
Abstract
Tamoxifen reduces primary breast cancer incidence, yet causes serious side effects. To date, few women with increased breast cancer risk have elected to use tamoxifen for chemoprevention. The objective of the study was to determine women’s knowledge of and attitudes toward tamoxifen following exposure to a tailored decision aid (DA). A total of 632 women with a 5-year risk of breast cancer ≥1.66% (Mean = 2.56, range = 1.7–17.3) were recruited from two healthcare organizations. Participants viewed an online DA that informed them about their 5-year risk of breast cancer and presented individually tailored content depicting the risks/benefits of tamoxifen prophylaxis. Outcome measures included behavioral intentions (to seek additional information about tamoxifen, to talk to a physician about tamoxifen, and to take tamoxifen); knowledge; and perceived risks and benefits of tamoxifen. After viewing the DA, 29% of participants said they intended to seek more information or talk to their doctor about tamoxifen, and only 6% believed they would take tamoxifen. Knowledge was considerable, with 63% of women answering at least 5 of 6 knowledge questions correctly. Participants were concerned about the risks of tamoxifen, and many believed that the benefits of tamoxifen did not outweigh the risks. This study is the largest to date to test women’s preferences for taking tamoxifen and one of the largest to have tested the impact of a tailored DA. After viewing the DA, women demonstrated good understanding of tamoxifen’s risks and benefits, but most were not interested in taking tamoxifen for breast cancer chemoprevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
For almost 10 years, tamoxifen has been available as primary prophylaxis for women at increased risk of breast cancer. While approximately 10 million women are eligible for tamoxifen prophylaxis [1], few are willing to take tamoxifen [2–5]. Preliminary evidence suggests that women are reluctant to take tamoxifen in part out of concern about side effects [2, 4–6]—endometrial cancer, pulmonary embolism, stroke, deep vein thrombosis, cataracts, hormonal symptoms, and sexual problems—even though the serious risks are rare [3, 4, 7]. Indeed, women frequently overestimate the likelihood of these side effects [2].
Women are also reluctant to take tamoxifen because they lack confidence in its ability to prevent breast cancer [4, 7]. In one study, less than half of participants were confident that tamoxifen could reduce their cancer risk [4]. In another study, only half correctly described how much tamoxifen could reduce their cancer risk [2].
Several studies have used brief educational interventions to improve women’s knowledge of tamoxifen’s risks and benefits; none significantly increased the number of women willing to take tamoxifen [2–4]. Thus, even women who are knowledgeable about the pros and cons of tamoxifen may still forgo it. Methodological limitations, however, call into question the generalizability of these educational interventions. First, two of the studies had small sample sizes (n < 50), making it difficult to discern the true level of interest in tamoxifen [2, 3]. Second, the interventions were brief, raising questions as to whether women had enough information to make such a complex decision. Third, only one intervention included tailored estimates of the risks and benefits of tamoxifen (i.e., statistics based on each woman’s medical history rather than population-based) [3]. Tailored information is critical in this context, because the risks and benefits of tamoxifen vary significantly across women. Without tailoring, women may conclude that the risks and benefits do not apply to them, thereby decreasing the intervention’s effectiveness.
This study assesses high-risk women’s attitudes about tamoxifen after exposure to a comprehensive, tailored decision aid (DA) for tamoxifen chemoprevention. We had no a priori hypotheses regarding how our DA would affect behavioral intentions, and did not design the DA to persuade women to take tamoxifen. Instead, our aim was to present balanced information to increase women’s knowledge regarding tamoxifen’s risks and benefits and to determine whether women who were knowledgeable about the risks and benefits of tamoxifen would be willing to take it to prevent breast cancer.
Methods
Overview
We recruited women at high risk of developing a primary breast cancer in the next 5 years from two large health care organizations. Participants whose 5-year risk was ≥1.66% (estimated by the Gail model [8]) received an online, tailored DA, entitled “Guide to Decide.” After reading the DA, women answered questions about their behavioral intentions, knowledge, and risk perceptions regarding tamoxifen.
Development of the DA
Design
The DA educated women about their 5-year risk of breast cancer, and the risks and benefits of taking tamoxifen. The DA (a pdf version is available at www.cbdsm.org/downloads/tamoxifenda.pdf) described cancer, breast cancer, and the risk factors for breast cancer. The DA then gave women their individually tailored 5-year risk of breast cancer, as determined by participants’ Gail Model score [9] (emphasizing the number was a 5-year, rather than lifetime, risk). Next, the DA described tamoxifen (i.e., a drug that has been used for several decades, was first used to prevent recurrence, and has recently been shown to prevent primary breast cancer), how it works, and how it has been studied (i.e., the P1 trial methodology and results) [9]. Then, the DA presented tailored estimates (age- and race-based) of the risks/benefits of tamoxifen for endometrial cancer, blood clotting problems (stroke, pulmonary embolism, deep vein thrombosis), hormone symptoms, sexual side effects, breast cancer, and bone fractures (see Table 1, for examples). The risk and benefit information was presented in a table format or in a pictograph that displayed the number of individuals who would experience a risk or benefit from tamoxifen. In all cases, participants were given the baseline chance of any of the health conditions occurring, as well as the likelihood of the health conditions occurring if one was to take tamoxifen.
We tested five methods for communicating the risks and benefits of tamoxifen using a 16-arm fractional factorial design. These factors were: (1) pictograph versus table presentation of risk/benefits, (2) incremental versus total risk presentation (i.e., highlighting the incremental risk/benefit of tamoxifen vs. just giving overall risk statistics), (3) statistics using denominator of 100 versus 1000, (4) order of risks and benefits (i.e., risks vs. benefits presented first), and (5) presence/absence of contextual information (i.e., whether participants received statistics about colon cancer, heart attack, and all cause mortality). Results by factor are presented elsewhere [10]. Here, we collapse the data across all factors to assess the overall impact of the DA on women’s behavioral intentions, knowledge, and risk perceptions.
Pre-testing
Breast cancer experts reviewed the DA for accuracy and balance. We then tested it in four racially and socioeconomically diverse focus groups. Finally, we conducted usability testing with 10 women to measure study duration, ensure participants interpreted the questions as intended, and assess their perception of the online DA.
Intervention study
Recruitment
Participants were recruited from two large healthcare organizations (Henry Ford Health System in Michigan and Group Health in Washington state) associated with the National Cancer Institute’s Cancer Research Network. After obtaining IRB approval, we used electronic medical data to determine a preliminary 5-year risk of breast cancer and whether women had contraindications to tamoxifen (i.e., renal or liver disease, history of pulmonary embolism, or deep vein thrombosis). Eligible women received invitation letters with a study description, website address, username, and password. Non-responders received a second letter of invitation. Interested women logged in and were screened for eligibility. Women aged 40–74 (the approved ages for tamoxifen prophylaxis) whose 5-year risk was >1.66% (based on the risk level used in the NSABP P-1 study) were eligible to continue [8]. Exclusion criteria included prior history of breast cancer or tamoxifen use, contraindications to tamoxifen, participation in the STAR trial [11], or terminal illness.
Procedure
After providing informed consent, participants completed a baseline questionnaire and were randomized to view one of the 16 versions of the DA. Each version contained the same basic information, but differed in the presentation of numerical risk/benefit information. After reviewing the DA, participants completed a post-test containing measures developed by the investigators, and psychometrically tested in a pilot study of several hundred women.
Measures
Behavioral intentions
Intentions were measured with three questions: (1) “How likely are you to look for more information about tamoxifen (for example, use the Internet, call the numbers listed on the website, etc.)?"; (2) “How likely are you to talk to your doctor about tamoxifen?"; and (3) “Given what you know right now, how likely do you think you are to take tamoxifen in the next year?” Responses ranged from 1 = “not at all likely” to 5 = “extremely likely”. Questions were averaged to form a composite measure. The reliability coefficient (alpha) was 0.82. In some analyses, answers were dichotomized (1–3 = unlikely to engage in behavior, and 4–5 = likely to engage in behavior).
Actual behavior
Three months following their participation in the study, participants were e-mailed a link to a short (10-min) survey. Three questions inquired of their tamoxifen-related health behaviors during the past 3 months: whether or not they looked for more information about tamoxifen, talked to their doctor about tamoxifen, and/or began taking tamoxifen.
Knowledge
Knowledge was assessed with four questions about the risks of tamoxifen (endometrial cancer, hormonal symptoms, blood clotting problems, and cataracts), and two about the benefits (breast cancer, and broken bones). Participants indicated who were more likely to experience each risk and benefit: (1) women who take tamoxifen, (2) women who do not take tamoxifen, (3) both groups are equally likely, and (4) don’t know. Responses were scored as correct or incorrect (don’t know was coded as incorrect), and correct responses were summed. The reliability coefficient (alpha) was 0.85.
Perceptions of the risks and benefits
Participants indicated how likely they were to get breast cancer and how worried they would be about experiencing side effects if they did or did not take tamoxifen. These four questions used 5-point Likert scales (1 = ‘not at all’ to 5 = ‘extremely’). Finally, we asked “How good of a choice is taking tamoxifen as a way to reduce your chance of getting breast cancer?” (1 = “For me it is not a good choice at all” to 5 = “For me it is an extremely good choice.”)
Reasons for not taking tamoxifen
Among women who indicated they were unlikely to take tamoxifen, we assessed five reasons: (1) “I don’t like the idea of taking pills every day”; (2) “It is better to do without medicines”; (3) “I find it a nuisance to take a pill every day”; (4) “I am worried about the side effects of tamoxifen”; and (5) “I don’t think the benefits of tamoxifen are worth the risks of tamoxifen.” Responses ranged from 1 = “strongly disagree” to 5 = “strongly agree”.
Analyses
This article provides a numerical and graphical summary of the data using means, standard deviations, bar plots, and two-way tables. Chi-square analyses tested for differences in intentions to engage in tamoxifen-related behavior. In chi-square analyses, we trichotomized Gail score (<2.0, 2.0–2.9, 3.0+) and dichotomized age (<60, ≥60). Logistic regression was used to test for impact of knowledge on intention to take tamoxifen.
In our analyses, 19% of women indicated that tamoxifen would not reduce their breast cancer risk. This suggests some participants either did not read the DA, did not understand the content, or did not believe tamoxifen would reduce their risk of breast cancer. We performed a sensitivity analysis excluding these women. The results were qualitatively similar to the main analysis; thus, in the results section below we present data from the full sample.
Cases were included in analyses based on whether each individual variable was answered. Thus, for each analysis the N differed. Missing data was ≤7% for all variables.
Results
Participants
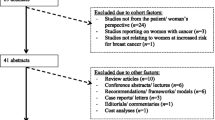
Of the 8,896 women who received an invitation letter, 1,218 (14%) visited the website. Of these, 749 (61%) were eligible and 663 (89% of eligible) consented to participate. Ultimately, 632 participants (84%) completed the post-test. The DA and the post-test took an average of 49 min to complete (range = 15–173; 78 subjects who took ≥3 h were excluded from the timing analysis, assuming that they left their computers but were included in all the analyses described in this article).
Table 2 describes the sample’s demographic characteristics. Participants were on average 58.9 years old, White, and well-educated. Gail scores ranged from 1.7–17.3 (M = 2.56, SD = 1.26).
Behavioral intentions
After viewing the DA, 28.8% indicated they were likely to look for more information about tamoxifen, and 29.5% indicated they were likely to talk to their physician about tamoxifen (see Fig. 1). However, only 5.8% of participants indicated they were likely to take tamoxifen in the next year. As previously found [2–4], few women were interested in seeking more information about tamoxifen, and even fewer had interest in taking tamoxifen.

Percent of women expressing interest in tamoxifen
We found a positive relationship between Gail scores and desire to talk to a physician about tamoxifen (χ2 = 7.31, P < .03, Fig. 2). However, there was no association between Gail scores and intention to look for information or take tamoxifen. We also found that women under 60 years of age were more likely to believe they would take tamoxifen (χ2 = 4.32, P < .04).

Percent of women expressing interest in tamoxifen by Gail score
Actual behavior
At 3 months, 0.9% (N = 3) of participants had started taking tamoxifen, 5.8% of participants had talked with their physician, and 5.4% had looked for more information. Neither Gail score nor age significantly predicted any of these three behaviors. However, an examination of the relationship between Gail scores and behavior reveals a non-significant trend. Specifically, compared to those with the lowest scores (<2 and 2.0–2.9) those with highest Gail scores (3.0 and higher) had notably higher rates of having looked for additional information (4.0%, 4.3%, 10.6%) or of having talked with their doctor (4.8%, 4.4%, 10.6%), compared to those with lower Gail scores.
Knowledge
One reason for the low level of interest in taking tamoxifen could have been that, even after reviewing our DA, women were unaware of tamoxifen’s risk and benefits. In order to test this possibility, we examined participants’ knowledge of tamoxifen’s risks and benefits. Participants answered, on average, 4.31 (SD = 2.01) of the six questions correctly. Sixty-three percent of the participants answered at least five questions correctly, and 41.4% answered all six correctly (Fig. 3). Knowledge was the highest for awareness that tamoxifen decreases breast cancer (81.0% accuracy) and lowest for awareness that it increases the frequency of cataracts (68.0% accuracy). Thus, most participants had substantial knowledge about tamoxifen’s risks and benefits, especially breast cancer risk reduction.

Percent of women answering each knowledge question correctly
There was no relationship between knowledge and participants’ likelihood of seeking more information or talking with their doctor. There was a significant relationship between knowledge and participants’ intention to take tamoxifen. We first examined whether those with poor knowledge of the risks and benefits were more likely to indicate a desire to take tamoxifen. While only 3% of the sample answered all the six questions incorrectly, they made up 9% of those who indicated they were likely to take tamoxifen. After controlling for the five factors in a logistical regression, knowledge predicted willingness to take tamoxifen (OR = 0.31, P = .08). Similarly, when examining people’s response to only the risk questions, we found that while only 13% of the sample answered all the four risk questions incorrectly, these participants composed 31.4% of those who indicated that they were likely to take tamoxifen (OR = 0.22, P < .001). Finally, when limiting our analysis to the benefit questions, we found that 11% of the sample answered both questions incorrectly, yet they composed 17% of those who indicated a desire to take tamoxifen. However, this was not a significant trend. Taken together, these results suggest that those who are relatively uninformed about tamoxifen were most likely to be interested in taking it. Given that only three women began taking tamoxifen, analyses of the impact of knowledge on actual behavior (i.e., taking tamoxifen) are not possible.
Subjective perceptions of the risks and benefits of tamoxifen
Another explanation for the low level of interest in taking tamoxifen may be participants’ subjective perceptions of the risks and benefits of tamoxifen. A person may know tamoxifen reduces breast cancer risk in most women, but still believe it would not decrease her own risk. We analyzed responses to two questions asking participants to rate the likelihood of being diagnosed with breast cancer if they did or did not take tamoxifen. Difference scores between these variables showed a majority of participants (56.0%) perceived their own risk of breast cancer would decrease if they took tamoxifen; however, 38.3% had difference scores of zero, indicating that they believed they would not experience a change in their risk. Participants who believed their risk of breast cancer would decrease by taking tamoxifen were more likely to say they would look for information, talk to their doctor, or take tamoxifen (F’s = 30.39–42.54, P’s < .001).
The likelihood of experiencing side effects was perceived to be moderate (M = 3.28, SD = 1.03). However, participants reported high levels of worry about developing side effects (M = 4.06, SD = 0.95). Furthermore, 60% of participants believe tamoxifen was not a good choice for them (M = 2.22, SD = 1.10); only 12.8% believed it was a good choice.
Other reasons for not taking tamoxifen
Eighty percent of women who indicated that they were unlikely to take tamoxifen expressed worry about side effects, and 58.8% indicated that the benefits were not worth the risks. In addition, 40.1% disliked the idea of taking pills everyday, 28.2% felt it is better to do without medicines, and 22.9% felt it is a nuisance to take a pill everyday.
Discussion
After receiving a detailed, individually tailored, online DA, most of our participants—women at high risk for breast cancer—understood that tamoxifen reduces the risk of cancer and believed that tamoxifen would lower their own breast cancer risk. Still, they had little interest in taking tamoxifen and even fewer actually took tamoxifen (or even looked for more information or talked with their physician). Thus, even when adequately informed about tamoxifen, many women at elevated risk are unwilling to accept the risks of tamoxifen to reduce their breast cancer risk. These findings extend previous studies, which have demonstrated that most women are not interested in taking to tamoxifen to prevent primary breast cancer [2–4]. Again, similar to previous study, we found that women’s reluctance was due to concerns about side effects and the belief that the risks outweigh the benefits. Our results go beyond previous studies in that women received a very detailed DA that included individually tailored risk/benefit information. Furthermore, our sample size was significantly greater than that of previous studies and included participants recruited from two geographically distinct sites (Seattle and Detroit).
Although many women were reluctant to take tamoxifen, almost a third expressed a desire to learn more. These women were more likely to have a higher 5-year risk of breast cancer and to be younger. Finally, and disconcertingly, we found evidence that our study participants who had poor knowledge of tamoxifen’s risks were more likely to be interested in taking tamoxifen.
Our participants’ lack of interest in tamoxifen does not mean that our DA failed. The DA was not designed to convince women to take tamoxifen. It was designed to neutrally present risk and benefit information, so that participants could decide, for themselves or with their doctors, whether tamoxifen was a good option. DAs such as ours help people make “preference sensitive decisions,” where the right choice depends on a patient’s values [12]. The goal is not to lead people toward one treatment, but to help them weigh their options. By this measure, the Guide to Decide demonstrated that when women are informed of their potential risks and benefits in the context of a computerized decision-aid, few seem interested in tamoxifen.
Although this study provides one of the first tests of a tailored DA in a large, geographically diverse population, our study does have several limitations. First, our sample comprised mostly of White women. Low recruitment of African American women has plagued other studies [2–4] including the NSABP P-1 trial of tamoxifen [9]. A second limitation was the use of an online DA. While web-based DAs can ultimately increase intervention reach, this modality limits participation to only those with Internet access. Third, our sample included only women with health care coverage. These limitations led to a relatively educated sample and a low response rate. In fact, we believe that one of the primary reasons for our low response rate is lack of Internet access or lack comfort with using the Internet. More specifically, we believe that one reason for a lack of lower educated women in our sample is due to their lack of access to the Internet. However, it is important to note that even Internet studies that target Internet users often show low response rates [13]. Other reasons include lack of interest on the topic or lack of time to complete a 30–60 min study (as described in the recruitment letter). Thus, our findings may not be generalizable to women of other racial and ethnic groups and to less educated or economically disadvantaged women. That said, we would expect our sample to be biased in favor of women who are more likely to consider using tamoxifen, since they had access to drug coverage. Still, only 6% were interested in taking tamoxifen. Fourth, this study did not include a control group. Past research has shown that DAs increase knowledge and influence treatment decisions [14]. Owing to a somewhat limited pool of eligible participants, we chose to expose all women to various versions of the DA. This decision allows comparison across presentation formats (data not presented here), but prevents us from comparing the results to those from women not exposed to this content. A final limitation is our decision to use the Gail Model to determine the risk of breast cancer. Our choice was based on the use of this model in the NSABP P-1 trial to determine women who are eligible for tamoxifen [9].
In summary, our results show that the women in our study, after being exposed to a state-of-the-art DA (complete with tailored statistics), were largely uninterested in taking tamoxifen to prevent breast cancer. This reluctance may be due to an informed decision that has carefully weighed the risks and benefits of tamoxifen. Whether these same attitudes will influence women’s acceptance of similar chemoprevention strategies (e.g., raloxifene) remains to be seen.
References
Freedman AN, Graubard BI, Rao SR, McCaskill-Stevens W, Ballard-Barbash R, Gail MH (2003) Estimates of the number of U.S. women who could benefit from tamoxifen for breast cancer chemoprevention. J Natl Cancer Inst 95(7):526–532
Rush Port E, Montgomery LL, Heerdt AS, Borgen PI (2001) Patient reluctance toward tamoxifen use for breast cancer primary prevention. Ann Surg Oncol 8(7):580–585
Stacey D, O’Connor AM, De Grasse C, Verma S (2003) Development and evaluation of a breast cancer prevention decision aid for higher-risk women. Health Expect 6:3–18
Melnikow J, Paterniti D, Azari R et al. (2005) Preferences of women evaluating risks of tamoxifen (POWER) study of preferences for tamoxifen for breast cancer risk reduction. Cancer 103(10):1996–2005
Bober SL, Hoke LA, Duda RB, Regan MM, Tung NM (2004) Decision-making about tamoxifen in women at high risk for breast cancer: clinical and psychological factors. J Clin Oncol 22(24):4951–4957
Salant T, Ganschow PS, Olopade OI, Lauderdale DS (2006) “Why take it if you don’t have anything?” Breast cancer risk perceptions and prevention choices at a public hospital. J Gen Intern Med 21:779–785
Metcalfe KA, Snyder C, Seidel J, Hanna D, Lynch HT, Narod S (2005) The use of preventative measures among healthy women who carry BRCA1 or BRCA2 mutation. Familial Cancer 4:97–103
Gail MH, Brinton LA, Byar DP et al (1989) Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst 81(24):1879–1886
Fisher B, Costantino JP, Wickerham DL et al (1998) Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst 90(18):1371–1388
Zikmund-Fisher BJ, Ubel PA, Smith DM et al (2008) Communicating side effect risks in a tamoxifen prophylaxis decision aid: the debiasing influence of pictographs. Patient Educ Couns 73(2):209–214
Vogel VG, Costantino JP, Wickerham DL et al (2006) Effects of tamoxifen vs. raloxifene on the risk of developing invasive breast cancer and other disease outcomes. J Am Med Assoc 295(23):2727–2741
Wennberg JE (2002) Promoting Disease Management in Medicare. Testimony before the Subcommittee on Health of the House Committee on Ways and Means, vol 2002
Couper M, Miller P (2008) Web survey methods. Public Opin Q 72(5):831–835
O’Connor AM, Rostom A, Fiset V et al (1999) Decision aids for patients facing health treatment or screening decisions: systematic review. Br Med J 319(7212):731–734
Acknowledgments
We thank Drs Victor Strecher, Priti Shah, and Mick Couper for their assistance with study design. The Center for Heath Communication Research (especially Michael Nowak) did an excellent job turning our DA into a well-designed and easily navigated web site. We also thank Roy Pardee and Rick Krajenta for their assistance with compiling the databases of eligible participants. We express our gratitude to the Department of Radiology at Henry Ford Health System, particularly Dr. Matthew Burke, for their help in identifying eligible patients. Finally, we are very grateful to all the women who participated in this study. Financial support for this study was provided by a grant from the National Institutes for Health (P50 CA101451). Drs. Fagerlin and Smith were supported by MREP early career awards from the U.S. Department of Veterans Affairs. Dr. Zikmund-Fisher is supported by a career development award from the American Cancer Society. The funding agreements insured the authors’ independence in designing the study, interpreting the data, and publishing the report.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fagerlin, A., Zikmund-Fisher, B.J., Smith, D.M. et al. Women’s decisions regarding tamoxifen for breast cancer prevention: responses to a tailored decision aid. Breast Cancer Res Treat 119, 613–620 (2010). https://doi.org/10.1007/s10549-009-0618-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-009-0618-4