
Aging in Down syndrome (DS) is accompanied by neuropathological features of Alzheimer’s disease (AD). Therefore, DS has been proposed as a model to study predementia stages of AD. MRI-based measurement of grey matter atrophy is an in vivo surrogate marker of regional neuronal density. A range of neuroimaging studies have described the macroscopic neuroanatomy of DS. Recent studies using sensitive quantitative measures of region-specific atrophy based on high-resolution MRI suggest that age-related atrophy in DS resembles the pattern of brain atrophy in early stages of AD. The pattern of atrophy determined in predementia DS supports the notion that AD-type pathology leads to neuronal degeneration not only in allocortical, but also in neocortical brain areas before onset of clinical dementia. This has major implications for our understanding of the onset and progression of AD-type pathology both in DS and in sporadic AD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The Neuropathology of DS as a Model for Preclinical Alzheimer’s Disease
Subjects with Down syndrome (DS) older than 40 years show an age-related cognitive impairment with early memory involvement followed by a linear decline in non-memory cognitive function (Alexander et al., 1997; Lai and Williams, 1989; Schapiro, et al., 1992). Cognitive impairment progresses to a dementia syndrome resembling Alzheimer’s disease (AD) (Alexander et al., 1997; Evenhuis, 1990; Lai and Williams, 1989; Schapiro, et al., 1992). Prevalence of dementia has been estimated to reach 5% to 10% until the fifth decade of life and 40% to 50% by the sixth decade of life in DS (Evenhuis, 1990; Lai and Williams, 1989). Postmortem studies show that at 40 years of age virtually all DS subjects have neuropathological lesions that meet the pathological criteria for AD (Mann et al., 1984; Wisniewski et al., 1985a, b). Similar to patients with sporadic AD, elderly DS subjects show cerebral atrophy, deposition of A\(\upbeta\) protein in extracellular senile plaques and perivascular amyloid (amyloid angiopathy), intra-neuronal neurofibrillary tangles (NFT) and extracellular neuritic plaques and neuropil threads (Jellinger and Bancher, 1998; Mann, 1988). A\(\upbeta\) protein derives from atypical splicing of an ubiquitous transmembrane protein, the amyloid precursor protein, which is coded on chromosome 21 (Vassar, 2005). Neuritic changes arise from the formation of paired helical filaments (PHF) containing polymerized hyperphosphorylated tau protein triplets and cause disruption of the neuronal cytoskeleton with loss of synapses and neurons and altered cortico-cortical connectivity, leading to disconnection of the cerebral cortex (Morrison et al., 1986). Neuropathological changes in sporadic AD follow a specific sequence starting in transentorhinal and entorhinal cortex in preclinical stages, later spreading to the hippocampus and involving neocortical association regions in more advanced stages of disease. Primary sensorimotor areas are relatively spared even at severe stages of AD (Braak et al., 1997). A subcortical area typically affected is the cholinergic nucleus basalis Meynert in the basal forebrain (Mesulam, 2004; Teipel et al., 2005). Although the role of plaques and NFT in the pathogenesis of AD remains undetermined, clinicopathological studies have shown that both lesions, if present in sufficient numbers, particularly in the neocortex, are the best morphological marker for AD. Recent studies on neuronal death in AD have indicated only an indirect relationship between neuronal loss and both A\(\upbeta\) deposition and NFTs. Therefore, both AD markers appear to increase the risk of cells to degenerate, but are not the sole cause of the degenerative process in AD.
DS subjects can exhibit significant amyloid deposition in the cerebral cortex already in their third or fourth decade of life (Ikeda et al., 1989; Rumble et al., 1989). Earliest pathological changes are thought to occur in the medial temporal lobe, after which they are found in neocortical association regions by age of 40 (Hof et al., 1995; Hyman et al., 1995; Mann and Esiri, 1989; Sadowski et al., 1999). An important factor for the development of the neuropathological and clinical phenotype of AD in elderly DS subjects is an increased amyloid burden due to an extra copy of the amyloid precursor protein gene on chromosome 21 (Rumble et al., 1989). The laminar and regional cortical distribution of amyloid and neurofibrillary pathology and neuronal loss closely resembles that of AD. On this basis, DS has been proposed as a model to study the predementia stages of AD (Mann, 1988). There are, however, dissimilarities between both pathologies. Pyramidal neuron abnormalities with reduced dendritic arborization, decreased numbers of spines, spine atrophy and anomalies of spine orientation are already present in infancy and fetal stages of DS (Becker et al., 1991b). Additionally, there are cytoskeletal abnormalities in DS (Mann et al., 1989). These developmental abnormalities make the brain of DS subjects vulnerable for any type of lesions and might contribute to the early onset of dementia in DS subjects. Therefore, the use of DS as a predementia model of AD has to take into account that developmental abnormalities and DS-specific degenerative processes contribute to the neuropathological substrate of dementia in DS.
Methodological Basis of MRI Analysis Techniques
MRI-based measurement of regional brain atrophy can provide an in vivo estimate of neuronal loss in neurodegenerative disease. This has specifically been shown for hippocampus atrophy as a measure of allocortical neuronal loss in AD (Bobinski et al., 2000; Jack et al., 2002; Nagy et al., 1996). There are no clinical–pathological correlational studies for other MRI-based volumetric measurements, such as entorhinal cortex, cortical gray matter volume or corpus callosum, but in vivo estimates of atrophy derived from MRI-based measurements in areas other than the hippocampus agree with the distribution of neuronal loss and neurofibrillary pathology in postmortem studies in AD (Chetelat and Baron, 2003; Nagy et al., 1999; Smith, 2002; Weis et al., 1991a). Therefore, MRI-based measurement of regional brain atrophy may also be useful in elderly DS subjects to determine brain atrophy related to AD-type pathology. Based on the evidence from neuropathological studies these changes can be interpreted as in vivo marker of progressive AD-related neuron loss. As structural MRI has no known side effects in patients without ferromagnetic implants, it allows repeated examinations over time to study the progression of regional atrophy. Volumetric assessments are based on three-dimensional T1 weighted MRI sequences with a spatial resolution of about 1 mm in all three axes. Acquisition of such a sequence takes about 10–15 min on a 1.5 Tesla scanner. In recent years, 3-T scanners became more widely available so that in the near future volumetric studies will use T1 weighted sequences at 3-T with higher resolution and higher signal to noise ratio.
A wide array of techniques has been developed to determine the extent of regional brain atrophy from volumetric MRI data: (i) visual rating scales, (ii) observer-driven manual volumetry (Fig. 1) and (iii) automated voxel-based techniques (Fig. 2).

Manual volumetric measures. (a) Hippocampus/amygdala volumetry. Left: sagittal MRI section through the right hippocampus with the hippocampus (light blue) and the amygdala (turquoise, anterior to hippocampus) manually labeled. Right: three-dimensional reconstruction of the hippocampus and amygdala from manually labeled volumetric MRI scans (Hampel et al., 2002b). (b) Corpus callosum. Midsagittal MRI section through the brain with the corpus callosum and five corpus callosum subregions manually outlined (Teipel et al., 2002a). C1 – Rostrum; C2 – anterior truncus; C3 – middle truncus; C4 – posterior truncus and isthmus; C5 – Splenium. (c) Lobar volumes. Upper row: Schematic drawing of lobar borders on the sagittal surface of the brain: central sulcus between frontal and parietal lobes; lateral sulcus between frontal and temporal lobes; geometrical construction based on the sulcus parieto–occipitalis and the most posterior point of the lateral sulcus between parietal, temporal and occipital lobes. Lower row: Lobar borders projected on the lateral surface projection of the brain from a volumetric MRI scan (Bokde et al., 2002).

The processing stream of classical VBM An MRI volume of the brain in native space (a) is transformed into standard space according to the Talairach and Tournoux coordinate system (Talairach and Tournoux, 1988) using a non-linear transformation algorithm in reference to a standard brain template (b), resulting in an MRI brain volume in standard space (c). This volume is segmented into cerebrospinal fluid (d), gray matter (e) and white matter (f) maps. After smoothing with a Gaussian kernel (g), MRI volumes in standard space are pooled across several subjects and can be subjected to statistical analysis on a voxel by voxel basis, typically using the general linear model framework (matrix h).
Visual rating scales are easily applicable at the cost of relatively low inter-rater reliability (Frisoni et al., 2003). Moreover, they are limited to few anatomical features, like gross brain atrophy, ventricular enlargement or hippocampus atrophy. They are useful for the assessment of individual brain atrophy in clinical routine. Manual volumetric measures are time-consuming, but provide much higher inter-rater reliability. Like visual ratings, manual volumetric measures are limited to few anatomical features. In contrast, automated morphometric techniques provide fast and reliable segmentation of a multitude of anatomical features within a spatial resolution at voxel-level (Ashburner and Friston, 2000). However, all automated techniques are prone to artifacts induced by differences in image quality leading to local misregistration (Bookstein, 2001). This is particularly true for multicenter data, so that few studies so far have tried to pool MRI data from several centers for automated morphometric analysis. Results from automated analysis always should be compared with findings from manual volumetric studies and results from independent samples to assess their validity.
MRI Shows the Neuroanatomy of DS in vivo
The neuroanatomy of DS has two dimensions: (i) the developmental abnormality of the brain constituting an important part of the DS phenotype and (ii) the progressive brain atrophy with advancing age in DS adults that is superimposed on the developmental abnormality and is believed to result partly from AD-type pathological changes. In recent years, autopsy data on the neuroanatomy of DS have been complemented by an increasing body of evidence from in vivo structural imaging using CT and to a larger extent MRI.
MRI Shows the Developmental Abnormalities of the DS Brain
The brain of DS subjects is characterized by several postmortem macroscopic features which are related to pre- and post-natal abnormalities in synaptogenesis leading to retardation of brain growth (Schmidt-Sidor et al., 1990): lower brain weight and brachycephaly, with a small cerebellum, frontal and temporal lobes, reduced number and depth of the cerebral sulci, and a narrow superior temporal gyrus (Becker et al., 1991a; Coyle et al., 1986; Wisniewski, 1990). Even after controlling for body size, brain volume is smaller in DS subjects compared to age-matched normal controls (Raz et al., 1995; Yoshimura et al., 1990). MRI studies show a consistent phenotype of regional brain abnormalities compared to age-matched non-DS subjects. Table I gives an overview on MRI volumetric findings in young and non-demented adult DS subjects compared to age-matched non-DS controls.
Consistent with postmortem data, overall brain volume is reduced in DS subjects, including cerebellum and cerebral gray and white matter. Hippocampus volume is disproportionally reduced, whereas amygdala volume reductions do not exceed the overall reduction of brain size. Interestingly, parahippocampal gyrus volume is relatively larger in DS (Kesslak et al., 1994; Raz et al., 1995). This might be related to developmental abnormalities in neurogenesis. Only one study investigated the relative reductions of cerebral lobe volumes in DS (Pinter et al., 2001b), one study investigated volumes of anterior and posterior cortex (Jernigan, et al., 1993). Cerebral volume reductions were predominant in frontal and occipital lobes, as well as in planum temporale and superior temporal gyrus. Absolute volumes of temporal and parietal lobes were reduced, but these effects were no more significant after adjustment for overall brain size. The relative preservation of temporal lobe volume was related to a significantly larger white matter volume after adjustment for brain size. The authors speculated that this might reflect a selective abnormality in white matter maturation. An additional factor, however, may be methodological difficulties in determining the posterior borders of the temporal lobes on MRI scans, as their method relied on a semi-automated parcellation of the brain using a pediatric template. It is not clear from the study whether the use of a normal pediatric brain template might have introduced a bias in defining the lobe borders on the differently proportioned brains of the DS subjects. In two previous studies, subcortical gray matter structures (basal ganglia, thalamus) were normal in DS (Jernigan et al., 1993; Pinter et al., 2001b).
MRI Shows Effects of Aging on the DS Brain
Potential Study Designs
Age-related changes of brain morphometry in elderly non-demented DS subjects are thought to represent the effect of preclinical AD-type pathology. However, the effects of aging are superimposed on preexisting developmental brain abnormalities in DS. Therefore, the design of an MRI study may depend upon the specific question to be answered. Not every design is able to differentiate between developmental abnormalities and age-related changes of the brain in DS. Three basic designs can be distinguished:
-
(i)
studies comparing elderly DS subjects with elderly non-DS subjects are suitable for the description of correlations between regional brain measurements and cognitive abnormalities, but not the differentiation between the contribution of developmental and age-related alterations.
-
(ii)
studies comparing elderly DS subjects with younger DS subjects can describe age-related alterations in brain morphology possibly linked to AD-type pathology. However, they cannot distinguish between the effects of age and AD-type pathology.
-
(iii)
studies providing an intra-individual timeline of regional brain atrophy are often difficult to perform due to methodological limitations (changes in scanner hardware over time, selection bias over time due to non-randomly missing subjects), but are the gold standard to determine the effect of AD-type pathology on the DS brain.
MRI Findings on Age Effects in the Medial Temporal Lobes
In recent years, in vivo studies using magnetic resonance imaging (MRI) have investigated age-related brain atrophy in DS. Several computer assisted tomography (CT) and MRI studies have reported significantly reduced volumes of the hippocampus and adjacent medial temporal lobe structures with advancing age in non-demented DS subjects (Kesslak et al., 1994; Krasuski et al., 2002; Lawlor et al., 2001). Hippocampus and amygdala volumes are significantly correlated with decline of memory function, even after controlling for overall cognitive performance and age (Krasuski et al., 2002). These findings agree with neuropathological evidence of extensive tangle pathology and neuronal loss in entorhinal cortex and hippocampus (Hof et al., 1995; Sadowski et al., 1999) as well as the early decline of memory function in elderly DS subjects.
Two studies found no atrophy of hippocampus and parahippocampal gyrus before onset of dementia. Both studies, however, together with others showed reductions of hippocampus and parahippocampal gyrus volumes in elderly demented DS subjects compared to non-demented, younger DS subjects (Aylward et al., 1999; Pearlson et al., 1998; Raz et al., 1995). In summary, hippocampus volume declines with age, most likely even before onset of dementia. This decline is superimposed on developmental reductions of hippocampus volume. Parahippocampal gyrus volume declines with age in DS, this decline, however, seems to start from a developmentally relatively spared or even increased parahippocampal volume.
MRI Findings on Age Effects in Neocortical Areas
The most consistent age-related finding in DS subjects outside of the medial temporal lobe in cross-sectional studies was an increase of ventricular volume with age in demented elderly DS subjects (Ikeda and Arai, 2002; Kesslak et al., 1994). There are only few studies focusing on the onset and progression of neocortical atrophy in DS adults. Manual measures of total brain and gray matter volumes showed no significant atrophy before the onset of dementia (Kesslak et al., 1994; Pearlson et al., 1998; Raz, et al., 1995; Schapiro et al., 1989; 1992). However, demented DS subjects showed progressive atrophy of brain gray matter predominantly in temporal lobes, and widening of cerebrospinal fluid spaces in serial CT examinations (Ikeda and Arai, 2002; Lai and Williams, 1989; Schapiro et al., 1989). It has been suggested that significant brain atrophy occurs only when dementia becomes manifest in older DS subjects (Schapiro et al., 1989). Evidence from AD, however, suggests that regional atrophy precedes onset of clinical dementia not only in the hippocampus, but also neocortical brain regions (Fox et al., 2001; Karas et al., 2004; Pennanen et al., 2005). The lack of predementia neocortical atrophy in DS found in these earlier studies might be related to low sensitivity of the measures employed, particularly CT-based volumetry and visual ratings, a relatively narrow age-range, and small sample sizes.
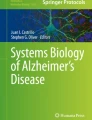
Recent studies have employed more sensitive markers to detect neocortical atrophy in predementia stages of DS. A potential marker of neocortical degeneration is the corpus callosum (Hampel et al., 2002a). The corpus callosum fibers originate from layer III and V pyramidal neurons in the cerebral cortex (Innocenti, 1986), which are early and specifically affected by AD-type pathology (Morrison et al., 1986; Pearson et al., 1985). Corpus callosum area is reduced both in postmortem examination (Weis et al., 1991a) and in in-vivo MRI studies (Hampel et al., 1998) in AD patients. Corpus callosum area correlates with measures of cortical dysfunction derived from PET and EEG, supporting the notion that corpus callosum atrophy can be used as a marker of neocortical neuronal degeneration in AD (Hampel et al., 2002a; Janowsky et al., 1996; Teipel et al., 1998, 1999, 2002b; Yamauchi, et al., 1993). On this basis, we determined corpus callosum atrophy in 34 DS subjects and 32 healthy control subjects. We found significant atrophy of the corpus callosum even before onset of dementia in DS adults (Teipel et al., 2003). The extent of corpus callosum atrophy in elder compared to younger DS subjects was comparable to that of hippocampus atrophy. The age-related decrease of corpus callosum was most pronounced in the splenium area, representing projections from posterior temporal, superior parietal and occipital cortex (De Lacoste et al., 1985). These findings suggest that loss of inter-hemispheric projecting neurons in posterior association cortex precedes the clinical onset of dementia in DS. Corpus callosum atrophy is a specific marker for the loss of intra-cortical projecting neurons, but has limited spatial resolution. Therefore, in a subsequent study, we used an automated voxel-based approach to determine the extent of regional cortical gray matter loss in predementia stages of DS (Teipel et al., 2004). In recent years, voxel-based morphometry (VBM) has been developed to search the entire brain for morphological changes (Ashburner and Friston, 2000). VBM is observer independent and automated, and therefore highly replicable. It allows for processing of a high number of scans within a relatively short time, and can detect morphological changes throughout the entire brain. Using VBM, we investigated age-related changes of gray matter volume within a DS group (Teipel et al., 2004). Gray matter maps were determined from volumetric T1 weighted MRI scans obtained in coronal orientation on a 1.5-T scanner (General Electric Signa II, Milwaukee). The protocol followed a modification of the previously established processing stream of VBM (Fig. 2) (Good et al., 2001). In a group of 32 DS subjects, age was significantly correlated with decline of cortical gray matter in parietal, frontal and occipital cortex (mainly lingual cortex), as well as temporal lobe and parahippocampal gyrus. The effects were most pronounced in superior parietal lobes, which agrees with the findings of predominant corpus callosum atrophy in the splenium receiving major projections from superior parietal lobes (Fig. 3).

Age-related reduction of cortical gray matter and corpus callosum area in non-demented DS subjects Upper row: Color coded map of significant negative correlations between gray matter and age projected on the normalized rendered brain surface from the MRI scan of a DS subject. Gray matter is significantly reduced with age in bilateral superior parietal lobes, prefrontal cortex and lateral temporal lobes, as well as medial temporal lobes (not shown) (Teipel et al., 2004). Lower row: Midsagittal section, outlining the corpus callosum. Age-related reductions are most pronounced in posterior corpus callosum (splenium) (Teipel et al., 2003). This area is known to receive major projections from posterior association cortex, particularly superior parietal lobes (De Lacoste et al., 1985).
This study only included subjects without dementia, from 25 up to 62 years of age. When cortical gray matter volumes were correlated with a test of verbal memory, decline in memory performance was correlated with reduced gray matter volume in left superior and middle temporal gyrus, bilateral precuneus, left hippocampus, right middle temporal gyrus, and right middle frontal gyrus. Therefore, even after controlling for age and general cognitive function, correlations between episodic memory and gray matter volume revealed brain areas which are thought to be associated with visual attention (precuneus) (Corbetta et al., 1995), episodic memory encoding (hippocampus) (Greicius et al., 2003; Squire and Zola-Morgan, 1991), episodic memory retrieval (right prefrontal cortex) (Lee, et al., 2000; Rugg et al., 2002) and language (left temporal pole, left lateral temporal cortex, including Wernike’s area) (Benson, 1988; Cabeza and Nyberg, 2000). These findings may indicate that impaired memory performance in the DS subjects is related to local morphological brain changes, most likely on the basis of developmental abnormalities or neurodegenerative changes or both. One has, however, to take into account that only non-demented subjects were included which led to a ceiling effect in the memory scores.
MRI findings on age-related brain changes in DS are summarized in Table II.
Interpretation of MRI Findings and Their Limitations
These findings suggest that, like in AD, regional brain atrophy, including hippocampus, parahippocampus, but also neocortical association areas, accompanies aging in DS and can be detected even before the onset of clinical dementia. The most likely substrate of these macroscopic changes are progressive AD-related pathological changes in the DS brain composed of tangle and plaque accumulation as well as synaptic and neuronal loss. These changes precede the onset of dementia in DS and can be detected in vivo using high resolution imaging techniques like hippocampus and corpus callosum volumetry as well as VBM.
There are, however, two caveats to be taken into account for the interpretation of these findings: First, DS is a developmental disorder and therefore any age related changes are superimposed on developmental abnormalities. This is well illustrated by a recent study (White et al., 2003) demonstrating morphological differences between adult non-demented DS subjects and healthy age matched controls using MRI and VBM. DS subjects had reduced gray matter volume in cerebellum, left medial frontal lobe, right superior and middle temporal lobe, and anterior and middle cingulated gyrus. This regional pattern of gray matter changes is clearly distinct from the age effects we found in the non-demented DS subjects using VBM (Teipel et al., 2004). It can, however, not be excluded that age effects are masked by higher variability of brain morphology in brain areas which are severely affected by developmental abnormalities. Second, the resemblance between DS and AD neuropathology is close, but not perfect. Plaque density was found to be higher in many DS subjects compared to AD patients and more widely distributed throughout the cortex (Hof et al., 1995). Additionally, results of several studies suggest cytoskeletal abnormalities in DS (Mann et al., 1989), and overexpression of proteins other than amyloid which may contribute to neurodegeneration (De La Torre et al., 1996; Engidawork and Lubec, 2001). Therefore, the possibility cannot be excluded that age-effects on cortical gray matter in non-demented DS subjects reflect at least partially DS-specific degenerative processes other than AD.
Summary and Perspectives
There is conclusive evidence for both, developmental abnormality of neuroanatomy and age associated brain atrophy in DS. An important task for future studies is the quantitative analysis of serial MRI examinations in non-demented elderly DS subjects followed over several years, some of them until conversion into dementia. These data would be very important to distinguish between developmental and age-associated (degenerative) alterations of brain morphology in DS. A wide range of cross-sectional studies, however, provides strong evidence for an independent contribution of age-associated neurodegeneration to progressive brain atrophy, particular in medial temporal lobes and posterior association cortex, the typical predilection areas of sporadic AD. Therefore, MRI investigation of brain aging in DS not only gives new insight in the onset and progression of neurodegenerative changes in DS, but also opens a window into the preclinical stages of AD. The finding of allocortical and neocortical brain atrophy in non-demented elderly DS subjects suggests that both allocortical and neocortical neuronal loss precedes the onset of clinical dementia in AD-type pathology. This has implications for our understanding of the onset of allocortical and neocortical neurodegeneration in AD. In particular, it supports the notion that treatment in AD should be initiated early in the course of the disease in order to rely on intact neuronal systems and even suggests that treatment should precede onset of clinical dementia. This will be even more important once disease modifying treatment approaches become available. From the diagnostic perspective, the findings on neocortical atrophy in predementia stages of DS-related AD suggest that structural MRI analysis should not only involve hippocampal, but also neocortical measures for the early detection of AD-related pattern of brain atrophy.
References
Alexander G. E., Saunders A. M., Szczepanik J., Strassburger T. L., Pietrini P., Dani A., et al. (1997). Relation of age and apolipoprotein E to cognitive function in Down syndrome adults. Neuroreport 8:1835–1840
Ashburner J. and Friston K. J. (2000). Voxel-based morphometry–the methods. Neuroimage. 11:805–821
Aylward E. H., Li Q., Honeycutt N. A., Warren A. C., Pulsifer M. B., Barta P. E., et al. (1999). MRI volumes of the hippocampus and amygdala in adults with Down’s syndrome with and without dementia. Am. J. Psychiatry. 156:564–568
Becker L., Mito T., Takashima S. and Onodera K. (1991a). Growth and development of the brain in Down syndrome. In: Epstein C., (eds) The Morphogenesis of Down Syndrome. New York, Wiley-Liss, pp. 133–152
Becker L., Mito T., Takashima S. and Onodera K. (1991b). Growth and development of the brain in Down syndrome. Prog. Clin. Biol. Res. 373:133–152
Benson D. F. (1988). Classical syndromes of aphasia. In: Foller F., Grafman J., (eds) Handbook of Neuropsychology. Amsterdam, Elsevier
Bobinski M., de Leon M. J., Wegiel J., Desanti S., Convit A., Saint Louis L. A., et al. (2000). The histological validation of post mortem magnetic resonance imaging- determined hippocampal volume in Alzheimer’s disease. Neuroscience 95:721–725
Bokde A. L., Teipel S. J., Zebuhr Y., Leinsinger G., Gootjes L., Schwarz R., et al. (2002). A new rapid landmark-based regional MRI segmentation method of the brain. J. Neurol. Sci. 194:35–40
Bookstein F. L. (2001). “Voxel-based morphometry” should not be used with imperfectly registered images. Neuroimage. 14:1454–1462
Braak H., Griffing K. and Braak E. (1997). Neuroanatomy of Alzheimer’s disease. Alzheimer’s Research 3:235–247
Cabeza R. and Nyberg L. (2000). Imaging cognition II: An empirical review of 275 PET and fMRI studies. J. Cogn. Neurosci. 12:1–47
Chetelat G. and Baron J. C. (2003). Early diagnosis of Alzheimer’s disease: contribution of structural neuroimaging. Neuroimage 18:525–541
Corbetta M., Shulman G. L., Miezin F. M. and Petersen S. E. (1995). Superior parietal cortex activation during spatial attention shifts and visual feature conjunction. Science 270:802–805
Coyle J. T., Oster-Granite M. L. and Gearhart J. D. (1986). The neurobiologic consequences of Down syndrome. Brain Res. Bull. 16:773–787
De La Torre R., Casado A., Lopez-Fernandez E., Carrascosa D., Ramirez V. and Saez J. (1996). Overexpression of copper-zinc superoxide dismutase in trisomy 21. Experientia 52:871–873
De Lacoste M. C., Kirkpatrick J. B. and Ross E. D. (1985). Topography of the human corpus callosum. J. Neuropath. Exper. Neurol. 44:578–591
Engidawork E. and Lubec G. (2001). Protein expression in Down syndrome brain. Amino Acids 21:331–361
Evenhuis H. M. (1990). The natural history of dementia in Down’s syndrome. Arch. Neurol. 47:263–267
Fox N. C., Crum W. R., Scahill R. I., Stevens J. M., Janssen J. C. and Rossor M. N. (2001). Imaging of onset and progression of Alzheimer’s disease with voxel-compression mapping of serial magnetic resonance images. Lancet 358:201–205
Frangou S., Aylward E., Warren A., Sharma T., Barta P. and Pearlson G. (1997). Small planum temporale volume in Down’s syndrome: a volumetric MRI study. Am. J. Psychiatry. 154:1424–1429
Frisoni G. B., Scheltens P., Galluzzi S., Nobili F. M., Fox N. C., Robert P. H., et al. (2003). Neuroimaging tools to rate regional atrophy, subcortical cerebrovascular disease, and regional cerebral blood flow and metabolism: consensus paper of the EADC. J. Neurol. Neurosurg. Psychiat. 74:1371–1381
Good C. D., Johnsrude I. S., Ashburner J., Henson R. N., Friston K. J. and Frackowiak R. S. (2001). A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage 14:21–36
Greicius M. D., Krasnow B., Boyett-Anderson J. M., Eliez S., Schatzberg A. F., Reiss A. L., et al. (2003). Regional analysis of hippocampal activation during memory encoding and retrieval: fMRI study. Hippocampus 13:164–174
Hampel H., Teipel S. J., Alexander G. E., Horwitz B., Teichberg D., Schapiro M. B., et al. (1998). Corpus callosum atrophy is a possible indicator of region- and cell type-specific neuronal degeneration in Alzheimer disease: a magnetic resonance imaging analysis. Arch. Neurol. 55:193–198
Hampel H., Teipel S. J., Alexander G. E., Pogarell O., Rapoport S. I. and Moller H. J. (2002a). In vivo imaging of region and cell type specific neocortical neurodegeneration in Alzheimer’s disease Perspectives of MRI derived corpus callosum measurement for mapping disease progression and effects of therapy. Evidence from studies with MRI, EEG and PET. J. Neural. Transm. 109:837–855
Hampel H., Teipel S. J., Bayer W., Alexander G. E., Schwarz R., Schapiro M. B., et al. (2002b). Age transformation of combined hippocampus and amygdala volume improves diagnostic accuracy in Alzheimer’s disease. J. Neurol. Sci. 194:15–19
Hof P. R., Bouras C., Perl D. P., Sparks D. L., Mehta N. and Morrison J. H. (1995). Age-related distribution of neuropathologic changes in the cerebral cortex of patients with Down’s syndrome. Quantitative regional analysis and comparison with Alzheimer’s disease. Arch. Neurol. 52:379–391
Hyman B. T., West H. L., Rebeck G. W., Lai F. and Mann D. M. (1995). Neuropathological changes in Down’s syndrome hippocampal formation. Effect of age and apolipoprotein E genotype. Arch. Neurol. 52:373–378
Ikeda M. and Arai Y. (2002). Longitudinal changes in brain CT scans and development of dementia in Down’s syndrome. Eur. Neurol. 47:205–208
Ikeda S., Yanagisawa N., Allsop D. and Glenner G. G. (1989). Evidence of amyloid beta-protein immunoreactive early plaque lesions in Down’s syndrome brains. Lab. Invest. 61:133–137
Innocenti G. M. (1986). General organization of callosal connections in the cerebral cortex. In: Jones E. G., Peters A., (eds) Cerebral Cortex: Sensory Motor Areas and Aspects of Cortical Connectivity. New York NY, Plenum Publishing Corp., pp. 291–353
Jack C. R., Jr., Dickson D. W., Parisi J. E., Xu Y. C., Cha R. H., O’Brien P. C., et al. (2002). Antemortem MRI findings correlate with hippocampal neuropathology in typical aging and dementia. Neurology 58:750–757
Janowsky J. S., Kaye J. A. and Carper R. A. (1996). Atrophy of the corpus callosum in Alzheimer’s disease versus healthy aging. J. Am. Ger. Soc. 44:798–803
Jellinger K. A. and Bancher C. (1998). Neuropathology of Alzheimer’s disease: a critical update. J Neural. Transm. Suppl. 54:77–95
Jernigan T. L., Bellugi U., Sowell E., Doherty S. and Hesselink J. R. (1993). Cerebral morphologic distinctions between Williams and Down syndromes. Arch. Neurol. 50:186–191
Karas G. B., Scheltens P., Rombouts S. A., Visser P. J., van Schijndel R. A., Fox N. C., et al. (2004). Global and local gray matter loss in mild cognitive impairment and Alzheimer’s disease. Neuroimage 23:708–716
Kesslak J. P., Nagata S. F., Lott I. and Nalcioglu O. (1994). Magnetic resonance imaging analysis of age-related changes in the brains of individuals with Down’s syndrome. Neurology 44:1039–1045
Krasuski J.S., Alexander G.E., Horwitz B., Rapoport S.I. and Schapiro M.B. (2002). Relation of medial temporal lobe volumes to age and memory function in nondemented adults with Down’s syndrome: implications for the prodromal phase of Alzheimer’s disease. Am. J. Psychiatry 159:74–81
Lawlor B. A., McCarron M., Wilson G. and McLoughlin M. (2001). Temporal lobe-oriented CT scanning and dementia in Down’s syndrome. Int. J. Geriatr. Psychiatry 16:427–429
Lawlor B. A., McCarron M., Wilson G. and McLoughlin M. (2001). Temporal lobe-oriented CT scanning and dementia in Down’s syndrome. Int. J. Geriatr. Psychiatry 16:427–429
Lee A. C., Robbins T. W. and Owen A. M. (2000). Episodic memory meets working memory in the frontal lobe: functional neuroimaging studies of encoding and retrieval. Crit. Rev. Neurobiol. 14:165–197
Mann D. M. (1988). The pathological association between Down syndrome and Alzheimer disease. Mech. Ageing Dev. 43:99–136
Mann D. M. and Esiri M. M. (1989). The pattern of acquisition of plaques and tangles in the brains of patients under 50 years of age with Down’s syndrome. J. Neurol. Sci. 89:169–179
Mann D. M., Prinja D., Davies C. A., Ihara Y., Delacourte A., Defossez A., et al. (1989). Immunocytochemical profile of neurofibrillary tangles in Down’s syndrome patients of different ages. J. Neurol. Sci. 92:247–260
Mann D. M. A., Yates P. O. and Marcyniuk B. (1984). Alzheimer’s presenile dementia, senile dementia of Alzheimer type and Down’s syndrome in middle age form an age related continuum of pathological changes. Neuropath. Appl. Neurobiol. 10:185–207
Mesulam M. (2004). The cholinergic lesion of Alzheimer’s disease: pivotal factor or side show? Learn. Mem. 11:43–49
Morrison J. H., Scherr S., Lewis D. A., Campbell M. J. and Bloom F. E. (1986). The laminar and regional distribution of neocortical somatostatin and neuritic plaques: implications for Alzheimer’s disease as a global neocortical disconnection syndrome. In: Scheibel A. B., Weschler A. F., (eds) The Biological Substrates of Alzheimer’s Disease. New York, NY, Academic Press, pp. 115–131
Nagy Z., Hindley N. J., Braak H., Braak E., Yilmazer-Hanke D. M., Schultz C., et al. (1999). The progression of Alzheimer’s disease from limbic regions to the neocortex: clinical, radiological and pathological relationships. Dement. Geriatr. Cogn. Disord. 10:115–120
Nagy Z., Jobst K. A., Esiri M. M., Morris J. H., King E. M.-F., MacDonald B., et al. (1996). Hippocampal pathology reflects memory deficit and brain imaging measurements in Alzheimer’s disease: clinicopathological correlations using three sets of pathologic diagnostic criteria. Dementia 7:76–81
Pearlson G. D., Breiter S. N., Aylward E. H., Warren A. C., Grygorcewicz M., Frangou S., et al. (1998). MRI brain changes in subjects with Down syndrome with and without dementia. Dev. Med. Child Neurol. 40:326–334
Pearson R. C. A., Esiri M. M., Hiorns R. W., Wilcock G. K. and Powell T. P. S. (1985). Anatomical correlates of the distribution of the pathological changes in the neocortex in Alzheimer’s disease. Proc. Natl. Acad. Sci. USA. 82:4531–4534
Pennanen C., Testa C., Laakso M. P., Hallikainen M., Helkala E. L., Hanninen T., et al. (2005). A voxel based morphometry study on mild cognitive impairment. J. Neurol. Neurosurg. Psychiatry. 76:11–14
Pinter J. D., Brown W. E., Eliez S., Schmitt J. E., Capone G. T. and Reiss A. L. (2001a). Amygdala and hippocampal volumes in children with Down syndrome: a high-resolution MRI study. Neurology 56:972–974
Pinter J. D., Eliez S., Schmitt J. E., Capone G. T. and Reiss A. L. (2001b). Neuroanatomy of Down’s syndrome: a high-resolution MRI study. Am. J. Psychiatry 158:1659–1665
Raz N., Torres I. J., Briggs S. D., Spencer W. D., Thornton A. E., Loken W. J., et al. (1995). Selective neuroanatomic abnormalities in Down’s syndrome and their cognitive correlates: evidence from MRI morphometry. Neurology 45:356–366
Rugg M. D., Otten L. J. and Henson R. N. (2002). The neural basis of episodic memory: evidence from functional neuroimaging. Philos. Trans. R. Soc. Lond. B Biol. Sci. 357:1097–1110
Rumble B., Retallack R., Hilbich C., Simms G., Multhaup G., Martins R., et al. (1989). Amyloid A4 protein and its precursor in Down’s syndrome and Alzheimer’s disease. N. Engl. J. Med. 320:1446–1452
Sadowski M., Wisniewski H. M., Tarnawski M., Kozlowski P. B., Lach B. and Wegiel J. (1999). Entorhinal cortex of aged subjects with Down’s syndrome shows severe neuronal loss caused by neurofibrillary pathology. Acta Neuropathol. 97:156–164
Schapiro M. B., Haxby J. V. and Grady C. L. (1992). Nature of mental retardation and dementia in Down syndrome: study with PET, CT, and neuropsychology. Neurobiol. Aging 13:723–734
Schapiro M. B., Luxenberg J. S., Kaye J. A., Haxby J. V., Friedland R. P. and Rapoport S. I. (1989). Serial quantitative CT analysis of brain morphometrics in adult Down’s syndrome at different ages. Neurology 39:1349–1353
Schmidt-Sidor B., Wisniewski K. E., Shepard T. H. and Sersen E. A. (1990). Brain growth in Down syndrome subjects 15 to 22 weeks of gestational age and birth to 60 months. Clin. Neuropathol. 9:181–190
Smith A. D. (2002). Commentary: Imaging the progression of Alzheimer pathology through the brain. PNAS 99:4135–4137
Squire L.R. and Zola-Morgan S. (1991). The medial temporal lobe memory system. Science 253:1380–1386
Talairach J. and Tournoux P. (1988). Co-Planar Stereotaxic Atlas of the Human Brain. New York, Thieme
Teipel S. J., Alexander G. E., Schapiro M. B., Moller H. J., Rapoport S. I. and Hampel H. (2004). Age-related cortical grey matter reductions in non-demented Down’s syndrome adults determined by MRI with voxel-based morphometry. Brain 127:811–824
Teipel S. J., Bayer W., Alexander G. E., Zebuhr Y., Teichberg D., Kulic L., et al. (2002a). Progression of corpus callosum atrophy in Alzheimer disease. Arch. Neurol. 59:243–248
Teipel S. J., Bayer W., Alexander G. E., Zebuhr Y., Teichberg D., Kulic L., et al. (2002b). Progression of Corpus Callosum Atrophy in Alzheimer’s disease. Arch. Neurol. 59:243–248
Teipel S. J., Flatz W. H., Heinsen H., Bokde A. L. W., Schoenberg S. O., Stöckel S., et al. (2005). Measurement of basal forebrain atrophy in AD using MRI. Brain 128:2626–2644
Teipel S. J., Hampel H., Alexander G. E., Schapiro M. B., Horwitz B., Teichberg D., et al. (1998). Dissociation between white matter pathology and corpus callosum atrophy in Alzheimer’s disease. Neurology 51:1381–1385
Teipel S. J., Hampel H., Pietrini P., Alexander G. E., Horwitz B., Daley E., et al. (1999). Region specific corpus callosum atrophy correlates with regional pattern of cortical glucose metabolism in Alzheimer’s disease. Arch. Neurol. 56:467–473
Teipel S. J., Schapiro M. B., Alexander G. E., Krasuski J. S., Horwitz B., Hoehne C., et al. (2003). Relation of corpus callosum and hippocampal size to age in nondemented adults with Down’s syndrome. Am. J. Psychiatry 160:1870–1878
Vassar R. (2005). beta-Secretase, APP and Abeta in Alzheimer’s disease. Subcell. Biochem. 38:79–103
Wang P. P., Doherty S., Hesselink J. R. and Bellugi U. (1992). Callosal morphology concurs with neurobehavioral and neuropathological findings in two neurodevelopmental disorders. Arch. Neurol. 49:407–411
Weis S., Jellinger K. and Wenger E. (1991a). Morphometry of the corpus callosum in normal aging and Alzheimer’s disease. J. Neural. Transm. 33[Suppl]: 35–38
Weis S., Weber G., Neuhold A. and Rett A. (1991b). Down Syndrome: MR quantification of brain structures and comparison with normal control subjects. AJNR 12:1207–1211
White N. S., Alkire M. T. and Haier R. J. (2003). A voxel-based morphometric study of nondemented adults with Down Syndrome. Neuroimage 20:393–403
Wisniewski K. E. (1990). Down syndrome children often have brain with maturation delay, retardation of growth, and cortical dysgenesis. Am. J. Med. Genet. Suppl. 7:274–281
Wisniewski K. E., Dalton A. J., McLachlan C., Wen G. Y. and Wisniewski H. M. (1985a). Alzheimer’s disease in Down’s syndrome: clinicopathologic studies. Neurology 35: 957–961
Wisniewski K. E., Wisniewski H. M. and Wen G. Y. (1985b). Occurrence of neuropathological changes and dementia of Alzheimer’s disease in Down’s syndrome. Ann. Neurol. 17:278–282
Yamauchi H., Fukuyama H., Harada K., Nabatame H., Ogawa M., Ouchi Y., et al. (1993). Callosal atrophy parallels decreased cortical oxygen metabolism and neuropsychological impairment in Alzheimer’s disease. Arch. Neurol. 50:1070–1074
Yoshimura N., Kubota S., Fukushima Y., Kudo H., Ishigaki H. and Yoshida Y. (1990). Down’s syndrome in middle age. Topographical distribution and immunoreactivity of brain lesions in an autopsied patient. Acta Pathol. Jpn. 40:735–743
Acknowledgments
We thank Dr. Michael Ewers (LMU Munich) for critical reading of the manuscript. Part of this work was supported by grants of the Medical Faculty of the Ludwig–Maximilian University (Munich, Germany) to S.J.T., of the Hirnliga e. V. (Nürmbrecht, Germany) to S.J.T. and H.H., and by the German Competency Network on Dementias (Kompetenznetz Demenzen) funded by the Bundesministerium für Bildung und Forschung (BMBF), Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Teipel, S.J., Hampel, H. Neuroanatomy of Down Syndrome in vivo: A Model of Preclinical Alzheimer’s Disease. Behav Genet 36, 405–415 (2006). https://doi.org/10.1007/s10519-006-9047-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10519-006-9047-x