
Abstract
Genetic testing for BRCA1 and BRCA2 mutations in family members of individuals with known deleterious mutations can distinguish between patients at high risk of disease and those who are not. Some studies have suggested that individuals testing negative for known familial mutations (true negatives), may still have a higher risk of breast cancer (BC) than the general population. We have examined a prospectively followed cohort of true negative women in the US. Subjects were close relatives of known BRCA1 and BRCA2 mutation carriers who had undergone genetic testing, were negative for the known familial mutation, and were unaffected at the time of genetic testing. Standardized incidence ratios (SIR) and 95% confidence intervals (CI) were calculated using SEER incidence rates. Among 375 true negatives, two invasive and two in situ BC and no ovarian cancers were diagnosed with mean follow up of 4.9 years (total of 1,962 person-years). Four invasive BC were expected, whereas two were observed, for an age-adjusted SIR of 0.52 (95% CI 0.13–2.09). We observed more cases of in situ BC (n = 2) than were expected (n = 0.9; SIR = 2.30; 95% CI 0.57–9.19). There were no cases of ovarian cancer observed; 0.4 case was expected. In this prospective study of women who were unaffected at the time of genetic testing and who were negative for the known familial mutation in BRCA1/2, no excess risk of invasive BC was observed. Our data suggest that such women in the US should adhere to population-based guidelines for breast cancer screening.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Genetic testing for BRCA1 and BRCA2 mutations allows for the identification of women at high risk for breast and ovarian cancer with subsequent alteration of clinical management. Prophylactic oophorectomy [1–3] and mastectomy [4, 5] have been shown to decrease the risk of ovarian and breast cancer, and breast MRI screening is more sensitive than mammography for the detection of cancer in women with documented mutations [6, 7]. An additional important benefit of genetic testing is the identification of individuals who are negative for mutations known to be segregating in their family. An unaffected individual who undergoes testing for a BRCA1 or BRCA2 mutation that is known to exist in the family and tests negative has long been considered a “true negative”. Unless there are other risk factors for the development of cancer present, these individuals have been counseled that they are at similar risk as the general population for both breast and ovarian cancer. The differences in these risks are significant; for example, true negatives are informed that instead of a lifetime risk of breast cancer of 44–75% seen in BRCA1/2 mutation carriers [8, 9], their risk is approximately 13% as seen in the general population. Similarly, the lifetime risk of ovarian cancer in a true negative is estimated at 1–2% instead of 20–45% in BRCA1 mutation carriers and 10–20% in BRCA2 mutation carriers [8, 9]. Therefore, in most situations, true negative women are counseled to follow the same screening guidelines as women in the general population.
The paradigm reviewed above has recently been called into question by several small studies that have suggested that true negatives may in fact be at a slightly elevated risk of breast cancer compared to the general population, with relative risks of approximately 2.0 being described [10–12]. The mechanism of this possible increased risk has been postulated to be alterations in modifier genes (distinct from BRCA1 and BRCA2) which are co-inherited with BRCA1 or BRCA2 mutations. The studies demonstrating these increased risks have been limited by small sample size or a retrospective design. As a major benefit of genetic testing for BRCA1 and BRCA2 is to identify true negatives to avoid unnecessary screening and preventative interventions (such as mastectomy, oophorectomy, and chemoprevention), a more complete analysis of this crucial issue is required. In order to address this issue, we describe the experience of a large cohort of true negatives who were prospectively followed after receiving their negative genetic test results.
Methods
Databases
All individuals undergoing genetic testing at the University of Pennsylvania and Memorial Sloan Kettering Cancer Center are offered enrollment in ongoing registries which allow for serial follow up. Over 95% of patients in both institutions agree to participate. Questionnaires are sent to patients on an approximately yearly basis. In these questionnaires, patients are asked about changes to their own personal history as well as any new cancers in the family. Women who do not respond to mailed questionnaires receive follow-up telephone calls, and medical records are reviewed to identify new diagnoses of cancer. Pathology reports are obtained for confirmation of new diagnoses.
Eligibility criteria
Women who had undergone genetic testing for BRCA1 and BRCA2 mutations and who had signed informed consent to participate in IRB approved research protocols at the University of Pennsylvania (IRB Protocol #376800) and Memorial Sloan Kettering Cancer Center (IRB Protocols 96-051 and 97-029) were considered for inclusion. Women were considered eligible if they: (1) had a close relative of an individual with a known deleterious BRCA1 or BRCA2 mutation; (2) had undergone genetic testing for the known family mutation in BRCA1 or BRCA2; (3) had at least one follow up since having genetic testing; (4) had no prior cancer diagnosis at the time of their genetic testing (apart from in situ cervical cancer or non-melanoma skin cancer); and (5) had not undergone bilateral mastectomy prior to genetic testing or subsequent to genetic testing.
Genetic testing
All patients were tested for the known mutation in the family by direct sequencing. Besides, all individuals of Ashkenazi Jewish descent were tested for the three founder mutations in BRCA1 (185delAG, 5382insC) and BRCA2 (6174delT).
Data collection
The following information was recorded: (1) exact mutation in family, (2) date of genetic testing, (3) development of cancer, (4) cancer type, (5) date of last follow up, and (6) self-identified race. True negatives were considered as having had follow up if either they or their first degree or second-degree relative specifically provided information regarding any new cancer diagnosis, or lack thereof, in the true negative.
Statistical analysis
Follow-up time was initiated at the date of genetic testing. Study subjects were censored at the time of cancer diagnosis or at the last date of contact, whichever came first. The number of observed cases was compared to the expected number of cases using standardized incidence ratios (SIR) and 95% confidence intervals (CI). CI were calculated using the quadratic approximation to the Poisson log likelihood for the log-rate parameter. Expected cases were based on SEER 13 incidence rates for invasive breast and ovarian cancer and for in situ breast cancer from 1992 to 2005 among women 18 years or older (“all races”). Data were also analyzed using SEER 13 rates for white women. Statistical analyses were performed in STATA 9.0.
Results
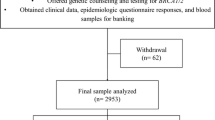
A total of 405 true negatives were identified in 249 families at the two centers, of which 378 (93%) had follow-up information, and whose characteristics are demonstrated in Table 1. Of these 378, 235 (62%) were identified at the University of Pennsylvania and 143 (48%) from Memorial Sloan Kettering Cancer Center. In 196 families, a single person tested negative, and in 54 two or more individuals were tested. Most families carried BRCA1 mutations (71.5%) and one family had both a BRCA1 and a BRCA2 mutation, but the subject included in this study was negative for both familial mutations. The median age at the time of genetic testing was 44 (range = 18–91). The mean follow-up time was 4.9 years (standard deviation = ±3.2, median = 4.5) with a total of 1,962 person-years of follow up.
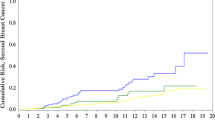
Two invasive breast cancers, two non-invasive breast cancers (ductal carcinoma in situ), and no ovarian cancers were diagnosed in the study group. According to SEER data, four invasive breast cancers were expected, whereas two were observed, for an age-adjusted SIR of 0.52 (95% CI 0.13–2.09) (Table 2). As 91% of patients were Caucasian, the analysis was also performed using SEER13 registry data among white women. Findings were very similar, with four expected invasive breast cancers and a SIR of 0.50 (95% CI 0.13–2.01).
One invasive cancer was diagnosed in a 42-year old woman who was negative for the familial BRCA1 mutation. Her tumor was estrogen receptor positive and HER2/neu positive with two positive lymph nodes. Following her diagnosis, the proband underwent repeat testing by comprehensive analysis which was negative for detectable BRCA1 or BRCA2 mutations. Her sister, mother, maternal aunt, and six maternal cousins all had ovarian cancer; in addition two maternal aunts and five maternal cousins had a diagnosis of breast cancer. All of those in the maternal lineage who underwent testing had the familial BRCA1 mutation. In addition to this very strong maternal history, the proband had one paternal aunt with breast cancer at age 50.
The second invasive breast cancer was in a 58-year old who tested negative for a familial 6174delT BRCA2 mutation and was diagnosed with a T3N3 tumor which was estrogen receptor (ER) positive and HER2/neu negative. Her sister had been affected with breast cancer at age 43 and was a documented mutation carrier. Her father had been diagnosed with breast and pancreatic cancer, and there was an extensive additonal history of breast and pancreatic cancer in her paternal lineage. Her maternal grandmother was reported to have been diagnosed with breast cancer at an unknown age, but her mother was unaffected by breast or ovarian cancer at age 82 and there was no other relevant history in that lineage.
We observed slightly more cases of in situ breast cancer (n = 2) than were expected (n = 0.9; SIR = 2.30; 95% CI 0.57–9.19). Similar findings were seen when examining only white women with 0.9 cases expected for a SIR of 2.23 (0.56–8.92). The first was diagnosed at age 45 with DCIS detected on routine screening mammogram which was ER and PR positive. She was negative for the known 185delAG BRCA1 mutation on the maternal side of the family on initial testing and on repeat testing following diagnosis. Her paternal history was notable for a father with prostate cancer at 68 and was otherwise unremarkable. The second case was woman diagnosed at age 53 with DCIS after testing negative for a BRCA2 6174del T mutation that had initially been identified in her sister, who had been diagnosed with bilateral breast cancer at ages 53 and 57. There was an extensive history of breast cancer in their mother (bilateral at ages 49 and 56), maternal aunt (age 43), and maternal great-aunt (age unknown). There was no history of cancer in her paternal lineage.
There were no cases of ovarian cancer observed, whereas 0.4 case was expected.
Nine of the 378 true negatives developed other (non-breast) cancers in the follow up: four non-melanoma skin cancers, two thyroid cancers, one each of melanoma, non-Hodgkin lymphoma, and renal cancer.
Discussion
In this study, we have found no increased risk of invasive breast cancer in women who did not inherit a known deleterious family mutation in BRCA1 or BRCA2 (true negatives). Our observations are in contrast to previous studies which have found a relative risk between 2 and 5. We did find a modestly elevated risk of DCIS, with a RR of 2, however, this result was not statistically significant.
The question of the risk of breast cancer in true negatives is of great importance to women undergoing genetic testing, and has significant implications for screening recommendations. Indeed, identification of true negatives is considered to be one of the major benefits of BRCA1 and BRCA2 testing, providing reassurance and the avoidance of unnecessary and costly screening and prevention strategies. However, if risk were to be elevated to the degree seen in previous studies of true negatives (relative risks of 2–5), screening recommendations may need to be altered, particularly outside of the United States where routine mammography often does not begin until after age 40. Our study provides data to support the current recommendations that true negatives adhere to population guidelines for breast cancer screening and does not support early or more intensive screening.
Our study differs from the previous studies in several ways. Smith et al. originally reported a retrospective series of 277 families in which 28 phenocopies were identified [10]. Phenocopies were defined in this situation as women who have breast cancer, but do not have the known familial mutation; they have the phenotype (breast cancer), but not the genotype (BRCA1 or BRCA2 mutation). BRCA1 or BRCA2 testing after the identification of a BRCA1 or BRCA2 mutation in the family found that 24% of women with breast cancer were phenocopies. The SIR for breast cancer for true negatives was calculated to be 5.3, with five breast cancers expected and 28 observed. After excluding families in which another source of familial risk could be identified (for example a paternal family history of breast cancer, in a family with a known maternal BRCA1 or BRCA2 mutation), the SIR was 3.2. Twenty-five of the 28 phenocopies already had breast cancer at the time of genetic testing. This approach introduces significant ascertainment bias, as families are more likely to come in for genetic testing and counseling when multiple family members are affected with cancer. In order to account for this, further analysis was done by Smith et al. examining women unaffected at the time of their negative test result. Three breast cancers were observed in 153 women in 818 person-years of follow up, whereas 1.4 were expected (SIR 2.1, CI 0.4–6.2). These data have been provocative, but given the small sample size, not definitive.
A second study by Gronwald et al. [11, 13] found one breast cancer in 74 non-carrier sisters of BRCA1 and BRCA2 mutation carriers. Of the 17 affected sisters of known mutation carriers, only one was a phenocopy (i.e., she tested negative for the known family mutation). After assuming similar rates in untested affected and unaffected sisters of mutation carriers, the authors estimated an SIR of 2.1 (95% CI 0.4–6.2) for true negatives in this study.
Rowan et al. [12] prospectively examined 101 women who had tested negative for known familial BRCA1 and BRCA2 mutation. Of these, three developed invasive breast cancer in follow up, with a SIR of 2.9 (95% CI 1.0–8.6). One of these three women was considered to be at modestly increased risk for breast cancer, despite her negative testing result, as her mother (also negative for the known family mutation) had bilateral breast cancer at ages 48 and 59. The other two were determined to be at average risk.
The elevated risk of breast cancer seen in true negatives seen in studies done to date is therefore based on fewer than 10 prospectively identified cases. A modeling study by Golgar et al. suggested that while ascertainment bias exists in such studies, an increased risk of breast cancer with a RR of 2, was possible. [14] While we cannot exclude an elevated risk of this magnitude, our results indicate that a greater risk is extremely unlikely.
Why might women who test negative for familial mutation in BRCA1 or BRCA2 be at increased risk? There are increasing data that suggest risk modifiers exist that affect the penetrance of BRCA1 and BRCA2 mutations. The penetrance estimates for BRCA1 and BRCA2 vary substantially across studies. For example, initial studies using highly affected families necessary to perform linkage analysis estimated that breast cancer risk in BRCA1 mutation carriers was as high as 85%. In contrast, population-based studies have demonstrated lifetime risk estimates of breast cancer in BRCA1 carriers as low as 36% [15]. Although some factors that impact penetrance are well established (such as mastectomy and oophorectomy) many are less well understood. Genotype–phenotype correlations may exist. For example, the ovarian cancer cluster region in BRCA2 is associated with a relatively higher risk of ovarian cancer than mutations elsewhere in the gene [16]. Allele-specific variation in penetrance likely explains only a small portion of the variability seen. Modifier genes (genes inherited along with BRCA1 and BRCA2 and affect their penetrance) are of substantial interest. Genome wide association and other studies have now identified several single nucleotide polymorphisms which modestly elevate risk in the general population; several of these also appear to modify breast cancer risk in BRCA2 mutation carriers [13, 17, 18]. Given the small effects of these individual SNPs, these data are not yet clinically useful. However, due to independent assortment, it is possible that such modifier genes could be inherited by a family member who did not inherit the BRCA1 or BRCA2 mutation. While these individuals would not have the dramatically elevated risk known to be associated with a BRCA1 or BRCA2 mutation, they might still have a modestly associated risk resulting from the independent effect of the modifiers.
The present study describes the largest cohort assembled to address the issue of breast and ovarian cancer risk in true negatives, and was conducted entirely prospectively. We excluded individuals who were affected at the time of testing, avoiding the possible ascertainment bias inherent in studies that included such individuals. Unlike other studies, we found no suggestion of an increased risk among true negatives. Although this is the largest prospective study done to date, the number of events remains small and the follow up relatively short. Based on the CI, the relative risk of breast cancer in the true negatives could be as high as two. This is the same risk as having one-first degree relative with postmenopausal breast cancer, a situation that does not currently lead to a recommendation for increased surveillance.
A limitation to our study is that we included follow-up information provided by first and second-degree relatives. Although there are data reporting of breast cancer cases accurate in first and second-degree relatives [19], it is possible that cases of breast cancer were not reported. Although this is a formal possibility, it seems unlikely given that communication in these families was adequate to disseminate genetic test results so that the unaffected women could be tested. In such families, communication of cancer diagnoses is also likely to be effective.
Importantly, not all true negatives for a known mutation in a family will be at population risk for breast cancer. Each individual coming in for genetic testing should have a careful analysis of additional family history (with a careful analysis of the lineage without a known mutation, as well as any breast cancers not explained by the familial mutation), histological risk factors (such as lobular carcinoma in situ or atypical ductal hyperplasia), and reproductive risk factors (age at first live birth, age at menarche, use of postmenopausal hormone replacement therapy). For example, women who have not inherited their mother’s BRCA1 mutation are still at increased risk of breast cancer if two of their paternal aunts had premenopausal breast cancer and were either untested or were tested and negative for detectable BRCA1/2 mutations. Other risk factors for breast cancer in true negatives must be recognized and incorporated into the individual’s risk assessment. Models such as the Breast Cancer Risk Assessment Tool (modified Gail model), Claus and Tyrer-Cuzik can be useful to assess risk in these situations [20].
Individuals from families with multiple cases of breast cancer are more likely to come for genetic testing than individuals with fewer cases. As recognized by genetic professionals and well described by Smith et al. [10], phenocopies do exist, particularly when there are a large number of affected individuals in a family, as there is a reasonable risk of breast cancer in the general population. For this reason, it is preferable to begin testing in a family in the individual with the highest prior probability of a BRCA1 or BRCA2 mutation. For example, women with ovarian cancer or very early onset breast cancer, will have a much higher chance of having a BRCA1/2 mutation than their relative with DCIS at 65 (which is much more likely to be sporadic).
The clinical question that faces us is the following, do we have sufficient data to recommend anything other than routine screening in women who are true negatives? At this time the available data, including this entirely prospective study, do not support additional measures, although continued prospective follow up is necessary.
References
Rebbeck TR, Lynch HT, Neuhausen SL, Narod SA, Van’t Veer L, Garber JE, Evans G, Isaacs C, Daly MB, Matloff E et al (2002) Prophylactic oophorectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med 346(21):1616–1622
Kauff ND, Satagopan JM, Robson ME, Scheuer L, Hensley M, Hudis CA, Ellis NA, Boyd J, Borgen PI, Barakat RR et al (2002) Risk-reducing salpingo-oophorectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med 346(21):1609–1615
Domchek SM, Friebel TM, Neuhausen SL, Wagner T, Evans G, Isaacs C, Garber JE, Daly MB, Eeles R, Matloff E et al (2006) Mortality after bilateral salpingo-oophorectomy in BRCA1 and BRCA2 mutation carriers: a prospective cohort study. Lancet Oncol 7(3):223–229
Rebbeck TR, Friebel T, Lynch HT, Neuhausen SL, van ‘t Veer L, Garber JE, Evans GR, Narod SA, Isaacs C, Matloff E et al (2004) Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: the PROSE Study Group. J Clin Oncol 22(6):1055–1062 Epub 2004 Feb 1023
Meijers-Heijboer H, van Geel B, van Putten WL, Henzen-Logmans SC, Seynaeve C, Menke-Pluymers MB, Bartels CC, Verhoog LC, van den Ouweland AM, Niermeijer MF et al (2001) Breast cancer after prophylactic bilateral mastectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med 345(3):159–164
Warner E, Plewes DB, Hill KA, Causer PA, Zubovits JT, Jong RA, Cutrara MR, DeBoer G, Yaffe MJ, Messner SJ et al (2004) Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 292(11):1317–1325
Leach MO, Boggis CR, Dixon AK, Easton DF, Eeles RA, Evans DG, Gilbert FJ, Griebsch I, Hoff RJ, Kessar P et al (2005) Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 365(9473):1769–1778
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A et al (2003) Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet 72(5):1117–1130
King MC, Marks JH, Mandell JB (2003) Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 302(5645):643–646
Smith A, Moran A, Boyd MC, Bulman M, Shenton A, Smith L, Iddenden R, Woodward ER, Lalloo F, Maher ER et al (2007) Phenocopies in BRCA1 and BRCA2 families: evidence for modifier genes and implications for screening. J Med Genet 44(1):10–15
Gronwald J, Cybulski C, Lubinski J, Narod SA (2007) Phenocopies in breast cancer 1 (BRCA1) families: implications for genetic counselling. J Med Genet 44(4):e76
Rowan E, Poll A, Narod SA (2007) A prospective study of breast cancer risk in relatives of BRCA1/BRCA2 mutation carriers. J Med Genet 44(8):e89 (author reply e88)
Antoniou AC, Sinilnikova OM, Simard J, Leone M, Dumont M, Neuhausen SL, Struewing JP, Stoppa-Lyonnet D, Barjhoux L, Hughes DJ et al (2007) RAD51 135G–>C modifies breast cancer risk among BRCA2 mutation carriers: results from a combined analysis of 19 studies. Am J Hum Genet 81(6):1186–1200
Goldgar D, Venne V, Conner T, Buys S (2007) BRCA phenocopies or ascertainment bias? J Med Genet 44(8):e86 (author reply e88)
Begg CB, Haile RW, Borg A, Malone KE, Concannon P, Thomas DC, Langholz B, Bernstein L, Olsen JH, Lynch CF et al (2008) Variation of breast cancer risk among BRCA1/2 carriers. JAMA 299(2):194–201
Gayther SA, Mangion J, Russell P, Seal S, Barfoot R, Ponder BA, Stratton MR, Easton D (1997) Variation of risks of breast and ovarian cancer associated with different germline mutations of the BRCA2 gene. Nat Genet 15(1):103–105
Antoniou AC, Spurdle AB, Sinilnikova OM, Healey S, Pooley KA, Schmutzler RK, Versmold B, Engel C, Meindl A, Arnold N et al (2008) Common breast cancer-predisposition alleles are associated with breast cancer risk in BRCA1 and BRCA2 mutation carriers. Am J Hum Genet 82(4):937–948
Antoniou AC, Sinilnikova OM, McGuffog L, Healey S, Nevanlinna H, Heikkinen T, Simard J, Spurdle AB, Beesley J, Chen X et al (2009) Common variants in LSP1, 2q35 and 8q24 and breast cancer risk for BRCA1 and BRCA2 mutation carriers. Hum Mol Genet 18(22):4442–4456
Schneider KA, DiGianni LM, Patenaude AF, Klar N, Stopfer JE, Calzone KA, Li FP, Weber BL, Garber JE (2004) Accuracy of cancer family histories: comparison of two breast cancer syndromes. Genet Test 8(3):222–228
Evans DG, Howell A (2007) Breast cancer risk-assessment models. Breast Cancer Res 9(5):213
Acknowledgment
MR wishes to acknowledge the invaluable assistance of Sara Spencer, MGC. This research was supported by the Cancer Genetics Network (HHSN21620074400C to SMD), the Marjorie Cohen Foundation (to SMD), Breast Cancer Research Foundation (to KN, MR and KO), Robert and Kate Niehaus Cancer Research Fund (to MR and KO), and Sharon Elghanayan Research Initiative (to MR and KO).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Domchek, S.M., Gaudet, M.M., Stopfer, J.E. et al. Breast cancer risks in individuals testing negative for a known family mutation in BRCA1 or BRCA2 . Breast Cancer Res Treat 119, 409–414 (2010). https://doi.org/10.1007/s10549-009-0611-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-009-0611-y