregnancy; therefore, these two somatotype variables largely reflect adiposity during the same period in life.
We found no association between current height or sitting height and percent MD among pre- or post-menopausal women. Attained height reflects in part nutritional influences and circulating levels of growth factors and insulin-like growth factor-1 (IGF-1) early in life [35, 36] while sitting height (e.g., trunk length) may reflect nutrition and energy availability up through the teen years [36–38]. However, IGF-1 has been inconsistently associated with MD in previous studies [39–45] and results from studies that have evaluated associations between height and MD have been mixed, with some reporting a positive association [15, 21, 46] and others reporting no association [19, 20, 47, 48], while no previous studies have evaluated sitting height.
While percent MD is considered a stronger predictor of breast cancer risk compared to absolute MD [49, 50], recent evidence has suggested that absolute dense area and absolute non-dense area may have independent effects on cancer risk [49, 51]. In these studies, which included predominantly Caucasian women, current BMI was inversely associated with absolute dense area of the breast and positively associated with absolute non-dense area [49, 51]. Among Mexican women, we observed positive associations of current BMI with absolute dense and non-dense breast area. This finding is consistent with the report by Tseng and Byrne in a Chinese immigrant population [52]. In the current analysis, body fatness earlier in life was not clearly associated with absolute dense or non-dense breast area, independent of current BMI. Similarly Tseng and Byrne did not observe associations of BMI at ages 20–29 with either absolute dense or non-dense breast area after adjustment for current BMI [52]. In the NHS, associations of childhood body fatness with absolute MD were reported briefly as “similar or attenuated” compared to results for percent MD [14]. Further research in this area is warranted.
There are some important potential limitations to our analysis. First, BMI is a strong negative predictor of MD; therefore, although we adjusted for current BMI in these analyses, there may be residual confounding by BMI. Second, body size in childhood and adolescence was recalled by adult women many years later. This exposure measure has been validated in another population [27] and was associated with percent MD among Caucasian women in two US studies [14, 15]; however, it is not known whether it adequately captures early life body fatness in Mexican women. Although current somatotype and BMI were significantly positively correlated in ESMaestras, there is a possibility of non-differential exposure misclassification for earlier life measures of body fatness, which could have biased our results toward the null.
Despite these potential limitations, our study also has a number of strengths. Importantly, this is the first study to evaluate associations between early life body size and MD in Mexican women. We had a relatively large sample size, which improved our statistical power to examine these associations and also allowed us to stratify by menopausal status. Because of detailed questionnaire information as well as in-person height and weight measurements, we were able to adjust for potential confounding and to evaluate these associations independent of current BMI.
In general, we observed no associations between body fatness in early life, current height, or current sitting height and percent MD in a population of Mexican women, independent of current BMI. We did observe a modest positive association between body fatness in early adulthood prior to first-term pregnancy and percent MD among postmenopausal women. This is the first study to evaluate these associations in Hispanic women, and, therefore, these findings require confirmation in other populations.
Abbreviations
- MD:
-
Mammographic density
- BMI:
-
Body mass index
- BBD:
-
Benign breast disease
- PMH:
-
Postmenopausal hormone
References
McCormack VA, dos Santos Silva I (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15(6):1159–1169. doi:10.1158/1055-9965.EPI-06-0034
Yaffe MJ (2008) Measurement of mammographic density. Breast Cancer Res 10(3):209. doi:10.1186/bcr2102
Martin LJ, Boyd NF (2008) Mammographic density. Potential mechanisms of breast cancer risk associated with mammographic density: hypotheses based on epidemiological evidence. Breast Cancer Res 10(1):201. doi:10.1186/bcr1831
World Cancer Research Fund/American Institute for Cancer Research (2007) Food, nutrition, physical activity, and the prevention of cancer: a global perspective. American Institute for Cancer Research, Washington
Palmer JR, Adams-Campbell LL, Boggs DA, Wise LA, Rosenberg L (2007) A prospective study of body size and breast cancer in black women. Cancer Epidemiol Biomarkers Prev 16(9):1795–1802. doi:10.1158/1055-9965.epi-07-0336
Michels KB, Terry KL, Willett WC (2006) Longitudinal study on the role of body size in premenopausal breast cancer. Arch Intern Med 166(21):2395–2402. doi:10.1001/archinte.166.21.2395
Magnusson CM, Roddam AW, Pike MC, Chilvers C, Crossley B, Hermon C, McPherson K, Peto J, Vessey M, Beral V (2005) Body fatness and physical activity at young ages and the risk of breast cancer in premenopausal women. Br J Cancer 93(7):817–824. doi:10.1038/sj.bjc.6602758
Baer HJ, Colditz GA, Rosner B, Michels KB, Rich-Edwards JW, Hunter DJ, Willett WC (2005) Body fatness during childhood and adolescence and incidence of breast cancer in premenopausal women: a prospective cohort study. Breast Cancer Res 7(3):R314–R325. doi:10.1186/bcr998
Weiderpass E, Braaten T, Magnusson C, Kumle M, Vainio H, Lund E, Adami HO (2004) A prospective study of body size in different periods of life and risk of premenopausal breast cancer. Cancer Epidemiol Biomarkers Prev 13(7):1121–1127
Magnusson C, Baron J, Persson I, Wolk A, Bergstrom R, Trichopoulos D, Adami HO (1998) Body size in different periods of life and breast cancer risk in post-menopausal women. Int J Cancer 76(1):29–34
London SJ, Colditz GA, Stampfer MJ, Willett WC, Rosner B, Speizer FE (1989) Prospective study of relative weight, height, and risk of breast cancer. JAMA 262(20):2853–2858
Le Marchand L, Kolonel LN, Earle ME, Mi MP (1988) Body size at different periods of life and breast cancer risk. Am J Epidemiol 28(1):137–152
Berkey CS, Frazier AL, Gardner JD, Colditz GA (1999) Adolescence and breast carcinoma risk. Cancer 85(11):2400–2409. doi:10.1002/(SICI)1097-0142(19990601)85:11<2400:AID-CNCR15>3.0.CO;2-O
Samimi G, Colditz GA, Baer HJ, Tamimi RM (2008) Measures of energy balance and mammographic density in the Nurses’ Health Study. Breast Cancer Res Treat 109(1):113–122. doi:10.1007/s10549-007-9631-7
Sellers TA, Vachon CM, Pankratz VS, Janney CA, Fredericksen Z, Brandt KR, Huang Y, Couch FJ, Kushi LH, Cerhan JR (2007) Association of childhood and adolescent anthropometric factors, physical activity, and diet with adult mammographic breast density. Am J Epidemiol 166(4):456–464. doi:10.1093/aje/kwm112
Harris HR, Tamimi RM, Willett WC, Hankinson SE, Michels KB (2011) Body size across the life course, mammographic density, and risk of breast cancer. Am J Epidemiol 174(8):909–918. doi:10.1093/aje/kwr225
Boyd NF, Lockwood GA, Byng JW, Little LE, Yaffe MJ, Tritchler DL (1998) The relationship of anthropometric measures to radiological features of the breast in premenopausal women. Br J Cancer 78(9):1233–1238
Vachon CM, Kuni CC, Anderson K, Anderson VE, Sellers TA (2000) Association of mammographically defined percent breast density with epidemiologic risk factors for breast cancer (United States). Cancer Causes Control 11(7):653–662
McCormack VA, dos Santos Silva I, De Stavola BL, Perry N, Vinnicombe S, Swerdlow AJ, Hardy R, Kuh D (2003) Life-course body size and perimenopausal mammographic parenchymal patterns in the MRC 1946 British birth cohort. Br J Cancer 89(5):852–859. doi:10.1038/sj.bjc.6601207
Jeffreys M, Warren R, Gunnell D, McCarron P, Smith GD (2004) Life course breast cancer risk factors and adult breast density (United Kingdom). Cancer Causes Control 15(9):947–955. doi:10.1007/s10522-004-2473-3
Lope V, Perez-Gomez B, Moreno MP, Vidal C, Salas-Trejo D, Ascunce N, Roman IG, Sanchez-Contador C, Santamarina MC, Carrete JA, Collado-Garcia F, Pedraz-Pingarron C, Ederra M, Ruiz-Perales F, Peris M, Abad S, Cabanes A, Pollan M (2011) Childhood factors associated with mammographic density in adult women. Breast Cancer Res Treat. doi:10.1007/s10549-011-1664-2
Gutierrez JP, Rivera-Dommarco J, Shamah-Levy T, Villalpando-Hernandez S, Franco A, Cuevas-Nasu L, Romero-Martinez M, Hernandez-Avila M (2012) Encuesta nacional de salud y nutricion 2012. Instituto Nacional de Salud Publica, Cuernavaca
Chavarri-Guerra Y, Villarreal-Garza C, Liedke PE, Knaul F, Mohar A, Finkelstein DM, Goss PE (2012) Breast cancer in Mexico: a growing challenge to health and the health system. Lancet Oncol 13(8):e335–e343. doi:10.1016/S1470-2045(12)70246-2
Romieu I, Lajous M (2009) The role of obesity, physical activity and dietary factors on the risk for breast cancer: Mexican experience. Salud Publica Mex 51(Suppl 2):s172–s180
Romieu I, Escamilla-Nunez MC, Sanchez-Zamorano LM, Lopez-Ridaura R, Torres-Mejia G, Yunes EM, Lajous M, Rivera-Dommarco JA, Lazcano-Ponce E (2011) The association between body shape silhouette and dietary pattern among Mexican women. Public Health Nutr 15(1):116–125. doi:10.1017/s1368980011001182
Martin LJ, Minkin S, Boyd NF (2009) Hormone therapy, mammographic density, and breast cancer risk. Maturitas 64(1):20–26. doi:10.1016/j.maturitas.2009.07.009
Must A, Willett WC, Dietz WH (1993) Remote recall of childhood height, weight, and body build by elderly subjects. Am J Epidemiol 138(1):56–64
Byng JW, Boyd NF, Fishell E, Jong RA, Yaffe MJ (1994) The quantitative analysis of mammographic densities. Phys Med Biol 39(10):1629–1638
Ursin G, Astrahan MA, Salane M, Parisky YR, Pearce JG, Daniels JR, Pike MC, Spicer DV (1998) The detection of changes in mammographic densities. Cancer Epidemiol Biomarkers Prev 7(1):43–47
Torres-Mejia G, De Stavola B, Allen DS, Perez-Gavilan JJ, Ferreira JM, Fentiman IS, Dos Santos Silva I (2005) Mammographic features and subsequent risk of breast cancer: a comparison of qualitative and quantitative evaluations in the Guernsey prospective studies. Cancer Epidemiol Biomarkers Prev 14(5):1052–1059. doi:10.1158/1055-9965.EPI-04-0717
Colditz GA, Frazier AL (1995) Models of breast cancer show that risk is set by events of early life: prevention efforts must shift focus. Cancer Epidemiol Biomarkers Prev 4(5):567–571
Tseng M, Olufade TO, Evers KA, Byrne C (2011) Adolescent Lifestyle Factors and Adult Breast Density in U.S. Chinese Immigrant Women. Nutr Cancer 63(3):342–349. doi:10.1080/01635581.2011.535955
Caire-Juvera G, Arendell LA, Maskarinec G, Thomson CA, Chen Z (2008) Associations between mammographic density and body composition in Hispanic and non-Hispanic white women by menopause status. Menopause 15(2):319–325. doi:10.1097/gme.0b013e3181405b8a
Gapstur SM, Lopez P, Colangelo LA, Wolfman J, Van Horn L, Hendrick RE (2003) Associations of breast cancer risk factors with breast density in Hispanic women. Cancer Epidemiol Biomarkers Prev 12(10):1074–1080
Rogers I, Metcalfe C, Gunnell D, Emmett P, Dunger D, Holly J (2006) Insulin-like growth factor-I and growth in height, leg length, and trunk length between ages 5 and 10 years. J Clin Endocrinol Metab 91(7):2514–2519. doi:10.1210/jc.2006-0388
Wadsworth ME, Hardy RJ, Paul AA, Marshall SF, Cole TJ (2002) Leg and trunk length at 43 years in relation to childhood health, diet and family circumstances; evidence from the 1946 national birth cohort. Int J Epidemiol 31(2):383–390
Lawlor DA, Okasha M, Gunnell D, Smith GD, Ebrahim S (2003) Associations of adult measures of childhood growth with breast cancer: findings from the British Women’s Heart and Health Study. Br J Cancer 89(1):81–87. doi:10.1038/sj.bjc.66009726600972
Gunnell D (2002) Can adult anthropometry be used as a ‘biomarker’ for prenatal and childhood exposures? Int J Epidemiol 31(2):390–394
Rice MS, Tworoger SS, Rosner BA, Pollak MN, Hankinson SE, Tamimi RM (2012) Insulin-like growth factor-1, insulin-like growth factor-binding protein-3, growth hormone, and mammographic density in the Nurses’ Health Studies. Breast Cancer Res Treat. doi:10.1007/s10549-012-2303-2
Byrne C, Colditz GA, Willett WC, Speizer FE, Pollak M, Hankinson SE (2000) Plasma insulin-like growth factor (IGF) I, IGF-binding protein 3, and mammographic density. Cancer Res 60(14):3744–3748
Aiello EJ, Tworoger SS, Yasui Y, Stanczyk FZ, Potter J, Ulrich CM, Irwin M, McTiernan A (2005) Associations among circulating sex hormones, insulin-like growth factor, lipids, and mammographic density in postmenopausal women. Cancer Epidemiol Biomarkers Prev 14(6):1411–1417. doi:10.1158/1055-9965
Diorio C, Berube S, Byrne C, Masse B, Hebert-Croteau N, Yaffe M, Cote G, Pollak M, Brisson J (2006) Influence of insulin-like growth factors on the strength of the relation of vitamin D and calcium intakes to mammographic breast density. Cancer Res 66(1):588–597. doi:10.1158/0008-5472.can-05-1959
dos Santos Silva I, Johnson N, De Stavola B, Torres-Mejia G, Fletcher O, Allen DS, Allen NE, Key TJ, Fentiman IS, Holly JM, Peto J (2006) The insulin-like growth factor system and mammographic features in premenopausal and postmenopausal women. Cancer Epidemiol Biomarkers Prev 15(3):449–455. doi:10.1158/1055-9965
Bremnes Y, Ursin G, Bjurstam N, Rinaldi S, Kaaks R, Gram IT (2007) Insulin-like growth factor and mammographic density in postmenopausal Norwegian women. Cancer Epidemiol Biomarkers Prev 16(1):57–62. doi:10.1158/1055-9965
Maskarinec G, Takata Y, Chen Z, Gram IT, Nagata C, Pagano I, Hayashi K, Arendell L, Skeie G, Rinaldi S, Kaaks R (2007) IGF-I and mammographic density in four geographic locations: a pooled analysis. Int J Cancer 121(8):1786–1792. doi:10.1002/ijc.22834
Dorgan JF, Klifa C, Shepherd JA, Egleston BL, Kwiterovich PO Jr, Himes JH, Gabriel KP, Horn LV, Snetselaar LG, Stevens VJ, Barton BA, Robson AM, Lasser NL, Deshmukh S, Hylton NM (2012) Height, adiposity and body fat distribution and breast density in young women. Breast Cancer Res 14(4):R107. doi:10.1186/bcr3228
Sung J, Song YM, Stone J, Lee K, Kim SY (2010) Association of body size measurements and mammographic density in Korean women: the Healthy Twin study. Cancer Epidemiol Biomarkers Prev 19(6):1523–1531. doi:10.1158/1055-9965
Riza E, Remoundos DD, Bakali E, Karadedou-Zafiriadou E, Linos D, Linos A (2009) Anthropometric characteristics and mammographic parenchymal patterns in post-menopausal women: a population-based study in Northern Greece. Cancer Causes Control 20(2):181–191. doi:10.1007/s10552-008-9232-8
Pettersson A, Hankinson SE, Willett WC, Lagiou P, Trichopoulos D, Tamimi RM (2011) Nondense mammographic area and risk of breast cancer. Breast Cancer Res 13(5):R100. doi:10.1186/bcr3041
Pettersson A, Tamimi RM (2012) Breast fat and breast cancer. Breast Cancer Res Treat 135(1):321–323. doi:10.1007/s10549-012-2186-2
Lokate M, Peeters PH, Peelen LM, Haars G, Veldhuis WB, van Gils CH (2011) Mammographic density and breast cancer risk: the role of the fat surrounding the fibroglandular tissue. Breast Cancer Res 13(5):R103. doi:10.1186/bcr3044
Tseng M, Byrne C (2011) Adiposity, adult weight gain and mammographic breast density in US Chinese women. Int J Cancer 128(2):418–425. doi:10.1002/ijc.25338
Acknowledgments
This work was supported by the American Institute for Cancer Research (05B047), CONACYT (14429), Ministry of Health Mexico, Avon Cosmetics, Fundación Banorte, Fundación Gruma, Bicentennial Fund Traveling Fellowship, Harvard School of Public Health Department of Epidemiology, and National Institutes of Health, National Cancer Institute (T32 CA09001, R25 CA098566).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Megan S. Rice and Kimberly A. Bertrand contributed equally to the manuscript and should be considered co-first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Rice, M.S., Bertrand, K.A., Lajous, M. et al. Body size throughout the life course and mammographic density in Mexican women. Breast Cancer Res Treat 138, 601–610 (2013). https://doi.org/10.1007/s10549-013-2463-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-013-2463-8