
Abstract
Although widely used, no proof exists for the feasibility of neurofeedback for reinstating the disordered excitatory–inhibitory balance, marked by a decrease in auditory alpha power, in tinnitus patients. The current study scrutinizes the ability of neurofeedback to focally increase alpha power in auditory areas in comparison to the more common rTMS. Resting-state MEG was measured before and after neurofeedback (n = 8) and rTMS (n = 9) intervention respectively. Source level power and functional connectivity were analyzed with a focus on the alpha band. Only neurofeedback produced a significant decrease in tinnitus symptoms and—more important for the context of the study—a spatially circumscribed increase in alpha power in right auditory regions. Connectivity analysis revealed higher outgoing connectivity in a region ultimately neighboring the area in which power increases were observed. Neurofeedback decreases tinnitus symptoms and increases alpha power in a spatially circumscribed manner. In addition, compared to a more established brain stimulation-based intervention, neurofeedback is a promising approach to renormalize the excitatory–inhibitory imbalance putatively underlying tinnitus. This study is the first to demonstrate the feasibility of focally enhancing alpha activity in tinnitus patients by means of neurofeedback.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Subjective tinnitus, a condition characterized by the sensation of a sound without any physical source, affects roughly 10 % of the general population. In 10 % of patients, the condition leads to a significant decrease in quality of life (Heller 2003). Consistent findings over the past years have shown that: (a) tinnitus is a disorder of the brain (Eggermont and Roberts 2004), (b) the underlying cause of tinnitus is a deficit of inhibition triggered by the loss of afferent input to relevant areas (Weisz et al. 2007a).
Recent research has also led to great insights into the neuronal correlates of tinnitus. A relevant finding is reduced ongoing (spontaneous) alpha power in auditory areas (Lorenz et al. 2009; Weisz et al. 2005; Weisz et al. 2007b). Originally attributed to the idling of the underlying cortical region (Pfurtscheller et al. 1996), recent studies have shown that alpha oscillations rather represent the excitatory–inhibitory balance of underlying cortical areas, with a strong alpha representing a state of relative inhibition. Furthermore, increasing evidence demonstrates that the occurrence of alpha oscillations is not limited to the visual and somatosensory system but is also found in the auditory system, with comparable functional correlates (Weisz et al. 2011). At a system level, three main lines of research concerning the power of alpha oscillations exist: (1) an active inhibition of cortical areas that would possibly interfere with a task to be solved (Jensen and Mazaheri 2010); (2) spontaneous fluctuations in alpha power that alter the perception of incoming stimuli or those induced at the cortical level (Min and Herrmann 2007; Romei et al. 2008a); and (3) the impact of resting-state alpha power on perception (Hanslmayr et al. 2007; Romei et al. 2008b) or its relationship with diseases like tinnitus (Lorenz et al. 2009; Weisz et al. 2005; Weisz et al. 2007a, b ). While the association between alpha oscillations and inhibition has until now been based on behavioral associations, a recent study by (Haegens et al. 2011) shows the link between cellular recordings, alpha power and behavioral measurements, thus strengthening the inhibition hypothesis. In conjunction with the aforementioned results on the neural correlates of tinnitus, the hypothesis is that decreased auditory cortical alpha in tinnitus could be a useful proxy for decreased inhibition in the auditory cortex. Interestingly, increases in alpha activity following neurofeedback have been reported to lead to significant decreases in distress scores (Crocetti and Forti 2011; Dohrmann et al. 2007a, b). Although it is tempting to presume that these alpha enhancements contributed to a normalization of the disturbed excitatory–inhibitory balance, the aforementioned studies lack convincing evidence that auditory cortical alpha activity had indeed been enhanced.
The current study investigates the feasibility of enhancing alpha oscillations in a focal manner—in this case in the primary auditory cortex. This was achieved via neurofeedback training that visualized alpha power projected to regional dipoles to the patients. This approach greatly differs from conventional neurofeedback training methods, which either feed back sensor-domain data from one electrode or apply a (weighted) average over electrodes in one region. Although widely employed in neurofeedback therapy paradigms, this approach suffers from the fact that signals acquired at EEG sensors are highly unspecific since they are the sum of multiple sources. Source space projection disentangles the different sources and thus targets the training region more precisely. In order to give evidence for this claim, data from the neurofeedback experiment are compared to neurophysiological modulations induced by a 1 Hz repetitive transcranial magnetic stimulation (rTMS) paradigm including within-subject sham control. This (allegedly inhibitory) cortical stimulation paradigm has been reported to be effective in some studies (Folmer et al. 2006; Khedr et al. 2009; Kleinjung et al. 2007; Lorenz et al. 2010), although a recent analysis of a large sample of patients in a double-blind controlled study has shown that the effects are weak and only about one third of patients actually responded to treatment (Langguth et al. 2012).
The tinnitus-induced distress cannot solely be explained by altered activity in lower-level auditory areas. It is therefore obvious that long-range connectivity between auditory and higher-order areas is of high interest, for which previous studies have already reported corresponding results (Plewnia 2010; Schlee et al. 2009; Vanneste et al. 2011). We therefore extended our analysis to scrutinize long-range connectivity in source space when modulations of cortical activity in the power domain were found as hypothesized.
Methods
Data from two experiments are reported. Subjects took part either in the rTMS or in the neurofeedback study.
Subjects
Initially, 12 patients took part in the neurofeedback study. Inclusion criteria for the neurofeedback study were as follows: (1) age between 18 and 75; (2) tinnitus duration of at least 1 year; (3) No history of neurological conditions; (4) no current psychiatric conditions excluding mild dysthymia or mild depression (assessed with the German version of the MINI interview (Lecrubier et al. 1997)). One patient decided to stop the treatment because of a lack of improvement. Three further patients completed the treatment but had to be excluded from data analysis due to excessive artifacts in the MEG data (criteria being a maximum of six bad channels and 40 % bad trials in the data). This left eight patients (one female, mean age ± standard deviation: 57 ± 9 years) for analysis. These patients had suffered from tinnitus for an average of 5.4 years (standard deviation: 6.4 years). The average distress, assessed using the German version of the tinnitus questionnaire (Goebel and Hiller 1994), was 22.6 (standard deviation: 10.0). One patient suffered from mild dysthymia according to the M.I.N.I. interview (Lecrubier et al. 1997) and was treated using 60 mg Amoxid per day. All other patients were free of psychiatric diagnoses and psychoactive medication. The rTMS study was conducted on 10 patients. Inclusion criteria for the rTMS study were as follows: (1) age between 18 and 85; (2) tinnitus duration between 1 and 4 years; (3) no history of neurological and psychological conditions. One patient was excluded due to artifacts in the MEG data. This left nine patients (two female, mean age ± standard deviation: 50 ± 15 years). These patients had suffered from tinnitus for an average of 2.3 years (standard deviation: 1.2 years). The average distress was 26.2 (standard deviation 14.8). All patients in the TMS group were free of psychiatric diagnoses and psychoactive medication. The groups did not differ in age (two-sided t test, p = 0.25), tinnitus distress (p = 0.9) and tinnitus duration (p = 0.2).
All patients provided their written informed consent prior to participating. The procedures of the rTMS study as well as the neurofeedback study were separately approved by the Institutional Review Board of the University of Konstanz.
Study Design
Neurofeedback
Patients in the neurofeedback group received 10 sessions of auditory alpha neurofeedback over a period of approximately 4 weeks (two to three sessions per week). Approximately 1 week before the first session and 1 week after the last session, 5 min of resting-state MEG (eyes open) were recorded using a 148-channel whole-head magnetometer system (MAGNES 2500WH, 4d Neuroimaging, San Diego, USA) installed in a magnetically shielded room (Vakuumschmelze Hanau, Germany).
Neurofeedback was conducted using a 32-channel EEG System (Neuroconn, Ilmenau, Germany). The acquired data were processed in real time using ConSole (Hartmann et al. 2011) and fed back to the patient via a TFT screen.
Each session consisted of one baseline measurement to calibrate the neurofeedback system, four training runs and another baseline measurement following the training in order to assess changes in cortical activity. In the training runs, patients were shown a feedback on the screen for 5 s without hearing a tone. They were instructed to consider this period as a baseline that showed how auditory areas of their brain behaved in the absence of input. Afterwards, patients were stimulated for another 5 s with a sound that was spectrally filtered to match their tinnitus percept as closely as possible (Noreña et al. 2002). An alpha increase above an individually defined threshold of one second within the second 5 s period was rewarded by displaying a smiley on the screen. We thus tried to exploit the well-known effect of auditory alpha desynchronizing upon sensory input (Lehtelä et al. 1997; Mimura et al. 1962; Weisz et al. 2011). The rationale behind this approach was to provide patients with the possible strategy of enhancing auditory alpha power by decreasing the attention paid to the sound (Müller and Weisz 2011). Apart from this, it should also be possible for patients to transfer the learned strategy of ignoring a “tinnitus-like” sound to ignoring the actual tinnitus percept. Baseline measurements only differed from the training runs insofar as they did not provide feedback to the patients. The patients were instructed to passively listen to the sounds with their eyes open.
Data acquired from 29 electrodes on the scalp and two electrodes beside and above the right eye to facilitate artifact correction were sent to ConSole. The DC part of the signal was filtered out using an optimized recursive filter (y(t) = x(t) − x(t − 1) + 0.995 × y(t − 1)). The data were then low-pass filtered (4th order Butterworth filter; cutoff: 16 Hz), average referenced and artifact corrected via ICA (JADE algorithm (Cardoso and Souloumiac 1993)). Next, the data were projected onto eight regional sources. The data of the two temporal sources were subjected to frequency analysis and the relative energy at the individual’s alpha frequency was averaged and fed back to a computer screen.
Tinnitus distress was measured in a diagnostic session approximately 1 week before the first MEG measurement and at the last neurofeedback session using the German adaption of the tinnitus questionnaire (Goebel and Hiller 1994).
rTMS
Patients in the rTMS group received sham and verum treatments in a pseudo-randomized crossover design. To avoid potential carryover effects, the two stimulation series were separated by 3 months. Ten sessions of rTMS were conducted over 10 consecutive working days using a biphasic MAGSTIM system (Rapid2, MAGSTIM CO., Whitland, Dyfed, UK) and an air-cooled figure-of-eight coil (MAGSTIM Air Film Coil, 70 mm). The handle of the coil was pointed upwards. Neuronavigation (Advanced Neuro Technology, Enschede, Netherlands) was used to target the main generator of the auditory N1 contralateral to the predominant tinnitus location (locations derived for all participants from data published by Lorenz et al. (2010)). Each rTMS session consisted of 1,000 pulses administered at 1 Hz, which is by far the most frequently used rTMS protocol in tinnitus treatment (see, e.g. Langguth et al. 2012). The intensity was 50 % of maximum stimulator output. The same parameters were applied for the sham condition, but the coil was tilted by 45° over one wing. As for the neurofeedback group, 5 min of resting-state MEG were recorded before and after each treatment series. The setup was the same as in the neurofeedback study. Tinnitus distress was measured when patients came for MEG examination using the German version of the TQ (Goebel and Hiller 1994).
Data from the rTMS group with a detailed region of interest analysis are presented in a companion article (Müller et al. 2013). The present study focuses on alpha-related changes and modulations in long-range connectivity patterns.
Data Analysis
MEG data from both neurofeedback and rTMS subjects were analyzed using FieldTrip (Oostenveld et al. 2011), an open source toolbox for MEG and EEG analysis in Matlab (The Mathworks). The 5 min resting-state data were epoched into segments of 2 sec each (no overlap). The resulting epochs were carefully examined for artifacts. Channels that showed excessive noise or other artifacts below 20 Hz were interpolated using spline interpolation (Perrin et al. 1989).
Subsequent analysis was carried out entirely in source space. We therefore generated equally spaced dipole grids of 5 mm and 10 mm resolution on the MNI brain provided by the SPM8 toolbox (http://www.fil.ion.ucl.ac.uk/spm/software/spm8/) and morphed the grid to the patients’ individual head shapes. The individual positions of the grid points in each patient’s brain thus approximately represented the same anatomical region. Forward models for each patient were computed using the “sensor-weighted overlapping spheres” algorithm (Huang et al. 1999).
For the power analysis, we first computed the cross-spectral density matrix (CSD) for each trial between 8 and 12 Hz (FFT with hanning taper). To calculate the spatial filter for source space projection, the data were first high-pass (8 Hz, 4th order zero-phase Butterworth filter) and low-pass (12 Hz, 4th order zero-phase Butterworth filter) filtered. The covariance between all channels of the filtered data was used to calculate the spatial filter using the LCMV beamformer algorithm (Van and Van 1997) with 15 % regularization. The resulting spatial filter was then used to project the CSD matrix into source space using the 5 mm grid. The diagonal of the resulting matrix was the energy of each channel in the respective frequency band, as used for further power analysis.
We used the 10 mm spaced grid for the connectivity analysis owing to memory and computing power constraints. The same forward models as in the power analysis were used. The spatial filter was again confined to activity between 8 and 12 Hz and regularized by 15 %. The CSD matrix was then projected onto source space. In order to calculate effective connectivity, the phase slope index (PSI) (Nolte et al. 2008; Nolte and Müller 2010) was calculated between the center frequency ±2 Hz. The PSI measures the slope of the difference of the phases of two signals in the frequency domain. As for every measure of effective connectivity, direction is determined by measuring if signal a comes before signal b or vice versa. The PSI exploits the fact that, if signal a comes before signal b, the slope of the difference between the phases of the signals is positive, while this difference is negative if signal b comes before signal a. A distribution of the resulting PSI values was calculated for each subject and condition (pre and post) and then used to threshold the individual connections. Only those connections that had a PSI value higher or lower than two standard deviations were kept. This thresholding provided the adjacency matrix required for the computation of node degree (Bullmore and Sporns 2009)—that is, the sum of each voxel’s connection to other voxels. We took advantage of the ability of the PSI to differentiate the direction of the connections. We named the connections from the perspective of the voxel being analyzed. If another voxel influences the voxel under scrutiny, this is defined as an incoming connection, because information is flowing into the voxel. Vice versa, if the voxel under scrutiny exerts influence on another voxel, i.e., information if flowing from the scrutinized voxel to another one, this connection is termed “outgoing”.
Statistical Analysis
In order to assess whether the decrease in tinnitus-related impairment differed between three groups (NFB, TMS, sham), we calculated the relative improvement for each patient in each group ((Pre–Post)/Pre). We then calculated individual, one-sided t tests (dependent samples for TMS vs. sham, independent samples for the other two combinations) and calculated the effect sizes (Cohen’s d) for each individual treatment approach.
The power and node degree of the MEG measurements were compared within each group using a cluster-based non-parametric, permutation-based statistic (Maris and Oostenveld 2007) that controls the type I error with respect to multiple comparisons. First, ordinary t statistics (post vs. pre, one-sided for power analysis, two-sided for node degree analysis) were calculated. The cluster-finding algorithm identified clusters of neighboring voxels and frequency bins that had a p < 0.05. The test statistic for the permutation test was the sum of all t values in a cluster. The statistic was repeated for shuffled data, for which data were randomly reordered across conditions (the null hypothesis stating that power or node degree did not differ between pre and post measurements). Upon each permutation, the cluster with the highest sum of t values was kept. By these means, a null distribution of 1,000 permutations could be created and the p values for the empirically derived clusters could be calculated.
Results
Tinnitus Questionnaires
We compared the behavioral effect of all three interventions measured using the German version of the TQ. Patients in the neurofeedback group improved significantly compared to patients in the sham group (p < 0.005), decreasing TQ scores on average from 22.6 (standard deviation: 10.0) to 14.8 (standard deviation: 11.2), resulting in an effect size of 0.74. They also performed significantly better than patients in the rTMS group (p < 0.03). Patients in the rTMS group did not perform better than under sham treatment (p < 0.19), achieving an effect size of only 0.14 (0.13 in the sham condition) (see Fig. 1).

Average distress decrease for the three conditions involved in the study according the tinnitus questionnaire. Only neurofeedback led to a significant decrease in distress (p < 0.005)
Power Analysis
As stated in the introduction, the main goal of both intervention techniques is an increase in inhibitory activity in auditory cortical regions, which should manifest itself through increases in alpha oscillations in auditory cortical areas. However, we were additionally interested in whether other areas would also be modulated by one of the approaches used. To circumvent the problem of multiple comparisons, we used a cluster-based, non-parametric permutation-based approach (Maris and Oostenveld 2007). However, no significant cluster was found for either condition.
In a next step, we used an exploratory approach, focused in detail on the auditory cortices, the regions that were the initial target of both treatments. These results showed a significant increase (p < 0.05) in alpha power following treatment in the vicinity of the right auditory cortex for the neurofeedback group alone. Verum rTMS led to a non-significant increase in alpha power, while the effect in the sham condition remained negligible, as can be seen in Fig. 2. To further investigate whether the three groups differed with respect to an alpha power increase in the right auditory cortex, we used one-sided t tests to compare the relative increases around the voxel showing the highest t value (averaged over all conditions, cubic ROI with 10 mm edge length (dependent samples for rTMS vs. sham, independent for the other two)). Neurofeedback significantly increased alpha power in this region compared the sham condition (p < 0.04) as well as showing a trend when compared to the rTMS conditions (p < 0.09). The comparison rTMS to sham did not reach significance (see Fig. 2b). The spectrum over a broader frequency range also shows an increase of alpha power after TMS intervention. Yet, this is confined to a very small band and might as well be a statistical artifact. In summary, this confirms that the effect is specific to (a) the neurofeedback approach and (b) the alpha band (see Fig. 3).

Increase in alpha power following treatment at right auditory regions. a Voxels in the neurofeedback condition that showed a significant increase in alpha power. The effect was located at and in the vicinity of BA41. b Comparison of the relative alpha increase for all three conditions

Pre–post frequency spectra for all three conditions. Significant frequency bins (one sided t test, p < 0.05, uncorrected) are marked in darker colors. As hypothesized, only neurofeedback treatment yields a significant increase of about 40 % which is focused on the alpha band. TMS intervention leads to a small, yet mostly insignificant increase at a very narrow frequency range around alpha as well as two tiny increases in the beta band
Neurofeedback is still the only condition in which we saw an alpha power increase after we had repeated the analysis using the hemisphere ipsilateral to stimulation for the rTMS conditions (data not shown).
Connectivity Analysis
Recent publications suggest a relationship between local synchronization in the alpha band and long-range connectivity of the specific region with other areas in the brain (Haegens et al. 2011; Jensen and Mazaheri 2010), although this idea still awaits empirical confirmation. We thus analyzed whether the reported increase in alpha power in the right auditory cortex following neurofeedback training would co-occur with a decrease in that region’s long-range connectivity. The so-called node-degree, a graph-theoretical measure that counts the significant connections (here computed via the PSI method) to and from one node (in this case, one voxel), was calculated.
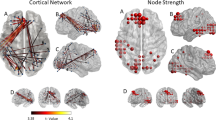
The cluster-based strategy for the whole cortex did not reveal any significant cluster in any group or condition. At the uncorrected level, we did, however, find a significant increase in outgoing connections following treatment of the neurofeedback group in a region directly neighboring the alpha power increase (Fig. 4), i.e., the amount of voxels influenced by activity in the depicted region was increased after the treatment. In order to scrutinize a possible relationship between the two regions, we correlated the voxels with the highest t values in each of the regions, using the relative change in power and connectivity. This correlation between power and an increase in connectivity was neither significant testing for a linear correlation (r = 0.27, p = 0.52), nor when we tested it with the non-parametric spearman correlation (r = 0.36, p = 0.39), which may be due to the low amount of remaining patients. However, we found that, of the eight patients in the analysis, six showed an increase in power, seven showed an increase in outgoing connectivity and power. In seven of the eight patients, power and connectivity at the non-overlapping right auditory areas changed in the same direction (either both increased or decreased). The null hypothesis of the latter distribution being due to chance can be rejected according to a one-sided binomial test with a significance level of 0.05 (p = 0.03). This is suggestive of a relationship (albeit not linear) between alpha power and connectivity changes.
Nevertheless, increases and decreases in long-range connectivity are more ubiquitous than the aforementioned effects for power (i.e., local synchrony). We found that auditory areas in the left hemisphere received significantly less information after neurofeedback training (Fig. 5).

a Increase in alpha node degree for outgoing connections following neurofeedback training. The effect is located in an adjacent region that shows the power increase. As can be seen in subfigure b, the overlap between both regions is very small (Color figure online)

Decrease in alpha node degree for ingoing connections following neurofeedback training. The effect is located at the left BA41 and in neighboring regions
Discussion
In recent years, a relationship between the severity of tinnitus distress and a chronic decrease in alpha synchronization in auditory cortical areas has been proposed (e.g., Lorenz et al. 2009; Weisz et al. 2007a, b ). According to this framework, one therapeutic approach to alleviate tinnitus by normalizing the disturbed excitatory–inhibitory balance should be to reliably increase auditory cortical alpha power using, for instance, neurofeedback. We also expected to observe an increase in alpha power in auditory cortical areas following the application of 1 Hz (putatively inhibitory) rTMS, as this is a widely accepted indicator of cortical inhibition and is directly related to the proposed mechanism behind this method.
Recent research has shown positive results for neurofeedback on cognitive performance (see, e.g., Zoefel et al. 2011) as well as specifically on tinnitus distress (Crocetti and Forti 2011; Dohrmann et al. 2007a), while the effects of rTMS seem to be smaller and less reliable (Khedr et al. 2009; Kleinjung et al. 2007; Langguth et al. 2012; Meng et al. 2011). The current study only shows significant effects in patients who were treated using neurofeedback, whereas the rTMS effects are marked by an enormous interindividual variability.
At the behavioral level, patients in the neurofeedback group decreased their distress by an average of 35 % (see Fig. 1). This finding confirms other studies, in which alpha-based neurofeedback was used (Crocetti and Forti 2011; Dohrmann et al. 2007b), although these protocols differed. However, due to the small number of patients in each of the groups and the missing control group for the neurofeedback patients, this study is not intended to be a treatment study. The more interesting (and valid) findings are about the neurophysiological changes induced by the two “therapeutic approaches” and the sham condition.
Although the claim of both interventions is the long-lasting modulation of the cortical networks responsible for the tinnitus perception and/or the distress caused by it, the current study is the first to systematically scrutinize the impact of both methods at a cortical level. More specifically, both methods claim to induce local changes that can be operationalized by modulations in local synchrony, visible in the MEG as altered oscillatory power.
Although both methods targeted the same regions, we only found alpha power modulations at auditory sites in the neurofeedback group, albeit only in the right and not in the similarly targeted left hemisphere (see Fig. 2). One possible explanation for this is that as the activity in both of the left and right hemispheres was averaged prior to feedback, it was sufficient to increase alpha power at the right source alone in order to evoke positive feedback. Neurofeedback was also the only condition that yielded improvements in tinnitus distress. The strong regional specificity of the alpha effects in the auditory cortex argues against notions that neurofeedback enhanced “relaxation” alpha, thus leading to non-specific clinical improvements. However, the correlation between the alpha power increase and distress alleviation is far from significant under the assumption that a potential relationship could be linear. The question of whether a relationship exists between the failure of rTMS to improve tinnitus distress and the absence of an alpha power increase or if rTMS exploits a different mechanism not covered in our analysis in order to increase inhibition remains speculative. Other rTMS studies have shown more positive results at the behavioral level but have not reported neurophysiological effects (Folmer et al. 2006; Khedr et al. 2009; Kleinjung et al. 2007; Langguth et al. 2006). It might also be worthwhile to consider a different rTMS paradigm. For instance, stimulating with 10 Hz could lead to promising results (for a review see, e.g., Kleinjung et al. 2007), especially as recent studies have shown that rTMS is able to entrain underlying regions, although only short term effects are reported so far (see, e.g., Thut et al. 2011).
Apart from local synchronization (measured by power changes in oscillatory activity), we also searched for modulations in long-range connectivity induced by the applied techniques. In the neurofeedback condition, we found an increase in the outgoing node degree in the alpha band—in other words, the number of other voxels in the brain receiving input from the seed voxel. The effect was found in an area directly adjacent to the region in which alpha power increased following neurofeedback treatment (see Fig. 4). Both effects were very stable, as six of eight patients showed a power increase, seven an increase in outgoing connectivity, and in seven the power modulation matched with the connectivity modulation. Two possible explanations exist for this: the power increase in the right primary auditory regions was driven by an increased outgoing information flow from the neighboring region (although this is not backed by the data), or the inhibition of the right primary auditory regions led to increased outgoing activity in the neighboring one by means of lateral inhibition. Of course, volume conduction between the two neighboring areas could also explain the effect. However, volume conduction could not explain why the effect was restricted to outgoing connectivity as well as the strong segregation between the region of power and outgoing connectivity increase.
In addition to the effect co-occurring with the power increase, the left auditory cortex showed a decrease in ingoing connections following neurofeedback treatment that was not accompanied by a significant power change (see Fig. 5). However, although this claim is speculative, training the brain to increase alpha power at a specific site should, according to recent research, lead to decreased functional connectivity (Jensen and Mazaheri 2010).
Conclusion
In the current study, neurofeedback was clearly superior to rTMS with respect to decreasing tinnitus distress. Interestingly, these positive behavioral effects were accompanied by strong increases in alpha power co-occurring with a neighboring decrease in outgoing alpha connectivity and thereby putative inhibition in auditory areas. These effects suggest for the first time that EEG neurofeedback can be used to target tinnitus-relevant processes and brain regions with high spatial specificity. Neither verum nor sham rTMS treatment showed effects on distress or on the power of ongoing alpha oscillations following treatment.
The neurophysiological effects of neurofeedback shown in this study are very specific to the areas that were trained. The question of whether rTMS provides a similar specific modulation cannot be answered here, as no corresponding effect was found. However, it is likely that rTMS reduces tinnitus (as observed in other studies) via a mechanism different to those found for neurofeedback and maybe even via influencing areas distant from the stimulation site. If this is the case, rTMS effects could also manifest themselves differently.
References
Bullmore E, Sporns O (2009) Complex brain networks: graph theoretical analysis of structural and functional systems. Nat Rev Neurosci 10:186–198. doi:10.1038/nrn2575
Cardoso JF, Souloumiac A (1993) Blind beamforming for non-Gaussian signals. Radar and Signal Processing, IEE Proceedings F. IET, pp 362–370
Crocetti A, Forti S (2011) Neurofeedback for subjective tinnitus patients. Auris Nasus Larynx 38:735–738. doi:10.1016/j.anl.2011.02.003
Dohrmann K, Elbert T, Schlee W, Weisz N (2007a) Tuning the tinnitus percept by modification of synchronous brain activity. Restor Neurol Neurosci 25:371–378. doi:17943012
Dohrmann K, Weisz N, Schlee W et al (2007b) Neurofeedback for treating tinnitus. Prog Brain Res 166:473–485
Eggermont JJ, Roberts LE (2004) The neuroscience of tinnitus. Trends Neurosci 27:676–682. doi:10.1016/j.tins.2004.08.010
Folmer RL, Carroll JR, Rahim A et al (2006) Effects of repetitive transcranial magnetic stimulation (rTMS) on chronic tinnitus. Acta Otolaryngol 126:96–101. doi:10.1080/03655230600895465
Goebel G, Hiller W (1994) The tinnitus questionnaire: a standard instrument for grading the degree of tinnitus—results of a multicenter study with the tinnitus questionnaire. HNO 42:166–172
Haegens S, Nácher V, Luna R et al (2011) α-Oscillations in the monkey sensorimotor network influence discrimination performance by rhythmical inhibition of neuronal spiking. Proc Natl Acad Sci USA. doi:10.1073/pnas.1117190108
Hanslmayr S, Aslan A, Staudigl T et al (2007) Prestimulus oscillations predict visual perception performance between and within subjects. Neuroimage 37:1465–1473. doi:10.1016/j.neuroimage.2007.07.011
Hartmann T, Schulz H, Weisz N (2011) Probing of brain states in real-time: introducing the ConSole environment. Front Psychol. doi:10.3389/fpsyg.2011.00036
Heller AJ (2003) Classification and epidemiology of tinnitus. Otolaryngol Clin North Am 36:239–248. doi:10.1016/S0030-6665(02)00160-3
Huang M, Mosher JC, Leahy R (1999) A sensor-weighted overlapping-sphere head model and exhaustive head model comparison for MEG. Phys Med Biol 44:423
Jensen O, Mazaheri A (2010) Shaping functional architecture by oscillatory alpha activity: gating by inhibition. Front hum neurosci 4:8
Khedr E, Rothwell J, El-Atar A (2009) One-year follow up of patients with chronic tinnitus treated with left temporoparietal rTMS. Eur J Neurol 16:404–408. doi:10.1111/j.1468-1331.2008.02522.x
Kleinjung T, Steffens T, Londero A, Langguth B (2007) Transcranial magnetic stimulation (TMS) for treatment of chronic tinnitus: clinical effects. Prog Brain Res 166:359–367. doi:10.1016/S0079-6123(07)66034-8
Langguth B, Hajak G, Kleinjung T et al (2006) Repetitive transcranial magnetic stimulation and chronic tinnitus. Acta Otolaryngol 126:102–104. doi:10.1080/03655230600895457
Langguth B, Landgrebe M, Frank E, et al. (2012) Efficacy of different protocols of transcranial magnetic stimulation for the treatment of tinnitus: pooled analysis of two randomized controlled studies. World j biol psychiatry: the official journal of the World Federation of Societies of Biological Psychiatry 1–10. doi:10.3109/15622975.2012.708438
Lecrubier Y, Sheehan D, Weiller E et al (1997) The mini international neuropsychiatric interview (MINI): a short diagnostic structured interview—reliability and validity according to the CIDI. Eur Psychiatry 12:224–231. doi:10.1016/S0924-9338(97)83296-8
Lehtelä L, Salmelin R, Hari R (1997) Evidence for reactive magnetic 10 Hz rhythm in the human auditory cortex. Neurosci Lett 222:111–114. doi:10.1016/S0304-3940(97)13361-4
Lorenz I, Müller N, Schlee W et al (2009) Loss of alpha power is related to increased gamma synchronization-A marker of reduced inhibition in tinnitus? Neurosci Lett 453:225–228. doi:10.1016/j.neulet.2009.02.028
Lorenz I, Müller N, Schlee W et al (2010) Short-term effects of single repetitive TMS sessions on auditory evoked activity in patients with chronic tinnitus. J Neurophysiol 104:1497. doi:10.1152/jn.00370.2010.Short-Term
Maris E, Oostenveld R (2007) Nonparametric statistical testing of EEG-and MEG-data. J Neurosci Methods 164:177–190. doi:10.1016/j.jneumeth.2007.03.024
Meng Z, Liu S, Zheng Y, Phillips J (2011) Repetitive transcranial magnetic stimulation for tinnitus. Cochrane Database of Syst Rev. doi:10.1002/14651858.CD007946.pub2
Mimura K, Sato K, Ozaki T et al (1962) On the physiological significance of the EEG changes caused by sonic stimulation. Electroencephalogr Clin Neurophysiol 14:683
Min B-K, Herrmann CS (2007) Prestimulus EEG alpha activity reflects prestimulus top-down processing. Neurosci Lett 422:131–135. doi:S0304-3940(07)00701-X
Müller N, Weisz N (2011) Lateralized auditory cortical alpha band activity and interregional connectivity pattern reflect anticipation of target sounds. Cereb Cortex. doi:10.1093/cercor/bhr232
Müller N, Lorenz I, Langguth B, Weisz N (2013) rTMS induced tinnitus relief is related to an increase in auditory cortical alpha activity. PLoS ONE 8:e55557. doi:10.1371/journal.pone.0055557
Nolte G, Müller K-R (2010) Localizing and estimating causal relations of interacting brain rhythms. Front hum neurosci 4:209. doi:10.3389/fnhum.2010.00209
Nolte G, Ziehe A, Nikulin V et al (2008) Robustly estimating the flow direction of information in complex physical systems. Phys Rev Lett 100:1–4. doi:10.1103/PhysRevLett.100.234101
Noreña AJ, Micheyl C, Chéry-Croze S, Collet L (2002) Psychoacoustic characterization of the tinnitus spectrum: implications for the underlying mechanisms of tinnitus. Audiol Neurootol 7:358–369. doi:10.1159/000066156
Oostenveld R, Fries P, Maris E, Schoffelen J-M (2011) Fieldtrip: open source software for advanced analysis of MEG, EEG, and invasive electrophysiological data. Comput Intell Neurosci 2011:1–9. doi:10.1155/2011/156869
Perrin F, Pernier J, Bertrand O, Echallier JF (1989) Spherical splines for scalp potential and current density mapping. Electroencephalogr Clin Neurophysiol 72:184–187
Pfurtscheller G, Stancák A Jr, Neuper C (1996) Event-related synchronization (ERS) in the alpha band—an electrophysiological correlate of cortical idling: a review. Int j psychophysiol 24:39–46
Plewnia C (2010) Brain stimulation: new vistas for the exploration and treatment of tinnitus. CNS Neurosci Ther 00:1–13. doi:10.1111/j.1755-5949.2010.00169.x
Romei V, Brodbeck V, Michel C et al (2008a) Spontaneous fluctuations in posterior alpha-band EEG activity reflect variability in excitability of human visual areas. Cereb cortex 18(9):2010–2018. doi:10.1093/cercor/bhm229
Romei V, Rihs T, Brodbeck V, Thut G (2008b) Resting electroencephalogram alpha-power over posterior sites indexes baseline visual cortex excitability. NeuroReport 19:203–208. doi:10.1097/WNR.0b013e3282f454c4
Schlee W, Müller N, Hartmann T et al (2009) Mapping cortical hubs in tinnitus. BMC Biol 7:80. doi:10.1186/1741-7007-7-80
Thut G, Veniero D, Romei V et al (2011) Rhythmic TMS causes local entrainment of natural oscillatory signatures. Curr Biol 21:1176–1185. doi:10.1016/j.cub.2011.05.049
Van Veen B, Van Drongelen W (1997) Localization of brain electrical activity via linearly constrained minimum variance spatial filtering. IEE Trans Biomed Eng 44(9):867–880
Vanneste S, Focquaert F, Van de Heyning P (2011) Different resting state brain activity and functional connectivity in patients who respond and not respond to bifrontal tDCS for tinnitus suppression. Exp Brain Res 210:217–227. doi:10.1007/s00221-011-2617-z
Weisz N, Moratti S, Meinzer M et al (2005) Tinnitus perception and distress is related to abnormal spontaneous brain activity as measured by magnetoencephalography. PLoS Medicine 2:e153. doi:10.1371/journal.pmed.0020153
Weisz N, Dohrmann K, Elbert T (2007a) The relevance of spontaneous activity for the coding of the tinnitus sensation. Prog Brain Res 166:61–70. doi:10.1016/S0079-6123(07)66006-3
Weisz N, Müller S, Schlee W et al (2007b) The neural code of auditory phantom perception. J Neurosci 27:1479. doi:10.1523/JNEUROSCI.3711-06.2007
Weisz N, Hartmann T, Müller N, Obleser J (2011) Alpha rhythms in audition: cognitive and clinical perspectives. Front Psychol. doi:10.3389/fpsyg.2011.00073
Zoefel B, Huster RJ, Herrmann CS (2011) Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage 54:1427–1431. doi:10.1016/j.neuroimage.2010.08.078
Acknowledgments
The authors wish to thank Daria Laptinskaya, Gabriela Salagean, Hadas Gorodetzky, Sylvie Roth and Christiane Wolf for their help in acquiring the data and Ken Gildner for language editing. This study was supported by the Tinnitus Research Initiative (Grant No: TE 06 02), the Deutsche Forschungsgemeinschaft (Grant No: WE 4156/2-1) and the Ministerium für Wissenschaft, Forschung und Kunst Baden-Württemberg (Grant No: 33-7532.20/627).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hartmann, T., Lorenz, I., Müller, N. et al. The Effects of Neurofeedback on Oscillatory Processes Related to Tinnitus. Brain Topogr 27, 149–157 (2014). https://doi.org/10.1007/s10548-013-0295-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10548-013-0295-9