
Abstract
Clinical trials conducted in Western countries have shown that aromatase inhibitors are associated with better disease-free survival (DFS) than tamoxifen in postmenopausal early breast cancer. Because pharmacogenetic differences in drug-metabolizing genes may cause ethnic differences, assessment of the efficacy and tolerability of aromatase inhibitors in non-white women is warranted. This open-label, randomized clinical trial included 706 postmenopausal Japanese women with hormone-receptor-positive breast cancer, who had received tamoxifen for 1 to 4 years as adjuvant therapy. This study was closed early after entry of ~28% of the initially planned patients. They were randomly assigned to either switch to anastrozole or to continue tamoxifen for total treatment duration of 5 years. Primary endpoints were DFS and adverse events. At a median follow-up of 42 months, the unadjusted hazard ratio was 0.69 (95% confidence interval, 0.42–1.14; P = 0.14) for DFS and 0.54 (95% CI, 0.29–1.02; P = 0.06) for relapse-free survival (RFS), both in favor of anastrozole. The incidence of thromboembolic events in the tamoxifen group and bone fractures in the anastrozole group was not excessively high. Switching from tamoxifen to anastrozole was likely to decrease disease recurrence in postmenopausal Japanese breast cancer patients. Ethnic differences in major adverse events may be attributable to a low baseline risk of these events in Japanese.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence of breast cancer in Japanese women is increasing, while it remains much lower than that in Western women [1]. Nonetheless, breast cancer has been the most common type of cancer in Japanese women since the 1990s [1]. Mortality from breast cancer is decreasing in Western countries owing to the increased use of screening mammography and adjuvant therapy [2], but continues to increase in Japan. As for adjuvant therapy, most newly developed drugs are available in Japan, but data from randomized controlled trials in Asian women are often lacking.
Tamoxifen, classified as a selective estrogen-receptor modulator, for 5 years has been the gold standard for adjuvant hormonal therapy in women with early breast cancer. Although tamoxifen is generally well tolerated, it can cause serious complications such as endometrial cancer or deep venous thrombosis [3]. Tamoxifen significantly decreases disease recurrence and increases overall survival (OS) irrespective of nodal status and age [4], but some patients become resistant to tamoxifen and have recurrence. Therefore, the development of improved strategies is awaited. Randomized controlled trials have compared aromatase inhibitors with tamoxifen for adjuvant treatment in postmenopausal women with hormone-responsive breast cancer. Studies comparing 5 years of treatment with anastrozole or letrozole with 5 years of treatment with tamoxifen showed a 15% improvement in disease-free survival (DFS) at 100 months [5] or an 18% reduction in the risk of an event at 51 months [6]; however, neither study showed a significant improvement in OS. Switching from tamoxifen to aromatase inhibitors has been also compared with tamoxifen for 5 years, given for a total of 5 years. Switching from tamoxifen to anastrozole improved DFS by 65% at 36 months in one study [7] and by 40% at 28 months in another [8]. In another randomized trial, switching from tamoxifen to exemestane improved DFS by 32% at 31 months [9].
These clinical trials were conducted in Western countries and included only small numbers of Asian women. When we apply these results to Asian populations, ethnic differences in drug metabolizing genes such as cytochrome P450 (CYP)2D6 genotype may be appreciable, because CYP2D6 metabolizes tamoxifen into its more potent metabolite, endoxifen. Polymorphisms of the CYP2D6 gene may thus alter the response to tamoxifen [10]. About 10% of whites are classified as inactive metabolizers of tamoxifen, resulting in decreased turnover of tamoxifen into its active metabolite, endoxifen [11]. In contrast, less than 1% of Japanese are inactive metabolizers of tamoxifen, and about 20% are intermediate metabolizers [12]. Such ethnic differences in the CYP2D6 gene may lead to differences between whites and Japanese in the efficacy and safety of tamoxifen, especially when compared with those of aromatase inhibitors. This situation is further complicated by the fact that the distribution of CYP19 gene (aromatase) polymorphisms differs among distinct ethnic populations [13], potentially causing differences between whites and Japanese in the efficacy and safety of aromatase inhibitors. In fact, one placebo-controlled trial of letrozole after 5 years of tamoxifen in postmenopausal women with early breast cancer showed that letrozole improved DFS in whites, but not in women from minority groups [14]. Therefore, clinical trials assessing the efficacy and safety of aromatase inhibitors in non-white women are warranted. Here, we report the results of switching adjuvant therapy from tamoxifen to anastrozole in postmenopausal Japanese women with breast cancer who were enrolled in an open-label, randomized clinical trial, designated the N-SAS BC03 study (UMIN CTRID: C000000056).
Study design
This study was a multi-institutional, open-label, randomized control trial, designed to compare the efficacy and safety of tamoxifen with those of tamoxifen followed by anastrozole in postmenopausal women with hormone-responsive breast cancer, who remained disease-free after having received tamoxifen for 1 to 4 years as adjuvant therapy. The subjects were randomly assigned to continue to receive tamoxifen (20 mg per day) or to switch to anastrozole (1 mg per day). The total duration of treatment was 5 years (Fig. 1). The primary endpoints were DFS and adverse events. The secondary endpoints were relapse-free survival (RFS), OS, and the health-related quality of life (HRQOL). At the time of randomization, treatment assignments were adjusted according to the following factors: clinical stage (I, IIA, IIB/IIIA/IIIB) [15]; the number of metastases to axillary lymph nodes (0/1–3/more than 3); HER2 status (unknown/0, 1+, 2+/3+); tumor size (<3 cm/≥3 cm), estrogen receptor (ER) and progesterone receptor (PR) status (ER[+], PR[+]/ER[+], PR[−]/ER[−], PR[+]); type of surgery (breast-conserving surgery/mastectomy); duration of tamoxifen administration (1.0–<2.0 years/2.0–4.0 years); age (younger than 60 years/60 years or older); chemotherapy (performed/not performed); and institution. Menopause in this study was defined as follows: an age of > 60 years, an age of > 45 years with amenorrhea for 1 year or longer without hysterectomy, or bilateral ovariectomy.

Study design. TAM tamoxifen, ANA anastrozole
Patients and methods
Eligible patients were postmenopausal women who had undergone surgery for histologically confirmed stage I, IIA, IIB, IIIA, or IIIB [15] unilateral primary invasive breast cancer that was positive for estrogen receptor, progesterone receptor, or both; all patients had postoperatively received adjuvant tamoxifen for 1 to 4 years. Patients also had to be younger than 75 years and to have adequate organ functions at the time of enrollment. Diagnostic imaging studies, including chest radiography (or computed tomography), abdominal ultrasonography (or computed tomography), bone scintigraphy (or radiography), and mammography, were performed within 6 months before the day of enrollment and repeated annually thereafter. Adjuvant therapy should have been started within 12 weeks after surgery. Preoperative endocrine therapy with tamoxifen or preoperative chemotherapy was allowed. Patients were excluded if they had any of the following conditions: invasive cancer in other organs for which treatment was not completed within 5 years; a medical history of deep venous thrombosis; or osteoporosis requiring treatment or a medical history of bone fracture due to osteoporosis. Follow-up of the patients was scheduled as follows: physical examination was scheduled every 3 months for 1 year, for every 6 months from year 2 to five, and annually thereafter by year 10. Diagnostic imaging was scheduled annually that included chest X-ray or CT, abdominal ultrasonography or CT, bone X-ray or bone scan.
Data on the following prespecified adverse events were prospectively collected: hot flashes, nausea, anorexia, fatigue/asthenia, mood alteration, headache, arthralgia, leukocytopenia, hepatic dysfunction (aspartate aminotransferase and alanine aminotransferase), ischemic cerebrovascular disorders, ischemic cardiovascular disorders, thrombosis (including all types), genital bleeding, vaginal discharge, bone fracture and endometrial cancer. Data on adverse events were prospectively collected at 3-month intervals for the first year and at 6-month intervals thereafter for a total of 5 years after randomization. Toxicity was recorded according to the National Cancer Institute Common Toxicity Criteria, version 2.0. HRQOL was also assessed; the results will be presented elsewhere (Ohsumi S et al., in preparation).
Written informed consent was obtained from all subjects after they had received an explanation of the clinical trial. The protocol was approved by the institutional review board of each participating institution before enrollment began. The trial was conducted in accordance with the Declaration of Helsinki (1996 revision).
Statistics
Eligible patients were randomly assigned to continue tamoxifen or to switch to anastrozole in a ratio of 1:1 according to the allocation adjustment factors described above, using a dynamic allocation method. DFS and RFS were calculated from the date of randomization to the date of confirmation of an initial event. All of the following were considered events for DFS: locoregional relapse, distant metastasis, asynchronous cancer or secondary cancer (except skin basal cell cancer/spinocellular cancer and uterine intraepithelial cancer), and death from any cause. The data were censored on the day on which the above events were last confirmed to be absent or on the day on which survival was last confirmed for survivors. Events for RFS were locoregional relapse and distant metastasis. The data were censored on the day on which the above events were last confirmed to be absent, on the day of occurrence of asynchronous or secondary cancer, or on the day on which none of the above events was confirmed. For patients who died with none of the above events confirmed, data were censored on the date of death.
This study was designed to test the hypothesis that switching to anastrozole from tamoxifen does not worsen outcomes (non-inferiority) or improves outcomes (superiority). Non-inferiority in terms of DFS, OS, and RFS was to be tested at the acceptable upper limit of the hazard ratio (anastrozole group vs. tamoxifen group) of 1.1 and a significance level of 2.5% (one-sided). We initially set the target number of patients at 2,500. Because recruitment was slower than anticipated and the results of other clinical trials comparing tamoxifen with aromatase inhibitors appeared, we decided to terminate accrual at the end of 2005 after an accrual of a total of 706 patients. Statistical considerations were amended in October 2007 on the basis of the following reported hazard ratios of aromatase inhibitors versus tamoxifen: 0.68 in the IES031 [9], 0.60 in the ARNO95/ABCSG8 [8], and 0.35 in the ITA [7]. The numbers of events required to demonstrate the non-inferiority of anastrozole to tamoxifen at a hazard ratio of 1.1 were 51 and 85, respectively, assuming a hazard ratio of anastrozole over tamoxifen of 0.50 or 0.60, an alpha value of 0.025 (unilateral), and a power of 80%, based on the method of Lakatos and Lan [16]. Sixty-five or 120 events were required to demonstrate the superiority of anastrozole over tamoxifen under the same conditions. An interim analysis of efficacy endpoints was planned when the 50% of the estimated events were reached so that the disadvantageous treatment arm would not be continued if the interim results failed to demonstrate non-inferiority of the anastrozole group on the basis of Bayesian predictive power less than 5 to 10% or if the anastrozole group showed remarkable superiority over the tamoxifen group.
Results
Patients
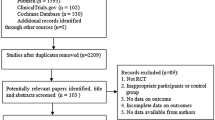
From November 2002 through December 2005, a total of 706 patients (tamoxifen group, n = 352; anastrozole group, n = 354) were recruited at 71 institutes in Japan. Three patients in the tamoxifen group and seven in the anastrozole group did not start the allocated treatment and were excluded from analysis. The full analysis set thus consisted of 696 patients (tamoxifen group, n = 349; anastrozole group, n = 347). The demographic characteristics of the patients are shown in Table 1. Baseline characteristics were well balanced between the two groups.
Efficacy endpoints
The present analysis was conducted at a median follow-up period of 42 months (range, 3.2–60 months) according to the statistical amendment described above. There were 26 DFS-related events in the anastrozole group as compared with 37 in the tamoxifen group, and 15 RFS-related events in the anastrozole group as compared with 28 in the tamoxifen group. The unadjusted hazard ratios were 0.69 (95% CI, 0.42 to 1.14; P = 0.14 by the log-rank test) for DFS (Fig. 2) and 0.54 (95% CI, 0.29–1.02; P = 0.06 by the log-rank test) for RFS (Fig. 3), both in favor of anastrozole. Distribution of events was shown in Table 2. There was no significant difference in OS (P = 0.59). The estimated 3-year rate of DFS was 90.7% (95% CI, 87.5–93.8%) in the tamoxifen group and 94.3% (95% CI, 91.7–96.9%) in the anastrozole group. The estimated 3-year rate of RFS was 93.1% (95% CI, 90.3–95.8%) in the tamoxifen group and 96.6% (95% CI, 94.6–98.6%) in the anastrozole group. There were four deaths in the anastrozole group, including one due to breast cancer, as compared with six deaths in the tamoxifen group, including three due to breast cancer. The estimated 3-year rate of OS was 98.8% (95% CI, 97.5–100%) in the tamoxifen group and 99.6% (95% CI, 98.8–100%) in the anastrozole group. On the basis of these results, the independent data-monitoring committee recommended to make this analysis to be final and to release the data.

Kaplan–Meier probability of disease-free survival. TAM tamoxifen, ANA anastrozole

Kaplan–Meier probability of relapse-free survival. TAM tamoxifen, ANA anastrozole
A subgroup analysis was planned to explore the interactions of anastrozole or tamoxifen with stratified factors on disease-free survival (Fig. 4). The beneficial effect of anastrozole over tamoxifen was suggested in node-positive patients, those who were younger than 60 year old, those who have had mastectomy, those who had tamoxifen administration for 1–2 years or those who have had adjuvant chemotherapy.

Subgroup analysis of disease-free survival. The hazard ratio was not able to be estimated in subgroups of stage IIIA and Her2 3+ , because of the lack of event in the anastrozole group. TAM tamoxifen, ANA anastrozole
Safety endpoints
Predefined adverse events which were collected prospectively are summarized in Table 3. Menopausal symptoms such as hot flashes and vaginal discharge were more common in the tamoxifen group (44.7 vs. 36.3% and 24.4 vs. 16.1%), and arthralgia was more common in the anastrozole group (31.8 vs. 50.4%), of which differences were statistically significant. There were no thromboembolic events in the tamoxifen group, and there was one grade four event in the anastrozole group. The number of patients who had bone fractures was nine in tamoxifen group and five in anastrozole group. Contralateral breast cancer was reported in two patients in the tamoxifen group and two in the anastrozole group. Second malignancies other than contralateral breast cancer were reported in seven patients in the tamoxifen group (including one endometrial cancer) and seven in the anastrozole group (including no endometrial cancer).
Discussion
The role of tamoxifen as the gold standard for adjuvant hormonal treatment in postmenopausal women with early breast cancer has been challenged by aromatase inhibitors in several clinical trials. The use of aromatase inhibitors was consistently associated with a modest decrease in disease recurrence as compared with tamoxifen. There are three basic treatment strategies for aromatase inhibitors: aromatase inhibitors can be given from the start of adjuvant treatment for 5 years (initial strategy); aromatase inhibitors can be given after initial treatment with tamoxifen for a combined total of 5 years (switch strategy); or aromatase inhibitors can be given after 5 years of treatment with tamoxifen.
In this study, we compared tamoxifen for 5 years with tamoxifen for 1 to 4 years, followed by anastrozole for a total treatment period of 5 years in Japanese population (switch strategy). The unadjusted hazard ratio was 0.69 (95% CI, 0.42–1.14) for DFS and 0.54 (95% CI, 0.29–1.02) for relapse-free survival (RFS), both in favor of anastrozole. The range of the 95% CI was large because of the relatively small number of events, but the hazard ratio of 0.69 for DFS in our study was in line with the results of previous clinical trials in which tamoxifen was switched to aromatase inhibitors [7–9, 17, 18]. Therefore, our study provides the first evidence that switching to aromatase inhibitor from tamoxifen is as effective in Asian women as in Western women irrespective of ethnic differences in polymorphisms of the CYP2D6 or CYP19 genes, and also suggests that aromatase inhibitors would also be effective in the initial strategy.
A planned subgroup analysis suggested that progesterone receptor status did not influence the efficacy of anastrozole. Benefit of anastrozole seen in patients with node positive, those who have had mastectomy or adjuvant chemotherapy suggested that the superiority of anastrozole was evident in patients with more advanced disease. We could assess the better timing to switch to anastrozole by this subgroup analysis which has not been reported previously, because the duration of tamoxifen therapy in the present study was allowed between 1 and 4 years.
Data on predefined adverse events were prospectively collected to monitor the safety profile of anastrozole as compared with that of tamoxifen. Overall, the safety profile was similar to that obtained in studies of Western women in terms of menopausal symptoms and arthralgia, but there were some differences. Hot flashes and vaginal discharge were more common in the tamoxifen group. Arthralgia was more common and more severe in the anastrozole group. In contrast to the studies conducted in Western countries, the fracture rate was lower in the anastrozole group (n = 5) than in the tamoxifen group (n = 9), also this difference was not statistically significant. Vertebral fractures occurred in one patient in the anastrozole group and three in the tamoxifen group. Hip fractures occurred in zero patients in the anastrozole group and one in the tamoxifen group. The reason for the lower frequency of fractures in the anastrozole group is unclear. This might have happened by chance, or because patients who required medication for osteoporosis were excluded, or because Japanese women who receive anastrozole are less likely to have bone fractures. The last hypothesis is supported by the presence of ethnic differences in the baseline fracture risk, with Asian populations having the lowest risk [19]. Further studies are needed to draw firm conclusions, but this issue is important because the risk of bone fractures, one of the most serious adverse effects of anastrozole, might be negligible in Japanese women. Another important finding of our study was that the incidence of thromboembolic events was very low in both groups, i.e., only one patient in anastrozole group or 0.14% of the entire study group. Because the baseline risk of idiopathic deep venous thrombosis in Asians is much lower than that in whites [20], our results suggest that the risk of deep venous thrombosis, one of the most serious toxic effects of tamoxifen, may be negligible in Japanese women.
In conclusion, our study provided additional evidence that switching to anastrozole from tamoxifen for a total treatment period of 5 years is likely to be of benefit for postmenopausal Japanese women with early breast cancer actually being treated with tamoxifen than continued treatment with tamoxifen for 5 years. The toxicity profile of this regimen in Japanese women differed in some respects with that previously reported in Western women.
References
The editorial board of the cancer statistics in Japan (2008) Cancer statistics in Japan, 2008. Foundation for promotion of cancer research, Tokyo, p 35
Berry DA, Cronin KA, Plevritis SK et al (2005) Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med 353:1784–1792
Fisher B, Costantino JP, Wickerham DL et al (1998) Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst 90:1371–1388
Early Breast Cancer Trialists’ Collaborative Group (2005) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 365:1687–1717
The Arimidex, Tamoxifen, Alone or in Combination (ATAC) Trialists’ Group (2008) Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol 9:45–53
Coates AS, Keshaviah A, Thürlimann B et al (2007) Five years of letrozole compared with tamoxifen as initial adjuvant therapy for postmenopausal women with endocrine-responsive early breast cancer: update of study BIG 1–98. J Clin Oncol 25:486–492
Boccardo F, Rubagotti A, Puntoni M et al (2005) Switching to anastrozole versus continued tamoxifen treatment of early breast cancer: preliminary results of the Italian Tamoxifen Anastrozole Trial. J Clin Oncol 23:5138–5147
Jakesz R, Jonat W, Gnant M et al (2005) Switching of postmenopausal women with endocrine-responsive early breast cancer to anastrozole after 2 years’ adjuvant tamoxifen: combined results of ABCSG trial 8 and ARNO 95 trial. Lancet 366:455–462
Coombes RC, Hall E, Gibson LJ et al (2004) A randomized trial of exemestane after two to three years of tamoxifen therapy in postmenopausal women with primary breast cancer. N Engl J Med 350:1081–1092
Goetz MP, Rae JM, Suman VJ et al (2005) Pharmacogenetics of tamoxifen biotransformation is associated with clinical outcomes of efficacy and hot flashes. J Clin Oncol 23:9312–9318
Broly F, Gaedigk A, Heim M et al (1991) Debrisoquine/sparteine hydroxylation genotype and phenotype: analysis of common mutations and alleles of CYP2D6 in a European population. DNA Cell Biol 10:545–558
Yokota H, Tamura S, Furuya H et al (1993) Evidence for a new variant CYP2D6 allele CYP2D6 J in a Japanese population associated with lower in vivo rates of sparteine metabolism. Pharmacogenetics 3:256–263
Ma CX, Adjei AA, Salavaggione OE et al (2005) Human aromatase: gene resequencing and functional genomics. Cancer Res 65:11071–11082
Moy B, Tu D, Pater JL et al (2006) Clinical outcomes of ethnic minority women in MA.17: a trial of letrozole after 5 years of tamoxifen in postmenopausal women with early stage breast cancer. Ann Oncol 17:1637–1643
Sobin LH, Fleming ID (1997) TNM classification of malignant tumors, 5th edn. Wiley, New York
Lakatos E, Lan KK (1992) A comparison of sample size methods for the logrank statistic. Stat Med 11:179–191
Boccardo F, Rubagotti A, Guglielmini P et al (2006) Switching to anastrozole versus continued tamoxifen treatment of early breast cancer. Updated results of the Italian tamoxifen anastrozole (ITA) trial. Ann Oncol 17(Suppl 7):vii 10–vii 14
Coombes RC, Kilburn LS, Snowdon CF et al (2007) Survival and safety of exemestane versus tamoxifen after 2–3 years’ tamoxifen treatment (Intergroup Exemestane Study). Lancet 369:559–570
Barrett-Connor E, Siris ES, Wehren LE et al (2005) Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res 20:185–194
White RH, Zhou H, Romano PS (1998) Incidence of idiopathic deep venous thrombosis and secondary thromboembolism among ethnic groups in California. Ann Intern Med 128:737–740
Acknowledgments
We are indebted to all women who participated in the study. We thank all physicians contributing to this trial. We thank Mizuki Yamauchi and Yumiko Nomura for data management, and Hitoshi Masuda for his editorial assistance. This study was funded by Comprehensive Support Project for Oncology Research (CSPOR) of Public Health Research Foundation. The corporate and individual sponsors of this study are listed on the CSPOR website (http://www.csp.or.jp/cspor/kyousan_e.html). The pharmaceutical manufacturer/distributor who had provided financial contribution as a corporate sponsor took no part in this study other than providing information relevant to proper use of the study drugs. All decisions concerning the planning, implementation and publication of this study were made by the executive committee of this study.
Author information
Authors and Affiliations
Corresponding author
Appendix
Rights and permissions
About this article
Cite this article
Aihara, T., Takatsuka, Y., Ohsumi, S. et al. Phase III randomized adjuvant study of tamoxifen alone versus sequential tamoxifen and anastrozole in Japanese postmenopausal women with hormone-responsive breast cancer: N-SAS BC03 study. Breast Cancer Res Treat 121, 379–387 (2010). https://doi.org/10.1007/s10549-010-0888-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-010-0888-x