
Abstract
Background Several randomized controlled trials have confirmed the usefulness of trastuzumab as an adjuvant therapy for HER2-overexpressed breast cancer patients; however, the costs for 1-year treatment are high. Therefore, we performed an economic analysis regarding the efficient distribution of medical resources. Methods To analyze the cost-effectiveness for a 1-year adjuvant trastuzumab treatment group compared with the observation group, we constructed a Markov model adopting a 3% per year discount rate for costs and outcomes. The time horizon was 50 years. The perspective was that of health-care payers, as only direct medical costs were calculated. The outcome was measured as life-year gained (LYG) from 2-year follow-up HERA trial data. Results The ICER of the standard setting (5 years efficacy and 50–60 kg patient weight) was JPY 2,600,000 (€17,000) per LYG. The calculation results of other weight class ICER were JPY 2,200,000 (€15,000) and JPY 3,300,000 (€22,000) per LYG for the patients, respectively, who weighed less than 50 kg, and 60–75 kg. In the sensitivity analysis, the period of trastuzumab efficacy was the most influential parameter for the result of cost-effectiveness. However, even if the trastuzumab efficacy were to continue for only 2 years, at least, which is a conservative setting judging from the joint analysis (NSABP B-31 and NCCTG N9831 trials), the ICER remains acceptable for any weight class. Conclusion These results suggest that the 1-year adjuvant trastuzumab treatment is cost-effective. Both clinical and economic benefits were superior for the 1-year adjuvant trastuzumab treatment group compared with the observation group.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In Japan, the number of patient deaths due to breast cancer is increasing, while breast cancer mortality in Europe and the USA has generally improved since the 1990s [1]. The death toll from breast cancer is estimated as 10,000 persons per year, and reducing deaths due to breast cancer is one of the most important issues for women’s public health.
Trastuzumab (Herceptin®) is a humanized monoclonal antibody that selectively targets the human epidermal growth factor type-2 (HER2) receptor. Amplification of the HER2 gene and overexpression of the HER2 protein, considered to be poor-prognosis factors, are observed among 20–30% of breast cancer patients [2]. Trastuzumab administered as combination therapy with chemotherapy has been proved to significantly improve disease-free survival, overall survival, and health-related quality of life (QoL) for metastatic breast cancer patients [3–5]. After 2005, several randomized control trials (RCTs) have confirmed the usefulness of trastuzumab as adjuvant therapy for HER2-positive patients, not only as metastatic therapy. Ongoing large multicenter adjuvant trastuzumab RCTs: 1) the Herceptin Adjuvant (HERA) trial [6, 7], 2) the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-31 trial [8], 3) the North Central Center Treatment Group (NCCTG) N9831 trial [8], and 4) the Breast Cancer International Research Group (BCIRG) 006 trial [9], have shown good results, whereby the hazard ratio of the recurrence rate was about 0.5 even for HER2-positive patients who had a poor prognosis.
Though the cost of adjuvant trastuzumab treatment is high, the National Institute for Health and Clinical Excellence (NICE) in the UK has recommended adjuvant trastuzumab treatment for HER2-positive breast cancer patients based on the 1-year follow-up data of HERA trial [6, 10]; however, no such recommendation exists in Japan, and there have been no results of cost-effectiveness analysis based on the 2-year follow-up data of the HERA trial [7].
Therefore, this cost-effectiveness analysis (CEA) is designed to examine the economic efficiency of adjuvant trastuzumab treatment based on the 2-year follow-up data of HERA trial to support societal decision-making.
Patients and methods
Economic analysis
To analyze the cost-effectiveness of adjuvant trastuzumab treatment compared with observation alone, we used the Markov model by which the most common clinical transitions and health state transitions were simulated from multiple data sources. The model was build by TreeAge Pro 2006 (TreeAge Software, Inc, Williamstown, MA). One Markov cycle length corresponded to 1 month.
We adopted a 3% discount rate per year for costs and outcomes [11]. The discount-rate range for sensitivity analysis was 0–6%. The time horizon was 50 years (i.e., 600 Markov cycles), meaning that essentially all patients are considered as being dead.
The analysis perspective was that of health-care payers, and we calculated only the direct medical costs by the piece, because we were interested in the impact on the medical costs of adjuvant trastuzumab therapy. Neither indirect costs (work loss, etc.) nor direct non-medical costs (transportation cost, etc.) were considered. The primary result is indicated as the incremental cost per incremental life-year-gained (LYG). We used the exchange rate of €1 = JPY 150.
Hypothetic patients
Patients eligible for the HERA trial with HER2-positive breast cancer, who met the entry criteria, were considered as hypothetic patients of this economic analysis. Their median age was 49, and Japanese and node-negative patients were also included.
Based on the interim analysis of 2-year HERA follow up in 2007 [7], we only compared the economic efficiency for the 1-year of trastuzumab group (initial dose 8 mg/kg, maintenance dose 6 mg/kg, every 3 weeks for 1 year) and the observation group (adjuvant or neoadjuvant chemotherapy only). The hazard ratio for the risk of recurrence in the 1-year trastuzumab group, compared with the observation group, was 0.64 (95% confidence interval: 0.54–0.76; P < 0.0001), which was subject to probabilistic sensitivity analysis on the presumption of normal distribution on the log scale.
Major assumption
It is unknown how long the effect of trastuzumab continues, because HERA data cover only a 2-year median follow-up period. To take this uncertainty into account, the cost-effectiveness of trastuzumab was calculated for three hypothetic scenarios, with risk reduction continuing constantly for 2 years (conservative scenario), 5 years (standard scenario), and 10 years (optimistic scenario). After the end of the efficacy period of trastuzumab, the recurrence risk of the trastuzumab group is assumed to be equal to that of the observation group.
The next hypothesis is that trastuzumab is used for metastatic patients who have already been administered trastuzumab as adjuvant therapy. According to an inquiry survey of six Japanese leading hospitals participating in the HERA trial, most clinicians reported that they treated metastatic patients with trastuzumab after using it in an adjuvant setting and continued its combination therapy until a patient no longer responded to 3rd-line chemotherapy.
Patient weight may greatly influence the economic analysis result by determining the dose of trastuzumab. Japanese women, in their 50s, weigh an average of 54 kg. We assumed a patient weight of 50–60 kg (two 150 mg vials and one 60 mg vial) with a sensitivity analysis for patients weighing 50 kg (two 150 mg vials) and 60–75 kg (three 150 mg vials).
The assumed risk of recurrence during the first 5 years is higher than that during the next 5 years. The exact change of recurrence risk is not well defined, particularly not for HER2-positive patients. We presumed the recurrence risk after 5 years to be half that of the previous 5 years, continuing for the patients’ lifetime [1]. This parameter was also subject to sensitivity analysis.
Furthermore, trastuzumab-caused cardiac events, which may affect Qol, are thought to be reversible [12, 13]; and thus may not affect life-year.
Markov model and therapeutic strategy
Figure 1(a) shows our constructed Markov model, modeling the therapeutic strategy for metastatic patients recommended by Hortobagyi [14], as both hormone therapy and chemotherapy until 3rd-line, followed by palliative care. This Markov model mainly consists of four parts, “without recurrence,” “local recurrence,” “metastatic recurrence,” and “death,” which are split into some parts corresponding to chemotherapy or hormone therapy stage.

(a) Markov model. All patients start in the “without recurrence.” Patients move to an alternative health state with transition probability until they reach “death.” Arrows indicate the passages from one state to another. (b) Assumed process of breast cancer treatment. The white letters on a dark eclipse background mean concrete treatment. AI: aromatase inhibitor, TAM: tamoxifen, LH-RH: LHRH agonist, MPA: medroxyprogesterone acetate T: trastuzumab, TAX: paclitacel, VNB: vinorelbine, CAP: capecitabine
Transition rate and model parameters were based on the HERA trial [7], and other published clinical trials [3, 15–19], (Table 1(a)). Transition rate was calculated from percentages of events or median time to progression and is assumed to follow a beta distribution in probabilistic sensitivity analysis. The percentage of cardiotoxicity is 0.6% (severe), 2% (symptomatic), and 3% (asymptomatic) [7], Although in Fig. 1(a) the arrows of each state to death were not drawn, this transition rate, which is the probability of death due to causes other than breast cancer, is considered to be equal to the natural death rate in Japan.
We also postulated a standard therapeutic strategy corresponding to each Markov state Fig. 1(b), by referring to the Japanese clinical practice guideline for breast cancer and multiple experts’ opinions. In Japan, little cost-of-illness data exist; e.g., the treatment cost for metastatic patients is unknown, so we calculated the sum of each treatment cost in constructing this Markov model and estimated only direct medical costs based on the per piece Japanese drug tariff and reimbursement schedule, (Table 1 (b)). This included the cost of supportive care (anti-emetic agents [22], etc.), heart monitoring, routine follow-up [21], diagnostic imaging, blood tests, and so on. In the probabilistic sensitivity analysis, all cost data were modeled as normal distributions with the base-case value as the mean.
Results
Cost effectiveness result
The cost-effectiveness analysis compared the 1-year trastuzumab group with the observation group (Table 2). The ICER of the standard setting (5 years efficacy and 50–60 kg) was JPY 2,740,000 (€18,000) per LYG. The calculation results of other scenario ICER were JPY 1,920,000 (€13,000) and JPY 1,080,000 (€7,200) per LYG for the period of trastuzumab efficacy, respectively, of 10 years (a somewhat optimistic scenario), and throughout the life time (optimistic scenario).
The ICER becomes higher, however, with increased patient weight. At the 60–75 kg weight class, which is heavier than the standard class, the ICER changed from JPY 2,300,000 (€15,000) to JPY 7,400,000 (€49,000) for differing trastuzumab efficacy periods (5 to 50 years) and at 50–60 kg, which is a lighter class, ranged from JPY 1,500,000 (€10,000) to JPY 5,100,000 (€34,000).
Sensitivity analysis
The most influential parameter was the period of trastuzumab efficacy. The results are shown in Fig. 2 for every weight class; and when trastuzumab efficacy continues for more than 2 years, the ICER was less than JPY 7,500,000 (€50,000) for any weight class. Other one-way sensitivity analyses for parameters (discount rate, recurrence rate, cardiotoxicity costs, and terminal costs), showed little change. Among them, however, the discount rate was the most influential parameter, and all the results of sensitivity analyses in the standard scenario were less than JPY 5,000,000 (€33,000).

Uncertainty of cost-effectiveness analysis. The relation between ICER and efficacy period of trastuzumab by weight class
The ICER was changed to ¥4,700,000 (€31,000), ¥1,900,000 (€14,000), and ¥1,300,000 (€9,000) per LYG for the period of trastuzumab efficacy, respectively, of 2, 5, and the10 years, based on the 1-year follow-up data [6].
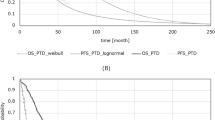
The acceptability curve of the standard setting is shown in Fig. 3(a), and the probability that the ICER of 1-year trastuzumab was less than JPY 5,400,000 (€36,000) was above 95%. Figure 3(b) shows the incremental cost-effectiveness plane and the 5 percentile and 95 percentile for incremental LYG were estimated to be 0.77 and 1.65. The 5 percentile and 95 percentile for incremental costs were JPY 900,000 (€15,000) and JPY 5,550,000 (€28,000).

(a) Acceptability curve for 1-year trastuzumab versus observation in a standard setting (5 years of efficacy and 50–60 kg) simulated 10,000 times (b) Incremental cost-effectiveness plane for trastuzumab versus observation alone
Discussion
In Japan, as with other developed countries, the serious social problem of burgeoning medical costs, caused by rapid aging and the evolution of healthcare technology prompts us to consider the efficiency of new expensive healthcare technology.
For metastatic patients, the trastuzumab ICER was estimated as £19,000 (monotherapy) and £37,500 (combination) by NICE, which recommended both trastuzumab monotherapy and combination therapy based on this economic evaluation [23]. Furthermore, NICE issued the guidance recommending trastuzumab as a treatment option based on the 1-year follow-up data of the HERA trial [10]. They estimated that the ICER of 1-year trastuzumab was £18,000 per additional QALY ranging from £16,000 to £33,000.
NICE suggests that the ICER threshold should be £20,000 to £30,000 (=JPY 5,000,000–JPY 7,000,000) per QALY. In the US, $50,000 or $100,000 per QALY is often used as the threshold. In Japan, no cost effectiveness threshold for treatment has been determined; however, it is thought that the values of the NICE’s thresholds are acceptable, because of the similar economic and medical environments in UK and Japan.
In US trials, weekly adjuvant trastuzumab therapy had an ICER of US$ 18,970 per QALY [24] and US$ 39,982 per QALY [25] estimating from the joint analysis (NSABP B-31 and NCCTG N9831 trials) [8]. Both papers also conclude that adjuvant trastuzumab is cost-effective. It confirms that the conclusion is consistent between the HERA trial and the joint analysis-based economic evaluation.
We calculated the ICER based on the 2-year follow-up data of the HERA trial in this analysis, although other cost-effectiveness analyses of trastuzumab were based on 1-year follow-up data. We had difficulty showing the exact ICER value and predicting the long-term prognosis for the trastuzumab patients’ group, which greatly influences the result of this economic evaluation. The results of other large trials, B31/N9831, show that the hazard ratio in the third or fourth year is nearly equal to that in the first year [8]. It is natural to assume that the efficacy of the HERA regimen continues for at least an equivalent period. Thus, we think the base case is 5 years. However, when trastuzumab efficacy continues at least for more than 2 years, which is a conservative setting, the ICER is less than JPY 7,500,000 (€50,000) for any weight class. There is little difference between LYG and QALY in oncology [26], so we could conclude that the 1-year trastuzumab treatment is cost-effective from this analysis, even based on 2-year follow-up data.
The limitation of this result is that our endpoint is LYG not QALY, because in Japan there are no HRQoL data for breast cancer patients applied to our analysis, and we decided it was better to use LYG than the QALY calculated by foreign, not Japanese utility values. In addition, the transition rates derived from published data and costs were calculated by the construction of a standard therapy model, not analyzed by using patient-level data.
In this analysis we adopted the health-care payers’ perspective. When the perspective was changed to a societal one, the indirect costs of the trastuzumab group were higher than those of the control group in the first yearly period of trastuzumab therapy. But considering that the expected value of incremental effectiveness is more than 1 year, the indirect costs of the trastuzumab group were lower, as a whole.
It is important to analyze not only the cost-effectiveness but also the budget impact. We considered the incremental cost of 1-year trastuzumab treatment as JPY 2,000,000–4,000,000 (€13,000–26,000) from Table 2. Then, by estimating the number of new breast cancer patients per year to be 40,000, of which 20% are HER2-positive, the total incremental cost was JPY 16–32 billion (€105–210 million), if all the HER2-positive patients were treated by trastuzumab.
In the Finland Herceptin (FinHer) trial [27], 9 weeks of trastuzumab injections yielded a hazard ratio equivalent to that of other studies in which trastuzumab was administered for 1 year. We cannot conclude that 9 weeks of injections is optimal from the FinHer trial, because it included fewer patients (N = 232). But this RCT showed a noteworthy result. If the efficacy of 9 weeks of injections is nearly equal to that of 1-year injections, 9-week treatment would be more cost-effective as well as provide greater patient convenience. However, the optimal period of adjuvant trastuzumab treatment has not yet been decided. At present, in the HERA trial, the comparison of 1-year and 2-year treatments has not been demonstrated. When they are available, the cost-effectiveness analyses will play an important role in determining the optimized treatment period.
The price of trastuzumab (¥78,074 (€520) per 150 mg vial) in Japan is lower than that in the UK (£407.40 (€650) per 150 mg vial), which is less than that in other developed countries. At the same time, the Japanese women’s average weight is less than that of westerners, and they have the highest life expectancy rates in the world. Though NICE estimated the average cost per person as £24,600 (JPY 5,900,000) in the UK [10], our calculated cost is JPY 3,390,000 (£14,000) in the standard setting. The Japanese women have an advantage over westerners in cost-effectiveness of adjuvant trastuzumab administration.
Based on the results of some RCTs and our economic analysis, we can conclude that the 1-year trastuzumab adjuvant treatment is superior to observation only in terms of the cost-effectiveness.
References
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) (2005) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 365:1687–1717
Slamon DJ, Clark GM, Wong SG et al (1987) Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 235:177–182
Slamon DJ, Leyland-Jones B, Shak S et al (2001) Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 344:783–792
Marty M, Cognetti F, Maraninchi D et al (2005) Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol 23:4265–4274
Osoba D, Slamon DJ, Burchmore M et al (2002) Effects on quality of life of combined trastuzumab and chemotherapy in women with metastatic breast cancer. J Clin Oncol 20:3106–3113
Piccart-Gebhart MJ, Procter M, Leyland-Jones B et al (2005) Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 353:1659–1672
Smith I, Procter M, Gelber RD et al (2007) 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: a randomised controlled trial. Lancet 369:29–36
Romond EH, Perez EA, Bryant J et al (2005) Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 353:1673–1684
Slamon D, Eiermann W, Robert N et al (2006) BCIRG 006: 2nd interim analysis phase III randomized trial comparing doxorubicin and cyclophosphamide followed by docetaxel (AC→T) with doxorubicin and cyclophosphamide followed by docetaxel and trastuzumab (AC→TH) with docetaxel, carboplatin and trastuzumab (TCH) in Her2 neu positive early breast cancer patients. Breast Cancer Res Treat 100(Sup.1):abstr 52
National Institute for Health and Clinical Excellence (2006) Trastuzumab for the adjuvant treatment of early-stage HER2-positive breast cancer.
Weinstein MC, Siegel JE, Gold MR et al (1996) Recommendations of the panel on cost-effectiveness in health and medicine. JAMA 276:1253–1258
Ewer MS, Vooletich MT, Durand JB et al (2005) Reversibility of trastuzumab-related cardiotoxicity: new insights based on clinical course and response to medical treatment. J Clin Oncol 23:7820–7826
Suter TM, Cook-Bruns N, Barton C (2004) Cardiotoxicity associated with trastuzumab (Herceptin) therapy in the treatment of metastatic breast cancer. Breast 13:173–183
Hortobagyi GN (1998) Treatment of breast cancer. N Engl J Med 339:974–984
Mouridsen H, Gershanovich M, Sun Y et al (2001) Superior efficacy of Letrozole versus Tamoxifen as first-line therapy for postmenopausal women with advanced breast cancer: results of a phase III study of the international Letrozole breast cancer group. J Clin Oncol 19:2596–2606
Klijn JG, Blamey RW, Boccardo F et al (2001) Combined tamoxifen and luteinizing hormone-releasing hormone (LHRH) agonist versus LHRH agonist alone in premenopausal advanced breast cancer: a meta-analysis of four randomized trials. J Clin Oncol 19:343–353
Toi M, Saeki T, Aogi K et al (2005) Late phase II clinical study of vinorelbine monotherapy in advanced or recurrent breast cancer previously treated with anthracyclines and taxanes. Jpn J Clin Oncol 35:310–315
Fumoleau P, Largillier R, Clippe C et al (2004) Multicentre, phase II study evaluating capecitabine monotherapy in patients with anthracycline- and taxane-pretreated metastatic breast cancer. Eur J Cancer 40:536–542
Le MG, Arriagada R, Spielmann M et al (2002) Prognostic factors for death after an isolated local recurrence in patients with early-stage breast cancer. Cancer 94:2813–2820
Briggs A (2001) Handling uncertainty in economic evaluation and presenting the results. In: Drummond M, McGuire A (eds) Economic evaluation in health care: merging theory with practice. Oxford university press, Oxford
Smith TJ, Davidson NE, Schapira DV et al (1999) American Society of Clinical Oncology 1998 update of recommended breast cancer surveillance guidelines. J Clin Oncol 17:1080–1082
Kris MG, Hesketh PJ, Somerfield MR et al (2006) American Society of Clinical Oncology guideline for antiemetics in oncology: update 2006. J Clin Oncol 24:2932–2947
National Institute for Health and Clinical Excellence (2002) Guidance on the use of trastuzumab for the treatment of advanced breast cancer
Liberato NL, Marchetti M, Barosi G (2007) Cost effectiveness of adjuvant trastuzumab in human epidermal growth factor receptor 2—positive breast cancer. J Clin Oncol 25:625–633
Kurian AW, Thompson RN, Gaw AF et al (2007) A cost-effectiveness analysis of adjuvant trastuzumab regimens in early HER2/neu—positive breast cancer. J Clin Oncol 25:634–641
Tammy TO (2004) Cost-effectiveness versus cost-utility analysis of interventions for cancer: does adjusting for health-related quality of life really matter? Value in Health 7:70–78
Joensuu H, Kellokumpu-Lehtinen PL, Bono P et al (2006) Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med 354:809–820
Acknowledgement
This study was performed as the Comprehensive Support Project for Health Outcomes Research project (CSP-HOR) established by the Public Health Research Foundation (PHRF). We thank the PHRF for the grant supporting our study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shiroiwa, T., Fukuda, T., Shimozuma, K. et al. The model-based cost-effectiveness analysis of 1-year adjuvant trastuzumab treatment: based on 2-year follow-up HERA trial data. Breast Cancer Res Treat 109, 559–566 (2008). https://doi.org/10.1007/s10549-007-9679-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-007-9679-4