
Abstract
The current study leveraged the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort (n = 4504 White boys, n = 4287 White girls assessed from the prenatal period through 18.5 years of age) to test a developmental cascade from genetic and prenatal substance use through pubertal timing and parenting to the severity of (regardless of type) and directionality (i.e., differentiation) of externalizing and internalizing problems to adolescent substance use. Limited associations of early pubertal timing with substance use outcomes were only observable via symptom directionality, differently for girls and boys. For boys, more severe exposure to prenatal substance use influenced adolescent substance use progression via differentiation towards relatively more pure externalizing problems, but in girls the associations were largely direct. Severity and especially directionality (i.e., differentiation towards relatively more pure externalizing problems) were key intermediaries in developmental cascades from parental harsh discipline with substance use progressions for girls and boys.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Key theories of the development of substance use highlight cascading biological and environmental influences that are both independently and jointly associated with later adolescent substance use (Dodge et al. 2009). These developmental cascades are likened to individual streams (e.g., particular influences, like genetics and prenatal exposures) that flow into each other and grow larger. Later, new streams (e.g., parenting environment) add to the growing rivers, and as the developmental influences come together and grow stronger, they gain momentum leading to outcomes (e.g., adolescent substance use) that seem unavoidable, at least near the end of the developmental cascade (Dodge et al. 2009; Masten et al. 2005). A feature of this theory is that the earliest influences are small, observable mainly through more proximal or intermediary influences and processes that involve both the child and their environment, whereas ‘downstream’ developmental influences have much stronger and seemingly less tractable associations with the developmental outcome.
Developmental cascades have been particularly important for understanding adolescent substance use, which is influenced by multiple factors often conceptualized as working together to increase risk via accumulating, dynamic processes (Dodge et al. 2009). The earliest influences on adolescent substance use include genetics (Hopfer et al. 2003) and prenatal risk (particularly substance use exposure; Irner 2012). Intermediary factors contributing to risk for adolescent substance use include parenting during childhood and adolescence (i.e., harsh discipline, low warmth, and low monitoring; Donaldson et al. 2016; Neiderhiser et al. 2013), peers during later childhood and adolescence (e.g., delinquency, substance use; Schelleman-Offermans et al. 2013) and pubertal timing (Marceau and Jackson 2017). The most proximal and strongest predictors of adolescent substance use are internalizing (Hussong et al. 2017) and especially externalizing problems during middle childhood and early adolescence (Hicks et al. 2011).
The present study used the Avon Longitudinal Study of Parents and Children (ALSPAC) to assess developmental cascades from polygenic risk and prenatal substance use through harsh discipline, pubertal onset, and externalizing and internalizing problems to late adolescent substance use outcomes (see Fig. 1, conceptual model). Examining these multiple influences together will elucidate how pubertal timing and parental harsh discipline operate within a larger developmental cascade, or highlight which factors emerge as particularly important in the context of a larger model of the development of substance use. Externalizing and internalizing problems in adolescence can be either positively correlated in the case of comorbidity, or negatively correlated in the case of differentiated problems within individuals. This phenomenon makes it difficult to understand the relative role of problem type vs. severity of comorbid problems in many studies. A novel contribution of this study is our conceptualization of externalizing and internalizing problems using a severity–directionality model (Essex et al. 2003). This model provides a unique and important within-person perspective on comorbidity by reorganizing externalizing and internalizing problems into a score reflecting the severity of comorbid problems, which is measured orthogonally to a second score reflecting the differentiation or specificity of problem type as predominantly externalizing or internalizing. The severity–directionality model of externalizing and internalizing symptoms is expected to clarify the role of behavioral problems in developmental cascades to adolescent substance use.

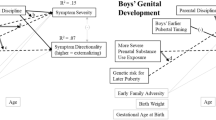
Conceptual model. System severity and directionality are orthogonal constructs. Ext > Int denotes a preponderance of externalizing problems rather than internalizing problems. Int > Ext denotes a preponderance of internalizing rather than externalizing problems. (+) Indicates hypothesized positive correlations (e.g., a risk factor). (−) Indicates hypothesized inverse associations (e.g., a protective factor). Hashed lines denote correlations among predictor that are present in families where the same parents provide genetic, prental and parenting influences, as in the present study
Pubertal timing and substance use
Puberty unfolds during late childhood/early adolescence and encompasses sex-specific hormone changes and visible changes in secondary sex characteristics (e.g., females: breasts, males: facial hair) that are driven by sex-specific biology (Grumbach and Styne 2003). There is strong evidence that in females, starting puberty earlier is linked to more externalizing and especially internalizing problems (Ullsperger and Nikolas 2017), as well as increased adolescent substance use (Marceau et al. 2015a). In the ALSPAC cohort, girls’ earlier pubertal timing has been linked to alcohol and cannabis use (but not smoking; Hummel 2014). These findings are primarily explained by the developmental readiness hypothesis, stating that youth who go through puberty early are not cognitively or emotionally prepared for the biological and social changes associated with the physical maturation of puberty, which increases risk for maladjustment (Ge and Natsuaki 2009). Early pubertal onset is thought to influence adolescent substance use through biological mechanisms (i.e., hormone changes) and by socially-driven mechanisms (e.g., shifting responsibilities and relationships at home; associating with older peers; Mendle et al. 2007).
For males, both earlier and later pubertal timing have been related to externalizing problems as well as earlier and faster progressions though a variety of substance use milestones (Mendle and Ferrero 2012). The social compensation hypothesis suggests that some boys who are, or who perceive themselves to be, less physically mature due to delayed pubertal onset may engage in more risky behaviors (e.g., substance use) to ‘prove’ their maturity despite their more juvenile appearance (Marceau et al. 2015a). This mechanism is likely to be environmentally mediated, given evidence later puberty is more often associated with substance use outcomes in boys when assessed via visual cues (i.e., self-report or secondary sex characteristics). This is in contrast to measures of hormone levels or changes, which tend to show effects of earlier maturation on substance use involvement (Marceau et al. 2019a). The measure of puberty used in ALSPAC is parent- and youth-reported ratings of secondary sex characteristics, and thus profiles of pubertal risk for late adolescent substance use are expected to be earlier onset for girls but later onset for boys. Finally, based on recent findings suggesting that earlier externalizing and internalizing problems do not predict the timing of puberty (Beltz et al. 2020; Deardorff et al. 2021), pubertal timing is placed before internalizing and externalizing problems in the present developmental cascade (Fig. 1).
Initiation of the proposed developmental cascade
Pubertal timing is genetically influenced (Day et al. 2017), and associated with key prenatal insults, specifically substance use during pregnancy (Irner 2012; Maisonet et al. 2010). Twin studies have found genetic influences common to pubertal timing and adolescent substance use in girls (Corley et al. 2015), and externalizing problems in one study (Vaughan et al. 2015) but not in others (e.g., Dick et al. 2000; Eriksson et al. 2005). However, twin studies (Marceau et al. 2012) and LD regression studies (Zheng et al. 2017) have found that genetic influences on pubertal maturation are largely non-overlapping with those on internalizing phenotypes. Two recent studies found that pubertal timing did not mediate the association of family history of substance use with adolescent substance use (Marceau et al. 2019a; Weigard et al. 2020). These findings suggest that genetic risk for substance use is unlikely to initiate developmental cascades involving pubertal timing (e.g., in contrast to Corley et al. 2015, which was a bivariate twin model first estimating genetic influences on pubertal timing). Further, in the ALSPAC cohort, timing of girls’ breast development partially mediated associations of polygenic risk for early pubertal timing and self-reported depressive symptoms at age 16.5 years (Horvath et al. 2020). Thus, available evidence points to genetic risk for earlier pubertal timing specifically as a potential initiator of developmental cascades involving pubertal timing. We extend this work to explore whether substance use during pregnancy is also a potential initiator of developmental cascades involving pubertal timing. Our manuscript uses the same measure of genetic risk as presented in Horvath et al. (2020), but embedded in a larger developmental model (with prenatal risk and parenting), including a different construct for child behavior (severity and directionality) that is parent-reported, a different quantification of pubertal timing, and extending out to youth-reported substance use.
Intermediary influences in the proposed developmental cascade
Parental harsh discipline
Parental harsh discipline has emerged as a key, intermediary predictor of externalizing problems and adolescent substance use (Brenner and Fox 1998; Riggins-Caspers et al. 2003). Even in the context of developmental cascades including genetic and prenatal risks and stress biology, adoptive parents’ harsh discipline has emerged as a key influence predicting more externalizing and internalizing problems in childhood (Marceau et al. 2015b). There is empirical support of associations of physical discipline with later adolescent externalizing and internalizing problems in studies of biologically-related families that were stronger than other parenting measures (e.g., Bender et al. 2007). Although there is evidence of reciprocal relations (e.g., Lansford et al. 2011) as well as evocative gene–environment correlation processes (Button et al. 2008) underlying associations of parents’ discipline and child behavior problems, harsh discipline goes beyond contingent responsivity. Indeed, harsh discipline is considered an ineffective strategy that is a key feature of coercive cycles whereby youths’ externalizing behaviors elicit ineffective punishment from parents, which backfires and instead leads to worse externalizing problems repeatedly over time (Patterson 1982). Our focus is on this latter pathway, of harsh discipline predicting later problems, although we acknowledge that the associations likely arise due to prior transactional, evocative processes. Thus, based on a large body of work, parental harsh discipline is expected to play a key role in developmental cascades to adolescent substance use (Dodge et al. 2009) primarily through more proximal associations with adolescent externalizing (Bailey et al. 2009) and, to a lesser extent, internalizing problems (Rose et al. 2018). Additionally, by including a measure of harsh discipline in the developmental cascade from genetic influences on puberty through pubertal onset to transitions to substance use, we may identify whether puberty-related genes represent a specific gene–environment correlation in this process.
Externalizing and internalizing problems
One of the strongest predictors of adolescent substance use is earlier behavior problems (Colder et al. 2013; Lansford et al. 2008). Externalizing problems are more often associated with substance use, but internalizing problems are as well (Hussong et al. 2017). Further, there is evidence supporting developmental cascades such that internalizing and especially externalizing problems mediate links from genetic and environmental (e.g., parenting) risk factors for adolescent alcohol, cigarette, and marijuana use (Marceau et al. 2020a; Trucco et al. 2016, 2018; Weymouth et al. 2019). Although the role of externalizing problems is clear and robust, the role of internalizing problems is less clear, and may be substance-specific or model-dependent (Marceau et al. 2020a; Trucco et al. 2018). A test of competing hypotheses for the developmental influence of internalizing problems on adolescent alcohol use suggested that internalizing symptoms that co-occur with externalizing problems put children at higher risk for alcohol use than chronically elevated “pure” internalizing problems (Scalco et al. 2020). This finding is consistent with the idea that the common etiology shared between externalizing and internalizing (Marceau and Neiderhiser 2020; Rhee et al. 2015) may drive positive associations between internalizing problems and substance use during adolescence. Findings of protective effects of internalizing problems for some forms of substance use (including in the ALSPAC cohort for early adolescent alcohol use; Edwards et al. 2014) may reflect the effect of specific, “pure” internalizing problems: for example, anxiety-related behaviors could lead to reduced involvement with substance-using peers (Colder et al. 2013). Novel approaches to understanding the role of internalizing problems in developmental models and in relation to externalizing problems are needed to extend this literature. One such novel approach is to leverage the severity–directionality model of comorbid internalizing and externalizing problems (Essex et al. 2003).
Severity and directionality
In the severity-directional model, the dimension of symptom severity reflects the severity of total problems (Marceau and Neiderhiser 2020). To achieve very high severity, youth must have both types of problems, and so high symptom severity can be thought of as a measure of the within-person comorbidity of externalizing and internalizing problems. Symptom directionality is an orthogonal dimension, indicating the preponderance of symptoms on a scale from pure internalizing (i.e., more negative values) to pure externalizing (i.e., more positive values). Scores near zero on this dimension reflect balanced or comorbid externalizing and internalizing problems, regardless of severity of symptoms (if any symptoms are present) or a lack of either (if no symptoms are present).
A recent twin study found that both severity and directionality of externalizing and internalizing problems were highly heritable (~ 60–65%; Marceau and Neiderhiser 2020). Identified predictors of symptom severity include familial factors (i.e., early life stress, family conflict/resolution; Essex et al. 2011; Marceau et al. 2015c; Neiderhiser et al. 2016) likely reflecting both genetic and shared environmental influences. However, there is some evidence that the prenatal environment may be particularly important for the directionality of problems experienced in childhood and early adolescence. In an adopted-at-birth design, exposure to obstetric complications in the context of genetic risk for substance use predicted a preponderance of internalizing problems at 4.5 years (Neiderhiser et al. 2016) whereas smoking during pregnancy predicted a preponderance of externalizing problems in 7–16 year olds in a sibling comparison study of maternal smoking during pregnancy (Ekblad et al. 2020). To date, no studies have examined whether severity or directionality of symptoms predict adolescent substance use, or whether severity or directionality plays a role in developmental pathways to adolescent substance use. Based on the studies of transitions to substance use reviewed above, we expect that symptom severity (regardless of type) would predict increased adolescent substance use, and that directionality would independently predict substance use such that a preponderance of internalizing problems would be protective, but a preponderance of externalizing problems would be risky for adolescent substance use.
Present study
The present study uses data from the Avon Longitudinal Study of Parents and Children (ALSPAC), a large cohort of youth followed beginning in the prenatal period and assessed through late adolescence, in order to test a novel developmental cascade from genetic and prenatal substance use through pubertal timing and parenting to behavioral risk and subsequently adolescent substance use. A key novel contribution of this study is our attention to early developmental influences, particularly genetic risk for early pubertal timing and prenatal risks. A second novel contribution of this study is that we leverage the severity–directionality model of comorbidity to shed a new and complementary light on the literature examining the unique and overlapping roles of internalizing and externalizing problems on the development of substance use. We examine alcohol, cigarette, and cannabis use progression (e.g., status along a series of use milestones for each of these three substances that are commonly used during late adolescence) in order to explore whether the developmental pathways assessed here are substance-specific or general. Finally, as is standard in studies of puberty, we examine boys and girls separately because of qualitative differences in the underlying biology, physical manifestations, and timing of puberty across sexes, and because of established sex differences in the robustness and direction of associations of pubertal timing and substance use.
Hypotheses
Several general predictions emerge from our conceptual model (Fig. 1). We expect that genetic risk for pubertal timing will predict pubertal onset. We expect that prenatal substance use exposure will predict earlier pubertal onset, increased symptom severity and directionality (specifically a preponderance of externalizing problems following Ekblad et al. 2020), and increased substance use progression. We expect parents’ harsh discipline will predict higher symptom severity based on findings from studies showing that familial factors predict severity but not directionality (e.g., Marceau et al. 2015c; Neiderhiser et al. 2016) and more speculatively, substance use. We expect that earlier pubertal onset will predict higher externalizing/internalizing symptom severity, directionality (a preponderance of internalizing problems) and substance use progression in girls, but that later pubertal onset will predict higher symptom severity, symptom directionality (a preponderance of externalizing problems) and substance use progression in boys. Finally, we hypothesize that both symptom severity and directionality (specifically a preponderance for externalizing problems) will predict more substance use progression. We expect that youth with directionality scores indicating a strong preponderance of internalizing problems will have particularly low rates of substance use. We expect to find indirect effects across these influences in line with Fig. 1, supporting developmental cascades.
Method
Participants
The current study used data from the ALSPAC (Boyd et al. 2013; Fraser et al. 2013). Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time. Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. The initial ALSPAC cohort included 14,541 pregnancies with expected delivery dates between April 1st, 1991 and December 31st, 1992; of these, 13,988 children were alive at 12 months. This cohort was bolstered when the children reached 7 years of age, resulting in 913 additional children (although these children were missing for prenatal risk). In the total ALSPAC sample (the initial sample plus 913 children from the age 7 bolster), there are data available for 15,589 fetuses (14,901 alive at 1 year of age). Of these children, 96% were White. The analytic sample for the current study was restricted to youth from the total sample who were of European ancestry and had both genetic data and any phenotypic data (n = 8791). Phenotypic data included prenatal substance use data, data on pubertal timing, parent discipline at age 9.5 or 11.5 years, internalizing and externalizing problems at age 13 years, substance use at 18.5 years, and covariates (i.e., birth weight, gestational age, and family adversity at 2–4 years of age, sex, and age at the age 13 and 18.5 year assessments). Missing data patterns are presented after the measures. The study website contains details of all the data that is available through a fully searchable data dictionary and variable search tool: http://www.bristol.ac.uk/alspac/researchers/our-data/. Analysis of these data was also approved by the Purdue University Institutional Review Board.
Measures
Polygenic risk for later pubertal timing
A total of 9912 children were genotyped using the Illumina HumanHap550 quad genome-wide SNP genotyping platform, generated by Sample Logistics and Genotyping Facilities at Wellcome Sanger Institute and LabCorp (Laboratory Corporation of America) using support from 23andMe. Data were imputed to 1000 genomes phase 1 version 3 using the Impute2 software (see ALSPAC documentation for further details). Standard quality control was conducted on the genome-wide SNP data using Plink (Purcell et al. 2007); we excluded samples with sex mismatch, call rate < 95%, unexpected first-degree relatedness, too much or too little heterozygosity, and non-European ancestry. This resulted in a total n of 8952 individuals with genetic data.
The polygenic risk score (PRS) was calculated using summary statistics from the largest available GWAS on age at menarche to date: Day et al. (2017) which included data collected from women in 40 studies from the ReproGen consortium, 23AndMe, and Biobank studies (N = 328,345). This sample did include ALSPAC (~ 3% of the sample), however, prior work found that this inclusion of ALSPAC data did not overly inflate effects of the PRS based on sensitivity analyses using weights from the Day et al. (2017) replication sample (deCODE; N = 39,543 women; Horvath et al. 2020). Day et al. (2017) identified 389 SNPs and corresponding effect weights associated with age at menarche at the genome-wide level (p < 5e−8) with available summary statistics. Of those, 372 were included in ALSPAC, and 337 remained after quality control (e.g., minor allele frequency < 0.01, missingness per marker > 0.01). All 337 SNPs showed adequate genotyping and Hardy–Weinberg equilibrium. There was no evidence of linkage disequilibrium (> 0.3) among these 337 SNPs. Thus, the PRS was calculated by summing (across SNPs for each individual) the product of the effect of each included SNP as identified by Day et al. (2017) and the number of effect alleles present for each individual (Maier et al. 2018). These scores were created and used previously (Horvath et al. 2020). Notably, Day et al. (2017) also provided summary statistics for age at voice break in boys. Here, we used only the PRS for age at menarche, as Horvath et al. (2020) showed that this score better predicted pubertal timing (estimated age at Tanner Stage 3 from growth models) for both boys and girls than the corresponding PRS for males’ age at voice break.
Prenatal substance use
Mothers were assessed twice during pregnancy: (i) prior to 18 weeks gestation, and (ii) around 32 weeks gestation. In the first questionnaire, mothers reported on the number of cigarettes per day they smoked “at the moment”, as well as how many drinks of beer or lager (half-pints), wine (glasses), spirits (pub-measures), and other alcohol drinks (pub-measures) on week days and weekend days. The ALSPAC team created a variable for total weekly alcohol consumption by summing the responses on these alcohol measures. In the second assessment, women reported on the number of cigarettes smoked per day, binned into 0 cigarettes = 0, 1–4 cigarettes = 1, 5–9 cigarettes = 5, 10–14 cigarettes = 14, 15–19 cigarettes = 15, 20–24 cigarettes = 20, 25–29 cigarettes = 25, and 30+ cigarettes = 30 in the first 3 months of pregnancy (e.g., 1st trimester), and in the past 2 weeks (e.g., 3rd trimester). Women reported on how often they drank alcohol drinks (never, < 1 glass/week, at least 1 glass/week, 1–2 glasses every day, at least 3–9 glasses every day, or at least 10 glasses) “in the first three months of this pregnancy” (e.g., 1st trimester), as well as “around the time you first felt the baby move” (typically during the 2nd trimester) with instructions to report on the past 2 weeks if she had not yet felt the baby move. Women also reported on the frequency with which they smoked cannabis (everyday, 2–4 times/week, once/week, < once/week, not at all) “in the first three months of this pregnancy” and “between then and now”. Finally, women also reported on amphetamine, barbiturate, crack, cocaine, heroin, methadone, ecstasy, and other drug use “during this pregnancy” on a scale including the following options: nearly every day, once+ per week, once+ per month, or not at all.
Because we were interested in substance use that could potentially harm the fetus, and because the metrics and number of assessments for each substance differed, we used the McNeil–Sjöstrom scale to create a weighted risk total score (McNeil et al. 1994). Specifically, this scale assigns risks values (1 = Not harmful or relevant; 2 = Not likely harmful or relevant; 3 = Potentially but not clearly harmful or relevant; 4 = Potentially clearly harmful or relevant; 5 = Potentially clearly greatly harmful/relevant; 6 = Very great harm to or deviation in offspring). For substance use during pregnancy these scores are based on both the substance used and frequency of use (see “Appendix” Part A, and Marceau et al. 2016 for details). Because some more commonly used substances were reported multiple times during pregnancy, while other more harmful substances were reported only about the whole pregnancy, we aggregated the repeated measures by taking the maximum score across assessments (e.g., for alcohol, smoking, and cannabis). The weighted severity score is the sum of the weighted scores for each individual substance across pregnancy, representing the severity of risk to the fetus of cumulative poly-substance use exposure.
Parental harsh discipline
Parents’ harsh discipline was measured at the 9.5 and 11.5 year assessments via parent report with the two items from the Discipline and Lifestyle questionnaire “How often is he/she punished?” and “How often do you slap or hit him/her?”. Each item was scored as follows: 0 = never, 1 = rarely, 2 = once or twice a month, 3 = once or twice a week, 4 = several times a week, 5 = every day. Items were averaged first within-assessment, but because of high correlations of the scales across assessments, r = 0.64, and better reliability of a four-item scale than a two-item scale, we averaged all four items into a single discipline item reflecting late childhood (age 9.5 and 11.5 years).Footnote 1 Items were correlated r = 0.31–0.57 within and across assessments, Cronbach’s α = 0.73.
Pubertal timing
Pubertal maturation was assessed via Tanner Stage line drawings (Morris and Udry 1980) 9 times (approximately yearly) from age 8 to 17 years. Raters could be parent only, child only, parent and child, “other” only, parent and other, child and other, or parent, child and other, and varied across assessments; most typically parents and children worked together in the early years, and children reported alone in the later years. Samples sizes by reporter and stage at every wave have been previously reported in the Supplemental Materials of Horvath et al. (2020). We operationalized pubertal timing as the age at the assessment in which Tanner Stage 2 was achieved from the repeated measures.
First, we located the first assessment at which Tanner Stage 2 was endorsed and coded the age at that assessment as our indicator of pubertal onset. Then, data cleaning (detailed in “Appendix” Part B) included removing individuals who never reached Tanner Stage 2 in the observed data and did not have data past the 6th wave. If there were data after wave 6, we top-coded so that they received an age at Tanner Stage 2 one year after their last observed assessment of Tanner Stage 1 in order to include them as relatively later pubertal timing (1–8 individuals across phenotypes). As is common in longitudinal puberty data, there were significant reports of regression (see “Appendix” Part B). If individuals regressed back to Tanner Stage 2, or regressed back to Tanner Stage 1 and subsequently reached Tanner Stage 2 again, we used the age at the second instance of reaching Tanner Stage 2. That is, we assumed the second instance was more accurate, based on data showing that younger children are less accurate reporters than older children since they are not aware of the changes yet to come and tend to over-estimate their stage (Shirtcliff et al. 2009). This was a particularly large problem for boys’ genital development (see “Appendix” Part B). If an individual regressed back to Tanner Stage 1 and never attained Tanner Stage 2, we removed the cases (n = 7–46 across phenotypes) because this pattern is not consistent with the biology of pubertal development and thus more likely to reflect measurement error. Finally, we removed individuals who had a missing assessment prior to reporting reaching Tanner Stage 2 (i.e., stage 1 at wave 1, a missing assessment, and stage 3 at wave 3), since differences of a year in age for attaining Tanner Stage 2 in the middle of the assessment period could have ramifications for rank order in the sample and therefore bias results. The exception was for if youth were only missing the first assessment and reported Tanner Stage 2 at the second assessment. n’s affected at each stage of cleaning for each of the four phenotypes are presented in “Appendix” Part B. The sample sizes with data judged to be of reasonable quality for age at Tanner Stage 2 were: girls’ breast development n = 3521; girls’ pubic hair development n = 3121; boys’ genital development n = 3300; boys’ pubic hair development n = 2573.
Externalizing and internalizing problems
Parents rated youths’ externalizing and internalizing problems in the last 6 months during mid-adolescence, at the age 13-year assessment. Externalizing problems were operationalized as the average of the hyperactivity (5 items, i.e., restless, distracted) and conduct problems (5 items, i.e., tantrums, fights) subscales of the Strengths and Difficulties Questionnaire (Goodman 1997; Goodman et al. 1998), and internalizing problems were operationalized as the emotional problems subscale (5 items, i.e., worries, unhappiness) of the same questionnaire. Following prior work (Marceau et al. 2015c; Marceau and Neiderhiser 2020), the externalizing and internalizing scores were simultaneously entered into a principal component analysis (PCA) and exactly two (orthogonal) factor scores were extracted and saved. The first score reflects severity, or what the scores have in common, and the second directionality—what differentiates the scores coded such that more positive scores indicate a preponderance of externalizing problems and more negative scores indicate a preponderance of internalizing problems. Findings from the PCA showed that severity accounted for 68% of the variance in externalizing and internalizing problems. As expected, externalizing and internalizing both loaded strongly on the severity factor (0.61). Externalizing problems loaded strongly and positively (0.88) on the directionality factor, and internalizing problems loaded equally and negatively on the directionality factor (− 0.88). Further details aiding in interpretation of severity and directionality (e.g., correlations with externalizing and internalizing) are presenting in “Appendix” Part C.
Substance use progression
Several substance use indicators were self-reported by adolescents at age 18.5 years. ALSPAC included items on the quantity and frequency of alcohol, cigarette, and cannabis use, as well as the Alcohol Use Disorders Identification Test (AUDIT; Saunders et al. 1993) and the Cannabis Abuse Screening Test (CAST; Legleye et al. 2007). From the available data, we created measures of substance use progression that assess how far along a continuum or progression of use milestones adolescents are at a particular assessment (Marceau et al. 2020b). For each of these measures, youth were coded into the highest category that they endorsed. See Table 1 for categories with N’s.
Covariates
We included birth weight and gestational age (the best estimate according to ALSPAC from multiple informants). We also included family adversity in early childhood (age 2–4 years) as a covariate. Family adversity was measured by the Family Adversity Index (short version), a sum score of binary indicators for (adversity absent = 0 vs. present = 1) early parenthood/pregnancy, housing: inadequacy, hosing does not meet basic living needs, housing defects/infestation, low education of mother and partner, financial difficulty, single parenthood (lack of partner), no partner affection, partner cruelty, large family size, major family problems, psychopathology of mother, drug and alcohol use of mother, mothers’ trouble with police, and mothers’ criminal convictions (see Bowen et al. 2005 for details).
Missing data
Compared to the full sample of 14,701 children alive at 1 year of age, our analytic sample—which included youth with genetic data and any of the measured phenotypic data—included 8791 (60%). Our analytic sample was more likely to have adequate housing, better education, and less financial difficulties (statistics available upon request). Despite p-values < 0.0001, these effects were relatively small (Cramer’s V < 0.13). Within our analytic sample, 25% were missing data on pubertal onset, 14% were missing data on parental harsh discipline, 38% were missing data on severity and directionality, and 70% were missing data on substance use. Compared to the full analytic sample, attrition was related to lower socioeconomic indicators, and being male (statistics available upon request). We also used a series of Kruskal–Wallis one-way analysis of variance tests to determine whether scores on the key study variables were related to missingness on other key study variables. Families that provided data on parental harsh discipline had youth with slightly later age at pubertal onset (except boys’ pubic hair) and lower severity, but no difference in directionality of externalizing and internalizing problems or substance use outcomes. Youth with puberty data had slightly lower severity of problems but no difference in directionality or substance use outcomes. Missingness on severity/directionality of externalizing and internalizing symptoms did not predict substance use outcomes. The overall pattern of findings suggests that the model is somewhat biased towards later pubertal timing and less severe problem behavior, which may lead to smaller associations among these constructs, and limited generalizability in processes for youth with particularly early puberty and severe problems. Despite these patterns of missing data, the sample was large for each construct, and missing data was accommodated using Full Information Maximum Likelihood in the models described below.
Analytic strategy
Hypotheses were tested using path analysis conducted in R(lavaan) (Rosseel 2012) using the se = “bootstrap” command to accommodate the skewed nature of the outcome data and to reduce bias in the p-values for the indirect effects. The models are based on n = 4504 boys and n = 4287 girls. Separate models were run for each pubertal onset phenotype (1 Girls’ breast development; 2 Girls’ pubic hair development; 3 Boys’ genital development; 4 Boys’ pubic hair development). Models included the paths shown in Fig. 1, but also included age at the 13-year assessment as a predictor of severity and directionality, age at the 18.5-year assessment as a predictor of the substance use outcomes, as well as family adversity, birth weight, and gestational age as predictors of or associated with all main study variables. Hypotheses were tested via the presence or absence of hypothesized pathways at p < 0.05. There were 70 direct paths estimated in each model, although 59 were identical across models 1 and 2 (with 11 unique paths in each—those involving the pubertal timing variable which differed across models), and 59 identical across models 3 and 4 (again with 11 unique paths that included a pubertal timing variable and thus differed across models). A Bonferroni adjustment for 162 unique tests yields p < 0.0003. We also tested for indirect effects from genetic and prenatal substance use through pubertal onset to severity, directionality, and substance use outcomes, and from prenatal substance use, pubertal onset and parental harsh discipline through severity and directionality to substance use outcomes. Because of the complexity of models and hypotheses, we interpret findings holistically, weighing information based on nominal and Bonferroni-adjusted p-values, effect size (e.g., correlation coefficients, standardized estimates), consistency with zero-order correlations, and consistency across models.
Results
Frequencies for late adolescent substance use progression categories are presented in Table 1. The majority of girls and boys had progressed at least to binge drinking (6+ in a day) in late adolescence, with nearly half showing signs of hazardous drinking or likely dependence. About half of girls and boys never smoked cigarettes. Whereas about 35 to 40% of youth were in the low stages of progression (ever smoked or recently smoked), only ~ 10% smoked daily or heavily daily. About two-thirds of girls and boys never used cannabis, with the majority of users in the initial stages of progression: only having tried cannabis. About 10% of the sample used cannabis recently, on a monthly basis, or showed signs of dependence.
Descriptive statistics for the other study variables are presented in Table 2. 20% of girls and 22% of boys were exposed to substance use during pregnancy that constituted at least a potential risk to the fetus. For parents’ discipline, observed values matched the possible range from 0 to 5, but low average levels for girls (0.97) and boys (1.16) indicated that on average this sample experienced low levels of harsh discipline. Average age at breast development onset was earlier than pubic hair onset for girls, as expected (Grumbach and Styne 2003). Girls’ average age at pubic hair onset was earlier than boys’, as expected (Grumbach and Styne 2003). However, average age at genital development onset was earlier than average age at breast development onset, reflecting that boys’ perceptions of genital development onset are particularly biased (e.g., reported as earlier than probably true).
Hypothesis testing
Bivariate correlations are presented in Table 3. Generally, findings in the hypothesis-testing model matched what was observed in the bivariate correlations. We note any instances of differing results in the text below. All models fit the data well (see Figs. 2, 3). Figure 2 presents the findings from direct and indirect path estimates across the two models for girls: including (1) breast development and (2) pubic hair development. Figure 3 presents the findings from direct and indirect paths estimated across the two models for boys: including (3) genital development and (4) pubic hair development. Standardized parameter estimates and p-values for key direct effects (excluding covariate effects) are presented in Table 4, and indirect effects are presented in Table 5. Full model results including unstandardized parameter estimates, standard errors and confidence intervals and covariate effects are provided in Supplemental Tables S1 (breast development) and S2 (pubic hair development) for girls, and Tables S3 (genital development) and S4 (pubic hair development) for boys. In the text below, if effects are specified as ‘nominal’ in the text below, this indicates p < 0.05 but not p < 0.0003. Effects presented without the qualifier of ‘nominal’ survived Bonferroni adjustment (p < 0.0003).

Model results: girls. BD indicates breast development. PH indicates pubic hair development. Any statistics not represented with BD or PH applied to both models. All paths are positive associations unless noted with (−) to indicate an inverse association. Hashed lines denote association significant at p < 0.05, bold lines denote association significant at p < 0.0003 (adjusted for multiple testing). Gray lines are covariate effects

Model results: boys. GD indicates genital development. PH indicates pubic hair development. Any statistics not represented with GD or PH applied to both models. All paths are positive associations unless noted with (−) to indicate an inverse association. Hashed lines denote association significant at p < 0.05, bold lines denote association significant at p < 0.0003 (adjusted for multiple testing). Gray lines are covariate effects
Girls
Genetic risk for later pubertal timing predicted later timing of both breast and pubic hair development onset, as expected. Genetic risk was not directly related to prenatal substance use, harsh discipline, externalizing/internalizing symptom severity and directionality, and substance use outcomes. Prenatal substance use exposure did not predict pubertal timing in either model. Prenatal substance use exposure was not directly related to parental discipline, externalizing/internalizing symptom severity, or directionality. More severe prenatal substance use had direct effects on increased cannabis and smoking use, and a nominal direct effect on increased alcohol use.
Parental harsh discipline predicted higher symptom severity as well as a preponderance of externalizing problems. A modest bivariate correlation of earlier age at breast development onset with more severe problems did not persist in the context of the model, likely due to shared variance with parental harsh discipline (as earlier onset of breast but not pubic hair development was nominally associated with more harsh discipline). Earlier pubertal onset of pubic hair (but not breast) development nominally predicted directionality in the hypothesized direction (a preponderance for internalizing problems) but not severity. There was also a nominal indirect effect of genetic risk for pubertal timing via the timing of pubic hair onset to symptom directionality. Probes of these relations (“Appendix” Part C) suggest that this effect is best interpreted such that genetic risk for early puberty indirectly predicted a preponderance of internalizing problems via earlier pubic hair development onset.
Higher symptom severity was related to more smoking, and nominally to more cannabis use, but not to alcohol use progression. Symptom directionality, specifically a preponderance of externalizing problems, was related to more smoking and cannabis use, and nominally to more alcohol use. The modest bivariate correlations of more late adolescent smoking with both earlier age at breast development onset and parental harsh discipline did not persist in the context of the model. Pubertal onset was not directly associated with substance use outcomes. Harsh discipline was nominally related to more cannabis use, but not to alcohol use or smoking. Thus, shared variance between girls’ breast development and parental discipline noted above likely explain the null findings of breast development, whereas the association of harsh discipline may have been mediated by symptom severity and directionality.
Indeed, there were indirect effects from more parental harsh discipline via both having more severe problems and having relatively more pure externalizing problems (directionality) to more smoking. There were also nominal indirect effects from more parental harsh discipline via more severe and more pure externalizing (directionality) problems to more cannabis use. There was a nominal indirect effect from more parental harsh discipline via relatively more pure externalizing problems (directionality, but not severity of problems) to more alcohol use. Further, there were nominal indirect effects from earlier timing of pubic hair development to a preponderance of internalizing problems to more smoking, and alcohol and cannabis use. Probes of these relations (“Appendix” Part C) suggest that these effects are best interpreted such that girls with earlier timing of pubic hair onset are at increased risk for internalizing problems which then exert a protective effect against alcohol use. However, for cannabis and smoking, the evidence (“Appendix” Part C) is more consistent with an interpretation such that girls with relatively later timing of puberty were somewhat more likely to have more externalizing-type problems, which put them at particular risk of more cannabis use and smoking.
Boys
For boys, genetic risk for later pubertal timing predicted pubic hair development onset, but not genital development onset. Genetic risk was not directly related to prenatal substance use exposure, harsh discipline, externalizing/internalizing symptom severity and directionality, and substance use outcomes. Prenatal substance use exposure nominally predicted earlier timing of genital but not pubic hair development onset. Prenatal substance use exposure predicted a preponderance of externalizing symptoms (directionality, but not severity of problems), but was not directly related to parental discipline or substance use outcomes. That is, the moderate bivariate correlation of more severe prenatal substance use exposure and more smoking did not persist in the context of the model, suggesting that the association was fully mediated by symptom directionality. Indeed, there were nominal indirect effects from more prenatal substance use exposure via directionality (differentiation towards exhibiting specifically externalizing problems) to more smoking as well as to alcohol and cannabis use.
Parental harsh discipline predicted higher symptom severity as well as a preponderance of externalizing problems (directionality). Pubertal onset was unrelated to symptom severity in either model. A modest bivariate correlation of earlier age at pubic hair development onset with a preponderance of externalizing problems did not persist in the full model, likely due to shared variance with the early life family adversity covariate. Onset of genital development did nominally predict directionality, although not entirely as expected: genital development onset predicted problem type differentiation such that later genital development was related to experiencing more internalizing problems and earlier genital development was related to experiencing more externalizing problems (“Appendix” Part C).
Higher symptom severity was nominally related to more smoking and cannabis use, but not to alcohol use progression. Symptom directionality, specifically a preponderance of externalizing problems, was related to more smoking and nominally to more alcohol and cannabis use. Neither harsh discipline nor pubertal onset was directly associated with substance use outcomes. However, there were nominal indirect effects from genital development onset via directionality to smoking and cannabis use. Probes of these relations (“Appendix” Part C) revealed that the best interpretation of these indirect effects was that earlier genital development was indirectly associated with progression to more advanced stages of smoking and cannabis use via differentiation towards exhibiting more externalizing problems. Further, the modest bivariate correlation between parental harsh discipline and smoking did not persist in the context of the model, suggesting that the association was fully mediated by symptom severity and directionality. Specifically, there was an indirect effect from more parental harsh discipline via a preponderance of externalizing problems to more smoking. There were also nominal indirect effects from more parental harsh discipline via a preponderance of externalizing problems to more alcohol and cannabis use, as well as from more parental harsh discipline via higher symptom severity to more smoking and cannabis use.
Discussion
The present study leveraged the Avon Longitudinal Study of Parents and Children (ALSPAC) to test for developmental cascades associated with the progression of alcohol, smoking, and cannabis use in late adolescence, consistent with current theories of the development of adolescent substance use (Dodge et al. 2009). Specifically, we modeled developmental cascades that included biological and putatively environmental influences beginning with polygenic influences related to pubertal timing and severity of exposure to prenatal substance use, and including intermediary influences of parental harsh discipline and the timing of pubertal onset on transitions from novel features of proximal behavioral risk for substance use (severity and directionality of mid-adolescent externalizing and internalizing problems) with later adolescent substance use progressions. We found robust evidence of developmental cascades involving the severity and directionality of externalizing and internalizing problems as intermediaries between associations of parental harsh discipline with substance use progressions for girls and boys. We also found evidence for some sex-specific cascades of pubertal timing and (for boys only) exposure to prenatal substance use via symptom directionality to late adolescent substance use.
Initiation of developmental cascades
Genetic influences
We provide some support to emerging evidence that genetic risk for early puberty may initiate developmental cascades for girls, indirectly influencing differentiation towards internalizing problems via earlier pubertal onset. For example, in the same sample (using a different measure of pubertal timing), Horvath et al. (2020) found an indirect effect from the same polygenic score via age at the midpoint of breast development (as opposed to at the initiation of pubic hair development found here) to later adolescent depressive symptoms—and no indirect effects in boys. It is unclear why pubic hair onset was a stronger predictor in this study than the more visible changes related to breast development onset. Reported breast development without areolar staging is more biased in youth with more adipose tissue, as fat can be mistaken for breast development (Dorn et al. 2006). Speculatively, if hormone changes do underlie the association of genetic influences of puberty-related genes with differentiation toward internalizing symptoms, this association may be clearer for pubic hair development because self- and parent- reports of pubic hair development could contain less of this over-estimate of early stages of puberty found for breast development. Or, adrenal hormones (contributing to the development of pubic hair) may be more important than gonadal hormones (contributing to breast development) for problem differentiation in girls. It will be critical to replicate this indirect effect from puberty-related genes to differentiation towards internalizing problems in other samples with other measures of puberty and that include hormone ascertainment in order to understand when and why different pubertal phenotypes mark this potential genetic influence. However, in the context of the larger developmental cascades, wherein differentiation towards externalizing problems played a much more prominent role, the sparse findings with regard to genetic risk for pubertal timing and downstream correlates of pubertal timing indicate that genetic risk related to pubertal timing is not a critical initiator of developmental cascades to substance use progressions in late adolescence.
Prenatal substance use exposure
In contrast, our findings suggest that severity of prenatal substance use exposure may be a key differentiating influence that pushes boys towards externalizing problems in particular. This is consistent with recent findings from a sibling-comparison design (that examined boys and girls together) wherein the sibling whose mother smoked (or smoked more) during pregnancy had a greater preponderance of externalizing problems than their co-sibling who was exposed to no (or less severe) smoking during pregnancy (Ekblad et al. 2020). More severe exposure to substance use during pregnancy was also related to severity of problems in both boys and girls. Therefore, we hypothesize that smaller correlations noted in the literature of substance use during pregnancy with internalizing-type problems (Khoury et al. 2018; Min et al. 2020) are potentially the result of comorbid externalizing problems, with prenatal substance use exposure operating to simultaneously differentiate youth problems in the direction of externalizing problems while also making those problems more severe. This is, of course, a causal hypothesis, and the present study—based entirely on correlations within families where parents and children share genes, prenatal, and postnatal environments—cannot support such claims. Future work designed to test causal mechanisms are important for testing this hypothesis.
It was also interesting that prenatal substance use exposure was directly related to adolescent substance use progression for girls, but indirectly via specifically a preponderance of externalizing problems for boys. Recent accumulating evidence suggests that prenatal risk exposures could be more influential for boys’ behavioral development than girls’, and our findings are consistent with studies finding effects on boys but not girls when studying associations of prenatal substance use exposure with externalizing problems earlier in development (Marceau et al. 2019b). However, the presence of direct effects (i.e., outside of developmental cascades), in this study for girls suggests an unknown mechanism by which prenatal exposures have longer-term impacts that emerge later for girls. That is, by examining severity and directionality in the context of developmental cascades to substance use, we provide evidence that prenatal substance use exposure may indeed be particularly problematic for boys’ substance use because it serves as a differentiator pushing boys towards exhibiting externalizing problems earlier in childhood. However, prenatal substance use during pregnancy does not similarly serve as a differentiator of problem type for girls, and more work is needed to determine how prenatal substance use is associated with adolescent substance use for girls.
Intermediate influences
Parental harsh discipline
We found that parental discipline was indirectly associated with smoking and cannabis use in boys and girls via both severity and differentiation towards more externalizing problems, and with alcohol use progression in boys and girls via differentiation towards more externalizing problems. Critically, harsh discipline emerged as a robust predictor of severity and directionality in the context of the other constructs and covariates (i.e., even early life adversity). Harsh discipline is known to be heritable, and because of the composition of the sample (i.e., parents who are biologically related to and provide the caregiving environment for youth) the associations cannot be interpreted as entirely environmental. Based on prior literature, the associations we find for parental harsh discipline with severity and directionality are possibly, in part, a proxy for a transactional evocative gene–environment correlation process that unfolds over time (Button et al. 2008; Elam et al. 2018). We show that these processes are important not only as a non-specific risk factor for externalizing and internalizing problems, but also as a differentiator for externalizing problems. This is consistent with the notion of coercive cycles, developed specifically to explain transactional roles of harsh discipline and conduct problems (Patterson 1982). Further, we found no evidence of direct effects of harsh discipline on substance use, further corroborating the importance of coercive cycles as a part of a developmental cascade greatly increasing risk, indirectly through externalizing problems, for substance use progression in late adolescence (Dodge et al. 2009). This was true even in a complex developmental model that included other key influences on adolescent substance use identified in the literature.
The polygenic score was not associated with harsh discipline; therefore, the genes that are involved in gene–environment correlation processes serving to increase severity and push youth towards externalizing problems are unlikely to be puberty-related genes, specifically. However, the (small) observed correlations between parental discipline and some measures of pubertal onset may indicate that pubertal maturation perceived by parents and youth may be a contributing input for evocative gene–environment correlation processes that ultimately contributes to adolescent substance use progression. That is, as parents and youth notice pubertal onset, parents may directly treat youth differently/with more rules, responsibilities, and consequences, or may adapt their parenting strategies in response to children’s own autonomy-seeking reactions to pubertal onset (Marceau et al. 2020b).
Pubertal timing
There are several considerations regarding the measurement of pubertal onset in the current study that are important to keep in mind prior to interpreting findings. A strength was the repeated measures, allowing for relative precision in prospectively measuring pubertal onset (defined as attaining Tanner Stage 2), at least as perceived by parents and youth. ALSPAC is not the only study to use a combination of parent and youth report particularly at earlier ages (e.g., see the Wisconsin Study of Families and Work; Ellis and Essex 2007). This strategy is thought to prevent some of the bias related to youth who do not yet know what puberty is (because they have not yet experienced it) thinking they are more mature than they would be as rated by a professional. However, overlaying patterns of regression and raters suggest that parents and youth together over-rated boys as beginning genital development early. Even when using the second time of reaching Tanner Stage 2 for 948 boys, the age of attaining genital development Tanner Stage 2 was just under 10 years old. This is surprisingly early, and likely reflects poor measurement or understanding of this component of development. This extra bias for genital development is consistent with findings from Shirtcliff et al. (2009) showing that correlations between youth ratings of Tanner Stages vs. physical examination were somewhat lower for boys’ genital development (r = 0.60) than for boys’ pubic hair development (r = 0.71) or either girls’ phenotypes (r’s > 0.83). In general, findings regarding boys’ genital development especially, but indeed all measures of pubertal onset in this study should be interpreted as perceived onset rather than ‘actual’ onset.
With regard to our findings, the findings for girls were highly consistent with the literature that shows a clear role for pubertal maturation (of pubic hair onset at least) in increasing specifically internalizing problems, likely in part due to hormonal mechanisms (Copeland et al. 2019). For boys, perceived timing of genital development onset equally differentiated boys who thought they matured early towards externalizing-type problems, and boys who thought they matured late towards internalizing-type problems. This is a novel finding in the literature, consistent with some reports that early puberty is related to externalizing problems in boys (particularly White boys; Marceau et al. 2019a) that support the developmental readiness hypothesis (Ullsperger and Nikolas 2017), but not others that support the social compensation hypothesis (Marceau and Jackson 2017). Typically, studies examining associations of pubertal timing and externalizing and internalizing do not consider comorbidity (see Stice et al. 2001 for an exception in girls). Examining directionality of problems lead to several insights that can serve as the basis for novel hypotheses. (1) Boys’ perceptions may be particularly critical (above actual development) to understanding the role of pubertal maturation (Mendle 2014) in terms of differentiation of problems, given that these findings were not present for pubic hair development, only for genital development which showed clearer evidence of perceptual bias. (2) These perceptions may have more to do with the type of problem boys exhibit than the severity of problems. If this is the case, it is unsurprising that mixed, inconsistent, and small effects riddle the literature, as most measures of externalizing and internalizing problems assess the severity of each rather than the extent to which they are differentiated regardless of severity (i.e., directionality). Future work may confirm this new hypothesis that perceived puberty may differentiate problem type in boys, with longer-term consequences for downstream developmental outcomes like substance use.
Severity and directionality
Our analysis of severity and directionality yielded several new insights for transitions across adolescence from behavioral (externalizing and internalizing) risk to substance use progression. For boys and girls, severity of problems played a critical role in developmental cascades from more severe prenatal substance use exposure and late childhood parental discipline to further progression of the less normative substances: smoking and cannabis use. Severity of problems as measured in the severity–directionality model are analogous to the total level of symptoms regardless of type. Youth may have moderately high severity scores if they have a lot of symptoms of only one problem type, but to score very highly on this dimension, youth must be at least somewhat comorbid for externalizing and internalizing problems (Marceau and Neiderhiser 2020). Predictors of severity can be thought of as non-specific risk factors for behavioral problems (Shirtcliff and Essex 2008). Predicting directionality can be thought of as predicting problem differentiation (Marceau and Neiderhiser 2020). Our findings suggest a role of severity regardless of problem type in developmental cascades, as expected. However, there were more and stronger effects of directionality with all three substances, and particularly for boys. These effects often corroborated evidence from other designs suggesting that externalizing problems in particular posed a specific risk for substance use. Overall, the observed pattern of findings suggests that the primary role of internalizing symptoms for substance use outcomes is not protective, but rather risky through its comorbidity with externalizing problems (except, perhaps, for alcohol).
Alcohol, smoking, and cannabis use progressions
Alcohol use was nearly ubiquitous in late adolescence in the ALSPAC sample, reflecting the legality and popularity/normative nature of alcohol use in this population. This likely contributed to weaker findings of the various risk factors and especially problem behaviors predicting alcohol progression: most youth, well-adjusted or otherwise, use alcohol to a certain degree. However, for alcohol, we did see some protective effect of internalizing problems against alcohol use problems for girls and especially for boys (see “Appendix” Part C for fuller explanation). The inhibitory effect of anxiety on social drinking (Hussong et al. 2011) may have only been strong enough to observe in this sample for alcohol use because only youth with a tendency toward more pure internalizing problems were more likely to stop at early stages of alcohol use. In contrast, smoking and cannabis use were less often endorsed (with 50% and 40% at any stage of smoking and cannabis use, respectively). In this sample, therefore, smoking and cannabis use reflected somewhat less normative substances, and were more strongly linked to developmental cascades of risk that included prenatal substance use exposure and parental discipline, and transitions through earlier psychopathology. As adolescent substance use is highly predictive of future problems especially if use has progressed beyond more normative stages, these cascades may indicate pathways of lasting risk (e.g., Sartor et al. 2016). Future research tracking this sample through emerging adulthood may reveal whether these pathways do index lasting risk.
Limitations
The large and well-characterized ALSPAC cohort allowed us to test complex models of developmental cascades to substance use progression. However, these findings are quite limited in generalizability, given the homogeneity and relative privilege of sample, especially of those who continued through the end of the study. Our sample consists of White European youth, and the findings presented here likely are culturally specific to that group, especially given race/ethnic differences in discipline practices (Silveira et al. 2021) and evidence that harsh discipline is not linked to externalizing problems in race/ethnic minority groups as strongly as in White samples (Lansford 2010). Indeed, there is evidence of race/ethnic differences in other developmental cascades—namely pathways from genetic and/or prenatal risk through cortisol reactivity for externalizing and substance use have been found in Black (Buckingham-Howes et al. 2016; Conradt et al. 2014) but not White adolescents (Marceau et al. 2020a). It is critical to identify and test the appropriate developmental cascades within underrepresented groups to move our field forward.
Further, although we included several theoretically important factors in our developmental cascade models, other influences are also important to consider, including peer influences. Similarly, our cascade models are also over-simplified in terms of processes, examining only snapshots on the longest timescale of child and adolescent development. For example, our inclusion of a single measure of parental harsh discipline and a single measure of severity and directionality years later grossly over-simplifies the complex transactional associations expected at shorter timescales (e.g., over the course of conversations which accumulate and canalize into habitual patterns across development; Lougheed 2020). And, that measure of harsh discipline reflected the combination of two items, only one of which has face validity as a measure of harsh discipline. Sensitivity analyses (available upon author request) found that the present analyses do likely represent harsh discipline, although use of more nuanced measures will be important for future work. Another methodological limitation is that ALSPAC was included in the GWAS from which the PRS was formed, which may have slightly inflated results of the PRS (see Horvath et al. 2020). Finally, our pathway-based cascade model does not incorporate contextual influences (i.e., moderators) that are known to be important for the development of substance use. Despite these limitations, our models provide a valuable perspective on adolescent substance use development.
Conclusions and future directions
Using an alternative measurement strategy for examining externalizing/internalizing symptom comorbidity, the present study most strongly supported developmental cascades involving differentiation towards externalizing problems and total symptom severity as intermediaries between associations of parental harsh discipline with substance use progressions for girls and boys. Our findings make three main novel contributions to the literature. First, the strongest role of internalizing problems was to increase risk of substance use via comorbidity with externalizing problems, adding to general symptom severity, especially for less normative substances. There was very limited evidence of protective effects of relatively pure internalizing and only for the normative outcome: alcohol use. Second, the presence of more and stronger effects of directionality than severity suggest that the mechanism of action of the diverse predictors examined here in terms of risk for adolescent substance use is more due to pushing youth towards a specific type of (externalizing) behavior than generally increasing the level of problems. Finally, there was support of developmental cascades from more severe exposure to prenatal substance use to adolescent substance use progression specifically for boys, whereas for girls the associations were direct. Considering that many studies earlier in childhood find that prenatal risks may disproportionately affect males, and specifically link to externalizing problems, our findings provide suggest that prenatal effects for girls may operate through other pathways and/or may surface later in development—a new hypothesis in need of interrogation.
Data availability
Data for the current study is available from the ALSPAC study: http://www.bristol.ac.uk/alspac/researchers/access/.
Code availability
Derived variables and associated code for variables created in this study are returned to the ALSPAC Executive Team, and are available/distributed by ALSPAC. Data analytic scripts or additional details are freely available upon author request.
Notes
We also considered a more restrictive measure of harsh discipline that included only the slapped/hit item, averaged across the 9.5 and 11.5 year assessments. Results (available on author request) were practically identical when using this more restrictive measure; we elected to present findings from the more psychometrically sound four-item measure.
References
Bailey JA, Hill KG, Oesterle S, Hawkins JD (2009) Parenting practices and problem behavior across three generations: monitoring, harsh discipline, and drug use in the intergenerational transmission of externalizing behavior. Dev Psychol 45(5):1214–1226
Beltz AM, Corley RP, Wadsworth SJ, DiLalla LF, Berenbaum SA (2020) Does puberty affect the development of behavior problems as a mediator, moderator, or unique predictor? Dev Psychopathol 32(4):1473–1485
Bender HL, Allen JP, McElhaney KB, Antonishak J, Moore CM, Kelly HOB, Davis SM (2007) Use of harsh physical discipline and developmental outcomes in adolescence. Dev Psychopathol 19(1):227
Boyd A, Golding J, Macleod J, Lawlor DA, Fraser A, Henderson J, Molloy L, Ness A, Ring S, Davey Smith G (2013) Cohort Profile: The ‘Children of the 90s’—the index offspring of the Avon Longitudinal Study of Parents and Children. Int J Epidemiol 42(1):111–127
Bowen E, Heron J, Waylen A, Wolke D, & ALSPAC Study Team (2005) Domestic violence risk during and after pregnancy: findings from a British longitudinal study. BJOG Int J Obstet Gynaecol 112(8):1083–1089
Brenner V, Fox RA (1998) Parental discipline and behavior problems in young children. J Genet Psychol 159(2):251–256
Buckingham-Howes S, Mazza D, Wang Y, Granger DA, Black MM (2016) Prenatal drug exposure and adolescent cortisol reactivity: association with behavioral concerns. J Dev Behav Pediatr 37(7):565–572
Button TMM, Lau JYF, Maughan B, Eley TC (2008) Parental punitive discipline, negative life events and gene–environment interplay in the development of externalizing behavior. Psychol Med 38(1):29–39
Colder CR, Scalco M, Trucco EM, Read JP, Lengua LJ, Wieczorek WF, Hawk LW Jr (2013) Prospective associations of internalizing and externalizing problems and their co-occurrence with early adolescent substance use. J Abnormal Child Psychol 41(4):667–677
Conradt E, Abar B, Lester BM, LaGasse LL, Shankaran S, Bada H, Bauer CR, Whitaker TM, Hammond JA (2014) Cortisol reactivity to social stress as a mediator of early adversity on risk and adaptive outcomes. Child Dev 85(6):2279–2298
Copeland WE, Worthman C, Shanahan L, Costello EJ, Angold A (2019) Early pubertal timing and testosterone associated with higher levels of adolescent depression in girls. J Am Acad Child Adolesc Psychiatry 58(12):1197–1206
Corley RP, Beltz AM, Wadsworth SJ, Berenbaum SA (2015) Genetic influences on pubertal development and links to behavior problems. Behav Genet 45(3):294–312
Day FR, Thompson DJ, Helgason H, Chasman DI, Finucane H, Sulem P, Ruth KS, Whalen S, Sarkar AK, Albrecht E (2017) Genomic analyses identify hundreds of variants associated with age at menarche and support a role for puberty timing in cancer risk. Nat Genet. https://doi.org/10.1530/ey.15.7.5
Deardorff J, Marceau K, Johnson M, Reeves J, Biro FM, Kubo A, Greenspan LC, Laurent C, Windham GC, Pinney SM, Kushi LH, Hiatt RA (2021) Girls’ timing and tempo and mental health: a longitudinal examination in an ethnically-diverse sample. J Adolesc Health 68(6):1197–1203
Dick DM, Rose RJ, Viken RJ, Kaprio J (2000) Pubertal timing and substance use: associations between and within families across late adolescence. Dev Psychol 36(2):180–189
Dodge KA, Malone PS, Lansford JE, Miller S, Pettit GS, Bates JE (2009) A dynamic cascade model of the development of substance-use onset. Monogr Soc Res Child Dev 74(3):vii–119
Donaldson CD, Handren LM, Crano WD (2016) The enduring impact of parents’ monitoring, warmth, expectancies, and alcohol use on their children’s future binge drinking and arrests: a longitudinal analysis. Prev Sci 17(5):606–614
Dorn LD, Dahl RE, Woodward HR, Biro F (2006) Defining the boundaries of early adolescence: a user’s guide to assessing pubertal status and pubertal timing in research with adolescents. Appl Dev Sci 10(1):30–56
Edwards AC, Latendresse SJ, Heron J, Cho SB, Hickman M, Lewis G, Dick DM, Kendler KS (2014) Childhood internalizing symptoms are negatively associated with early adolescent alcohol use. Alcohol Clin Exp Res 38(6):1680–1688
Ekblad MO, Marceau K, Rolan E, Palmer RH, Todorov A, Heath AC, Knopik VS (2020) The effect of smoking during pregnancy on severity and directionality of externalizing and internalizing symptoms: a genetically informed approach. Int J Environ Res Public Health 17(21):7921
Elam KK, Chassin L, Pandika D (2018) Polygenic risk, family cohesion, and adolescent aggression in Mexican American and European American families: developmental pathways to alcohol use. Dev Psychopathol 30(5):1715–1728
Ellis BJ, Essex MJ (2007) Family environments, adrenarche, and sexual maturation: a longitudinal test of a life history model. Child Dev 78(6):1799–1817
Eriksson C, Kaprio J, Pulkkinen L, Rose R (2005) Testosterone and alcohol use among adolescent male twins: testing between-family associations in within-family comparisons. Behav Genet 35(3):359–368
Essex MJ, Klein MH, Cho E, Kraemer HC (2003) Exposure to maternal depression and marital conflict: gender differences in children’s later mental health symptoms. J Am Acad Child Adolesc Psychiatry 42(6):728–737
Essex MJ, Shirtcliff EA, Burk LR, Ruttle PL, Klein MH, Slattery MJ, Kalin NH, Armstrong JM (2011) Influence of early life stress on later hypothalamic-pituitary-adrenal axis functioning and its covariation with mental health symptoms: a study of the allostatic process from childhood into adolescence. Dev Psychopathol 23:1039–1058. https://doi.org/10.1017/s0954579411000484
Fraser A, Macdonald-Wallis C, Tilling K, Boyd A, Golding J, Davey Smith G, Henderson J, Macleod J, Molloy L, Ness A (2013) Cohort profile: the Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol 42(1):97–110
Ge X, Natsuaki MN (2009) In search of explanations for early pubertal timing effects on developmental psychopathology. Curr Dir Psychol Sci 18(6):327–331
Goodman R (1997) The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry Allied Discipl 38(5):581–586
Goodman R, Meltzer H, Bailey V (1998) The Strengths and Difficulties Questionnaire: a pilot study on the validity of the self-report version. Eur Child Adolesc Psychiatry 7(3):125–130
Grumbach MM, Styne DM (2003) Puberty: ontogeny, neuroendocrinology, physiology, and disorders. In: Larsen PR, Kronenberg HM, Melmed S, Polonsky KS (eds) Williams textbook of endocrinology, vol 10. WB Saunders, Philadelphia, pp 1115–1286
Hicks BM, Schalet BD, Malone SM, Iacono WG, McGue M (2011) Psychometric and genetic architecture of substance use disorder and behavioral disinhibition measures for gene association studies. Behav Genet 41(4):459–475
Hopfer CJ, Crowley TJ, Hewitt JK (2003) Review of twin and adoption studies of adolescent substance use. J Am Acad Child Adolesc Psychiatry 42(6):710–719
Horvath G, Knopik VS, Marceau K (2020) Polygenic influences on pubertal timing and tempo and depressive symptoms in boys and girls. J Res Adolesc 30(1):78–94
Hummel A (2014) Substance use in adolescent girls: the interplay of pubertal timing, family and peer influence. Cardiff University, Cardiff
Hussong AM, Jones DJ, Stein GL, Baucom DH, Boeding S (2011) An internalizing pathway to alcohol and substance use disorders. Psychol Addict Behav J Soc Psychol Addict Behav 25(3):390–404
Hussong AM, Ennett ST, Cox MJ, Haroon M (2017) A systematic review of the unique prospective association of negative affect symptoms and adolescent substance use controlling for externalizing symptoms. Psychol Addict Behav J Soc Psychol Addict Behav 31(2):137–147
Irner TB (2012) Substance exposure in utero and developmental consequences in adolescence: a systematic review. Child Neuropsychol J Normal Abnormal Dev Child Adolesc 18(6):521–549
Khoury JE, Jamieson B, Milligan K (2018) Risk for childhood internalizing and externalizing behavior problems in the context of prenatal alcohol exposure: a meta-analysis and comprehensive examination of moderators. Alcohol Clin Exp Res 42(8):1358–1377
Lansford JE, Erath S, Yu T, Pettit GS, Dodge KA, Bates JE (2008) The developmental course of illicit substance use from age 12 to 22: links with depressive, anxiety, and behavior disorders at age 18. J Child Psychol Psychiatry Allied Discipl 49(8):877–885
Lansford JE (2010) The special problem of cultural differences in effects of corporal punishment. Law Contemp Probl 73(2):89–106
Lansford JE, Criss MM, Laird RD, Shaw DS, Pettit GS, Bates JE, Dodge KA (2011) Reciprocal relations between parents’ physical discipline and children’s externalizing behavior during middle childhood and adolescence. Dev Psychopathol 23(01):225–238
Legleye S, Karila L, Beck F, Reynaud M (2007) Validation of the CAST, a general population Cannabis Abuse Screening Test. J Subst Use 12(4):233–242
Lougheed JP (2020) Parent–adolescent dyads as temporal interpersonal emotion systems. J Res Adolesc 30(1):26–40
Maier R, Visscher P, Robinson M, Wray N (2018) Embracing polygenicity: a review of methods and tools for psychiatric genetics research. Psychol Med 48(7):1055–1067
Maisonet M, Christensen KY, Rubin C, Holmes A, Flanders WD, Heron J, Ong KK, Golding J, McGeehin MA, Marcus M (2010) Role of prenatal characteristics and early growth on pubertal attainment of British girls. Pediatrics 126(3):e591–e600
Marceau K, Neiderhiser J, Lichtenstein P, Reiss D (2012) Genetic and environmental influences on the association between pubertal maturation and internalizing symptoms. J Youth Adolesc 41(9):1111–1126
Marceau K, Abar C, Jackson K (2015a) Parental knowledge is a contextual amplifier of associations of pubertal maturation and substance use. J Youth Adolesc 44(9):1720–1734
Marceau K, Laurent H, Neiderhiser J, Reiss D, Shaw D, Natsuaki M, Fisher P, Leve L (2015b) Combined influences of genes, prenatal environment, cortisol, and parenting on the development of children’s internalizing versus externalizing problems. Behav Genet 45:268–282
Marceau K, Zahn-Waxler C, Shirtcliff EA, Schreiber JE, Hastings P, Klimes-Dougan B (2015c) Adolescents’, mothers’, and fathers’ gendered coping strategies during conflict: youth and parent influences on conflict resolution and psychopathology. Dev Psychopathol 27(4pt1):1025–1044
Marceau K, De Arujo-Greecher M, Miller ES, Massey SH, Mayes LC, Ganiban JM, Reiss D, Shaw DS, Leve LD, Neiderhiser JM (2016) The Perinatal Risk Index: early risks experienced by domestic adoptees in the united states. PLoS ONE 11(3):e0150486
Marceau K, Jackson K (2017) Deviant peers as a mediator of pubertal timing–substance use associations: the moderating role of parental knowledge. J Adolesc Health 61(1):53–60
Marceau K, Kirisci L, Tarter RE (2019a) Correspondence of pubertal neuroendocrine and Tanner stage changes in boys and associations with substance use. Child Dev 90(6):e763–e782
Marceau K, Rolan E, Leve LD, Ganiban JM, Reiss D, Shaw DS, Natsuaki MN, Egger H, Neiderhiser JM (2019b) Parenting and prenatal risk as moderators of genetic influences on conduct problems during middle childhood. Dev Psychol 55:1164–1181. https://doi.org/10.1037/dev0000701
Marceau K, Brick L, Knopik VS, Reijneveld SA (2020a) Developmental pathways from genetic, prenatal, parenting and emotional/behavioral risk to cortisol reactivity and adolescent substance use: a TRAILS study. J Youth Adolesc 49:17–31
Marceau K, Nair N, Rogers ML, Jackson KM (2020b) Lability in parent- and child-based sources of parental monitoring is differentially associated with adolescent substance use. Prev Sci 21(4):1–12
Marceau K, Neiderhiser J (2020) Generalist genes and specialist environments for adolescent internalizing and externalizing problems: a test of severity and directionality. Dev Psychopathol. https://doi.org/10.1017/S0954579420001108
Masten AS, Roisman GI, Long JD, Burt KB, Obradović J, Riley JR, Boelcke-Stennes K, Tellegen A (2005) Developmental cascades: linking academic achievement and externalizing and internalizing symptoms over 20 years. Dev Psychol 41(5):733
McNeil TF, Cantor-Graae E, Sjöström K (1994) Obstetric complications as antecedents of schizophrenia: empirical effects of using different obstetric complication scales. J Psychiatr Res 28(6):519–530
Mendle J, Turkheimer E, Emery RE (2007) Detrimental psychological outcomes associated with early pubertal timing in adolescent girls. Dev Rev 27(2):151–171
Mendle J, Ferrero J (2012) Detrimental psychological outcomes associated with pubertal timing in adolescent boys. Dev Rev 32(1):49–66
Mendle J (2014) Beyond pubertal timing: new directions for studying individual differences in development. Curr Dir Psychol Sci 23(3):215–219
Min MO, Albert JM, Lorincz-Comi N, Minnes S, Lester B, Momotaz H, Powers G, Yoon D, Singer LT (2020) Prenatal substance exposure and developmental trajectories of internalizing symptoms: toddlerhood to preadolescence. Drug Alcohol Depend 218:108411
Morris NM, Udry JR (1980) Validation of a self-administered instrument to assess stage of adolescent development. J Youth Adolesc 9(3):271–280
Neiderhiser JM, Marceau K, De Araujo-Greecher M, Ganiban JM, Mayes LC, Shaw DS, Reiss D, Leve LD (2016) Estimating the roles of genetic risk, perinatal risk, and marital hostility on early childhood adjustment: medical records and self-reports. Behav Genet 46:334–352. https://doi.org/10.1007/s10519-016-9788-0
Neiderhiser JM, Marceau K, Reiss D (2013) Four factors for the initiation of substance use by young adulthood: a 10-year follow-up twin and sibling study of marital conflict, monitoring, siblings, and peers. Dev Psychopathol 25(Special Issue 01):133–149
Patterson G (1982) Coercive family process: a social learning approach. Castalia, Eugene
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, Maller J, Sklar P, De Bakker PI, Daly MJ (2007) PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 81(3):559–575
Rhee SH, Lahey BB, Waldman ID (2015) Comorbidity among dimensions of childhood psychopathology: converging evidence from behavior genetics. Child Dev Perspect 9(1):26–31
Riggins-Caspers KM, Cadoret RJ, Knutson JF, Langbehn D (2003) Biology–environment interaction and evocative biology–environment correlation: contributions of harsh discipline and parental psychopathology to problem adolescent behaviors. Behav Genet 33(3):205–220
Rose J, Roman N, Mwaba K, Ismail K (2018) The relationship between parenting and internalizing behaviours of children: a systematic review. Early Child Dev Care 188(10):1468–1486
Rosseel Y (2012) lavaan: an R package for structural equation modeling. J Stat Softw 48(2):36
Sartor CE, Jackson KM, McCutcheon VV, Duncan AE, Grant JD, Werner KB, Bucholz KK (2016) Progression from first drink, first intoxication, and regular drinking to alcohol use disorder: a comparison of African American and European American youth. Alcohol Clin Exp Res 40(7):1515–1523
Saunders JB, Aasland OG, Babor TF, De la Fuente JR, Grant M (1993) Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction (abingdon Engl) 88(6):791–804
Scalco MD, Colder CR, Read JP, Lengua LJ, Wieczorek WF, Hawk LW (2020) Testing alternative cascades from internalizing and externalizing symptoms to adolescent alcohol use and alcohol use disorder through co-occurring symptoms and peer delinquency. Dev Psychopathol 33(1):1–18
Schelleman-Offermans K, Knibbe RA, Kuntsche E (2013) Are the effects of early pubertal timing on the initiation of weekly alcohol use mediated by peers and/or parents? A Longitudinal Study. Dev Psychol 49(7):1277–1285
Shirtcliff EA, Essex MJ (2008) Concurrent and longitudinal associations of basal and diurnal cortisol with mental health symptoms in early adolescence. Dev Psychobiol 50(7):690–703
Shirtcliff EA, Dahl RE, Pollak SD (2009) Pubertal development: correspondence between hormonal and physical development. Child Dev 80(2):327–337
Silveira F, Shafer K, Dufur MJ, Roberson M (2021) Ethnicity and parental discipline practices: a cross-national comparison. J Marriage Fam 83(3):644–666
Stice E, Presnell K, Bearman SK (2001) Relation of early menarche to depression, eating disorders, substance abuse, and comorbid psychopathology among adolescent girls. Dev Psychol 37(5):608
Trucco EM, Hicks BM, Villafuerte S, Nigg J, Burmeister M, Zucker RA (2016) Temperament and externalizing behavior as mediators of genetic risk on adolescent substance use. J Abnormal Psychol 125(4):565–575
Trucco EM, Villafuerte S, Hussong A, Burmeister M, Zucker RA (2018) Biological underpinnings of an internalizing pathway to alcohol, cigarette, and marijuana use. J Abnormal Psychol 127(1):79–91
Ullsperger JM, Nikolas MA (2017) A meta-analytic review of the association between pubertal timing and psychopathology in adolescence: are there sex differences in risk? Psychol Bull 143(9):903
Vaughan EB, Van Hulle CA, Beasley WH, Rodgers JL, D’Onofrio BM (2015) Clarifying the associations between age at menarche and adolescent emotional and behavioral problems. J Youth Adolesc 44(4):922–939
Weigard AS, Hardee JE, Zucker RA, Heitzeg MM, Beltz AM (2020) The role of pubertal timing in the link between family history of alcohol use disorder and late adolescent substance use. Drug Alcohol Depend 210:107955
Weymouth BB, Fosco GM, Feinberg ME (2019) Nurturant-involved parenting and adolescent substance use: examining an internalizing pathway through adolescent social anxiety symptoms and substance refusal efficacy. Dev Psychopathol 31(1):247
Zheng J, Erzurumluoglu AM, Elsworth BL, Kemp JP, Howe L, Haycock PC, Hemani G, Tansey K, Laurin C, Pourcain BS (2017) LD Hub: a centralized database and web interface to perform LD score regression that maximizes the potential of summary level GWAS data for SNP heritability and genetic correlation analysis. Bioinformatics 33(2):272–279
Acknowledgements
We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC Team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses.
Funding
The UK Medical Research Council and Wellcome (Grant Ref. 217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC. This publication is the work of the authors, who will serve as guarantors for the contents of this paper. A comprehensive list of grants funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf). GWAS data was generated by Sample Logistics and Genotyping Facilities at Wellcome Sanger Institute and LabCorp (Laboratory Corporation of America) using support from 23andMe. This research was specifically funded by the National Institute on Drug Abuse (K01 DA039288, Marceau).
Author information
Authors and Affiliations
Contributions
KM conceived of the study, analyzed the data, and drafted the manuscript. GH and AL were instrumental in construction of key study variables. VK was instrumental in conceptualizing the study. All authors edited the manuscript and approved of the final manuscript prior to submission.
Corresponding author
Ethics declarations
Conflict of interest
Kristine Marceau, Gregor Horvath, Amy Loviska, and Valerie Knopik declare that they have no conflict of interest.
Ethical approval
Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Ethical approval for the present data analysis was also obtained from the Purdue University IRB.
Informed consent
Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Marceau, K., Horvath, G., Loviska, A.M. et al. Developmental Cascades from Polygenic and Prenatal Substance Use to Adolescent Substance Use: Leveraging Severity and Directionality of Externalizing and Internalizing Problems to Understand Pubertal and Harsh Discipline-Related Risk. Behav Genet 51, 559–579 (2021). https://doi.org/10.1007/s10519-021-10068-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10519-021-10068-6