
Abstract
While many reports describe health-related quality of life (QOL) among breast cancer survivors, few compare QOL before and after diagnosis and whether changes in QOL substantially differ from changes experienced by all women during aging. QOL was examined in a cohort of female residents of Beaver Dam, Wisconsin, aged 43–86 years at the time of a 1988–1990 baseline examination (N = 2,762; 83% of eligible). Participants were re-contacted four times through 2002 to ascertain QOL using the 36-item Short Form Health Survey (SF-36). QOL data for 114 incident breast cancer cases identified by data linkage with the statewide cancer registry were compared with data for 2,527 women without breast cancer. Women with breast cancer averaged 4.5 (95% CI: 1.6, 7.3) points lower than control women on the SF-36 Physical Component Summary (PCS) scale, regardless of time since diagnosis (up to 13 years). Women with breast cancer also reported lower scores on the SF-36 Mental Component Summary (MCS) scale within two years after diagnosis, but not at more distant times. In longitudinal analyses, 26 women who completed the SF-36 before and after breast cancer diagnosis experienced larger declines than age-matched controls in seven of the eight SF-36 health domains (all but role-emotional) and reported relative declines of −7.0 (95% CI: −11.5, −2.6) and −2.9 (95% CI: −6.3, 0.6) on the PCS and MCS scales, respectively. These results suggest that breast cancer survivors experience relative declines in health-related QOL across a broad spectrum of domains, even many years after diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over 2 million women in the United States are living with breast cancer [1]. With the success of early detection through mammography and improving therapies, more women faced with a breast cancer diagnosis are surviving longer [1, 2]. For these reasons, issues of quality of life (QOL)—not just length of survival—merit receiving greater attention from researchers, clinicians, and survivors.
QOL as an outcome has been incorporated within many clinical trials of cancer-directed therapy [3–5]. Clinical studies often evaluate QOL as a secondary outcome (with primary outcomes defined as clinical response, disease-free survival, or overall survival) in relation to different chemotherapy regimens or surgical approaches, the occurrence of lymphedema or menopausal symptoms, or the efficacy of complementary or alternative therapies. Treatment-based studies are often limited to the first year or two after diagnosis [6, 7], and these unique patient populations may not be representative of all survivors [8, 9].
Although many studies have reported on QOL in survivors according to treatment, few studies have examined baseline or personal characteristics before treatment initiation in relation to QOL after treatment [10]. In general female populations, overall QOL tends to decrease with higher age and increasing number of comorbid conditions [11]. Independent of specific diseases, QOL scores in breast cancer survivors also tend to decrease as Karnofsky performance status scores decrease or the total number of comorbid conditions increases [12, 13]. Further, the relation between age and changes in QOL after diagnosis is complex. Several studies have evaluated age in relation to QOL in breast cancer survivors and asymptomatic control women either using a single cross-sectional assessment [14] or using repeated assessments of QOL to examine changes in breast cancer survivors (but not controls) over the course of their treatment and recovery [15–18]. The studies that have examined differences in QOL and functional status at more than one time point in women with invasive breast cancer as well as comparison women without breast cancer have suggested that physical limitations and declines in functional status are greatest in younger women [19–22]. These results indicate that studies of QOL in breast cancer survivors are needed that include a comparison group of women without breast cancer and carefully account for age and co-existing health conditions to understand the unique effects that breast cancer has on QOL, separate from the effects of aging.
We examined health-related QOL outcomes among women with and without breast cancer who participated in the Beaver Dam Studies. This long-term and well-described cohort population provided a unique opportunity to evaluate QOL both before and after the breast cancer diagnosis.
Methods
The source population for this analysis consists of female participants of the Beaver Dam Studies which have been investigated extensively to evaluate eye disease [23, 24], hearing loss [25, 26], and other health outcomes [27, 28]. The recruitment methods and characteristics of this population have been previously described [24, 29, 30]. Briefly, residents aged 43–84-years old of Beaver Dam, Wisconsin, were identified by a private census from September 1987 to May 1988. Of the 5924 residents who were identified and invited to participate in the study, 4926 (83%) completed a baseline examination between March 1988 and September 1990. This included 2762 women. The study was approved by the University of Wisconsin Institutional Review Board and all participants provided written informed consent.
Data collection
Cohort participants were contacted for data collection as many as six times since 1988. After baseline, all eligible cohort participants were invited to two follow-up examinations (at five and ten years) as part of the Beaver Dam Eye Study [29, 30]. Concurrent examinations of the full cohort for the Epidemiology of Hearing Loss Study occurred with the Eye Study during 1993–1995 and 1998–2000. The Epidemiology of Hearing Loss Study also included an examination limited to older participants (75 years of age and older) during 1995–1998, and an additional interview of the cohort during 2000–2002 [25, 26]. Additionally, a random sample of 1653 participants in the baseline examination was selected for examination in the Health Outcomes Study during January 1991—September 1992 and again 18–24 months later during the five year follow up examination [27]. Participation exceeded 80% at each examination.
Health related QOL. The Medical Outcomes Study Short Form 36 Health Status Survey (SF-36) [11, 31] is a generic 36-item health status instrument, measuring eight domains of health: physical functioning (PF), role limitations because of physical problems (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations because of emotional problems (RE), and mental health (MH). Each scale is scored on a range from 0 (poorest health) to 100 (best health). The two norm-based Physical Component Summary (PCS) scale and Mental Component Summary (MCS) scales are calculated from these eight scales. Three scales contribute primarily to the PCS scale (physical functioning, bodily pain, role limitations because of physical problems), two scales contribute primarily to the MCS scale (social functioning, role limitations because of emotional problems) and the remaining three scales contribute substantially to both summary scales (vitality, general mental health, general health perceptions). The SF-36 questionnaire also contains the self-rated overall health question, “How would you rate your overall health now?”, with five answer options “excellent”, “very good”, “good”, “fair”, and “poor”.
The SF-36 was administered four times between 1991 and 2002 to the Beaver Dam Cohort. It was asked to a random sample of the cohort during 1991–1992 and to these same selected participants during the 1993–1995 five-year follow-up (686 of 839 were successfully re-interviewed). The SF-36 was administered to the Epidemiology of Hearing Loss cohort during 1998–2000 and 2000–2002.
Additionally, at the baseline visit as well as the five- and ten-year follow up examinations, participants were asked “How would you rate your overall health now?”, with four answer options “excellent”, “good”, “fair”, and “poor”.
Covariates. Extensive information regarding comorbidities, menopausal status, lifestyle factors (smoking, physical activity), anthropomorphic measurements (height, weight) and demographics (age, education, income, marital status) was collected at the 1988–1990 baseline and five- and ten-year follow-up visits. Comorbidities included hypertension, angina, myocardial infarction, stroke, arthritis, diabetes, and emphysema.
Breast cancer ascertainment
Women in the Beaver Dam Studies without a self-reported personal history of breast cancer at the baseline 1988–1990 examination were eligible for this study. Women with breast cancer diagnosed prior to the 1988–1990 baseline examination were excluded (N = 106). Incident diagnoses of breast cancer (N = 114) occurring between the baseline examination and the end of the study period (1988–2002) were ascertained through linkage with the Wisconsin Cancer Reporting System (Division of Public Health, Department of Health and Family Services, Wisconsin). During the follow-up period, 67 of these women completed a total of 121 SF-36 surveys after their breast cancer diagnosis. Multiple SF-36 surveys (N = 4,201) were completed at different time points by 1,788 women without breast cancer at the time of the survey. Of the 114 incident breast cancer cases, 26 completed the SF-36 before and after diagnosis (Fig. 1). Forty-one women provided SF-36 information after their breast cancer diagnosis but not before (including 12 women diagnosed prior to the first administering of the SF-36 during the 1991–1992 interview period). Twenty-two women provided SF-36 information prior to their breast cancer diagnosis but not afterwards (7 of these women died during the study). Twenty-five women diagnosed with breast cancer did not attend any of the 4 examinations where the SF-36 was administered (13 of these women died during the study).

Study schema, 1988–2002
Fifteen self-reported breast cancer diagnoses during follow-up were not confirmed by the Wisconsin Cancer Reporting System. These women were excluded from the study.
Analyses
All analyses were performed using SAS Statistical Software (Version 9; SAS Institute, Inc., Cary, North Carolina). All calculations of SF-36 scale scores were performed using the scale scoring exercise (second edition) in SAS provided by the Medical Outcomes Trust.
Two sets of analyses were performed: a cross-sectional analysis and a longitudinal evaluation of change in QOL. The first was a cross-sectional comparison of SF-36 scores between women with and without breast cancer. A woman diagnosed with breast cancer during the study could contribute SF-36 information to both groups (the pre-diagnosis survey(s) to the “control” group and post-diagnosis survey(s) to the “breast cancer” group). Least squared means for SF-36 scale scores and p values were calculated using multivariable analysis of variance including a covariate for age. An unstructured correlation matrix was used to account for repeated SF-36 measurements on individuals, with the empirical method for calculating standard errors [32].
In the second set of analyses (longitudinal), women who completed an SF-36 before and after a breast cancer diagnosis (N = 26) were selected. Women without a diagnosis of breast cancer for the entire study period were frequency matched (4:1) by age (within five year strata) and interview completion pattern to the 26 women diagnosed with breast cancer between completed SF-36 surveys. For each woman with breast cancer who completed the SF-36 before and after a diagnosis, the most recent SF-36 questionnaire prior to diagnosis and first completed SF-36 questionnaire following diagnosis were used for analysis. The same interview periods were selected for frequency-matched women without a diagnosis of breast cancer. For example, if a woman who completed the SF-36 in 1991, 1993, and 1998 was diagnosed with breast cancer in 1992, the SF-36 scores from 1991 and 1993 were included as the before and after scores in the analysis. Similarly, for the four women matched to this case, the SF-36 scores from the same periods (1991–1992 and 1993–1995) were selected. Two of the 26 women with breast cancer could not be successfully matched. For these two women, the age requirement for matching was loosened to 10-year strata. This yielded a cohort of 26 women with breast cancer and 104 women without breast cancer. For all participants, the reference age was defined as the age at completion of the earlier SF-36 questionnaire (in this example, age at the 1991–1992 interview).
Chi-squared and Fisher’s Exact tests were used to compare the self-rated health status at the reference interview and the change in self-rated health status at follow-up of women who would go on to develop breast cancer to women who remained free from breast cancer. Multivariable logistic regression models were used to calculate odds ratios (OR) of a decline in self-rated overall health and 95% confidence intervals (CI). A decline was defined to include any progression from a higher to lower level of self-rated health (e.g. excellent to very good, good to poor, etc.). Multivariable logistic models were adjusted for age, self-rated overall health at the reference interview, time between interviews, body mass index and the number of comorbidities.
Linear regression was used to compare the change in SF-36 scores among women with and without a breast cancer diagnosis. The outcome variable represented the difference between the particular SF-36 scale at follow-up and the reference score. Multivariable linear models were adjusted for age, the particular SF-36 scale score at the reference interview, time between interviews, body mass index and the number of comorbidities.
Results
Among the 2656 women in the study, 114 women were diagnosed with a primary breast cancer between baseline and the end of follow-up in 2002. These included 15 in situ, 58 localized, 31 regional, and 8 distant staged cases (2 were missing stage information). The mean age at baseline was 62.6 years (SD = 11.5, range = 43–86) for women without breast cancer and 63.4 years (SD = 10.3, range = 45–84) for women who developed breast cancer.
Cross-sectional QOL
Compared to women without breast cancer, women who developed breast cancer were more likely to be overweight and to report more comorbidities (Table 1). There was no significant difference between the responses to the four-option self-rated overall health question at baseline (P = 0.41).
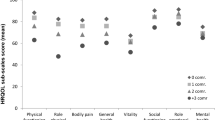
Compared to women without breast cancer, women with breast cancer reported lower scores on the physical function, physical role function, bodily pain, general health, vitality, and social function scales, as well as the PCS scale (Fig. 2). No differences were observed on the emotional role function, mental health, or MCS scales. After age adjustment, women with breast cancer at the time of the survey averaged 4.5 points lower on the PCS scale than women without breast cancer (40.4 vs. 44.9; 95% CI for difference: 1.6, 7.3; P = 0.002). There remained no significant difference in the MCS scale between women with and without breast cancer after age adjustment (54.2 vs. 54.8, respectively; P = 0.58). Further adjustment for other covariates did not substantially affect these results.

SF-36 scale scores by breast cancer status at time of interview, crude. *Indicates P < 0.05 for score comparison between women with and without breast cancer. Note that the MCS scale score for women without breast cancer is obscured by the MCS scale score for women with breast cancer
Stratifying women with breast cancer by time since diagnosis at the time of the interview revealed significant variation in the relation between breast cancer status and the SF-36 summary scales (Fig. 3). After age-adjustment, women with a breast cancer diagnosed less than two years prior to completing the SF-36 scored 3.6 points lower (95% CI: 0.3, 7.0) on the MCS scale than women without breast cancer (51.1 vs. 54.8, respectively; P = 0.03). However, women who had been diagnosed more than two years ago did not report lower scores on average on the MCS scale. In fact, women diagnosed with breast cancer eight or more years prior to completing the SF-36 scored 2.4 points higher (95% CI: 0.2, 4.6) on the MCS scale than women without breast cancer (57.2 vs. 54.8, respectively; P = 0.03). For the PCS scale, women with breast cancer reported lower scores compared to women without breast cancer regardless of time since diagnosis. The lowest PCS scores were observed among women diagnosed between 2.0 and 3.9 years prior to their completion of the SF-36 (38.5 vs. 44.9; P = 0.0002), which was the only category to reach statistical significance. Similar results were obtained when women who died during the course of the study were excluded from the analysis.

SF-36 Physical and Mental Component Summary scale scores by time since diagnosis, age adjusted. *Indicates P < 0.05 for comparison of summary scale score between women with and without breast cancer, grouped by time since diagnosis
Stage at diagnosis did not appear to modify the relation between the MCS scale and breast cancer status. However, women diagnosed with regional or distant staged breast cancer scored most poorly on the PCS scale (37.7 vs. 44.9 for women without breast cancer, age-adjusted; P = 0.002).
Longitudinal change in QOL
Twenty-six women completed an SF-36 questionnaire before and after their diagnosis. Age at diagnosis ranged from 48 to 93 years, with mean 70.1 years (SD = 11.9). Thirteen of the diagnoses were localized breast cancer, seven diagnoses were regional, four cases were in situ, and two diagnoses had unknown stage. On average, the women completed SF-36 surveys 1.9 years (SD = 1.6) before their diagnosis and 2.0 years (SD = 1.3) after diagnosis. The mean time between SF-36 surveys was 3.8 years (SD = 2.0, range = 2.0–8.1) for women diagnosed with breast cancer and 3.7 years (SD = 1.8, range = 0.9–8.4) for women without breast cancer.
At the reference interview (prior to diagnosis), women who went on to develop breast cancer were more likely to report worse self-rated overall health than age-matched women without breast cancer (P = 0.04). Over one-quarter (26.9%) of women who went on to develop breast cancer reported fair or poor health at the reference interview, compared to 6.8% of women who did not develop breast cancer. After diagnosis, women with breast cancer were 3.6 times as likely (95% CI: 1.5, 8.8) to report a decline in self-rated overall health status compared to women without breast cancer (P = 0.01). After adjusting for age and self-rated overall health at the initial visit covariates, women diagnosed with breast cancer were 13.4 times as likely as women who were not diagnosed with breast cancer to report a decline in self-rated overall health at the follow-up interview (95% CI: 3.6, 50.9; P = 0.0001). Further adjustment for other covariates did not significantly influence this estimate.
Overall, women diagnosed with breast cancer declined in each of the eight scales of the SF-36 health instrument, as well as the PCS and MCS scales (Fig. 4, Table 2). The largest declines were observed in general health (−15.2), physical functioning (−11.9), vitality (−11.7), and social functioning (−9.8). In all but the emotional role function scale, women diagnosed with breast cancer suffered larger declines in health than women who remained free from breast cancer. Relative to the controls, women with a breast cancer diagnosis had statistically significant declines in all scales except emotional role function, after adjusting for age and the relevant initial score. After additional adjustment for multiple covariates, the results were not substantially changed (Table 2). After multivariable adjustment, women diagnosed with breast cancer reported relative declines of −7.0 (95% CI: −11.5, −2.6) and −2.9 (95% CI: −6.3, 0.6) on the PCS and MCS scales, respectively, compared to controls.

Health status at baseline and follow-up interviews for women with breast cancer and age-matched women without a breast cancer diagnosis, by SF-36 scale
Discussion
In both cross-sectional and longitudinal analyses, we found that women diagnosed with breast cancer reported poorer health-related QOL compared to women without this diagnosis. Women with a breast cancer diagnosis reported lower scores in six of the eight SF-36 domains, as well as the PCS scale. Similarly, after a breast cancer diagnosis women were more than 10 times as likely to report a decline in self-rated health compared to age-matched control women, and suffered larger declines in seven of the eight SF-36 domains, as well as the PCS scale. The observed differences in the SF-36 scales were substantial (often exceeding 10 points) and remained after controlling for age, health status prior to diagnosis, number of comorbidities, and other covariates.
Several studies have evaluated the association between age at diagnosis and the impact of a breast cancer diagnosis. Satariano [19] found an interaction between age and the reporting of upper-body limitations three months after diagnosis (P = 0.02), with the magnitude of the case/control differences least pronounced for the oldest age group (75–84 years) and larger for younger age groups. Reassuringly, case/control differences in upper-body limitations were not significant 12 months after diagnosis because the cases tended to regain their upper-body strength during the first year (P = 0.67). Other studies suggest that the psychosocial impact of a breast cancer diagnosis is greater in younger women than in older women [20, 33, 34], including a study by Broeckel [20] which reported that younger age was positively related to poorer mental well-being and greater depressive symptomatology. In our study we did not detect an interaction between breast cancer status and age at diagnosis for either the MCS or PCS scales (P interaction = 0.77 and P interaction = 0.56, respectively). There was insufficient power to evaluate interactions in the longitudinal analysis.
In addition to the Satariano [19] and Broeckel [20] studies, only three published reports—all from the Nurses Health Study—have examined differences in functional status before and after a breast cancer diagnosis in women with breast cancer compared to women without breast cancer [21, 22, 35]. Nekhlyudov [35] found that women with ductal carcinoma in situ experienced significant short-term declines in the psychosocial QOL domains. In an analysis of health-related QOL following an invasive breast cancer diagnosis, Kroenke [22] expanded on the preliminary analysis of Michael et al. [21] Kroenke [22] described both relative and absolute changes in functional status among 1,082 female nurses diagnosed with invasive breast cancer and 121,887 female nurses without breast cancer between 1992 and 1997. Younger (ages 29–40 years), middle-aged (ages 41–64 years), and elderly women (ages ≥ 65 years) diagnosed with breast cancer during follow-up maintained their level of vitality relative to women without this diagnosis. Breast cancer survivors in all three age groups reported similar slight declines in physical function relative to women without breast cancer, although absolute declines were greatest for elderly women (about 10 points). Breast cancer survivors in all three age groups reported significant declines in physical role function, bodily pain, and social function relative to women without breast cancer. However, declines were greatest among young women (9 to 19 point decline). While the young breast cancer survivors reported significant absolute and relative declines in mental health (2–4 points), only the elderly breast cancer survivors experienced significant losses in emotional role function (5–8 points). These results may not be broadly generalizable to all breast cancer survivors since, as nurses, the participants in the Kroenke study may be better prepared to anticipate the effects of breast cancer treatments and obtain support in dealing with their diagnoses. In addition, socioeconomic status and baseline QOL scores in the Nurses’ cohorts were higher than the general population [11, 22].
Similarly, we found that breast cancer survivors reported lower health-related QOL across a broad spectrum of domains. In the cross-sectional analysis, women with breast cancer reported lower scores on the physical function, physical role function, bodily pain, general health, vitality, and social function scales. Little difference was observed in the emotional role function and mental health scales. Likewise, in the longitudinal analysis, declines were observed in each domain except emotional role function. It appeared that the relative scores compared to control women were lowest in the physical health as compared to mental health domains. In both the cross-sectional and longitudinal analyses, survivors reported poorer scores on the PCS scale. In the cross-sectional analysis, no difference was observed on the MCS scale between women with and without breast cancer; a small relative decline in the MCS scale was observed in the longitudinal analysis but this did not achieve statistical significance.
Among women with a diagnosis of breast cancer, most dimensions of QOL are generally poor immediately after breast surgery, although most women begin to recover within the post-operative year [15, 36]. It is unknown whether this post-treatment improvement achieves levels similar to those prior to diagnosis. According to the study described by Kroenke [22], certain QOL domain levels may stabilize throughout the survival period, while other domain levels decline depending on age. We similarly found that as time increased since diagnosis, PCS scale scores decreased to a low 2–4 years after diagnosis, after which no further declines were observed (adjusting for age). For the MCS scale, women recently diagnosed reported substantial deficits compared to control women, however, those diagnosed more than two years prior reported similar levels as controls, perhaps even surpassing control women with increasing time since diagnosis.
Vacek [37] suggests that breast cancer reduces QOL by a magnitude similar to other health problems. However, each health condition probably does not impact quality of life similarly, and they most likely interact so that the combined effect is not simply the sum of each contributor. Many older women report multiple comorbid health conditions. In the Beaver Dam population (men and women, mean age 64 years), 82% of participants reported at least 1 medical condition, and 62% of participants reported 2 or more [27]. In our cross-sectional analysis we found no evidence that the number of comorbid conditions significantly influenced the association between breast cancer status and PCS or MCS scale scores (P interaction = 0.57 and P interaction = 0.16, respectively).
Our study, while having many strengths, involved a few limitations that should be considered. Not all women participated in every health assessment over the course of follow-up, either because of refusal, loss to follow-up, or because random sub-samples were selected. Incomplete participation and relatively small numbers of cancer cases may have contributed to the observation that women with breast cancer had lower SF-36 scale values prior to diagnosis than women without breast cancer. However, response rates were outstanding throughout follow-up, ranging between 81% and 89%, and losses to follow-up were minimal, so that the participants likely are representative of the larger Beaver Dam population. Women in the study were of varied socioeconomic and educational status and all aged greater than 45 years. Nevertheless, residents of Beaver Dam, Wisconsin are overwhelmingly of European ancestry and may not be representative of older women in minority racial and ethnic groups.
In conclusion, our study provides further evidence that relative to control women, breast cancer survivors experience declines in health-related QOL across a broad spectrum of health domains. Particularly among the physical health domains, this deficit in QOL remains even 10 years or more after the breast cancer diagnosis. Future studies will continue to clarify the potential modifying effects of age, comorbidities, and other factors on the QOL impact of a breast cancer diagnosis.
References
Ries L, Melbert D, Krapcho M et al (2007) SEER Cancer Statistics Review, 1975–2004. National Cancer Institute, Bethesda, MD, http://seer.cancer.gov/csr/1975_2004/, based on November 2006 SEER data submission, posted to the SEER web site
Brenner H (2002) Long-term survival rates of cancer patients achieved by the end of the 20th century: a period analysis. Lancet 360(9340):1131–1135
Goodwin PJ, Black JT, Bordeleau LJ et al (2003) Health-related quality-of-life measurement in randomized clinical trials in breast cancer—taking stock. J Natl Cancer Inst 95(4):263–281
Costantino J (2002) The impact of hormonal treatments on quality of life of patients with metastatic breast cancer. Clin Ther 24(Suppl C):C26–42
Land SR, Wickerham DL, Costantino JP et al (2006) Patient-reported symptoms and quality of life during treatment with tamoxifen or raloxifene for breast cancer prevention: the NSABP Study of Tamoxifen and Raloxifene (STAR) P-2 trial. JAMA 295(23):2742–2751
Poole CJ, Earl HM, Hiller L et al (2006) Epirubicin and cyclophosphamide, methotrexate, and fluorouracil as adjuvant therapy for early breast cancer. N Engl J Med 355(18):1851–1862
Martin M, Pienkowski T, Mackey J et al (2005) Adjuvant docetaxel for node-positive breast cancer. N Engl J Med 352(22):2302–2313
Li BD, Brown WA, Ampil FL et al (2000) Patient compliance is critical for equivalent clinical outcomes for breast cancer treated by breast-conservation therapy. Ann Surg 231(6):883–889
Mandelblatt J, Figueiredo M, Cullen J (2003) Outcomes and quality of life following breast cancer treatment in older women: When, why, how much, and what do women want? Health Qual Life Outcomes 1(1):45
Mols F, Vingerhoets AJ, Coebergh JW et al (2005) Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer 41(17):2613–2619
Ware J Jr, Snow K, Kosinski M et al (1993) SF-36 health survey manual and interpretation guide. The Health Institute, New England Medical Center, Boston, MA
Shimozuma K, Sonoo H, Ichihara K (1995) Analysis of the factors influencing the quality of life of patients with advanced or recurrent breast cancer. Surg Today 25(10):874–882
Engel J, Kerr J, Schlesinger-Raab A et al (2003) Predictors of quality of life of breast cancer patients. Acta Oncol 42(7):710–718
Satariano WA, Ragheb NE, Buck KA et al (1989) Aging and breast cancer: a case–control comparison of instrumental functioning. J Aging Health 1:209–233
Bloom JR, Stewart SL, Chang S et al (2004) Then and now: quality of life of young breast cancer survivors. Psychooncology 13(3):147–160
Ganz PA, Guadagnoli E, Landrum MB et al (2003) Breast cancer in older women: quality of life and psychosocial adjustment in the 15 months after diagnosis. J Clin Oncol 21(21):4027–4033
Vinokur AD, Threatt BA, Caplan RD et al (1989) Physical and psychosocial functioning and adjustment to breast cancer. Long-term follow-up of a screening population. Cancer 63(2):394–405
Vinokur AD, Threatt BA, Vinokur-Kaplan D et al (1990) The process of recovery from breast cancer for younger and older patients. Changes during the first year. Cancer 65(5):1242–1254
Satariano WA, Ragland DR (1996) Upper-body strength and breast cancer: a comparison of the effects of age and disease. J Gerontol A Biol Sci Med Sci 51(5):M215–219
Broeckel JA, Jacobsen PB, Balducci L et al (2000) Quality of life after adjuvant chemotherapy for breast cancer. Breast Cancer Res Treat 62(2):141–150
Michael YL, Kawachi I, Berkman LF et al (2000) The persistent impact of breast carcinoma on functional health status: prospective evidence from the Nurses’ Health Study. Cancer 89(11):2176–2186
Kroenke CH, Rosner B, Chen WY et al (2004) Functional impact of breast cancer by age at diagnosis. J Clin Oncol 22(10):1849–1856
Klein BE, Klein R, Lee KE et al (2006) Statin use and incident nuclear cataract. JAMA 295(23):2752–2758
Klein R, Klein BE, Linton KL et al (1991) The Beaver Dam Eye Study: visual acuity. Ophthalmology 98(8):1310–1315
Cruickshanks KJ, Tweed TS, Wiley TL et al (2003) The 5-year incidence and progression of hearing loss: the epidemiology of hearing loss study. Arch Otolaryngol Head Neck Surg 129(10):1041–1046
Cruickshanks KJ, Wiley TL, Tweed TS et al (1998) Prevalence of hearing loss in older adults in Beaver Dam, Wisconsin. The Epidemiology of Hearing Loss Study. Am J Epidemiol 148(9):879–886
Fryback DG, Dasbach EJ, Klein R et al (1993) The Beaver Dam Health Outcomes Study: initial catalog of health-state quality factors. Med Decis Making 13(2):89–102
Shankar A, Klein BE, Klein R (2004) Relationship between white blood cell count and incident hypertension. Am J Hypertens 17(3):233–239
Klein R, Klein BE, Lee KE (1996) Changes in visual acuity in a population. The Beaver Dam Eye Study. Ophthalmology 103(8):1169–1178
Klein R, Klein BE, Lee KE et al (2001) Changes in visual acuity in a population over a 10-year period: The Beaver Dam Eye Study. Ophthalmology 108(10):1757–1766
Ware J Jr, Kosinski M, Keller S (1994) SF-36 physical and mental health summary scales: a user’s manual. Health Assessment Lab, New England Medical Center, Boston, MA
Palta M (2003) Quantitative methods in population health; extensions of ordinary regression. John Wiley & Sons, Inc, Hoboken, NJ
Ganz PA, Desmond KA, Leedham B et al (2002) Quality of life in long-term, disease-free survivors of breast cancer: a follow-up study. J Natl Cancer Inst 94(1):39–49
Ganz PA, Greendale GA, Petersen L et al (2003) Breast cancer in younger women: reproductive and late health effects of treatment. J Clin Oncol 21(22):4184–4193
Nekhlyudov L, Kroenke CH, Jung I et al (2006) Prospective changes in quality of life after ductal carcinoma-in-situ: results from the Nurses’ Health Study. J Clin Oncol 24(18):2822–2827
Shimozuma K, Ganz PA, Petersen L et al (1999) Quality of life in the first year after breast cancer surgery: rehabilitation needs and patterns of recovery. Breast Cancer Res Treat 56(1):45–57
Vacek PM, Winstead-Fry P, Secker-Walker RH et al (2003) Factors influencing quality of life in breast cancer survivors. Qual Life Res 12(5):527–537
Acknowledgements
This study was supported in part by faculty startup funds from the University of Wisconsin School of Medicine & Public Health, National Institutes of Health grants U10 EY006594 and R01 AG11099, grant HS06941 by the Agency for Healthcare Research and Quality, and grant POP0504237 by the Komen for the Cure breast cancer foundation. The authors would like to acknowledge Kristine Lee, Scot Moss, Michael Knudtson, Laura Stephenson and the staff of the Wisconsin Cancer Reporting System, Hazel Nichols, Andy Bersch, Moneen Meuer, Mayor Jack Hankes, and the participants of the Beaver Dam Studies for their invaluable contributions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Trentham-Dietz, A., Sprague, B.L., Klein, R. et al. Health-related quality of life before and after a breast cancer diagnosis. Breast Cancer Res Treat 109, 379–387 (2008). https://doi.org/10.1007/s10549-007-9653-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-007-9653-1