
Abstract
Taxanes (paclitaxel and docetaxel) comprise a class of mitotic inhibitors which considered highly active chemotherapeutic agents against cancer cells, and have become a cornerstone in the treatment of patients with early and advanced breast cancer. Following the initial generation of trials conducted to prove their efficacy, investigators turned to explore which taxane is superior in terms of efficacy, side effects, and quality of life based on head-to-head comparisons of paclitaxel versus docetaxel containing regimens. Moreover, many trials conducted to evaluate the optimal taxane dosing and schedule. This commentary discusses the ERASME 3 trial which compared the quality of life after four courses of doxorubicin combination with either paclitaxel or docetaxel, and also, it reviews all trials compared paclitaxel to docetaxel in both early and metastatic disease settings, in terms of efficacy, dosing, schedule, and toxicity profile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Taxanes are among the most successful chemotherapy agents used in the management of breast cancer. The taxanes exert their antitumor activity by binding tubulin and stabilizing nonfunctional microtubule bundles, thereby blocking normal mitotic spindle development and causing cell cycle arrest in G2 phase [1]. Although synthesis of paclitaxel and its analogue, docetaxel, first began in the late 1970s and early 1980s, clinical development of the taxanes for breast cancer treatment was flourished in the 1990s, when the antitumor activity of single-agent regimens in patients with advanced disease began to be documented in phase II trials [2–6]. Initially, the use of taxanes was limited by hypersensitivity reactions, but once these were better managed (largely by premedication with steroids), taxane use became more common. After it have showed efficacy in metastatic breast cancer, the taxanes are now vital component in the treatment of early-stage disease, in which their addition to adjuvant treatment of early breast cancer has been shown to improve overall survival. Combinations of taxanes with other chemotherapeutic agents and targeted therapies have further improved survival for both early and metastatic disease. New formulations of taxanes (ABI-007) may both improve antitumor activity and reduce toxicity [7, 8].
This commentary reviews the current status of taxane therapy of breast cancer; it discusses efficacy and tolerability of taxane monotherapy or combination therapy, in comparison with other standard regimens in both early and metastatic disease settings, in terms of overall response rate (ORR), time to progression (TTP), and overall survival (OS). Also, it addresses important clinical questions of optimal taxane dose and schedule, and the preferred taxane (based on head-to-head comparison).
The ERASME trial
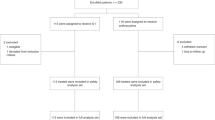
The ERASME 3 trial [9] presented in this issue of Breast Cancer Research and Treatment is a randomized controlled trial comparing the combination of doxorubicin and paclitaxel (AP) with the combination of doxorubicin and docetaxel (AD) in the setting of front-line chemotherapy for metastatic breast cancer. The primary endpoint of the trial, somewhat unusually, is overall quality of life (QoL), or more specifically, quality of life measured at the single time point of four cycles of chemotherapy.
Why chose such a time-point, and why chose 4 cycles of therapy? QoL was chosen because, in the author’s words “We hypothesized that AD and AP combinations would yield similar results in terms of ORR and PFS, but were likely to have different toxicity profiles and hence could derive different benefits in terms of QoL”. But is this the case? A randomized controlled trial of docetaxel versus paclitaxel showed a significant overall survival advantage favoring docetaxel in front-line metastatic breast cancer (15.4 vs. 12.7 months, P = 0.03) [10], and, in an admittedly underpowered survival analysis performed in the Erasme trial, AP came close to beating AD (27.3 vs. 21.4 months, P = 0.081). Would a larger trial have shown a survival advantage? It is of course impossible to say.
Regarding QoL, 4 cycles represents a convenient time-point for measurement. Most of those fated to respond (and therefore benefit symptomatically) will have done so by this point, and few of those destined to progress on chemotherapy will have done so. Compliance (always a concern in QoL studies) remained good, and patients had not yet crossed over to single agent therapy.
So how did the regimens compare? In general terms, they were equivalent. This is not to say that the regimens had identical effects; real differences in toxicity exist. But QoL measurements are blunt instruments, and unable to provide evidence for subtle distinctions between the two chemotherapy regimens examined.
Why might this be the case? QoL is an amalgam of many things. These include therapeutic effects (shrinkage and drug toxicity), tumor-driven effects, host differences (both physical and psychological) and ultimately unmeasurable aspects of the human spirit. A chemotherapy regimen is only likely to improve QoL in a symptomatic patients who responds to chemotherapy (i.e., you can’t make someone who is asymptomatic feel better by administering cytotoxic chemotherapy), and only then if not outweighed by toxic effects.
Taxanes in metastatic breast cancer (MBC)
The ERASME 3 trial represents part of a long duel in the breast cancer world. Taxanes have demonstrated efficacy in multiple large and high quality phase III trials in the metastatic setting, but is there a “best” taxane? And what do we even mean by “best”?
Paclitaxel
Paclitaxel monotherapy has significant activity in both Anthracycline-naive (ORR 35–55%) [11–13] and Anthracycline-refractory MBC (ORR consistently at least 20%) [2, 4, 11–16]. Response rates obtained in randomized controlled trials has—as is not unusual in the breast cancer field—resulted in lower response rates than in the initial Phase II trials.
Dose and schedule
The original “standard” dose of paclitaxel was 175 mg/m2 over 3 h every 3 weeks; a lower dose (135 mg/m2) [17] has inferior efficacy, and higher doses (210 and 250 mg/m2) did not improve response rate, survival, or quality of life in CALBG 9342 [18]. Although higher dose therapy was associated with a slight improvement of TTP, it was offset by higher toxicity [18, 19]. Continuous 24-h infusion of paclitaxel, results in a higher tumor ORR than when administered as a 3-h infusion, but does not significantly improve TTP or OS. It has increased hematologic toxicity and decreased neurosensory toxicity [11].
Weekly doses of paclitaxel (80–100 mg/m2) can be administered continuously for several weeks with minimal myelosuppression. ORR are at least as high as would be expected from every 3-week therapy (53% and 22% in two separate studies) [20, 21], even in patients with anthracycline-refractory MBC. Weekly paclitaxel (80 mg/m2) was directly compared to every 3-week therapy (175 mg/m2) in the CALGB 9840 trial [22]. In this trial, weekly therapy was associated with a significantly higher ORR (40% vs. 28%) and longer TTP (9 vs. 5 months), but similar OS and worse neurotoxicity. Thus, the decision paclitaxel weekly versus every 3 weeks should be based upon a balance of toxicity and patient convenience.
ABI-007 (nab-paclitaxel)
ABI-007 (nab-paclitaxel) is Cremophor-free nanoparticle albumin-bound formulation of paclitaxel. Nab-paclitaxel does not require steroid premedication, and can be administered over 30 min without special tubing. Both weekly (100–150 mg/m2) and every 3 weekly Abraxane are active and well tolerated in taxane-refractory MBC [7, 8]. In one multicenter phase II trial, the objective response rates for patients undergoing first-line and beyond first-line therapy with nab-paclitaxel were 64% and 21%, respectively; and there were no hypersensitivity reactions [8].
Nab-paclitaxel has been compared to paclitaxel in a phase III trial [7] in which 460 patients with MBC were randomly assigned to nab-paclitaxel (260 mg/m2 over 30 min without premedication) or standard paclitaxel (175 mg/m2 over 3 h), both on day 1 every 21 days. Nab-paclitaxel was associated with a significantly higher response rate (33% vs. 19%), and longer TTP (23 vs. 17 weeks). Nab-paclitaxel was associated with no severe hypersensitivity reactions, and less grade 4 neutropenia (9% vs. 22%), but a higher rate of grade 3 sensory neuropathy (10% vs. 2%), which was reversible and short-lived. Nab-paclitaxel is approved in the United States for the treatment of MBC. Despite of all above mentioned advantages over unbound paclitaxel, nab-paclitaxel is significantly more expensive.
Docetaxel
Docetaxel is a semisynthetic analogue of paclitaxel, and like paclitaxel, it is highly effective even in heavily pretreated patients, with ORR up to 60% [5, 6, 23].
Dose and schedule
The standard dose is 100 mg/m2 over 1 h every 3 weeks. The optimal dose of docetaxel monotherapy was the subject of a randomized trial, in which 527 patients progressing after one prior regimen for metastatic disease, or within 6 months of adjuvant chemotherapy were randomly assigned to 60, 75, or 100 mg/m2 docetaxel, administered every 21 days [24]. A significant dose-response relationship was observed for tumor ORR (20%, 22%, and 30%, respectively) but not for TTP (13, 15, and 17 weeks, respectively) or OS (10.6, 10.3, and 12.3 months, respectively). The incidence of its toxicities (including grade 3 or 4 neutropenia and febrile neutropenia) was also dose-related.
Docetaxel, like paclitaxel, has been administered in a weekly schedule, at doses of 30–40 mg/m2 over 1 h, with response rates of 40–50% [25], and as with paclitaxel, is less myelosuppressive [26, 27]. However, weekly therapy is associated with increases in hyperlacrimation, skin- and nail-toxicity, and negatively affects quality of life [28]. Asthenia is particularly common with weekly docetaxel.
Is there a “best” taxane in the setting of MBC?
It is unclear which taxane is superior when taxane monotherapy is considered. In the only Phase III trial that directly compared docetaxel and paclitaxel head-to-head, 449 women who had received prior anthracyclines were randomly assigned to docetaxel (100 mg/m2) or paclitaxel (175 mg/m2 over 3 h) every 3 weeks [10]. The docetaxel group had a nonsignificantly higher response rate (32% vs. 25%, P = 0.1), modestly but significantly higher median TTP (5.7 vs. 3.6 months, P = 0.0001) and improved OS (15.4 vs. 12.7 months, P = 0.03). However, both hematologic and nonhematologic toxicity was worse with docetaxel.
Docetaxel has been compared to nab-paclitaxel in a 4-arm randomized Phase II trial recently presented in abstract form by Gradishar et al. [29]. While Phase II trials are not perfect venues to compare agents, docetaxel was outperformed with regard to ORR by nab-paclitaxel in this setting. A Phase III trial should now offer a definitive answer.
Given the results of CALGB 9840, we now know that weekly paclitaxel is superior to every 3 week paclitaxel, casting into doubt the superiority of docetaxel. Similarly, the head-to-head comparison of nab-paclitaxel with standard paclitaxel was a comparison employing every 3 week paclitaxel. At present, it seems reasonable to consider all three agents useful for metastatic breast cancer, but difficult to declare a “best” agent on objective grounds.
Adjuvant and neoadjuvant taxane therapy for early breast cancer
Adjuvant trial designs in the early 1990s were absent of taxanes. By the mid 1990s, the taxanes were included in adjuvant trials; initially in node-positive patients, and subsequently in both node-negative and node-positive patients. The results consistently demonstrated a benefit for taxane-based regimens as a component of adjuvant chemotherapy regimens for early breast cancer. A recent meta-analysis [30] of nine Phase III trials designed to assess if paclitaxel or docetaxel improve survival (included a total of 15,598 patients) found the absolute benefits in DFS and OS in favor of taxane based regimens ranged from 3.3% to 4.6% and from 2.0% to 2.8%, respectively.
Following the initial generation of adjuvant trials (Table 1), and parallel trials conducted in the metastatic setting, investigators then turned to the question of taxane superiority in the adjuvant setting. Is there a “best” taxane, and a “best” dose and schedule?
The ECOG E1199 trial [31] was conducted to answer this question. A total of 4,950 women with T1-3 N1-2 or T2-3 N0 breast cancer all received AC × 4 followed by randomization to one of four groups for sequential taxane therapy: every 3 weeks paclitaxel (175 mg/m2), weekly paclitaxel (80 mg/m2), every 3 weeks docetaxel (100 mg/m2), or weekly docetaxel (35 mg/m2). As presented at the 2007 ASCO meeting, while the initial 2 × 2 comparison for drug type and dosage revealed no statistically significant differences, comparison of all four arms revealed weekly paclitaxel and q3w docetaxel to be superior to q3w paclitaxel with regard to DFS, the primary study endpoint. The incidence of all grade 3–4 toxicity was higher in docetaxel arms, and docetaxel every 3 weeks was the most toxic.
Conclusions
Is the long duel over? The results of E1199, the only large adjuvant trial asking the direct comparison question, suggests that weekly paclitaxel and every 3 week docetaxel represent reasonable adjuvant taxane approaches. This verdict may be a temporary one. We currently lack adjuvant data with nab-paclitaxel, compared either with standard paclitaxel or docetaxel. The evolving therapeutic landscape is also changing, with the addition in recent years of adjuvant HER2-targeted therapy and the advent of genomic technologies and novel adjuvant therapies (e.g., bevacizumab) that may further alter our perception of both risk and benefit. Some stories never end in oncology, but all are altered in the telling.
References
Ringel I, Horwitz SB (1991) Studies with RP 56976 (taxotere): a semisynthetic analogue of taxol. J Natl Cancer Inst 83(4):288–291
Holmes FA, Walters RS, Theriault RL et al (1991) Phase II trial of taxol, an active drug in the treatment of metastatic breast cancer. J Natl Cancer Inst 83(24):1797–1805
Valero V, Holmes FA, Walters RS et al (1995) Phase II trial of docetaxel: a new, highly effective antineoplastic agent in the management of patients with anthracycline-resistant metastatic breast cancer. J Clin Oncol 13(12):2886–2894
Fountzilas G, Athanassiadis A, Kalogera-Fountzila A et al (1997) Paclitaxel by 3-h infusion and carboplatin in anthracycline-resistant advanced breast cancer. A phase II study conducted by the Hellenic Cooperative Oncology Group. Eur J Cancer 33(11):1893–1895
Dieras V, Chevallier B, Kerbrat P et al (1996) A multicentre phase II study of docetaxel 75 mg m-2 as first-line chemotherapy for patients with advanced breast cancer: report of the Clinical Screening Group of the EORTC. European Organization for Research and Treatment of Cancer. Br J Cancer 74(4):650–656
Ravdin PM, Burris HA 3rd, Cook G et al (1995) Phase II trial of docetaxel in advanced anthracycline-resistant or anthracenedione-resistant breast cancer. J Clin Oncol 13(12):2879–2885
Gradishar WJ, Tjulandin S, Davidson N et al (2005) Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J Clin Oncol 23(31):7794–7803
Ibrahim NK, Samuels B, Page R et al (2005) Multicenter phase II trial of ABI-007, an albumin-bound paclitaxel, in women with metastatic breast cancer. J Clin Oncol 23(25):6019–6026
Cassier PA, Chabaud S, Trillet-Lenoir V et al (2007) A phase-III trial of doxorubicin and docetaxel versus doxorubicin and paclitaxel in metastatic breast cancer: results of the ERASME 3 study. Breast Cancer Res Treat
Jones SE, Erban J, Overmoyer B et al (2005) Randomized phase III study of docetaxel compared with paclitaxel in metastatic breast cancer. J Clin Oncol 23(24):5542–5551
Smith RE, Brown AM, Mamounas EP et al (1999) Randomized trial of 3-hour versus 24-hour infusion of high-dose paclitaxel in patients with metastatic or locally advanced breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-26. J Clin Oncol 17(11):3403–3411
Paridaens R, Biganzoli L, Bruning P et al (2000) Paclitaxel versus doxorubicin as first-line single-agent chemotherapy for metastatic breast cancer: a European Organization for Research and Treatment of Cancer Randomized Study with cross-over. J Clin Oncol 18(4):724–733
Sledge GW, Neuberg D, Bernardo P et al (2003) Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J Clin Oncol 21(4):588–592
Geyer CE Jr, Green SJ, Moinpour CM et al (1998) Expanded phase II trial of paclitaxel in metastatic breast cancer: a Southwest Oncology Group study. Breast Cancer Res Treat 51(2):169–181
Vermorken JB, ten Bokkel Huinink WW, Mandjes IA et al (1995) High-dose paclitaxel with granulocyte colony-stimulating factor in patients with advanced breast cancer refractory to anthracycline therapy: a European Cancer Center trial. Semin Oncol 22(4 Suppl 8):16–22
Bishop JF, Dewar J, Toner GC et al (1999) Initial paclitaxel improves outcome compared with CMFP combination chemotherapy as front-line therapy in untreated metastatic breast cancer. J Clin Oncol 17(8):2355–2364
Nabholtz JM, Gelmon K, Bontenbal M et al (1996) Multicenter, randomized comparative study of two doses of paclitaxel in patients with metastatic breast cancer. J Clin Oncol 14(6):1858–1867
Winer EP, Berry DA, Woolf S et al (2004) Failure of higher-dose paclitaxel to improve outcome in patients with metastatic breast cancer: cancer and leukemia group B trial 9342. J Clin Oncol 22(11):2061–2068
Sparano JA (2000) Taxanes for breast cancer: an evidence-based review of randomized phase II and phase III trials. Clin Breast Cancer 1(1):32–40; discussion 1–2
Seidman AD, Hudis CA, Albanell J et al (1998) Dose-dense therapy with weekly 1-hour paclitaxel infusions in the treatment of metastatic breast cancer. J Clin Oncol 16(10):3353–3361
Perez EA, Vogel CL, Irwin DH, Kirshner JJ, Patel R (2001) Multicenter phase II trial of weekly paclitaxel in women with metastatic breast cancer. J Clin Oncol 19(22):4216–4223
Seidman A, Berry D, Cirrincione C et al (2004) CALGB 9840: phase III study of weekly paclitaxel via 1-hour infusion versus standard 3h infusion every third week in the treatment of metastatic breast cancer (MBC), with trastuzumab (T) for HER2 positive MBC and randomized for T in HER2 normal MBC (abstract)
O’Brien ME, Leonard RC, Barrett-Lee PJ, Eggleton SP, Bizzari JP (1999) Docetaxel in the community setting: an analysis of 377 breast cancer patients treated with docetaxel (Taxotere) in the UK. UK Study Group. Ann Oncol 10(2):205–210
Harvey V, Mouridsen H, Semiglazov V et al (2006) Phase III trial comparing three doses of docetaxel for second-line treatment of advanced breast cancer. J Clin Oncol 24(31):4963–4970
Burstein HJ, Manola J, Younger J et al (2000) Docetaxel administered on a weekly basis for metastatic breast cancer. J Clin Oncol 18(6):1212–1219
Loffler TM (1998) Is there a place for “dose-dense” weekly schedules of the taxoids? Semin Oncol 25(5 Suppl 12):32–34
Tomiak E, Piccart MJ, Kerger J et al (1994) Phase I study of docetaxel administered as a 1-hour intravenous infusion on a weekly basis. J Clin Oncol 12(7):1458–1467
Engels FK, Verweij J (2005) Docetaxel administration schedule: from fever to tears? A review of randomised studies. Eur J Cancer 41(8):1117–1126
Gradishar W, Krasnojon D, Cheporov S, Makhson A, Manikhas G, Clawson A, Hawkins MJ (2007) Randomized comparison of weekly or every-3-week (q3w) nab-paclitaxel compared to q3w docetaxel as first-line therapy in patients (pts) with metastatic breast cancer (MBC). J Clin Oncol, 2007 ASCO Annual Meeting Part I. Vol 25, No. 18S (June 20 Supplement), 2007:1032
Bria E, Nistico C, Cuppone F et al (2006) Benefit of taxanes as adjuvant chemotherapy for early breast cancer: pooled analysis of 15,500 patients. Cancer 106(11):2337–2344
Sparano J, Wang M, Martino S et al (2007) Phase III study of doxorubicin-cyclophosphamide followed by paclitaxel or docetaxel given every 3 weeks or weekly in patients with axillary node-positive or high-risk axillary node-negative breast cancer: results of the North American Breast Cancer Intergroup Trial E1199 Abstract). J Clin Oncol. 2007 ASCO Annual Meeting Part I. Vol 25, No. 18S (June 20 Supplement), 2007:516
Buzdar AU, Singletary SE, Valero V et al (2002) Evaluation of paclitaxel in adjuvant chemotherapy for patients with operable breast cancer: preliminary data of a prospective randomized trial. Clin Cancer Res 8(5):1073–1079
Henderson IC, Berry DA, Demetri GD et al (2003) Improved outcomes from adding sequential Paclitaxel but not from escalating Doxorubicin dose in an adjuvant chemotherapy regimen for patients with node-positive primary breast cancer. J Clin Oncol 21(6):976–983
Mamounas EP, Bryant J, Lembersky B et al (2005) Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: results from NSABP B-28. J Clin Oncol 23(16):3686–3696
Fountzilas G, Skarlos D, Dafni U et al (2005) Postoperative dose-dense sequential chemotherapy with epirubicin, followed by CMF with or without paclitaxel, in patients with high-risk operable breast cancer: a randomized phase III study conducted by the Hellenic Cooperative Oncology Group. Ann Oncol 16(11):1762–1771
Jones SE, Savin MA, Holmes FA et al (2006) Phase III trial comparing doxorubicin plus cyclophosphamide with docetaxel plus cyclophosphamide as adjuvant therapy for operable breast cancer. J Clin Oncol 24(34):5381–5387
Roche H, Fumoleau P, Spielmann M et al (2006) Sequential adjuvant epirubicin-based and docetaxel chemotherapy for node-positive breast cancer patients: the FNCLCC PACS 01 Trial. J Clin Oncol 24(36):5664–5671
Martin M, Pienkowski T, Mackey J et al (2005) Adjuvant docetaxel for node-positive breast cancer. N Engl J Med 352(22):2302–2313
Goldstein L, O’Neill A, Sparano J et al (2005) E2197: phase III AT (doxorubicin/docetaxel) vs. AC (doxorubicin/cyclophosphamide) in the adjuvant treatment of node positive and high-risk node negative breast cancer. Clin Oncol 23:7s (abstract)
Bear HD, Anderson S, Smith RE et al (2006) Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol 24(13):2019–2027
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Radaideh, S.M., Sledge, G.W. Taxane vs. taxane: is the duel at an end? A commentary on a phase-III trial of doxorubicin and docetaxel versus doxorubicin and paclitaxel in metastatic breast cancer: results of the ERASME 3 study. Breast Cancer Res Treat 111, 203–208 (2008). https://doi.org/10.1007/s10549-007-9776-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-007-9776-4