
Abstract
Topoisomerase IIα is not only a proliferation marker of tumor cells, but is also a target for anthracycline-based chemotherapy. Both in vitro and in vivo studies have shown that there is a relationship between topo IIα and chemosensitivity to anthracyclines, but the predictive role of topo IIα in breast cancer patients is still controversial. A meta-analysis based on published studies was performed to obtain an accurate assessment of the association between topo IIα and sensitivity to anthracycline-based chemotherapy. A total of 13 eligible studies, including 2,633 cases and 2,118 controls were identified. Topo IIα was associated with sensitivity to anthracyclines in locally advanced breast cancer patients who received neoadjuvant chemotherapy [five studies, including three using fluorescence in situ hybridization (FISH) and two using immunohistochemistry (IHC): relative risk (RR) = 1.93, 95% confidence interval (95% CI): 1.27–2.94, P = 0.002; two using FISH and three using IHC: RR = 1.98, 95% CI: 1.37–2.86, P < 0.001]. This association existed among three studies using FISH (RR = 2.03, 95% CI: 1.14–3.61, P = 0.017), but did not exist among three studies using IHC (P > 0.05). In early-stage breast cancer patients who received anthracycline-based adjuvant chemotherapy compared with non-taxane-based polychemotherapy, amplification [hazard ratio (HR) = 0.64, 95% CI: 0.49–0.83, P = 0.001; HR = 0.59, 95% CI: 0.35–1.01, P = 0.056] or deletion (HR = 0.82, 95% CI: 0.67–1.00, P = 0.051; HR = 0.58, 95% CI: 0.35–0.97, P = 0.036) of topo IIα was significantly associated with better recurrence-free survival and overall survival. In summary, the present meta-analysis suggests that topo IIα is a predictive factor for breast cancer patients who receive anthracycline-based chemotherapy. Larger and well-designed prospective studies are required to further evaluate the predictive role of topo IIα in clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite the fact that breast cancer continues to be the most common malignant tumor among women, it is a highly treatable disease. Currently, the systemic treatment of breast cancer has greatly contributed to the declining breast cancer mortality rates. As to adjuvant chemotherapy, effective agents include alkylating agents, anthracyclines, and taxanes. However, individualized treatment has not been widely carried out, because the recognition of sensitivity to certain kind of therapies is a prerequisite to individualized treatment.
Topoisomerase IIα (Topo IIα) is a critical nuclear DNA-binding enzyme: the gene that encodes this protein is located on chromosome 17q21. Topo IIα controls and modifies the topologic states of DNA [1]. Specifically, it reduces DNA supercoiling and twisting by cutting both strands of the DNA helix simultaneously. Once cut, the ends of the DNA are separated and a second DNA duplex is passed through the break, followed by religation of the cleaved DNA strand [2]. Disruption of topo IIα leads to double-strand DNA breaks and cell death.
Anthracyclines, one of the most widely used chemotherapeutic agents for breast cancer, have three major mechanisms of action: (1) inhibition of DNA and RNA synthesis by intercalation between base pairs of the DNA/RNA strand; (2) enhancement of catalysis of oxidation–reduction reactions; and (3) inhibition of topo IIα. Of note, the first and third mechanisms appear to be dependent on inhibition of topo IIα for cytotoxicity [3]. Topo IIα is not only a proliferation marker of tumor cells, but is also a target for anthracycline-based chemotherapy. Both in vitro and in vivo studies have demonstrated that there is a relationship between topo IIα expression levels and chemosensitivity to anthracyclines [4, 5], but these results have been controversial. Several studies [6–10], which included patients with locally advanced breast cancer and who were treated with neoadjuvant anthracycline-based chemotherapy, measured topo IIα levels by immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH). Results showed that amplification or overexpression of topo IIα was associated with a local response to anthracycline-based therapy. However, other studies [4, 11, 12] evaluated topo IIα status in locally advanced or metastatic breast cancer patients and drew different conclusions. In regards to early-stage breast cancer patients, some prospective studies [5, 13–16] performed recurrence-free survival (RFS) and/or overall survival (OS) comparisons between anthracycline-based and non-anthracycline study arms to evaluate the predictive value of topo IIα. These studies did not come to the same conclusion. In addition, the limited availability of samples resulted in variations in the clinical significance of the results of different topo IIα studies.
In order to further evaluate the role of topo IIα in predicting sensitivity to anthracyclines in breast cancer patients, we performed the present meta-analysis. Of note, Di Leo et al. presented a meeting report from a planned interim analysis of a meta-analysis regarding this issue 2 years ago [17], however, it only included studies comparing anthracycline-based therapy with cyclophosphamide, methotrexate, and fluorouracil (CMF) in early-stage breast cancer patients. In recent years, additional studies have been reported, as well as studies which focused on locally advanced patients who received neoadjuvant therapy, and metastatic breast cancer patients. Each of these patient groups are included in our study, which we hope will give a more precise estimation that will greatly improve the reliability of our conclusions.
Methods
Publication search
We searched PubMed, Medline, and Web of Science databases using the following search terms: “topoisomerase IIα,” “topo IIα,” “anthracyclines,” and “breast cancer.” All resulting studies were retrieved, and their references were checked for the other potentially relevant publications. Review articles were also scanned to find additional eligible studies. For studies with the same population, only the latest published was selected. Only those studies published in English were included in this meta-analysis.
Eligible studies and data extraction
Search results were screened according to the following inclusion criteria: (a) evaluation of topoisomerase IIα in predicting sensitivity to anthracyclines in early-stage breast cancer, locally advanced breast cancer, or metastatic breast cancer, (b) described therapy response, reported OS or RFS, (c) retrospective studies or prospective cohort studies, (d) inclusion of sufficient data to allow the estimation of a relative risk (RR) with a 95% confidence interval (95% CI), or a hazard ratio (HR) with a 95% CI, and (e) studies published in English. All studies included in our meta-analysis met all of the criteria outlined above. Letters to the editor, reviews, and articles published in a book or papers published in a language other than English were excluded.
The following variables were extracted from each study if available: first author’s surname, publication year, country, number of cases and controls, and number of different events of cases and controls. Information was carefully extracted independently from all eligible publications by three of the authors of the present study (Du YY, Zhou Q, and Yin WJ). Differences in the extraction of data were checked by a fourth investigator (Lu JS).
Statistical analysis
RR with 95% CI was employed to estimate the association between topo IIα and sensitivity to anthracyclines in locally advanced or metastatic breast cancer, because numbers of different events of cases and controls were provided in the studies. HR with 95% CI was used for assessing the association between topo IIα and sensitivity to anthracyclines, and in early-stage breast cancer RFS and/or OS comparisons were performed between different study arms and HR with 95% CI was provided. RFS was defined as time from random assignment to recurrence, including local breast chest wall and regional and/or distant recurrence and second primary cancer. Heterogeneity assumption was checked by the Q test, and a P-value greater than 0.10 indicated a lack of heterogeneity among studies. The pooled RR was calculated by a fixed-effects model (the Mantel–Haenszel method) or a random-effects model (the DerSimonian and Laird method) according to the heterogeneity. Funnel plots and the Egger’s test were employed to estimate the possible publication bias. We also performed sensitivity analysis by omitting each study or specific studies to find potential outliers.
Kaplan–Meier curves were analyzed by GetData Graph Digitizer 2.24 (free software downloaded for http://getdata-graph-digitizer.com). All statistical analyses were performed using Stata/SE software, version 10.0 (Stata Corporation, College Station, TX).
Results
Description of studies
A total of 14 publications met the inclusion criteria for the present analysis. Di Leo et al. published two articles on the same population, and evaluated topo IIα by IHC and FISH, although the study which measured topo IIα levels by IHC was excluded from our present study. Hence, 13 publications with 2,633 cases and 2,118 controls were a part of our meta-analysis. Five studies reported the association between topo IIα and the response rate of locally advanced breast cancer patients who received anthracycline-based neoadjuvant therapy [6–10], and three studies reported the association between topo IIα and response rate of advanced or metastatic breast cancer patients who received anthracycline-based salvage treatment [4, 11, 12]. Response was defined as complete response (CR) or partial response (PR), while non-response was defined as stable disease (SD) or progressive disease (PD) according to the International Union Against Cancer (UICC) criteria [18]. Topo IIα was evaluated by IHC and/or FISH in these studies.
In regards to early-stage breast cancer in the adjuvant setting, six studies compared anthracycline and non-anthracycline chemotherapy by evaluating topo IIα gene status and RFS and/or OS. Twelve studies considered the possible relationship between topo IIα and sensitivity to anthracyclines, while two studies failed to show such an association. BCIRG 006 compared AC → T with AC → TH and TCH in the adjuvant treatment of Her-2 amplified early-stage breast cancer patients, and we calculated the statistics of AC → TH and TCH arms to avoid the influence of herceptin. Tables 1 and 2 detail all the studies included in the meta-analysis.
Correlation of topo IIα with response rate of breast cancer patients who received anthracycline-based salvage treatment and neoadjuvant therapy
Among the studies of breast cancer patients who received anthracycline-based salvage treatment and neoadjuvant therapy, different measurements of topo IIα status (either by IHC or by FISH) have been employed to evaluate association of favorable responses to anthracycline-based chemotherapy, so we calculated the statistics of both protein and gene status of topo IIα. When locally advanced and metastatic breast cancer patients were both considered, topo IIα was associated with sensitivity to anthracyclines (six studies measured topo IIα status by IHC and two by FISH: RR = 1.87, 95% CI: 1.28–2.74, P = 0.001) (Fig. 1a); (four studies measured topo IIα status by IHC and four by FISH: RR = 1.81, 95% CI: 1.31–2.51, P < 0.001) (Fig. 1b) by D-L method.

Forest plots of RR were assessed for association between topo IIα and sensitivity to anthracyclines in locally advanced or metastatic breast cancer patients, in which all the studies measured topo IIα status by IHC with the exception of Coon’s study which measured topo IIα status by both IHC (a) and FISH ( b)
Among five studies of the neoadjuvant subgroup, two studies used an IHC assay and two used a FISH assay; only one study (Coon’s study) measured both protein and gene status of topo IIα, so the protein and gene status of topo IIα was separately calculated, and we obtained similar results. We found that topo IIα was associated with response rate of breast cancer patients who received anthracycline-based neoadjuvant therapy (Coon’s study measured topo IIα by IHC: RR = 1.93, 95% CI: 1.27–2.94, P = 0.002); (Coon’s study measured topo IIα by FISH: RR = 1.98, 95% CI: 1.37–2.86, P < 0.001). Moreover, when calculated using different measurement assays, we found that there was still an association between topo IIα status using FISH, and response to anthracycline-based neoadjuvant therapy (three studies, RR = 2.03, 95% CI: 1.14–3.61, P = 0.017), but there was no association in topo IIα status measured by IHC (three studies, P > 0.05) (Fig. 2). This might indicate that FISH is a better assay to use in the evaluation of topo IIα and sensitivity to anthracyclines.

Forest plots of RR were assessed for the evaluation of IHC and FISH in neoadjuvant settings
Then, we made subgroup analyses to further evaluate the role of topo IIα in locally advanced and metastatic breast cancer. In the salvage treatment subgroup, all the studies measured topo IIα protein levels, with the exception of Cardoso’s study, which measured both protein and gene status of topo IIα. Therefore, we calculated the protein and gene status of topo IIα as well. We found no relationship between topo IIα and sensitivity to anthracyclines (Cardoso’s study measured topo IIα by IHC: RR = 1.89, 95% CI: 0.64–5.56, P = 0.247); (Cardoso’s study measured topo IIα by FISH: RR = 1.55, 95% CI: 0.67–3.61, P = 0.310). The salvage treatment subgroup included two studies, which compared anthracyclines with taxanes. We used random effects to analyze the taxane groups, and found no relationship between topo IIα and sensitivity to taxane (RR = 1.24, 95% CI: 0.39–3.97, P = 0.716) (Fig. 3).

Forest plots of RR were assessed for association between topo IIα and sensitivity to taxanes in metastatic breast cancer patients
Impact of topo IIα on RFS of early-stage breast cancer in adjuvant setting
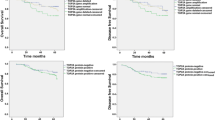
In regards to topo IIα amplified cases, anthracyclines were significantly associated with superior RFS (HR = 0.63, 95% CI: 0.49–0.83, P = 0.001) (Fig. 4a) compared with non-anthracycline chemotherapy in whole groups. One of the five adjuvant studies compared RFS between AC → TH arms and TCH arms, so we made subgroup analyses and tried to eliminate the interference of taxane. In the first subgroup, anthracycline regimens were compared with non-anthracycline non-taxane regimens, while in the second subgroup, the combination of anthracycline and taxane (AC → TH) was compared with regimens containing taxanes, but without anthracyclines (TCH). In the first subgroup, topo IIα amplification was associated with better RFS (HR = 0.48, 95% CI: 0.30–0.77, P = 0.002), while in the second subgroup, marginal significance of RFS benefit was observed in topo IIα amplified patients (HR = 0.73, 95% CI: 0.53–1.01, P = 0.054). In topo IIα deleted cases, we found that anthracyclines tended to improve RFS with marginal significance compared with non-anthracycline chemotherapy (HR = 0.82, 95% CI: 0.67–1.00, P = 0.051) (Fig. 4b). In the first subgroup, there was a relationship between anthracycline and better RFS (HR = 0.62, 95% CI: 0.39–0.96, P = 0.033). However, in the second subgroup, there was no statistical significance between anthracycline and better RFS (HR = 0.88, 95% CI: 0.70–1.10, P = 0.261). In topo IIα normal cases, anthracycline was not significantly associated with better RFS (HR = 0.88, 95% CI: 0.75–1.00, P = 0.05) in whole group (Fig. 4c). In both the first (HR = 0.86, 95% CI: 0.71–1.03, P = 0.107) and second subgroup (HR = 0.88, 95% CI: 0.70–1.10, P = 0.261), there was no relationship between anthracycline and better RFS.

Forest plots of HR for RFS were assessed for association between topo IIα and sensitivity to anthracyclines in early-stage breast cancer patients: topo IIα amplified cases (a), topo IIα deleted cases (b), and topo IIα normal cases (c)
Impact of topo IIα on OS of early-stage breast cancer in adjuvant settings
OS was involved in three adjuvant studies, and the pooled HR of the three studies containing 1,533 patients were analyzed. In topo IIα amplified cases, we found that anthracyclines tended to improve OS with marginal significance compared with non-anthracycline chemotherapy (HR = 0.59, 95% CI: 0.35–1.01, P = 0.056) (Fig. 5a). However, in topo IIα deleted cases, anthracycline was significantly associated with better OS (HR = 0.58, 95% CI: 0.35–0.97, P = 0.036) (Fig. 5b). In topo IIα normal cases, no difference in OS was observed between anthracycline and non-anthracycline-based therapy (HR = 0.90, 95% CI: 0.73–1.11, P = 0.337) (Fig. 5c).

Forest plots of HR for OS were assessed for association between topo IIα and sensitivity to anthracyclines in early-stage breast cancer patients: topo IIα amplified cases (a), topo IIα deleted cases (b), topo IIα normal cases (c)
Publication bias
Begg’s funnel plot with pseudo 95% confidence limits, and Egger’s test were performed to estimate the publication bias of the included literature. The shapes of the funnel plots did not reveal any evidence of obvious asymmetry, and the Egger’s test indicated the absence of publication bias (P > 0.05). Moreover, sensitivity analysis was carried out to estimate the influence of individual studies on the summary effect. No individual study dominated this meta-analysis, since omission of any single study made no difference (Figures not shown).
Discussion
The current meta-analysis of 13 studies systematically evaluated the association between topo IIα and sensitivity to anthracyclines with the largest populations. Studies included in this meta-analysis reported diverse results on this issue, which made it necessary to perform a quantitative aggregation of the results. Our results indicate that altered topo IIα status or overexpression of topo IIα may predict incremental benefits from anthracycline therapy. In early-stage breast cancer patients who received anthracycline-based adjuvant chemotherapy, amplification of topo IIα was significantly associated with better RFS and OS. Deletion of topo IIα tended to improve RFS and OS. In locally advanced breast cancer patients who received anthracycline-based neoadjuvant chemotherapy, amplification or overexpression of topo IIα was also associated with better response rates.
In locally advanced and metastatic breast cancer patients, amplification or overexpression of topo IIα was associated with sensitivity to anthracyclines. Our findings are consistent with most of the basic research on this issue. In addition, we made subgroup analyses to further evaluate the role of topo IIα. In the neoadjuvant subgroup, topo IIα was significantly associated with incremental benefits from anthracycline-based therapy. However, no significant association was found in the salvage treatment subgroup. One potential explanation is that there were only three studies in the subgroup and a small sample size, which made it difficult to obtain statistically significant data. Another explanation is that topo IIα might not be a single predictive marker in metastatic breast cancer as the biology of late-stage cancer is very different from early-stage cancer. Moreover, among the three studies, two included patients who received taxane-based chemotherapy as control cases. We analyzed those two studies and found that topo IIα was not associated with either anthracyclines or taxanes. One thing which should be noted is that in breast cancer patients, the overall response to anthracyclines is lower than the overall response to taxanes in advanced breast cancer [4]. This suggested that topo IIα could not be used to predict the response rate of chemotherapy in comparison between anthracyclines and taxanes.
Some retrospective studies [14, 15] found that patients with topo IIα-amplified breast cancer who were treated with anthracycline-based adjuvant chemotherapy, had better RFS and OS. In addition, some studies also found that deletion of topo IIα could predict a better outcome [13, 15] in early-stage breast cancer patients who received anthracycline-based adjuvant treatment. In the present meta-analysis, amplification or deletion of topo IIα was significantly associated with superior RFS and OS in early-stage breast cancer patients who received anthracycline-based adjuvant treatment if we excluded the interference of taxanes. It suggested that taxanes might also interfere with the evaluation of topo IIα in early-stage breast cancer patients who received anthracycline-based adjuvant chemotherapy. These were consistent with the result of salvage treatments in this meta-analysis.
There are some limitations in the present meta-analysis, which need to be acknowledged. First, although most of the studies of locally advanced and metastatic breast cancer patients defined “Response” as CR and PR, and “Non-response” as SD and PD, some studies had different definitions, which may lead to a misclassification bias. Second, the RFS and OS outcomes were based on individual unadjusted HRs, while a more precise assessment should be adjusted using other prognostic factors. Third, the inclusion criteria were not quite the same in all the studies. Finally, different measurements of topo IIα status (either by IHC or by FISH) have been employed to evaluate association with favorable response to anthracycline-based chemotherapy [19]. Cut-off values of topo IIα for both overexpression by IHC and gene amplification by FISH were not the same in each study. Therefore, standardization is of great importance when assessing topo IIα levels, which may help in obtaining an accurate picture of its clinical significance. Moreover, quantitative PCR may be useful in future prospective studies.
To sum up, the present study strongly suggests that topo IIα is associated with sensitivity to anthracyclines, especially in early-stage breast cancer patients who received anthracycline-based chemotherapy compared with non-taxane-based polychemotherapy. Amplification of topo IIα is significantly associated with better RFS and OS and deletion of topo IIα tends to improve RFS and OS. In locally advanced breast cancer patients who received neoadjuvant chemotherapy, amplification or overexpression of topo IIα is also associated with incremental benefits from anthracycline therapy. In addition, taxane might interfere with the evaluation of the predictive role of topo IIα. Therefore, we encourage further evaluations on the predictive role of topo IIα in larger, more comprehensive, and well-designed association studies.
References
Berger JM, Gamblin SJ, Harrison SC, Wang JC (1996) Structure and mechanism of DNA topoisomerase II. Nature 379:225–232
Kellner U, Sehested M, Jensen PB, Gieseler F, Rudolph P (2002) Culprit and victim—DNA topoisomerase II. Lancet Oncol 3:235–243
Oakman C, Moretti E, Galardi F, Santarpia L, Di Leo A (2009) The role of topoisomerase IIalpha and HER-2 in predicting sensitivity to anthracyclines in breast cancer patients. Cancer Treat Rev 35:662–667
Durbecq V, Paesmans M, Cardoso F et al (2004) Topoisomerase-II alpha expression as a predictive marker in a population of advanced breast cancer patients randomly treated either with single-agent doxorubicin or single-agent docetaxel. Mol Cancer Ther 3:1207–1214
Di Leo A, Gancberg D, Larsimont D et al (2002) HER-2 amplification and topoisomerase IIalpha gene aberrations as predictive markers in node-positive breast cancer patients randomly treated either with an anthracycline-based therapy or with cyclophosphamide, methotrexate, and 5-fluorouracil. Clin Cancer Res 8:1107–1116
Martin-Richard M, Munoz M, Albanell J et al (2004) Serial topoisomerase II expression in primary breast cancer and response to neoadjuvant anthracycline-based chemotherapy. Oncology 66:388–394
MacGrogan G, Rudolph P, Mascarel Id I et al (2003) DNA topoisomerase IIalpha expression and the response to primary chemotherapy in breast cancer. Br J Cancer 89:666–671
Coon JS, Marcus E, Gupta-Burt S, Seelig S, Jacobson K, Chen S, Renta V, Fronda G, Preisler HD (2002) Amplification and overexpression of topoisomerase IIalpha predict response to anthracycline-based therapy in locally advanced breast cancer. Clin Cancer Res 8:1061–1067
Park K, Kim J, Lim S, Han S (2003) Topoisomerase II-alpha (topoII) and HER2 amplification in breast cancers and response to preoperative doxorubicin chemotherapy. Eur J Cancer 39:631–634
Desmedt C, Azambuja E, Larsimont D et al (2009) Predicting the efficacy of anthracyclines in breast cancer (BC) patients: results of the neoadjuvant TOP trial. J Clin Oncol 27:523
Cardoso F, Durbecq V, Larsimont D et al (2004) Correlation between complete response to anthracycline-based chemotherapy and topoisomerase II-alpha gene amplification and protein overexpression in locally advanced/metastatic breast cancer. Int J Oncol 24:201–209
Jarvinen TA, Holli K, Kuukasjarvi T, Isola JJ (1998) Predictive value of topoisomerase IIalpha and other prognostic factors for epirubicin chemotherapy in advanced breast cancer. Br J Cancer 77:2267–2273
Knoop AS, Knudsen H, Balslev E et al (2005) Retrospective analysis of topoisomerase IIa amplifications and deletions as predictive markers in primary breast cancer patients randomly assigned to cyclophosphamide, methotrexate, and fluorouracil or cyclophosphamide, epirubicin, and fluorouracil: Danish Breast Cancer Cooperative Group. J Clin Oncol 23:7483–7490
Bartlett JM, Munro A, Cameron DA, Thomas J, Prescott R, Twelves CJ (2008) Type 1 receptor tyrosine kinase profiles identify patients with enhanced benefit from anthracyclines in the BR9601 adjuvant breast cancer chemotherapy trial. J Clin Oncol 26:5027–5035
O’Malley FP, Chia S, Tu D, Shepherd LE, Levine MN, Bramwell VH, Andrulis IL, Pritchard KI (2009) Topoisomerase II alpha and responsiveness of breast cancer to adjuvant chemotherapy. J Natl Cancer Inst 101:644–650
Slamon D, Eiermann W, Robert N et al (2009) Phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel (AC → T) with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab (AC → TH) with docetaxel, carboplatin and trastuzumab (TCH) in Her2neu positive early breast cancer patients: BCIRG 006 study. Cancer Res 69:500S
Di Leo A, Isola J, Piette F et al (2009) A meta-analysis of phase III trials evaluating the predictive value of HER2 and topoisomerase II alpha in early breast cancer patients treated with CMF or anthracycline-based adjuvant therapy. Cancer Res 69:99S
Hayward JL, Carbone PP, Heuson JC, Kumaoka S, Segaloff A, Rubens RD (1977) Assessment of response to therapy in advanced breast cancer: a project of the Programme on Clinical Oncology of the International Union Against Cancer, Geneva, Switzerland. Cancer 39:1289–1294
Buzdar AU (2006) Topoisomerase IIalpha gene amplification and response to anthracycline-containing adjuvant chemotherapy in breast cancer. J Clin Oncol 24:2409–2411
Author information
Authors and Affiliations
Corresponding author
Additional information
Yueyao Du and Qiong Zhou contributed equally to this study.
Rights and permissions
About this article
Cite this article
Du, Y., Zhou, Q., Yin, W. et al. The role of topoisomerase IIα in predicting sensitivity to anthracyclines in breast cancer patients: a meta-analysis of published literatures. Breast Cancer Res Treat 129, 839–848 (2011). https://doi.org/10.1007/s10549-011-1694-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-011-1694-9