
Abstract
Racial homophily (partnering with those of the same race) has been suggested as contributing to racial disparities in HIV among gay and bisexual men (GBM). Using a daily diary study, we examined racial homophily and its role in anal sexual behaviors in a sample of highly sexually active Black, White, and Latino GBM (N = 294, n = 3107 sexual events). In general, (1) men tended to partner with others of the same race, (2) HIV was more prevalent among men of color, and (3) race acted independent of whether one would engage in behaviors that would put them at highest risk for transmitting HIV (i.e., no main or interaction effects for insertive condomless anal sex (CAS) among HIV-positive men, and no main or interaction effects for receptive CAS among HIV-negative men). There were some main and interactive effects observed for lower risk behaviors (receptive CAS among HIV-positive men and insertive CAS among HIV-negative). Our findings suggest that racial disparities in HIV may be due to a higher exposure frequency (i.e., the frequency with which one comes into contact with a partner where a transmission could occur). However, men were also less likely to have anal sex when having sex with someone of the same race—a finding that works against the premise of higher exposure frequency. Future researchers should examine both racial homophily as well as variation in sexual behavior based on same-race or different-race partnerships.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
HIV continues to be a public health crisis among gay, bisexual, and other men who have sex with men (GBMSM) (CDC, 2015a, b). HIV incidence among GBMSM increased by 12 % from 27,668 in 2009 to 31,023 in 2013 (CDC, 2015c). Stall et al. (2009) described the inability to reduce the number of new infections as “running in place.” This phenomenon seems particularly relevant to men of color, for whom there have been clear and consistent racial disparities in HIV incidence that have been negatively impacting them for more than a decade (Clerkin, Newcomb, & Mustanski, 2011; Marks et al., 2008; Millett, Flores, Peterson, & Bakeman, 2007; Newcomb & Mustanski, 2013). Between 2009 and 2013, the estimated percentage of GBMSM diagnosed with HIV that were White decreased from 34 to 32 %, while the percentage of GBMSM diagnosed with HIV that were Latino increased from 23 to 24 %, and the percentage among those that were Black increased from 38 to 39 % (CDC, 2015c). To put this into perspective, 77.7 % of the US population is White, compared with only 13.2 % Black and 17.1 % Latino (US Census Bureau, 2015).
The racial composition of gay and bisexual men’s sexual networks has been suggested to contribute to racial disparities in HIV transmission (Clerkin et al., 2011; Fujimoto & Williams, 2015; Grov, Saleh, Lassiter, & Parsons, 2015a; Mustanski, Birkett, Kuhns, Latkin, & Muth, 2015; Newcomb & Mustanski, 2013). These disparities are thought to be the result of racial homophily, which refers to partnering with men who are the same race as you. In a study of GBMSM in New York City, Grov et al. (2015a) found that, among men in relationships, 61 % of Black men said their partners were also Black and 71 % of White men said their partner was also White. Latino men appeared to be the most diverse with regard to partners’ race, but they still partnered with other Latino men at higher rates than other groups (e.g., 44 % of Latino men said their partner was also Latino compared with only 16.9 %). Raymond and McFarland (2009), using a cross-sectional survey of GBMSM in San Francisco, reported that Black MSM had a threefold higher level of same race sexual partnering than would be expected by chance alone. In an online prospective diary study of GBMSM, Newcomb and Mustanski (2013) found that Black men reported significantly less unprotected sex than other groups, yet were the most racially homophilous group in terms of sexual partnerships. Mustanski et al. (2015), in a network study of young GBMSM, found no racial differences in individual engagement in HIV risk behaviors or concurrent sexual partnership. Instead, network characteristics showed racial differences, including sexual network density and assortativity by race. They concluded that most racial differences were in the direction of effects that would tend to increase HIV incidence among Black GBMBM and that racial disparities in HIV may be driven and/or maintained by a combination of racial differences in assortativity by race and increased sexual network density, rather than differences in individual’s HIV risk behaviors.
Greater racial homophily functions to increase an individual’s risk of HIV exposure if he is a member of a racial group with higher disease burden (i.e., greater prevalence among men of color) while simultaneously decreasing transmission risk for members of racial groups with lower prevalence (i.e., among White men). That is, in spite of data suggesting that men of color actually engage in equivalent or lower levels of HIV risk behavior than their White peers (Millett et al., 2007; Taylor et al., 2012), the potential for exposure to HIV is higher and may be driven, in part, by racially homophilous sexual networking (Clerkin et al., 2011; Mustanski et al., 2015).
A probability-based sample of urban GBMSM (Stall et al., 2002, 2003) in four U.S. cities found that sexually active men reported on average two to three male partners in 90 days prior to assessment. For the purpose of this study, we defined highly sexually active as having a minimum of nine male partners in the prior 90 days—roughly three times the average. Highly sexually active GBMSM are a critical population to both study in terms of factors associated with HIV and STI transmission risk behavior as well as develop tailored HIV prevention interventions. As a result of the sheer frequency in which they engage in sex, they have high potential to expose others to pathogens as well as become infected themselves. Yet, to our knowledge, no studies have examined racial homophily among highly sexually active gay and bisexual men. Furthermore, and to our knowledge, no such studies have examined the ways in which sexual behavior itself may change based on whether one is partnering with someone of the same or a different race. That is, given radicalized stereotypes regarding the sexual behavior particularly of racial and ethnic minorities (for a review, see Grov et al., 2015a; Lick & Johnson, 2015), we know little about whether GBMSMs’ sexual behavior varies based on whether they are with a partner of a same or different race.
To that end, we examined both racial homophily as well as its role in anal sexual behaviors based on whether one is with a same-race or different-race partner. Data were taken from a prospective daily diary study with a diverse sample of highly sexually active HIV-positive and HIV-negative GBM. The results of this study seek to add to our understanding of factors that contribute to racial disparities in HIV among GBM.
Method
Participants
Analyses for this manuscript were conducted on data from Pillow Talk, a study of highly sexually active (i.e., ≥9 male partners in 90 days) GBM in New York City (NYC) (Parsons et al., 2013). For the purposes of this project, we operationalized highly sexually active as having at least 9 sexual partners in the 90 days prior to enrollment. This entry criterion was based on prior research (Grov, Parsons, & Bimbi, 2010b; Parsons, Bimbi, & Halkitis, 2001; Parsons et al., 2008), including the aforementioned probability-based sample of urban GBMSM (Stall et al., 2002, 2003) that found nine partners were 2–3 times the average number of sexual partners among sexually active GBMSM. Recruitment and study procedures have been described elsewhere (Grov, Whitfield, Rendina, Ventuneac, & Parsons, 2015b; Parsons et al., 2013; Parsons, Rendina, Ventuneac, Moody, & Grov, 2015b; Parsons, Rendina, Ventuneac, Moody, & Grov, 2015c; Ventuneac, Rendina, Grov, Mustanski, & Parsons, 2015). In brief, we utilized a combination of recruitment strategies: (1) respondent-driven sampling; (2) Internet-based advertisements on social and sexual networking Web sites; (3) e-mail blasts through New York City gay sex party listservs; and (4) active recruitment in New York City venues such as gay bars/clubs, concentrated gay neighborhoods, and ongoing gay community events.
Enrollment began in February 2011 and closed in June 2013, during which time the project enrolled 376 men, 208 (55.2 %) of who were confirmed to be HIV-negative with a rapid HIV antibody test during their assessment. HIV-positive participants provided proof of serostatus (e.g., HIV medication bottle/prescription with their name). For the present study, we examined data from the 316 White, Black, and Latino men. Due to the small number of men from other races combined with the difficulty of determining same-race versus different-race partnerships among men of multiple races, these participants (n = 60) were not included in the present analyses. Of 316 men, two participants did not complete the CASI assessment and thus were missing demographic data, three did not complete the online daily diary, and 17 provided diary data but reported no sexual events. As such, the final analytic sample included 294 men (White n = 181, 61.6 %, Black n = 66, 22.4 %, and Latino n = 47, 16.0 %).
Procedure
To be eligible, participants had to: be at least 18 years of age; be biologically male and self-identified as male; report nine or more male sexual partners in the prior 90 days; be self-identified as gay, bisexual, or some other non-heterosexual identity (e.g., queer); and have daily access to the Internet (in order to complete the at-home daily diary). Participants completed a 1-h at-home online computer-assisted self-interview (CASI) followed by an in-person assessment. Final eligibility and enrollment were confirmed during the in-person appointment. The data for this paper were collected as part of the CASI conducted at home as well as a prospective online daily diary. Participants received a link to complete their diaries starting on the first day following their baseline appointment and continuing for 30 days. Unique links were e-mailed to participants at 8 pm each night, and participants were given until 10 a.m. the following morning to complete the survey before the link expired. All procedures were reviewed and approved by the Institutional Review Board of the City University of New York.
Measures
Online CASI Measures
Participants reported demographic characteristics, including sexual identity, age, race/ethnicity, education, and relationship status.
Daily Diary Measures
The diary measure was based on previous studies conducted with GBM (Grov, Golub, Mustanski, & Parsons, 2010a; Mustanski, 2007) and has been described in more detail elsewhere (Parsons, Rendina, Grov, Ventuneac, & Mustanski, 2015a; Rendina, Moody, Grov, Ventuneac, & Parsons, 2015). Each day, participants were asked whether they had engaged in any sexual activity with another person and, if so, were asked a series of questions for each partner they reported for that day (up to four unique partners per day). Participants indicated whether this person was a main partner or a casual partner as well as race or ethnicity they perceived this person to be (Black/African-American, Latino/Hispanic, Asian/Pacific Islander, White/European, Indian (not Native American), Middle Eastern, Native American/Alaskan Native, multiracial/multiethnic, unknown). In addition, participants indicated if they engaged in anal sex with this person, whether the sex was insertive and/or receptive, and whether a condom was used during the insertive and/or receptive anal sex. Participants also indicated the HIV serostatus of that partner: My partner told me he is HIV-positive (original emphasis), I think this partner is HIV-positive, I do not know this partner’s HIV status, I think this partner is HIV-negative, and my partner told me he is HIV-negative (original emphasis). Serconcordance was determined as having been told by the partner that he was the same HIV status as the participant. All other responses were coded as serodiscordant. For the present analyses, only sexual events with casual male partners were utilized (n = 3107 events). Please note there were 42 events recorded with a non-male casual partner, of which 22 were with cisgender females, 16 with transgender females, and 4 with transgender males. Moreover, these events occurred across only 14 participants, with half of them (n = 21) reported by a single participant. As a result, there were an insufficient number of cases to meaningfully analyze these data.
Participants’ partners were coded as being the same or a different race from the participant based on the participants’ perception of the partner’s (e.g., partners of Black participants who were perceived to be Black were coded as same race, while those perceived to be White were coded as a different race). For Latino participants who also identified themselves with a Black racial background, partners perceived to be Black or Latino were coded as partners of the same race. We had no additional data on partners coded as multiracial; thus, those partners were coded as being a different race from the participant. It is worth noting that there were 9 participants who identified as both Latino and Black and were coded as Latino—among them, there were 49 sex events recorded, with 19 partners being identified as Black and 12 as Latino, all of whom were coded as the same race as the participant. Three of the partners were identified as multiracial and the remaining 15 were identified as some other race, and all of these were coded as a different race than the participant.
Analytic Plan
We performed a series of generalized linear mixed models in SPSS version 22 to investigate a series of variables. We utilized a binomial outcome with a logit link across models, specifying a random intercept with an unstructured covariance matrix. Following an initial set of models run on the full sample in which we compared HIV-positive with HIV-negative men, all models were split by HIV status and run identically. All models were adjusted for whether or not the sexual partner was a new (i.e., first time) versus regular casual partner and whether the partner was known to be HIV-positive (i.e., seroconcordant). Variables of interest included a main effect of participant race at Level 2, a main effect of partner’s race (same vs different) at Level 1, and a cross-level interaction between participant and partner race, with White race serving as the referent category for participants and different race serving as the referent for partners. In total, we explored seven variations of dependent variables.
-
Model 1: Was the partner of the same race as the participant? (ref = no)
-
Model 2: Was the partner the same HIV status as the participant? (ref = no)
-
Model 3: Did the participant engage in any anal sex with the partner during this event? (ref = no)
-
Models 4 and 8: Did the participant engage in any receptive anal sex with the partner during this event? (ref = no)
-
Models 5 and 9: Did the participant engage in any insertive anal sex with the partner during this event? (ref = no)
-
Models 6 and 10: Did the participant engage in any condomless receptive anal sex with the partner during this event? (ref = no)
-
Models 7 and 11: Did the participant engage in any condomless insertive anal sex with the partner during this event? (ref = no)
Results
As shown in Table 1, 42.5 % of participants were HIV-positive, most were gay-identified, employed, college educated, and single. The average age was 37.6. The average number of diary surveys completed per participant was 22.1 (Mdn = 25.0, SD = 7.63), resulting in an average completion rate of 74 % and a median completion rate of 83 %. There were no significant differences in the probability of diary completion on a given day by HIV status nor by race or ethnicity. Overall, participants reported that 18.4 % (n = 571) of their male partners were Black, 22.5 % (n = 698) were Latino, 46.6 % (n = 1447) were White, 3.6 % (n = 111) were multiracial, 7.9 % (n = 245) were another race, and 1.1 % (n = 35) were of unknown racial/ethnic background. There were no significant racial or ethnicity differences in the odds of sexual activity with a casual partner on a given day. Of the sexual events recorded, 21.6 % (n = 671) were from Black participants, 12.1 % (n = 377) from Latino participants, and 66.3 % (n = 2059) from White participants.
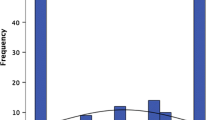
The first model in Table 2 displays the results of an analysis examining the relative prevalence of same- versus different-race partners by participant’s race, and Fig. 1 displays these findings graphically. There was evidence of racial homophily for all three groups. On average, White men partnered with other White men 56.4 % of the time, Black men partnered with other Black men 35.5 % of the time, and Latino men partnered with Latino men 33.3 % of the time. The 2010 NYC census data indicate that 44.0 % of New Yorkers are White, 25.5 % are Black, and 28.6 % are Latino, suggesting all racial groups are having sex with a greater proportion of men from their own race than would be expected based on sheer availability (U.S. Census Bureau, 2010). That is, were participant’s race is independent of their partners (i.e., selected at random), one would expect lower levels of same-race partnering for all three groups.

Homophily in sexual partnerships among Black, White, and Latino gay and bisexual men
Table 2 also presents a series of multilevel models examining the influence of participant race, partner race, and their interaction on sexual behavior. As shown in Model 2, neither participant nor partner race was significantly associated with whether or not the partner was of the same HIV status as the participant. As can be seen within Model 3, Latino participants had significantly higher odds of having anal sex than White participants, and across all participants, being with a same-race partner was associated with significantly lower odds of engaging in anal sex.
Behavior Among HIV-Positive Participants
We next review intersection of same- versus different-race partnerships on sexual behaviors separately for HIV-positive and HIV-negative participants.
Table 3 displays the results of four models examining the role of participant and partner race on receptive and insertive anal sex as well as receptive and insertive CAS for HIV-positive participants only. In Model 4, the dependent variable is receptive anal sex (i.e., bottoming). There was no effect of participant race (i.e., Black, White, and Latino men were equally likely to bottom overall), but being with a same-race partner significantly decreased the odds that participants bottomed. There was a significant interaction between participant and partner race for Black men, suggesting that Black men had higher odds than White men of bottoming when with a same-race partner.
In Model 5, the dependent variable is insertive anal sex (i.e., topping). The only significant finding with regard to race was that Black participants had higher odds than White participants of topping in general.
In Model 6, the dependent variable is receptive CAS. The model showed similar findings as were found for receptive sex in general (i.e., Model 4) and is plotted in Fig. 2. Black participants had lower odds of engaging in receptive CAS than White participants, but had significantly greater odds than White participants of engaging in receptive CAS when with a same-race partner.

HIV-positive participants. Black participants had lower odds of engaging in receptive CAS than White participants, but had significantly greater odds than White participants of engaging in receptive CAS with a same-race partner. There were no significant racial differences regarding insertive CAS
In Model 7, the dependent variable is insertive CAS. There were no significant racial differences regarding insertive CAS.
Behavior Among HIV-Negative Participants
Table 4 displays the results of the same analyses among the HIV-negative participants in the sample. Overall, we found no significant impact of participant or partner race or any interaction between the two for any of the four outcomes. However, marginally significant results for topping in Model 9 suggest that Black and Latino participants have somewhat higher odds than White participants of topping. Further, a marginally significant result in Model 11 regarding insertive CAS suggested that Latino men had somewhat higher odds than White men of engaging in insertive CAS when with a same-race partner (see Fig. 3). It is worth noting that, due to the low frequency of CAS among HIV-negative participants, there was less power to detect differences in these models compared to those in Table 3.

HIV-negative participants. No significant impact of participant or partner race on receptive CAS. A marginally significant result regarding insertive CAS suggested that Latino men had somewhat higher odds than White men of engaging in insertive CAS when with a same-race partner
Discussion
To our knowledge, this is the first study to examine racial homophily in the sexual partnerships of highly sexually active GBM, as well as its role in anal sexual behavior. As a population, highly sexually active individuals are of critical interest because they are centered at the nexus of large sexual networks and thus of critical importance for understanding the transmission of both HIV and STIs. For Black, White, and Latino men, there was evidence of racial homophily, suggesting that men partner with other men who are the same race at greater rates than would be expected were partners selected at random (i.e., if partner’s race was independent of participant’s), which is consistent with prior research (Clerkin et al., 2011; Grov et al., 2015a; Newcomb & Mustanski, 2013; Raymond & McFarland, 2009). Racial homophily in sexual partnering has been suggested to contribute to the high rates of HIV in minority communities (Clerkin et al., 2011; Fujimoto & Williams, 2015; Mustanski et al., 2015; Newcomb & Mustanski, 2013); however, this may work in two directions. For men of color, racial homophily may further drive racial disparities in HIV because of the higher community burden of STIs—which are known to facilitate easier HIV acquisition—and higher HIV prevalence already present among Black and Latino MSM communities (CDC, 2015a, b; Hogben & Leichliter, 2008; Mustanski et al., 2015; Raymond & McFarland, 2009; Sullivan et al., 2014). Meanwhile, for White men, racial homophily may help to decrease HIV exposure due to HIV’s lower prevalence among White GBM relative to GBM of color. Nevertheless, although men tended to partner with those who were the same race at rates that were higher than what would be expected were men choosing partners at random, being with a same-race partner was associated with significantly lower odds of engaging in anal sex, which would appear to contradict the argument of higher HIV exposure potential among men of color.
To further understand the role of participant’s race and his partner’s in anal sexual behavior, we assessed the role of racial homophily on CAS separately for HIV-positive and HIV-negative men. Prior studies investigating racial homophily among MSM using daily diaries or social networking analysis have not analyzed HIV-positive MSM separately from HIV-negative men (Mustanski et al., 2015) or excluded HIV-positive men (Newcomb & Mustanski, 2013). Thus, to our knowledge, this is the first study to investigate racial homophily across HIV statuses. We found main and interaction effects of participant and partner race on receptive CAS, though we found neither for insertive CAS. Black participants had lower odds of engaging in receptive CAS than White participants, but their odds were significantly greater when with a same-race partner than a different-race partner compared with White participants. Nonetheless, the overall probability of receptive CAS was lower for Black men than for White men regardless of partner type. In contrast, there were no significant differences in insertive CAS by participant or partner race—Black, White, and Latino HIV-positive men had similar odds of engaging in insertive CAS, and these rates did not change with same-race versus different-race partners. Among HIV-negative men, overall, rates of both receptive and insertive CAS were low. In contrast to HIV-positive men, there were no significant main or interaction effects of participant and partner race on either receptive or insertive CAS.
Taken together, our findings highlight the complexities of attempting to explain racial disparities in HIV incidence and prevalence among GBM. In general, (1) men tended to partner with others of the same race, (2) HIV is more prevalent among men of color, and (3) race acted independent of whether one would engage in behaviors that would put them at highest risk for transmitting HIV (i.e., no main or interaction effects for insertive CAS among HIV-positive men, and no main or interaction effects for receptive CAS among HIV-negative men). This would suggest that racial disparities in HIV may be due to a higher exposure frequency (i.e., the frequency with which one comes into contact with a partner where a transmission could occur). However, men were also less likely to have anal sex when having sex with someone of the same race—a finding that works against the premise of higher exposure frequency.
Previous research has noted that the racial composition of sexual networks likely plays integral roles in ongoing racial disparities in HIV incidence among GBMSM (Clerkin et al., 2011; Millett et al., 2007; Newcomb & Mustanski, 2013; Raymond & McFarland, 2009). Our findings add to this research, suggesting that there may be yet an additional layer—not only is it that the race of a person is associated with the race of his partners (i.e., the racial composition of his available sexual networks), but that his behavior may change depending upon whether that partner is the same race or of a different race (particularly among HIV-positive men). However, a purely behavioral focus may be inadequate to fully explain racial disparities in HIV, and researchers may be well served to examine additional variables such as viral load among HIV-positive men, STI history and presence, and structural factors such as racism and income inequality (Millett et al., 2007). We believe community-level interventions designed to reduce racial and ethnic biases within gay and bisexual communities may serve to reduce homophily in sexual partnerships and thus may help to reduce racial and ethnic disparities in HIV incidence among GBM. In addition, researchers might consider adapting demonstrated effective individual- and community-level interventions to include components that challenge racism and race-based stereotypes that exist in gay and bisexual communities (Grov et al., 2015a; Lick & Johnson, 2015).
In an effort to move toward interventions that would reduce HIV transmission risk, our findings highlight the need for more research to identify the mechanisms underlying the differences in behavior that we observed. It may be that perceptions of risk change based on a partner’s race. It is also possible that a sense of intimacy or shared experience increases—and stigma or rejection decreases—with same-race partners, particularly for non-White men, whereas White men probably do not feel a sense of stigma or possibility of rejection regardless of their partner’s race. Nevertheless, risk perceptions could still be changing for White men.
Further, it is understood that sexual encounters require, at minimum, two individuals, and thus, researchers may be well served to evaluate sexual behaviors among dyads. Understandably, this may be easier to accomplish with established partnerships (i.e., couples in a relationship) as opposed to casual partners. Future researchers would also be well served to include measures of pre-exposure prophylaxis (PrEP) in determining HIV acquisition risk. Our data were collected at a time when PrEP uptake was not yet widespread among HIV-negative GBMSM (Grov et al., 2015b).
Our findings must be interpreted in the context of limitations. First, this was a sample of highly sexually active GBM in NYC, and therefore, results may not generalize across the distribution of sexual activity levels. At the same time, the population in the study is one of particular interest for HIV prevention interventions. Second, it is important to note that the data provided here came from an observational diary study and that, although rates of missing data were low, we cannot attest to men’s behaviors on days they did not complete their diaries. Third, we have no way to verify the actual race or ethnicity of participants’ partners, as reports were based on participants’ perceptions. However, if indeed men’s behavior changes when they perceive their partner to be of a particular race, the objective reality of what that partner’s race actually is may be less important. That being said, participants’ perceptions could have some basis in objective reality as the modal way in which GBMSM meet sex partners today is via the Internet (Grov, Breslow, Newcomb, Rosenberger, & Bauermeister, 2014a), using Web sites and apps that often ask users to self-report their race as part of their profile. Further, there are many additional contextualizing facets of sexual encounters that we were unable to consider in this study. These include variables such as the ages of participants’ partners (Newcomb & Mustanski, 2013) and the locations where sex occurred (Balán, Barreda, Marone, Ávila, & Carballo-Diéguez, 2014; Grov, Rendina, Ventuneac, & Parsons, 2014b; Melendez-Torres, Nye, & Bonell, 2015). Next, although longitudinal data were taken from a daily diary, participant’s HIV statuses were stable during the data collection period. We cannot say whether men’s behavior was a result of their HIV status or vice versa. For example, is it that HIV-positive men more often take on an anal receptive role to reduce transmission risk to their partners, or is it that the receptive role was associated with their becoming HIV-positive in the first place?
In spite of these limitations, our study highlights that race matters not only in terms of what partners men may choose for themselves (or be available to them), but also in terms of the sexual behaviors men will engage in based on whether that person is of the same or a different race. We highlight, however, that neither race of participants nor of partners was significantly associated with behaviors that would have placed men at the greatest risk for transmitting HIV (insertive CAS for HIV-positive men and receptive CAS for HIV-negative men). For researchers, our findings highlight not only the importance of examining racial homophily, but also to examine how an individual’s behavior may change depending on whether his partner is of the same race or a different race. Given that our sample was all highly sexually active, it is necessary to replicate our analysis with different samples of GBM. Researchers may benefit by gathering qualitative data to determine why behavior may change.
References
Balán, I. C., Barreda, V., Marone, R., Ávila, M. M., & Carballo-Diéguez, A. (2014). Venues, patrons, and alcohol use dynamics: The creation of a high risk sexual environment. AIDS and Behavior, 18, 2097–2109.
CDC. (2015a). HIV among gay and bisexual men. Retrieved from http://www.cdc.gov/hiv/risk/gender/msm/facts/.
CDC. (2015b). HIV in the United States: At a glance. Retrieved from http://www.cdc.gov/hiv/statistics/basics/ataglance.html.
CDC. (2015c). HIV surveillance—Men who have sex with men (MSM). Retrieved from http://www.cdc.gov/hiv/pdf/statistics_surveillance_MSM.pdf.
Clerkin, E. M., Newcomb, M. E., & Mustanski, B. (2011). Unpacking the racial disparity in HIV rates: The effect of race on risky sexual behavior among Black young men who have sex with men (YMSM). Journal of Behavioral Medicine, 34(4), 237–243. doi:10.1007/s10865-010-9306-4.
Fujimoto, K., & Williams, M. L. (2015). Racial/ethnic differences in sexual network mixing: A log-linear analysis of HIV status by partnership and sexual behavior among most at-risk MSM. AIDS and Behavior, 19, 996–1004.
Grov, C., Breslow, A. S., Newcomb, M. E., Rosenberger, J. G., & Bauermeister, J. A. (2014a). Gay and bisexual men’s use of the internet: Research from the 1990s through 2013. Annual Review of Sex Research, 51(4), 390–409.
Grov, C., Golub, S. A., Mustanski, B., & Parsons, J. T. (2010a). Sexual compulsivity, state affect, and sexual risk behavior in a daily diary study of gay and bisexual men. Psychology of Addictive Behaviors, 24(3), 487–497. doi:10.1037/a0020527.
Grov, C., Parsons, J. T., & Bimbi, D. S. (2010b). Sexual compulsivity and sexual risk in gay and bisexual men. Archives of Sexual Behavior, 39(4), 940–949. doi:10.1007/s10508-009-9483-9.
Grov, C., Rendina, H. J., Ventuneac, A., & Parsons, J. T. (2014b). Partners met via sex parties present significantly greater odds for condomless anal sex among MSM: An event-level analysis of venues where male partners are met. Journal of Acquired Immune Deficiency Syndromes, 67, 564–568. doi:10.1097/QAI.0000000000000343.
Grov, C., Saleh, L. D., Lassiter, J. M., & Parsons, J. T. (2015a). Challenging race-based stereotypes about gay and bisexual men’s sexual behavior, and perceived penis size and size satisfaction. Sexuality Research and Social Policy, 12(3), 224–235. doi:10.1007/s13178-015-0190-0.
Grov, C., Whitfield, T. H. F., Rendina, H. J., Ventuneac, A., & Parsons, J. T. (2015b). Willingness to take PrEP and potential for risk compensation among highly sexually active gay and bisexual men. AIDS and Behavior, 19(12), 2234–2244. doi:10.1007/s10461-015-1030-1.
Hogben, M., & Leichliter, J. S. (2008). Social determinants and sexually transmitted disease disparities. Sexually Transmitted Diseases, 35(12 Suppl.), S13–S18. doi:10.1097/OLQ.0b013e31818d3cad.
Lick, D. J., & Johnson, K. L. (2015). Intersecting race and gender cues are associated with perceptions of gay men’s preferred sexual roles. Archives of Sexual Behavior, 44, 1471–1481.
Marks, G., Millett, G. A., Bingham, T., Bond, L., Lauby, J., Liau, A., … Stueve, A. (2008). Understanding differences in HIV sexual transmission among Latino and black men who have sex with men: The Brothers y Hermanos Study. AIDS and Behavior. doi:10.1007/s10461-008-9380-6.
Melendez-Torres, G. J., Nye, E., & Bonell, C. (2015). Is location of sex associated with sexual risk behaviour in men who have sex with men? Systematic review of within-subjects studies. AIDS and Behavior. doi:10.1007/s10461-015-1093-z.
Millett, G. A., Flores, S. A., Peterson, J. L., & Bakeman, R. (2007). Explaining disparities in HIV infection among black and white men who have sex with men: A meta-analysis of HIV risk behaviors. AIDS, 21(15), 2083–2091. doi:10.1097/QAD.0b013e3282e9a64b.
Mustanski, B. S. (2007). The influence of state and trait affect on HIV risk behaviors: A daily diary study of MSM. Health Psychology, 26(5), 618–626.
Mustanski, B. S., Birkett, M., Kuhns, L. M., Latkin, C. A., & Muth, S. Q. (2015). The role of geographic and network factors in racial disparities in HIV among young men who have sex with men: An egocentric network study. AIDS and Behavior, 19, 1037–1047. doi:10.1007/s10461-014-0955-0.
Newcomb, M. E., & Mustanski, B. (2013). Racial differences in same-race partnering and the effects of sexual partnership characteristics on HIV risk in MSM: A prospective sexual diary study. Journal of Acquired Immune Deficiency Syndromes, 62, 329–333.
Parsons, J. T., Bimbi, D. S., & Halkitis, P. N. (2001). Sexual compulsivity among gay/bisexual male escorts who advertise on the Internet. Sexual Addiction & Compulsivity, 8, 101–112. doi:10.1080/10720160127562.
Parsons, J. T., Kelly, B. C., Bimbi, D. S., DiMaria, L., Wainberg, M. L., & Morgenstern, J. (2008). Explanations for the origins of sexual compulsivity among gay and bisexual men. Archives of Sexual Behavior, 37(5), 817–826. doi:10.1007/s10508-007-9218-8.
Parsons, J. T., Rendina, H. J., Grov, C., Ventuneac, A., & Mustanski, B. (2015a). Accuracy of highly sexually active gay and bisexual men’s predictions of their daily likelihood of anal sex and its relevance for intermittent event-driven HIV pre-exposure prophylaxis. Journal of Acquired Immune Deficiency Syndromes, 68, 449–455.
Parsons, J. T., Rendina, H. J., Ventuneac, A., Cook, K. F., Grov, C., & Mustanski, B. (2013). A psychometric investigation of the Hypersexual Disorder Screening Inventory among highly sexually active gay and bisexual men: An item response theory analysis. Journal of Sexual Medicine, 10, 3088–3101.
Parsons, J. T., Rendina, H. J., Ventuneac, A., Moody, R. L., & Grov, C. (2015b). Syndemic production and sexual compulsivity/hypersexuality in a cohort of highly sexually active gay and bisexual men: Further evidence of a three group conceptualization. Archives of Sexual Behavior, 44, 1903–1913. doi:10.1007/s10508-015-0574-5.
Parsons, J. T., Rendina, H. J., Ventuneac, A., Moody, R. L., & Grov, C. (2015c). Hypersexual, sexually compulsive, or just highly sexually active? Investigating three distinct groups of gay and bisexual men and their profiles of HIV-related sexual risk. AIDS and Behavior. doi:10.1007/s10461-015-1029-7.
Raymond, H. F., & McFarland, W. (2009). Racial mixing and HIV risk among men who have sex with men. AIDS and Behavior, 13, 630–637. doi:10.1007/s10461-009-9574-6.
Rendina, H. J., Moody, R. L., Grov, C., Ventuneac, A., & Parsons, J. T. (2015). Aggregate and event-level associations of substance use and sexual behavior among gay and bisexual men: Comparing retrospective and prospective data. Drug and Alcohol Dependence, 154, 199–207. doi:10.1016/j.drugalcdep.2015.06.045.
Stall, R., Duran, L., Wisniewski, S. R., Friedman, M. S., Marshal, M. P., McFarland, W., … Mills, T. C. (2009). Running in place: Implications of HIV incidence estimates among urban men who have sex with men in the United States and other industrialized countries. AIDS and Behavior, 13, 615–629. doi:10.1007/s10461-008-9509-7.
Stall, R., Mills, T. C., Williamson, J., Hart, T., Greenwood, G., Paul, J., … Catania, J. A. (2003). Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. American Journal of Public Health, 93, 939–942. doi:10.2105/AJPH.93.6.939.
Stall, R., Paul, J. P., Greenwood, G., Pollack, L. M., Bein, E., Crosby, G. M., … Catania, J. A. (2002). Alcohol use, drug use and alcohol-related problems among men who have sex with men: The Urban Men’s Health Study. Addiction, 96(11), 1589–1601. doi:10.1046/j.1360-0443.2001.961115896.x.
Sullivan, P. S., Peterson, J., Rosenberg, E. S., Kelley, C. F., Cooper, H., Vaughan, A., … Sanchez, T. H. (2014). Understanding racial HIV/STI disparities in Black and White men who have sex with men: A multilevel approach. PLoS ONE, 9(3), e90514. doi:10.1371/journal.pone.0090514.
Taylor, B. S., Chiasson, M. A., Scheinmann, R., Hirshfield, S., Humberstone, M., Remien, R. H., … Wong, T. (2012). Results from two online surveys comparing sexual risk behaviors in Hispanic, black, and white men who have sex with men. AIDS and Behavior, 16(3), 644–652.
U.S. Census Bureau. (2010). State and county quick facts, New York City. Retrieved from http://quickfacts.census.gov/qfd/states/36/3651000.html.
U.S. Census Bureau. (2015). State and county quick facts. Retrieved from http://quickfacts.census.gov/qfd/states/00000.html.
Ventuneac, A., Rendina, H. J., Grov, C., Mustanski, B., & Parsons, J. T. (2015). An item response theory analysis of the Sexual Compulsivity Scale and its correspondence with the Hypersexual Disorder Screening Inventory among a sample of highly sexually active gay and bisexual men. Journal of Sexual Medicine, 12, 481–493. doi:10.1111/jsm.12783.
Acknowledgments
This project was supported by a research grant from the National Institute of Mental Health (R01-MH087714; Jeffrey T. Parsons, Principal Investigator). H. Jonathon Rendina was supported in part by a career development award from the National Institute on Drug Abuse (K01-DA039030). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors would like to acknowledge the contributions of other members of the Pillow Talk Research Team, particularly Demetria Cain, Ruben Jimenez, Brian Mustanski, John Pachankis, and Sitaji Gurung. We would also like to thank CHEST staff who played important roles in the implementation of the project: Chris Hietikko, Chloe Mirzayi, Anita Viswanath, and Thomas Whitfield, as well as our team of research assistants, recruiters, and interns. Finally, we thank Chris Ryan, Daniel Nardicio, and Stephan Adelson and the participants who volunteered their time for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Grov, C., Rendina, H.J., Ventuneac, A. et al. Sexual Behavior Varies Between Same-Race and Different-Race Partnerships: A Daily Diary Study of Highly Sexually Active Black, Latino, and White Gay and Bisexual Men. Arch Sex Behav 45, 1453–1462 (2016). https://doi.org/10.1007/s10508-015-0677-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-015-0677-z