
Abstract
Klotho is a single pass transmembrane protein, associated with premature aging. We identified tumor suppressor activities for klotho, associated with reduced expression in breast cancer. We now aimed to analyze klotho expression in early stages of breast tumorigenesis and elucidate mechanisms leading to klotho silencing in breast tumors. We studied klotho expression, using immunohistochemistry, and found high klotho expression in all normal and mild hyperplasia samples, whereas reduced expression was associated with moderate and atypical ductal hyperplasia. Promoter methylation and histone deacetylation were studied as possible mechanisms for klotho silencing. Using bisulfite sequencing, and methylation-specific PCR, we identified KLOTHO promoter methylation in five breast cancer cell lines and in hyperplastic MCF-12A cells, but not in the non-tumorous mammary cell line HB2. Importantly, methylation status inversely correlated with klotho mRNA levels, and treatment of breast caner cells with 5-aza-2-deoxycytidine elevated klotho expression by up to 150-fold. KLOTHO promoter methylation was detected in 8/23 of breast cancer samples but not in normal breast samples. Chromatin immunoprecipitation revealed that in HB2 KLOTHO promoter was enriched with AcH3K9; however, in breast cancer cells, H3K9 was deacetylated, and treatment with the histone deacetylase inhibitor suberoylanilide bishydroxamide (SAHA) restored H3K9 acetylation. Taken together, these data indicate loss of klotho expression as an early event in breast cancer development, and suggest a role for DNA methylation and histone deacetylation in klotho silencing. Klotho expression and methylation may, therefore, serve as early markers for breast tumorigenesis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The KLOTHO gene was first identified as a potent suppressor of aging [1]. Mice homozygous for a mutated KLOTHO allele exhibit a syndrome resembling human aging, while klotho over-expression extended mice lifespan [1, 2]. Klotho is a 1012-amino acid single pass transmembrane protein [1, 3–5], and its extracellular domain can be cleaved, shed into the serum, and it can act as a circulating hormone [1, 5–8]. Several activities of klotho have been described to date, including retention of the calcium channel TRPV5 [9], binding to fibroblast growth factor receptors (FGFR) 1–4, and acting as a co-receptor for FGF23 [10, 11]. Klotho is also a potent inhibitor of the insulin receptor (IR) and the IGF-1 receptor (IGF-1R) [10]. Since the IGF-1 and the insulin pathways play important roles in breast cancer pathogenesis [12, 13], we recently investigated klotho expression and activities in human breast cancer [14]. High klotho expression was found in normal breast samples, but very low expression was observed in invasive breast cancer. Moreover, over-expression of klotho reduced proliferation and inhibited ligand-dependent activation of the IGF-1 and insulin pathways in breast cancer cells. Furthermore, using a genetic screen, we identified a klotho variant as a risk modifier for breast cancer in BRCA1-carriers [15]. The role of klotho as a tumor suppressor was further established recently in cervical carcinoma, lung cancer, and melanoma [16–20].
Epigenetic alterations, namely, DNA methylation and histone modifications, play an important part in silencing of tumor suppressor genes [21]. Aberrant DNA methylation is mediated by DNA-cytosine methyltransferase (DNMTs) and is often found in CpG-rich sites, known as CpG islands, located in the promoter region of many genes. Post-translational histone modification is another mechanism that can modulate chromatin structure to regulate gene expression. DNA methylation is often associated with specific histone modifications that can cooperatively affect chromatin structure to silence gene expression. Thus, activation of either of these mechanisms can lead to inhibition of transcription and inactivation of tumor suppressor genes [21, 22]. Mechanisms underlying klotho silencing in breast cancer have not been elucidated yet. We have previously performed a pharmacological-based global screen for epigenetically silenced tumor suppressor genes in MCF-7 and MDA-MB-231 breast cancer cells [23, 24], and the KLOTHO gene was among the ones elevated following re-methylating treatment. KLOTHO promoter region is rich in CpG islands, suggesting hypermethylation as a possible mechanism for its silencing in breast cancer.
In the present study, we investigated klotho expression in breast tissues, and identified reduced klotho expression already at hyperplastic breast lesions. Accordingly, while KLOTHO promoter methylation was identified in all breast cancer cell lines tested, as well as in a ductal hyperplasia cell line, no methylation was observed in a non-tumorigenic mammary cell line. Moreover, promoter methylation was identified in 30% of breast cancer tumor samples, while no methylation was detected in normal breast. Finally, deacetylation of histone 3 was observed in breast cancer cell lines. Thus, our results identify klotho as an epigenetically silenced tumor suppressor gene in breast cancer.
Materials and methods
Chemicals, antibodies, and constructs
5-Aza-2-deoxycytidine (5-AZA) was obtained from Sigma (St. Louis, MO). Suberoyl anilide bishydroxamide (SAHA) was generously provided by V.M. Richon (Aton Pharma, Tarrytown, NY, USA).
Cells
Breast cancer cell lines were obtained from the American Type Culture Collection (Manassas, VA).
Patients samples
All samples were obtained after IRB approval. Immunohistochemistry (IHC) analysis was conducted at the Pathology Department of Cedars-Sinai Medical Center, LA, CA. Samples were obtained from 39 patients as follows: 13 had reduction mammoplasty for macromastia, seven underwent excisions for benign conditions (one fibroadenoma, one intraductal papilloma, five fibrocystic changes), six underwent excision for DCIS (ductal carcinoma in situ), and 13 underwent excisions/mastectomies for infiltrating ductal carcinoma. Normal tissues, ducts with usual ductal hyperplasia, and atypical ductal hyperplasia (ADH) away from the carcinoma were evaluated with klotho immunostains. The carcinomas in these cases were not evaluated. Tissues were collected from specimens to be discarded after routine surgical pathology diagnosis.
For DNA analysis
From Asaf-Harofeh Medical Center, seven frozen and fresh samples from breast tumors and their adjacent normal tissues, and three fresh normal breast tissues from reduction mammoplasties, were collected. Sixteen breast tumors and four normal adjacent tissues were obtained from Cedars-Sinai Medical Center. These samples were obtained, after informed consent, from surgically resected primary breast tumors of women diagnosed at Tarzana Medical Center (Tarzana, CA) from 2002 to 2004. All samples were examined histologically for the presence of tumor cells. Median age of these patients was 51, and 17 of the 23 tumor samples expressed the estrogen receptor (ER). Peripheral blood cells were obtained from healthy volunteers.
Data collected are presented here in line with the REMARK criteria [25].
IHC analysis
IHC analysis was performed as described [14]: five-micron sections were deparaffinized through xylenes and graded ethyl alcohols and then rinsed in water, followed by quenching of endogenous peroxidase activity by a 30% solution of hydrogen peroxidase in methanol for 10 min. Antigen retrieval was performed by boiling the slides in 0.01 mol/l sodium citrate buffer pH 6.0 in a microwave oven at maximum power for 1 min and at 20% power for 9 min, followed by a 20-min cool-down time and rinses in wash buffer. The slides were then incubated for 1 h with the anti-klotho antibody (Calbiochem, BD Biosciences, San Jose, CA, 1:100 dilution) after blocking with normal serum for 30 min, reacted with the secondary antibody for 30 min, and signal amplification and chromogen development were conducted for 30 min each. The stained slides were counterstained with hematoxylin and mounted. Antibody staining specificity was determined by staining kidney sections, and each run included appropriate positive and negative control slides. Staining was scored by percent of positive tumor cells and staining intensity.
Quantitative reverse transcription-PCR (Q-RT-PCR)
Total RNA was extracted using the RNA isolation kit (Sigma) and processed to cDNA with RevertAid (Fermentas, Vilnius, Lithuania). Primers were designed using Primer Express (Applied Biosystems, Foster City, CA) and synthesized by IDT (Coralville, IA). Klotho-specific primers were: Forward 5′-GCTCTCAAAG CCCACATACTG, reverse 5′-GCAGCATAACGATAGAGGCC. β-actin primers: Forward 5′-GGAGCCCGTCGGTAATTTTAA reverse 5′-TCTGCATGTGCGGTTGGTT. Amplification reactions were performed with Platinum qPCR SuperMix (Invitrogen, Carlsbad, CA) in triplicates in an ABI Prism™ 7000 (Applied Biosystems) as previously described [24]. PCR conditions: 2 min at 50°C, 2 min at 95°C, followed by 40 cycles of 15 s at 95°C and 45 s at 60°C.
Demethylation treatment, bisulfite sequencing, and methylation-specific PCR (MSP)
DNA was extracted from cell lines and clinical samples using Wizard® SV Genomic DNA isolation kit (Promega, Madison, WI). Bisulfite modification of DNA was performed using the EZ DNA Methylation Kit (Zymo Research, CA) according to the manufacturer’s recommendations. Methylation-specific primers, designed by MethPrimer (http://www.urogene.org/methprimer/) were used to amplify and clone a 75-bp region of KLOTHO promoter. Primers used: Forward GTTTTAGGGTTGTTTTTAGAGGA reverse AAAAAACACCTATTTCTCCCAACT. For sequence analysis, the PCR products were subcloned using InsTAclone™ PCR Cloning Kit (Fermentas, Lithuania). For quantitative methylation-specific PCR (Q-MSP): Two sets of specific primers were manually designed (methylated or unmethylated) for KLOTHO gene promoter, according to the recommendations of the MethPrimer program (www.ucsf.edu/urogene/methprimer/index.html) but no CpGs between the primers were allowed thus guaranteeing a uniform melting curve for each amplicon. Primer sequences are forward unmethylated GTGTTTGTTGGAGTGGCTGT; reverse unmethylated CACCATAAACATCCTACAAACAC; forward methylated CGTTTGTTGGAGCGGTTGC; reverse methylated GCCATAAACGTCCTACAAACG. The PCR mix contained 5 ng of sodium bisulfite-treated DNA, 200 nM of each primer, and SYBR Premix Ex Taq (Takara Bio Inc., Shiga, Japan) in 10 μl final reaction volume. Real-time PCR amplification was performed for 2 min at 95°C followed by 35 cycles of 1 s at 95°C and 30 s at 60°C; subsequently, a melting curve program was conducted (Rotor Gene 3000, Corbett, Australia). Human sperm DNA and DNA treated with SssI CpG methyltransferase (NEB, Ipswich, MA, USA) were used as nonmethylated and methylated DNA controls, respectively. True amplification products were recognized by their complete overlap with the control melting curves. The CT (cycle of threshold) of the methylated and the unmethylated products were used to calculate percent of methylation for each gene.
Breast cancer cell lines were treated with 5-AZA (5 μM for 3 days) and SAHA (2 μM for 24 h) either alone or in combination. For combined treatment, SAHA was added for the last 24 h of the experiment. Mock-treated cells were cultured similarly and used as a control.
Chromatin immunoprecipitation assay (CHIP)
Acetylated histone 3 CHIP was performed essentially as described [26]. HB2, MCF-7, and MDA-MB 231 cells were treated with SAHA, or control vehicle, for 24 h; then cells were collected by trypsinization. Cells were crosslinked with 1% formaldehyde for 10 min at room temperature followed by quenching with 0.125 M glycine. Crosslinked cells were washed twice with ice-cold PBS, once with lysis buffer 1 (50 mM Hepes pH 7.5, 140 mM NaCl, 1 mM EDTA, 10% glycerol, 0.5% Nonidet P-40, 0.25% Triton X-100, and protease inhibitors (Complete, Roche, Basel)) and once with lysis buffer 2 (200 mM NaCl, 1 mM EDTA pH 8, 0.5 mM EGTA, 10 mM Tris pH 8, and protease inhibitors). Washings with buffers 1 and 2 consisted of a 10-min rotation and a 7-min spin at 500×g (1,200 rpm) at 4°C. The resulting nuclei were lysed with ChIP lysis buffer (1% SDS, 10 mM EDTA, and 50 mM Tris pH 8.1) and sonicated (25 μg). Sonicated chromatin was diluted 10 times with ChIP dilution buffer (0.01% SDS, 1.1% Triton X-100, 1.2 mM EDTA, 16.7 mM Tris pH 8.1, and 167 mM NaCl) incubated overnight at 4°C with 10 μg of anti-acetyl-histone H3 antibody (Millipore, Billerica, MA) which was preincubated with 100 μl of sheep anti-rabbit IgG coated Dynabeads (M-280, Invitrogen). Following incubation, the beads were washed 5–8 times with RIPA buffer and once with TE followed by elution, decrosslinking, and proteinase K treatment. DNA was purified by phenol–chloroform extraction and ethanol precipitation. Analyses of specific loci were performed by Q-PCR (ABI Prism™ 7000, Applied Biosystems, Foster City, CA). Primer sequences designed for two different KLOTHO promoter regions were (Fig. 2a) set 1, Forward TTTCGGCCAGTCCCTAATTG, reverse CCACTCGGAGGCCCAAA; and set 2, forward TTTCCCTCCACAGCTCAGAT, reverse CCTTTCGGCTCTGACTTAGC. PCR conditions: 55°C for 2 min, 95°C for 2 min, and 40 cycles of 95°C for 15 s. Experiments were done in duplicates.
Statistical analysis
Each experiment was performed at least three times. The data were expressed as the mean ± SD or SE. Statistical significance was assessed by Student’s t test. A P value of <0.05 was considered statistically significant.
Results
Expression of klotho in breast tissue
We have shown before that klotho expression is high in normal breast, but its expression is reduced in 80% of premalignant DCIS lesions and in 78% of malignant IDC tissues compared to normal adjacent tissue [14]. We also showed that klotho expression was reduced in breast cell lines, as early as in the hyperplasia-derived cell line MCF-12A [14]. The low expression of klotho already in DCIS led us to study klotho expression in earlier lesions, namely, hyperplastic breast samples. We conducted IHC of 39 normal breast, and 23 samples of hyperplasia (two mild hyperplasia, 18 moderate to florid hyperplasia, and three ADH). Klotho staining was high in all normal tissues studied and in the mild hyperplasia (Fig. 1). However, klotho expression was reduced in 33% of moderate to florid hyperplasia, especially in focal areas, and in all ADH samples (Fig. 1).

Klotho expression is down-regulated in atypical breast hyperplasia. Immunohistochemical staining of klotho in mammary tissues. Depicted high klotho expression in normal and mild hyperplasia samples and reduced expression in moderate hyperplasia and atypical ductal hyperplasia (ADH). All at ×200 magnification
Methylation of the KLOTHO promoter in breast cancer cell lines
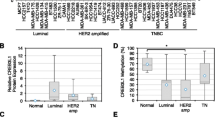
As klotho is a potent tumor suppressor in breast cancer [14], and as promoter hypermethylation of tumor suppressor is proposed as one of the mechanisms responsible for tumor suppression silencing during tumorigenesis, we studied KLOTHO promoter methylation in breast cancer. KLOTHO promoter region (including exon 1) contains a 1439-bp-long CpG island which spans from –677 to +762 relative to the start ATG codon. We conducted bisulfite sequencing and analyzed the methylation status of the region −268 to −342, spanning eight CpG dinucleotides (Fig. 2a), in HB2 (non-tumorous), MCF-12A (hyperplastic), MCF-7, MDA-MB-231, Hs578T, T47D, and BT474 (breast cancer cell lines). These cells represent various subtypes of breast cancer and differ in the expression patterns of the estrogen and progesterone receptors as well as Her2 [27]. At least five clones were analyzed for each cell line (Fig. 2b). While no significant methylation of the KLOTHO promoter was noted in HB2 cells (only one methylated CpG site in all alleles tested), extensive methylation was noted in all other cell lines, including MCF12A hyperplastic breast cell line. The highest methylation was observed in MCF-7 and T47D. These results were further validated using Q-MSP directed at a different site of the promoter, in MCF-7, MDA-MB-231, and HB2 cells (Fig. 2c). Similar to direct sequencing, no methylation was noted in HB2 cells, while KLOTHO promoter in MCF-7 cells was fully methylated, and 87% methylation was detected in MDA-MB-231 cells.

Methylation status of KLOTHO promoter in breast cancer cell lines. a Schematic presentation of KLOTHO promoter region. CpG island region is located between –677 and +762, and the regions used for bisulfite sequencing (the nucleotide sequence is below, and the eight CpG sites are indicated in bold) and MSP are indicated, as well as sequences amplified for ChIP analysis. b,c,d For methylation analysis, DNA was extracted from HB2, MCF12A, MCF-7, T47D, MDA-MB-231, Hs578T, and BT474 cells, treated with bisulfite, and the promoter region was amplified using PCR to the indicated regions. For bisulfate sequencing (b), the PCR product was cloned and sequenced. At least five alleles of each cell line were sequenced. Methylated cytosines in CpGs are marked as closed squares, and unmethylated as open squares. The results are averaged in (d). c For Q-MSP, bisulfate DNA, from HB2, MCF-7, and MDA-MB-231, was used as a template for Q-PCR, with two sets of primers, amplifying either methylated or unmethylated genomic DNA (see “Materials and methods” section). Results show amplification curves and percentage of methylated or unmethylated DNA using each set. Inverse correlation between promoter methylation (d) and klotho expression (e). Klotho mRNA levels were determined by Q-RT-PCR in the indicated breast cancer cell lines. The results are expressed in arbitrary units as a ratio of the target gene/β-actin transcripts (each value represents the mean of three measurements of the sample)
Importantly, DNA methylation (average, depicted in Fig. 2d) correlated with klotho mRNA expression, with the highest expression in HB2, and reduced expression in all other cell lines (Fig. 2e).
Methylation of the KLOTHO promoter in clinical breast cancer samples
We then studied KLOTHO promoter methylation in breast cancer samples. We examined 23 breast tumors, 11 normal breast adjacent to tumor, and three normal primary breast epithelial cells (organoids). Q-MSP analysis showed KLOTHO promoter methylation in one third (8/23) of clinical breast cancer samples, while no methylation was detected in normal breast samples (adjacent to tumor or in normal breast) (Table 1; P = 0.014 for the comparison between tumors and normal samples). No methylation was detected in white blood cells (WBC, n = 9), suggesting that the source of hypermethylation observed in tumors is indeed the tumor cells.
5-Aza-deoxycytidine elevates klotho expression in breast cancer cells
Treatment of cells with 5-aza-deoxycytidine (5-AZA) eliminates methylation of cytosine residues, thus elevating expression of genes silenced due to promoter hypermethylation [23, 28]. Treatment of MCF-7 and T47D cells with 5-AZA resulted in 150-fold increase in klotho mRNA expression, and tenfold increase was noted in MDA-MB-231 (Fig. 3). Only minimal effect was noted in Hs578T, MDA-MB-468, and HB2 cells (twofold increase or less).

Klotho expression is elevated following demethylation treatment. Breast cell lines were either mock-treated or treated with 5-AZA (5 μM for 3 days) or with SAHA (2 μM), or combined (SAHA added during the last 24 h of culture). Following treatment, RNA was isolated and was reverse transcribed. Klotho expression levels were determined by Q-RT-PCR. The experiments were repeated at least three times, and the results of a representative experiment are shown
Histone 3 deacetylation in breast cancer cell lines
As KLOTHO hypermethylation was detected in only 1/3 of breast tumors, we examined histone deacetylation as an additional mechanism responsible to klotho silencing in breast cancer. We conducted ChIP of acetylated histone 3 at lysine 9 (AcH3K9) in MCF-7, MDA-MB-231, and HB2 cells and found threefold enrichment of AcH3K9 at the promoter region of klotho in HB2 than that in MCF-7 and tenfold that in MDA-MB-231 cells (Fig. 4a). Next, we treated cells with SAHA, an inhibitor of histone deacetylase (HDAC), which induces expression of genes silenced by histone deacetylation [23, 28, 29]. In MCF-7 and MDA-MB-231 cells, following SAHA treatment, significant enrichment of the promoter region was observed (2.5-fold and 16-fold, respectively; Fig 4b). On the other hand, in HB2 cells, no enrichment following SAHA treatment was observed, indicating deacetylated H3K9 in MCF-7 and MDA-MB-231 cell lines, but not in the non-tumorous HB2 breast cells.

H3K9 is deacetylated in breast cancer cell lines. a Q-PCR results of KLOTHO promoter region (as shown in Fig. 2a, and “Materials and methods” section) of HB2, MCF-7, and MDA-MB-231 cell lines, from ChIP assay using anti-acetylated H3 antibodies. Similar findings were observed in two other experiments. b HB2, MCF-7, and MDA-MB-231 cell lines were treated for 24 h with SAHA or control and ChIP assay was conducted. Similar findings were observed in two other experiments
SAHA treatment elevated klotho mRNA expression only in MDA-MB-231 (Fig. 3). However, SAHA induces global changes in the expression of many genes [23], and its effects on klotho mRNA levels may be indirect and non-specific.
Discussion
Our observations indicate decreased klotho expression as an early event in the development of breast cancer. We identified two mechanisms underlying the decreased expression of klotho: hypermethylation of KLOTHO promoter, and deacetylation of histones attached to the promoter.
Benign breast disease (BBD) is associated with increased breast cancer risk [30]. Thus, proliferative lesions without atypia are associated with a 1.5- to 2-fold increased risk, whereas atypical hyperplasias are associated with a 4- to 5-fold increased breast cancer risk. To date, there are no reliable markers to predict whether hyperplasia, or ADH, will proceed to carcinoma. While methylation of various genes has been suggested as possible predictor markers for cancer development, more reliable predictive markers are needed [31]. We observed gradual decrease of klotho expression from normal breast tissues to hyperplasia, DCIS, and invasive cancer. Further studies are needed to test the role of klotho expression as a possible predictive marker for cancer development in patients suffering from BBD.
Hypermethylation of the promoter region is often involved in the silencing of tumor suppressor genes. Examples of genes that have been reported to be silenced by aberrant methylation in breast cancer include BRCA1, p16 and PGDH genes [28, 32, 33]. KLOTHO promoter region contains a CpG island spanning from −650 to +850, relative to ATG codon. We established the role of promoter hypermethylation in silencing the expression of klotho by means of direct methylation analysis (bisulfate sequencing of a promoter region, MSP directed at a different region), as well as by observing upregulation of klotho mRNA levels following treatment with the demethylating agent 5-AZA.
Klotho expression is reduced in about 80% of breast cancer samples [14], whereas methylation of KLOTHO promoter occurs in one third of breast cancer samples, suggesting additional mechanisms responsible for klotho down regulation in breast cancer. An additional mechanism responsible for silencing tumor suppressor genes in tumor cells is deacetylation of lysine residues of histones attached to promoter regions of tumor suppressor genes [22]. Indeed, ChIP analysis revealed that in breast cancer cells, but not in the non-tumorous breast cell line HB2, treatment with SAHA significantly enriched AcH3K9 in KLOTHO promoter region. This implies deacetylation of histones occupying KLOTHO promoter in breast cancer cells and suggest histone modifications as an additional mechanism involved in silencing KLOTHO in cancer. Our results are supported by a recent study showing KLOTHO promoter methylation and H3K9 deacetylation in cervical carcinoma [18].
The KLOTHO gene is located on chromosome, 13q12, a region that is deleted in various malignancies and is termed Deleted in Pancreatic Carcinoma (DPC1 and DPC2) [34]. This region contains known tumor suppressor genes, including, BRCA2 and RB and is suspected to hold additional tumor suppressors. Indeed, recent data indicate Brushes-1 and Aprin as potential tumor suppressor genes in this region [35, 36]. Previously, we have shown that klotho has several tumor suppressor characteristics, including reduced expression in breast tumors compared to normal breast, growth inhibitory effects on breast cancer cell lines [14], and a KLOTHO SNP that acts as a modifier gene in BRCA1 mutation carriers [15]. In this study, we show that two other characteristics of tumor suppressors are applied, i.e., reduced expression by hypermethylation of the promoter region and histone deacetylation.
In summary, this study has found that klotho levels were decreased at very early stages of breast tumorigenesis, and identified KLOTHO promoter methylation and histone modifications in breast cancer cell lines and tumors. These results suggest that klotho is a predictive marker for breast tumorigenesis.
References
Kuro-o M, Matsumura Y, Aizawa H, Kawaguchi H, Suga T, Utsugi T, Ohyama Y, Kurabayashi M, Kaname T, Kume E et al (1997) Mutation of the mouse klotho gene leads to a syndrome resembling ageing. Nature 390:45–51
Kurosu H, Yamamoto M, Clark JD, Pastor JV, Nandi A, Gurnani P, McGuinness OP, Chikuda H, Yamaguchi M, Kawaguchi H et al (2005) Suppression of aging in mice by the hormone Klotho. Science 309:1829–1833
Ito S, Kinoshita S, Shiraishi N, Nakagawa S, Sekine S, Fujimori T, Nabeshima Y (2000) Molecular cloning and expression analyses of mouse [beta]klotho, which encodes a novel Klotho family protein. Mech Develop 98:115–119
Matsumura Y, Aizawa H, Shiraki-Iida T, Nagai R, Kuro-o M, Nabeshima Y (1998) Identification of the human klotho gene and its two transcripts encoding membrane and secreted klotho protein. Biochem Biophys Res Commun 242:626–630
Shiraki-Iida T, Aizawa H, Matsumura Y, Sekine S, Iida A, Anazawa H, Nagai R, Kuro-o M, Nabeshima Y (1998) Structure of the mouse klotho gene and its two transcripts encoding membrane and secreted protein. FEBS Letters 424:6–10
Imura A, Iwano A, Tohyama O, Tsuji Y, Nozaki K, Hashimoto N, Fujimori T, Nabeshima Y (2004) Secreted Klotho protein in sera and CSF: implication for post-translational cleavage in release of Klotho protein from cell membrane. FEBS Letters 565:143–147
Chen C-D, Podvin S, Gillespie E, Leeman SE, Abraham CR (2007) Insulin stimulates the cleavage and release of the extracellular domain of Klotho by ADAM10 and ADAM17. Proc Natl Acad Sci 104:19796–19801
Ohyama Y, Kurabayashi M, Masuda H, Nakamura T, Aihara Y, Kaname T, Suga T, Arai M, Aizawa H, Matsumura Y et al (1998) Molecular cloning of rat klotho cDNA: markedly decreased expression of klotho by acute inflammatory stress. Biochem Biophys Res Commun 251:920–925
Cha S-K, Ortega B, Kurosu H, Rosenblatt KP, Kuro-o M, Huang C-L (2008) Removal of sialic acid involving Klotho causes cell-surface retention of TRPV5 channel via binding to galectin-1. Proc Natl Acad Sci 105:9805–9810
Kurosu H, Ogawa Y, Miyoshi M, Yamamoto M, Nandi A, Rosenblatt KP, Baum MG, Schiavi S, Hu M-C, Moe OW et al (2006) Regulation of fibroblast growth factor-23 signaling by Klotho. J Biol Chem 281:6120–6123
Urakawa I, Yamazaki Y, Shimada T, Iijima K, Hasegawa H, Okawa K, Fujita T, Fukumoto S, Yamashita T (2006) Klotho converts canonical FGF receptor into a specific receptor for FGF23. Nature 444:770–774
Wolf I, Sadetzki S, Catane R, Karasik A, Kaufman B (2005) Diabetes mellitus and breast cancer. Lancet Oncol 6:103–111
Yee D (2006) Targeting insulin-like growth factor pathways. Br J Cancer 94:465–468
Wolf I, Levanon-Cohen S, Bose S, Ligumsky H, Sredni B, Kanety H, Kuro-o M, Karlan B, Kaufman B, Koeffler HP et al (2008) Klotho: a tumor suppressor and a modulator of the IGF-1 and FGF pathways in human breast cancer. Oncogene 27:7094–7105
Wolf I, Laitman Y, Rubinek T, Abramovitz L, Novikov I, Beeri R, Kuro OM, Koeffler HP, Catane R, Freedman LS et al (2010) Functional variant of KLOTHO: a breast cancer risk modifier among BRCA1 mutation carriers of Ashkenazi origin. Oncogene 29:26–33
Chen B, Wang X, Zhao W, Wu J (2010) Klotho inhibits growth and promotes apoptosis in human lung cancer cell line A549. J Exp Clin Cancer Res 29:99
Doi S, Zou Y, Togao O, Pastor JV, John GB, Wang L, Shiizaki K, Gotschall R, Schiavi S, Yorioka N et al (2011) Klotho inhibits transforming growth factor-{beta}1 (TGF-{beta}1) signaling and suppresses renal fibrosis and cancer metastasis in mice. J Biol Chem 286:8655–8665
Lee J, Jeong D-J, Kim J, Lee S, Park J-H, Chang B, Jung S-I, Yi L, Han Y, Yang Y et al (2010) The anti-aging gene KLOTHO is a novel target for epigenetic silencing in human cervical carcinoma. Molecular Cancer 9:109–119
Lu L, Katsaros D, Wiley A, de la Longrais IA, Puopolo M, Yu H (2008) Klotho expression in epithelial ovarian cancer and its association with insulin-like growth factors and disease progression. Cancer Invest 26:185–192
Wang X, Chen B, Xu W, Liu S, Zhao W, Wu J (2011) Combined effects of klotho and soluble CD40 ligand on A549 lung cancer cells. Oncol Rep 25(5):1465–1472
Sharma S, Kelly TK, Jones PA (2010) Epigenetics in cancer. Carcinogenesis 31:27–36
Lo P-K, Sukumar S (2008) Epigenomics and breast cancer. Pharmacogenomics 9:1879–1902
Wolf I, Bose S, Desmond J, Lin B, Williamson E, Karlan B, Koeffler H (2007) Unmasking of epigenetically silenced genes reveals DNA promoter methylation and reduced expression of PTCH in breast cancer. Breast Cancer Res Treat 105:139–155
Wolf I, Bose S, Williamson EA, Miller CW, Karlan BY, Koeffler HP (2007) FOXA1: Growth inhibitor and a favorable prognostic factor in human breast cancer. Int J Cancer 120:1013–1022
McShane L, Altman D, Sauerbrei W, Taube S, Gion M, Clark G (2006) REporting recommendations for tumor MARKer prognostic studies (REMARK). Breast Cancer Res Treat 100:229–235
Gal-Yam EN, Egger G, Iniguez L, Holster H, Einarsson Sm, Zhang X, Lin JC, Liang G, Jones PA, Tanay A (2008) Frequent switching of Polycomb repressive marks and DNA hypermethylation in the PC3 prostate cancer cell line. Proc Natl Acad Sci 105:12979–12984
Lacroix M, Leclercq G (2004) Relevance of breast cancer cell lines as models for breast tumours: an update. Breast Cancer Res Treat 83:249–289
Wolf I, O’Kelly J, Rubinek T, Tong M, Nguyen A, Lin BT, Tai H–H, Karlan BY, Koeffler HP (2006) 15-Hydroxyprostaglandin dehydrogenase is a tumor suppressor of human breast cancer. Cancer Res 66:7818–7823
Richon VM, Emiliani S, Verdin E, Webb Y, Breslow R, Rifkind RA, Marks PA (1998) A class of hybrid polar inducers of transformed cell differentiation inhibits histone deacetylases. Proc Natl Acad Sci 95:3003–3007
Schnitt SJ (2003) Benign breast disease and breast cancer risk: morphology and beyond. Am J Surg Pathol 27:836–841
Hoque MO, Prencipe M, Poeta ML, Barbano R, Valori VM, Copetti M, Gallo AP, Brait M, Maiello E, Apicella A et al (2009) Changes in CpG islands promoter methylation patterns during ductal breast carcinoma progression. Cancer Epidem Biomar 18:2694–2700
Herman JG, Merlo A, Mao L, Lapidus RG, Issa J-PJ, Davidson NE, Sidransky D, Baylin SB (1995) Inactivation of the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers. Cancer Res 55:4525–4530
Mancini DN, Rodenhiser DI, Ainsworth PJ, O’Malley FP, Singh SM, Xing W, Archer TK (1998) CpG methylation within the 5′ regulatory region of the BRCA1 gene is tumor specific and includes a putative CREB binding site. Oncogene 16:1161–1169
Schutte M, Rozenblum E, Moskaluk CA, Guan X, Hoque AT, Hahn SA, da Costa LT, de Jong PJ, Kern SE (1995) An integrated high-resolution physical map of the DPC/BRCA2 region at chromosome 13q12. Cancer Res 55:4570–4574
Geck P, Maffini MV, Szelei J, Sonnenschein C, Soto AM (2000) Androgen-induced proliferative quiescence in prostate cancer cells: the role of AS3 as its mediator. Proc Natl Acad Sci 97:10185–10190
Schott DR, Chang JN, Deng G, Kurisu W, Kuo WL, Gray J, Smith HS (1994) A candidate tumor suppressor gene in human breast cancers. Cancer Res 54:1393–1396
Acknowledgments
This research was supported by The Riva and Joel Koschitzky Fund for Breast Cancer Research at the Sheba Medical Center; the Chief Scientist Office of the Ministry of Health, Israel (grant no. 4055_3 to IW); the Israel Cancer Association Research Grant; The Israel Science Foundation (to I.W.); the “Talpiut” Sheba Career Development Award; and the Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Conflicts of interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rubinek, T., Shulman, M., Israeli, S. et al. Epigenetic silencing of the tumor suppressor klotho in human breast cancer. Breast Cancer Res Treat 133, 649–657 (2012). https://doi.org/10.1007/s10549-011-1824-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-011-1824-4