
Abstract
Extramarital sexual partnerships are a common reason for intimate partner violence (IPV) in sub-Saharan Africa. Despite the fact that IPV requires an interaction between two partners, the majority of the research focuses on individuals rather than the broader relationship context where such violence takes place. Using a sample of 422 married couples from rural Malawi, this study examined the dyadic environment of marital infidelity and two types of IPV victimization: sexual coercion and physical abuse. We considered both self-reported marital infidelity and perceived partner infidelity to assess how well partners knew each other and to compare their respective associations with IPV. Logistic regression was used to test for associations between self-reported marital infidelity and IPV. Multilevel logistic regression was used to examine actor and partner effects of perceived partner infidelity on an individual’s and their partner’s experience of IPV. The results show that self-reported marital infidelity was not significantly associated with IPV for men or women. However, the perception of a partner’s infidelity was significantly associated with both an individual’s and their partner’s risk for sexual coercion and physical abuse. Contrary to the “sexual double standard” hypothesis, women were not significantly more likely than men to report being physically abused when their partners suspected infidelity. Future studies should continue to explore the relationship context of IPV in sub-Saharan Africa in order to understand how spouses mutually shape each other’s experience of IPV and subsequent health outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the African context, studies show that marital infidelity is a highly contentious issue (Schatz, 2005; Scorgie et al., 2009), particularly for its relationship with HIV/AIDS (Glynn, Caraël, Buvé, Musonda, & Kahindo, 2003). Beyond concerns of HIV infection, one important consequence of marital infidelity on health is intimate partner violence (IPV). Studies from across the region demonstrate that women who have multiple sexual partners or suspect that their partners are non-monogamous are more likely to experience IPV (Dunkle et al., 2004; Jewkes et al., 2006; Karamagi, Tumwine, Tylleskar, & Heggenhougen, 2006; Maman et al., 2002). To date, the majority of research on IPV in sub-Saharan Africa has been one-sided, focusing on either women as victims or men as perpetrators; however, this perspective limits our understanding of the broader dyadic context in which this violence takes place. Using a sample of married women and their partners from rural Malawi, the present study extended the predominantly individual-level body of research through a dyadic investigation of marital infidelity and two types of IPV victimization: sexual coercion and physical abuse.
Although there are a number of violence prevention programs in Africa that focus on men and masculinity (Dworkin, Treves-Kagan, & Lippman, 2013), IPV has historically been studied and addressed as a women’s public health issue. Indeed, studies show that African women experience high levels of physical and sexual violence over the course of their lifetimes (Fonck, Leye, Kidula, Ndinya-Achola, & Temmerman, 2005; Jewkes, Dunkle, Nduna, & Shai, 2010; Ntaganira et al., 2008), which ranges from 36 to 71 % (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). IPV can have significant impacts on women’s physical, reproductive, sexual, and mental health (Campbell, 2002; Garcia-Moreno et al., 2006). In Tanzania and South Africa, where HIV prevalence is high, IPV has also been documented as a risk factor for HIV/AIDS among women (Dunkle et al., 2004; Jewkes et al., 2010; Maman et al., 2002).
A variety of different social, behavioral, and structural factors surround IPV in sub-Saharan Africa, including younger age (Koenig et al., 2004; Were et al., 2011), lower education (Karamagi et al., 2006), being married (Koenig et al., 2004; Zablotska et al., 2009), alcohol use and abuse (Koenig et al., 2003; Zablotska et al., 2009), and supportive attitudes towards wife-beating (Alio et al., 2010; Koenig et al., 2004). Gender-based power imbalances are one of the most compelling explanations for IPV among women (Blanc, 2001). Power may be connected with IPV through its association with masculinity, male dominance, and control over women (Choi & Ting, 2008; Jewkes, 2002; Morrell, Jewkes, Lindegger, & Hamlall, 2013). In South Africa, for example, women in relationships with high levels of male control were more likely to report recent or previous IPV (Dunkle et al., 2004). In addition, structural factors related to poverty may also contribute to the experience of IPV through the pathway of masculinity. Men in poverty who are unable to live up to traditional gender norms related to the provider role may use violence to express their manhood and male identity (Jewkes, 2002).
Even though female-perpetrated violence tends to be less severe than violence committed by males (Archer, 2000), a few studies draw attention to men’s experience of IPV as victims of female abuse. In South Africa, Gass, Stein, Williams, and Seedat (2011) found that rates of physical abuse victimization were equally high among both men and women (21 vs. 29 %). Regarding sexual abuse, there are also a few accounts of African men being coerced into sex by older women (Dunkle et al., 2007; Simpson, 2007) and by their wives (Conroy, 2013). Outside of marriage, scholars have noted that men’s experience of sexual coercion can emerge through the more shaded areas of female sexual desire, heavy persuasion, and unwanted sexual touching (Sikweyiya & Jewkes, 2009). Within marriage, men’s experience of sexual coercion is less understood but may be attributed to women’s strong sense of sexual agency. For example, in Malawi, Tawfik and Watkins (2007) described a discourse of passion, love, and lust among women who actively pursued their own sexual desires and may seek another sexual partner if husbands failed to meet their needs. However, male-dominant sexual scripts, such as the belief that “men are expected to initiate sex,” provides a code of conduct for sexual-decision making within marriage (Mbweza, Norr, & McElmurry, 2008). Therefore, it is possible that husbands who are pressured or persuaded by a sexually assertive wife may feel that they were coerced into sex. More empirical evidence is needed to understand men’s experiences of IPV and gender differences in the prevalence and patterns of IPV within marriage.
Paradoxically, these studies examine IPV at the individual-level despite the fact that relationship violence is an interdependent behavior and thus requires the presence of both partners. According to interdependence theory, each couple member is believed to have a certain amount of influence over the interaction that they have together; thus, an understanding of such behaviors necessitates that both partner’s perspectives be taken into account (Kelley & Thibalt, 1978). Here, we do not intend to suggest that women are fully capable of preventing rape or physical abuse or that they should be blamed for contributing to their own experience of violence. But rather, we suggest that relationship violence may be better understood as a product of both partners’ beliefs, attributes, and behaviors: as a dyadic process. For example, one explanation that has been offered to understand IPV posits that as women gain more power in society, transgress from traditional gender roles, or challenge the patriarchal gender order, men retaliate with violence in order to maintain their status and position (Jewkes, 2002). Others have noted that the portrayal of women as completely vulnerable, without agency, or control over their relationships is problematic (Higgins, Hoffman, & Dworkin, 2010; Watkins & Swidler, 2012) and this may prevent the field from moving forward to understand the relational aspect of violence.
Indeed, couples studies from the West have identified several important relationship-level correlates of IPV, including relationship dominance, decision-making power, and couple communication patterns (Babcock, Waltz, Jacobson, & Gottman, 1993; Coleman & Straus, 1986; Karakurt & Cumbie, 2012). Together, these studies highlight that there are multiple different pathways to violence that depend upon both partner’s perspectives. For example, in couples from the US, men who reported higher male dominance were more likely to be both victims and perpetrators of aggression; similar associations were found for women who reported higher female dominance (Karakurt & Cumbie, 2012). Another study on couples from the US found that marital conflict was more common in male-dominated and female-dominated relationships as compared to egalitarian relationships in which couples were more likely to agree about power relations (Coleman & Straus, 1986). Though power relations within couples from the US are substantially different from those in sub-Saharan Africa, the findings provide more information on marital violence than if one partner was studied in isolation.
In sub-Saharan Africa, less research on IPV has taken a dyadic perspective. Of the few studies that used data on both partners, the focus has been on economic resources and, together, these studies offer mixed support for the role of economic power imbalances on IPV victimization (Choi & Ting, 2008; Conroy, 2013). A systematic review of economic empowerment and violence in low and middle income countries also finds divergent evidence for the role of income generation on women’s risk of violence (Vyas & Watts, 2009). One explanation may be that it not the economic difference itself, but rather a change in one partner’s economic status (e.g., women become employed, men face employment difficulties) that may trigger violence (Krishnan et al., 2009).
Marital Infidelity and IPV in Sub-Saharan Africa
In sub-Saharan Africa, marital infidelity may be connected to physical abuse through the following possible pathways, which are strongly tied to normative gender roles. First, men who have concurrent sexual partners may be more prone to physical violence in general, such as through the attachment to masculine identities that emphasize sexual conquests and male-dominance (Boonzaier, 2005; Malamuth, Sockloskie, Koss, & Tanaka, 1991). Second, women who believe that their husbands have an extramarital sexual partner may react violently towards the men out of jealousy and anger (Karamagi et al., 2006). Third, men may use violence in response to their partner’s accusations of infidelity, as noted in Tanzania and Rwanda (Lary, Maman, Katebalila, & Mbwambo, 2004; van der Straten, King, Grinstead, Serufilira, & Allen, 1995). Finally, men who suspect their wives have extramarital sexual partners may use violence to reclaim authority in the household and to reprimand a wife who they perceive is disobedient (Kim & Motsei, 2002). In Uganda, women who had sex outside their marriages were at a significantly higher risk for IPV (Karamagi et al., 2006).
The negative consequences of infidelity, such as physical abuse, may be more severe for women suspected of infidelity than for men guilty of the same behaviors (Hatcher et al., 2013). In many parts of Africa, multiple sexual partners signify economic prosperity and bring social status to men (Smith, 2009; Swidler & Watkins, 2007). While some women challenge these social norms by threatening to divorce an unfaithful partner who may bring HIV into the family (Schatz, 2005; Watkins, 2004), there still exists a sexual double standard around marital infidelity that makes it more socially acceptable for men than women to engage in sex outside of the marital dyad.
For sexual coercion, the connection with infidelity is conceptually different and likely to be mediated by perceived risk for HIV. When serostatus is unknown, perceptions of risk are informed by what one partner knows about the other’s sexual history. In Malawi, marital infidelity was found to be the strongest correlate of overestimating one’s own and a spouse’s risk for HIV (Anglewicz, Bignami-Van Assche, Clark, & Mkandawire, 2008). Even though there is a widespread belief that women are not supposed to decline sex with their husbands, it may be considered socially acceptable for a wife to refuse to have sex with a spouse deemed to be at risk for HIV (National Statistical Office & ICF Macro, 2011). Yet in practice, many women fail to negotiate the circumstances of sex with an unsafe partner. In Uganda, Koenig et al. (2004) showed that a woman’s experience of sexual coercion was strongly tied to her perception of a male partner’s risk for HIV. As the logic follows, married women who suspect their husbands are unfaithful and therefore at higher risk may be more likely to experience sexual coercion.
Given this background literature, this study had three main objectives: (1) to test whether individuals who self-reported marital infidelity were more likely to experience IPV victimization as compared to those who reported that they were faithful; (2) to test whether an individual’s perception of their spouse’s fidelity influenced both their own (called an “actor effect”) and their partner’s experience of IPV (called a “partner effect”); and (3) to test whether partner effects on physical IPV would be stronger for women than for men (i.e., gender is an effect modifier). In other words, when women’s partners suspect that they have an extramarital sexual partner, women will experience higher levels of physical violence than when men’s partners suspect men have an extramarital sexual partner.
The Malawi Context
Malawi is a small, landlocked country located in southeastern Africa with a population of 13.1 million (National Statistical Office & ICF Macro, 2011). The economy of Malawi is primarily driven by agriculture, which accounts for 30 % of the country’s GDP (National Statistical Office & ICF Macro, 2011). At the national level, the economy depends on substantial inflows of economic assistance from the International Monetary Fund, World Bank, and individual donor nations. The country is divided into three regions (north, central, and south) and 27 districts. This study was conducted in the Balaka district of southern Malawi. Like other districts, the area is rural and has minimal employment opportunities. In general, the southern region follows a matrilineal/matrilocal orientation where men physically move in with their wives’ families after marriage as compared to the predominantly patrilineal/patrilocal north (Chimbiri, 2007; Peters, 1997). The southern region of Malawi also has higher rates of divorce as compared to other regions with around 33 % of all marriages ending before their fifth year anniversary (Reniers, 2003). HIV prevalence in the southern district is 15 %, which is higher than the national average of 11 % (National Statistical Office & ICF Macro, 2011).
Intimate partner violence is pervasive in Malawi. A recent demographic report featuring a nationally representative sample showed that 25 % of women had experienced sexual violence. In the same report, 28 % of women had experienced physical violence (National Statistical Office & ICF Macro, 2011). Trends indicate that rates of sexual and physical IPV increase with age (up until 30 years), decrease with education, and are higher within marriage and in rural areas (National Statistical Office & ICF Macro, 2011). To the best of our knowledge, corresponding data on violence against men in Malawi have not been collected.
Method
Participants and Procedure
The data were from Tsogolo la Thanzi (TLTFootnote 1; “Healthy Futures” in Chichewa), a population-based panel study in the Balaka district of southern Malawi. TLT was designed to study how young adults who have grown up during the HIV/AIDS epidemic make decisions about marriage, childbearing, and sexual behavior. In 2009, approximately 1,500 women aged 15–25 years were randomly selected from a household listing of all residents living within a 7 km radius of the town center. At the time of the listing, the area contained 6,696 eligible women. Of the random sample of women who were asked to participate, 96.4 % of them completed baseline interviews. Women were given enumerated tokens and asked to recruit up to three male partners (husbands and boyfriends) to participate in the study. The use of enumerated tokens allowed for the verification of each male participant’s status as a named partner and the ability to identify his female partner in the sample. Other population-based studies from Malawi using similar sampling strategies have been successful with this approach (e.g., Helleringer & Kohler, 2007).
Longitudinal survey data were collected at 4-month intervals over a period of approximately three years (for a total of 8 waves). This study uses data from the third wave, collected between February and May 2010, when a special module on relationship power and IPV was added to the partnership survey. At Wave 3, 91.1 % of the Wave 1 sample of women was retained in the study. Of those, 823 women and 684 of their male partners were administered the relationship power module because they reported an ongoing sexual relationship (e.g., spouse, live-in partner, steady boyfriend/girlfriend, or new boyfriend/girlfriend) at Wave 3. Participants with multiple partners were asked these questions with regard to their most serious partner. For married participants, the spouse was automatically considered the reference partner. A couple dataset was created for all participants who answered the power questions about each other using a separate database linking women and their male partner (a total of 932 participants). Given that the sample consisted of couples, it was inherently biased towards serious partnerships (91 % of couples were married/cohabitating). The final sample was limited to married/cohabitating couples in order to be able to make generalizations about a defined population.
Measures
Dependent Variables
The two IPV outcome measures were derived from Pulerwitz et al. (2000) and then adapted to the Malawian context to ensure validity. In order to minimize the burden to TLT participants who were already subjected to lengthy interviews over 8 waves, the IPV measures were captured as dichotomous indicators and operationalized as affirmative responses to two separate questions about sexual coercion and physical abuse. Participants were asked if they were victims of IPV (but not if they were perpetrators) in relation to the reference partner noted in the IPV module. Sexual coercion was ascertained by asking participants, “Has your partner ever forced you to have sex when you did not want to?” In the local language of Chichewa, translation of the term “forced” does not apply to physical force or rape, but rather verbal pressure or persuasion to have sex in the face of opposition. Physical abuse was ascertained by asking participants, “Has your partner ever hurt you by beating you?” While multiple forms of physical abuse are possible, such as hitting, kicking or punching, the question on physical abuse was restricted to “beating” in order to reflect the predominant local term used to describe physical abuse in Malawi.
Independent Variables
Self-reported marital infidelity was captured as follows. At Wave 3, participants were asked how many people they had sex with in the past 4 months (including spouses), which covered the time period from Wave 2. At Wave 2, participants were asked the same question. At Wave 1, participants were asked about their number of sexual partners over a longer period: the past 12 months. We linked participants at Wave 3 with their corresponding data from Waves 1 and 2 to create a three-segment measure of infidelity over a 20-month period. If during any of the three segments a participant reported having more than one sexual partner, they were considered unfaithful for the entire 20-month period. The perceived likelihood of a partner having an affair was assessed by the statement: “My partner is probably having sex with someone else.” Participants stated whether they strongly agreed (1), agreed (2), disagreed (3), or strongly disagreed (4) with this statement. Responses were then collapsed into two categories (agreement/disagreement).
A number of demographic, couple, and behavioral factors were adjusted for in the statistical models: gender, age, years of education, the Household Goods Index (HGI), relationship duration, having at least one child together, and perceived HIV risk of self and partner. Gender was a binary variable (0 = female, 1 = male). Age and years of education were modeled as continuous variables. In Malawi, up to and including 8 years of education is considered primary school, 9 to 12 years is considered secondary school, and greater than 12 years is considered tertiary school. The HGI was an index of 9 common household goods (e.g., bicycle, television, bed with mattress, etc.) and was used to approximate household economic status. Relationship duration was computed by subtracting the date of the survey from the date the couple first started spending time together as more than friends. For shared children, a binary variable was created to indicate whether a couple had at least one child together. Couple discrepancies in the HGI (97.2 % reported a difference of less than 2 household items) and relationship duration (77.9 % reported a duration difference of less than 2 years) were resolved by replacing each partner’s value with the couple mean. For couples who disagreed about having at least one child together (6.4 %), the female partner’s report replaced the male partner’s report, which was believed to be more accurate.
For perceived HIV risk of self, participants were asked: “Pick the number of beans that reflect how likely it is that you are infected with HIV now” (0–10). Perceived HIV risk of partner was captured with the statement: “What is the likelihood that your partner is currently infected with HIV?” Response options included no likelihood, low, medium, high, and “I know she/he is (infected with HIV).” Based on the distribution, a binary variable was created where 0 referred to no or low likelihood of HIV infection and 1 referred to medium, high or certain likelihood of HIV infection.
Analytic Approach
The statistical analysis consisted of three main steps. In the first step, we tested for gender differences on key demographic characteristics, behavioral variables, and the two IPV outcomes of sexual coercion and physical violence. ANOVA was used to test for gender differences in continuous variables; χ 2 tests were used to test for gender differences in the remaining categorical variables; and logistic regression was used to test for gender differences on imputed variables. In the second step, gender-stratified logistic regression models were employed to test for bivariate associations between the set of independent variables, including self-reported marital infidelity, and the two IPV dependent variables. In the third step, we tested for actor–partner effects of perceived partner infidelity and the two IPV dependent variables.
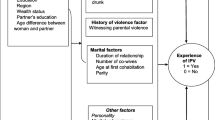
The Actor–Partner Interaction Model (APIM) was used as the primary analytical framework to test for actor and partner effects. For the analysis, the data were organized in a pairwise fashion such that each individual had their own record, but their partner’s information was also duplicated in the same record. The APIM is based on the premise that one partner’s attributes and behaviors can affect the other partner’s outcomes (Kenny, Kashy, & Cook, 2006). Each partner’s independent variable (i.e., perceived infidelity) was thought to affect both their dependent variable (i.e., IPV) (actor effect) and their partner’s dependent variable (partner effect). If partner effects were discovered, there would be evidence that the two couple members are part of an interdependent system (Kenny et al., 2006). Figure 1 provides a conceptual model for the APIM analysis used in this study.

APIM for perceived partner infidelity and two types of IPV victimization: sexual coercion and physical abuse. AE “actor effect”, PE “partner effect.” Subscripts refer to men (m) or women (w)
Multiple different analytic methods have been proposed to carry out the APIM technique (Kenny et al., 2006). In this study, we used the multilevel regression approach with interaction terms as outlined by Kenny et al. The use of a hierarchical model allowed us to solve an inherent problem of dyadic data: non-independence. Both dyad members’ (wife and husband) estimates of IPV were treated as the dependent variables while accounting for the higher-level couple unit. In the multilevel model, Level 1 represented all individuals and reports fixed effects whereas Level 2 (the group level) allowed for a random effect across dyads. Non-independence was assessed by computing the intraclass correlation coefficient (ICC) for the two dependent variables. The ICCs showed that there was modest evidence of non-independence. The ICC for sexual coercion showed that approximately 3.1 % of the variance was explained by the dyad (p = .26). For physical abuse, the ICC showed that 1.2 % of the variance was explained by the dyad (p = .40). Although these ICCs would be considered small by some researchers (e.g., Cohen, 1998), others argue that even a small level of non-independence can lead to biased estimates (Hox & Kreft, 1994). Therefore, to err on the side of caution, we used a multilevel model to test for actor and partner effects. In the final APIM analysis, the models included statistical controls for socioeconomic variables likely to be associated with IPV, namely, gender, age, education, and the HGI. In the sexual coercion models, perceived HIV risk of self and partner were also controlled for as described in our conceptual framework. All multilevel logistic regression models were estimated using the xtmelogit command in Stata 11.2.
The following checks were also performed. For the self-reported infidelity measure over the 20-month period, data were missing for 12 % of all participants—mostly male partners, who had not participated in the study at Wave 1. In addition, one participant had missing education data and two participants (from the same couple) had missing data for both IPV variables. For perceived HIV risk of partner, 55 participants reported that they “did not know” about whether their partner could be HIV infected. To handle these missing data, we performed multiple imputation via chained equations using the mi ice command in Stata to build an imputation model containing all predictors, covariates, and outcome variables. We generated 12 multiply imputed datasets corresponding to the largest percentage of missing data on a given variable (12 %). For participants who were together for longer than 8 months, their self-reported infidelity measure included responses from Waves 2 and 3. If they were together longer than 20 months, their infidelity measure included data from all three waves. This ensured that self-reported marital infidelity was captured during the relationship of interest at Wave 3. In addition, we checked for multi-collinearity among all independent variables by examining the variance inflation factor (VIF), which were all well below the recommended cutoff of 10 (Agresti & Finlay, 2009). For the final regression models, age was log transformed to reduce kurtosis. Perceived HIV risk of self was also slightly non-normal and transformed using the square-root function in Stata.
Results
Sample Characteristics
At TLT’s Wave 3, 844 men and women (422 couples) were asked the IPV questions. Table 1 shows selected characteristics for the sample of 422 married couples. The mean age for the study population was 25.2 years. Men were, on average, 5.5 years older than women and differences by gender were significant (p < .05). The mean years of education was 7.1 years, reflecting a primary school education. Men had, on average, 1.2 more years of education than women and differences by gender were significant (p < .05). The mean number of owned household items, which ranged from 0 to 7, for the total sample was 2.9. Four-fifths (80.1 %) of couples reported having at least one child together. On average, couples had been together for 5.3 years.
On a scale of 0–10, the mean value for perceived HIV risk of self was 1.8. Men did not report a significantly different perceived risk for HIV than women. Based on the imputed dataset, an estimated 6.3 % of participants believed that their partner had a higher likelihood of HIV infection (95 % CI 4.6–8.1). Women were more likely to believe their partners had a higher likelihood of HIV infection (8.7 %, 95 % CI 5.7–11.6) as compared to men (4 %, 95 % CI 2.0–5.9) and the gender difference was significant (p < .05). For perceived partner infidelity, 14.3 % of participants believed that their partners were unfaithful. Women were more likely to believe that their partners were unfaithful than men (18.5 compared to 9.5 %) and the gender difference was significant (p < .05).
Based on the imputed dataset, an estimated 7.1 % (95 % CI 5.2–8.9) of participants reported that they had at least one additional sexual partner over the last 20 months (or since their relationship started). Men were significantly more likely to report being unfaithful (12.8, 95 % CI 9.4–16.3) as compared to women (1.3, 95 % CI 0.13–2.4) (p < .05). In separate bivariate logistic regression models (results not shown), men’s odds of self-reported marital infidelity was 1.63 times higher when their partner suspected they had an extramarital sexual partner (OR = 1.63, 95 % CI 0.81–3.30) although it was not statistically significant. Given the low rates of reported infidelity among women, similar estimates could not be computed.
Almost 17 % of participants reported being coerced by their partner to have sex. Statistically significant gender differences were found with women reporting higher levels of sexual coercion (20.7 %) than men (12.1 %) (p < .05). Approximately 4 % of participants reported being physically abused by their partners. Statistically significant gender differences were also found with women reporting higher levels of physical abuse (6.7 %) than men (2.1 %) (p < .05). Sexual coercion and physical abuse were weakly correlated (r = .22); only 15.2 % of participants who reported being sexually coerced by their partner also reported being physically abused.
Self-Reported Marital Infidelity and Other Correlates of IPV
Table 2 shows the crude odds ratios (unadjusted) from the gender-stratified logistic regression analysis on sexual coercion and physical abuse victimization. For women and men, demographic and couple characteristics were not significantly associated with sexual coercion. In contrast to the women, men were more likely to report sexual coercion if they perceived themselves (OR = 1.58, 95 % CI 1.18–2.12, p < .01) and their partners (OR = 3.24, 95 % CI 1.08–9.71, p < .05) to be at greater risk for HIV. For women, those who perceived that their partners had an extramarital sexual partner were 2.18 times more likely to experience sexual coercion (OR = 2.18, 95 % CI 1.26–3.80, p < .01). For both women and men, self-reported marital infidelity was not significantly associated with sexual coercion.
For women, education was negatively associated with being a victim of physical abuse (OR = 0.86, 95 % CI 0.75–0.99, p < .05), whereas the perception of a partner’s infidelity was positively associated with physical abuse (OR = 2.69, 95 % CI 1.19–6.08, p < .05). For men, the log of age was positively associated with being a victim of physical abuse (OR = 107.87, 95 % CI 4.03–2889.71, p < .01). In addition, men who had been in longer relationships were more likely to report being a victim of physical abuse (OR = 1.28, 95 % CI 1.01–1.61, p < .05). Finally, self-reported marital infidelity among men was not significantly associated with physical abuse. For women, we could not establish a relationship with physical abuse due to low levels of self-reported marital infidelity. Given the level of missing data for self-reported marital infidelity over Waves 1–3 (12 %), we also conducted a logistic regression analysis using complete data at Wave 3 for self-reported marital infidelity in the past 4 months and still found no associations with IPV.
Actor–Partner Effects of Perceived Partner Infidelity on IPV
Because self-reported marital infidelity was not found to be a significant correlate of sexual coercion or physical abuse in the bivariate models, the APIM analysis focused solely on perceived partner infidelity as reported by both partners. It was predicted that an individual’s perception that their partner had an extramarital sexual partner would influence both their own (actor effect) and their partner’s experience (partner effect) of sexual coercion and physical abuse. Given that our APIM approach required the inclusion of interaction terms (Kenny et al., 2006), we focused the discussion on the full model results (main effects plus interaction terms) shown in Table 3. After controlling for other covariates in the full model, women’s odds of experiencing sexual coercion were 1.99 times higher when they perceived that their partner was having an affair (actor effect for women) (AOR = 1.99, 95 % CI 1.09–3.63, p < .05). There was a marginally significant gender difference in actor effects such that men’s odds of experiencing sexual IPV was 40 % less [1 − (1.99 × 0.30)] when they perceived their partner was having an affair (actor effect for men) (95 % CI 0.08–1.09, p = .068). On the other hand, men’s odds of experiencing sexual coercion were 2.03 times higher (1.04 × 1.95) when their partner perceived that they were having an affair, after controlling for other covariates (partner effect of women on men). There was no significant gender difference found for partner effects. As such, women’s odds of experiencing sexual coercion were also 2.03 times higher when their partners perceived that they were having an affair (partner effect of men on women). In a separate analysis (results not shown), we dropped the non-significant gender interaction term for partner effects and the main partner effect became statistically significant (p < .01). This suggests that for both men and women, actor and partner effects of perceived partner infidelity are significantly associated with sexual coercion.
The results for physical abuse were as follows, starting with the actor effects for the full model (refer to Table 3). After controlling for other covariates, women’s odds of experiencing physical abuse were 2.71 times higher when they perceived that their partner was having an affair (actor effect for women) (AOR = 2.71, 95 % CI 1.09–6.69, p < .05). For men, the odds of experiencing physical abuse were 1.71 times higher (2.71 × 0.63) when they perceived that their partner was having an affair (actor effect for men). Actor effects for physical abuse were not significantly different between men and women. It was also hypothesized that the partner effect of perceived infidelity would be a stronger correlate of physical abuse for women than for men. The results show evidence to the contrary. For women, the odds of physical abuse were 1.79 times higher when their partner perceived they were having an affair after controlling for other covariates (partner effect of men on women) (AOR = 1.79, 95 % CI 0.58–5.53). Conversely, men’s odds of experiencing physical abuse were 4.03 (1.79 × 2.25) times higher when their female partner perceived that they were having an affair (partner effect of women on men). Partner effects for physical abuse were not significantly different between men and women, suggesting that gender does not act as an effect modifier. Note that in the main effects model, there was a marginally significant partner effect for perceived partner infidelity on physical abuse (AOR = 2.41, 95 % CI 0.98–5.99, p = .056).
Discussion
This study examined the role of marital infidelity on IPV victimization using a couples’ sample of women and their male partners from rural Malawi. Rates of marital infidelity in this study were consistent with previous research findings. In a comparable study among married couples from rural Malawi, Anglewicz et al. (2008) found that 2 % of wives and 20 % of husbands reported having an extramarital sexual partner (as compared to 1.3 and 12.8 % in the current study). In another study from Malawi, similarly low levels of self-reported infidelity were found among women in the past 12 months (3 %) (Tawfik & Watkins, 2007). We found that perceived partner infidelity appeared to be a better correlate of IPV than self-reported infidelity, which was not significantly associated with either sexual coercion or physical abuse. While spousal perceptions of partner infidelity can be highly inaccurate, these beliefs may be more reliable than an individual’s own reported infidelity (Anglewicz et al., 2008). It is also possible that actual marital infidelity was underreported in this study, thus making it difficult to establish statistical associations with IPV. We speculate that women are more likely to underreport infidelity than men, given the existence of a nearly universal double standard that rewards men but punishes women for the same sexual behaviors (for an example in South Africa, see Wood & Jewkes, 1997). Indeed, empirical data from Malawi demonstrates that married men are significantly more likely to acknowledge having an extramarital sexual partner than women (Schatz, 2005).
As expected, this study found that perceptions of a partner’s infidelity affected both couple member’s experiences of sexual coercion. For example, if a wife perceived that her husband was having sex with someone else, she was more likely to experience sexual coercion herself. Her perception of a partner’s infidelity was associated with her partner’s risk of sexual coercion. In a sample of mostly married women from Uganda, Koenig et al. (2004) found that women experienced sexual coercion when they perceived their partner to be at higher risk for HIV. However, in the current study, the association between perceived partner infidelity and sexual coercion was not attenuated after adjusting for perceived risk of a partner (OR = 1.99, p = < .056 vs. AOR = 2.00, p = .056). This suggests that reluctance to have sex with a partner presumed to be having an affair goes beyond worries of contracting HIV. One explanation may be that women purposefully withhold sex from their husbands to punish them for engaging in what they perceive to be unacceptable behavior, as noted by Watts et al. (1998) in Zimbabwe. For the men presumed to be unfaithful, higher reports of unwanted sex could be attributed to decreased sexual desires or increased pressure for sex from a spouse out of sexual jealousy (Frieze, 1983; Gage & Hutchinson, 2006).
For physical violence, similar actor–partner effects were found. Women’s suspicions of partner infidelity were associated with higher reports of physical abuse among both women and their male partners. Women who perceived their male partner to be at higher risk for HIV may be more likely to resist sexual advances and their refusals could result in physical force or abuse by a male partner (Balmer, Gikundi, Kanyotu, & Waithaka, 1995). Women’s experience of physical abuse may also result from bringing up concerns about a partner’s extramarital relationships, as others have found elsewhere (van der Straten et al., 1995). It may be the case that men feel threatened and respond negatively to women who challenge traditional gender norms by directly addressing a partner’s infidelity.
It was surprising that women were not more likely to experience physical abuse when their partners suspected they were having an affair as compared to men whose wives suspected infidelity, especially in a setting where it is more socially acceptable for men to have extramarital sexual partners. Several explanations are possible. First, in this matrilineal/local region of Malawi where it is common for men to reside with their wives’ extended family, there may be a higher intolerance for violence against women. Second, it is conceivable that men living in poverty who are unable to provide for their families plead ignorance if their wives are bringing home money and material items in exchange for sex with other partners. Leach (1991) commented on women from Sierra Leone who seek lovers to make up for the financial neglect of husbands, who, in turn, tacitly accept their wives’ infidelity as a way of getting by. In another study from Nigeria, Cornwall (2002) noted that “men who are unable, or unwilling, to sustain the obligations of being a husband and those who have come to rely on their wives’ income to make up for their own social position are in a poor position to enforce control over their wives.” However, women engage in extramarital sex for a variety of different reasons other than economic necessity (e.g., see Parikh, 2009; Tawfik & Watkins, 2007) and thus this speculation may only apply to couples living in extreme poverty. Finally, there is evidence from Malawi that men may take more permanent measures when a wife is suspected of infidelity. Rather than using violence to reform behavior, a husband who truly believes his wife has an extramarital sexual partner may simply tell her to pack her bags and leave. In a discussion of female infidelity in rural Malawi, Schatz (2002) noted how if a man catches his wife “red-handed,” there is no choice but to divorce, adding “There is no such way a man can negotiate with his wife in such a situation.”
Several limitations of the present investigation are noteworthy. First, measures of violence are plagued by self-report biases around social desirability, reference group norms, and other factors, and this study was no exception. For example, women who subscribe to traditional beliefs around gender may not perceive sexual coercion as a form of violence but rather a wife’s obligation to her husband. Similarly, for physical abuse, supportive attitudes towards wife-beating may normalize the act of physical violence against women. For these reasons, it is possible that IPV was underreported among the participants. However, it is expected that violence underreporting would be non-systematic and bias the results towards the null hypothesis. Second, our sample was limited to married couples, making it difficult to generalize to other non-married populations. Yet, in Malawi, marriage is quasi-universal (National Statistical Office & ICF Macro, 2011) and therefore an analysis of IPV within marriage reflects the situation where violence would be most likely to occur. Among the non-married couples who were later excluded from the sample, none had reported any physical abuse. Third, this study was conducted in a predominantly matrilineal/local area of Malawi and therefore the results may not be generalizable to other regions of Malawi. For example, if women have more power in their marriages due to land ownership and familial social support, patterns of infidelity and violence may be very different than in the patrilineal/local regions. Fourth, the results of this study were less conclusive for men’s experiences of physical abuse due to low levels of reporting. Less than 2 % of men reported being a victim of physical abuse. In Malawi, it may be socially unacceptable and even embarrassing for men to report being physically dominated by a wife. Other researchers have noted this bias as well (Gass et al., 2011). Finally, it is possible that the two IPV outcome measures may have not been sensitive enough to capture the full range of experiences of IPV. More sensitive measures that include a series of questions about specific sexual, verbal, emotional, and physical actions may yield higher levels of reported IPV than what was reported in this study. Future studies should also include measures of severity given that female victimization has been shown to be more severe than male victimization (Archer, 2000). Specifically with regard to sexual violence, little is known about men’s experience of sexual coercion during marriage in this setting. Verbal pressure or persuasion to have sex represents a single dimension of sexual abuse and cannot account for the complexity and nuances of female-initiated sexual violence against men. Regardless, this study is one of the first to examine IPV in Malawi and forms the basis through which others can conduct a more extensive and in-depth investigation.
The results of this study have important public health implications. Rates of sexual coercion and physical violence among married couples in Malawi were relatively high and may be higher with more sensitive IPV measures. These findings bring attention to the need for violence prevention programs that challenge both long-lasting gender inequality and gender norms condoning violence against women and emerging forms of violence against men. The findings also highlight the importance of relationship context for an improved understanding marital violence. Specifically, it appears that it is not actual infidelity, but rather a partner’s perception of infidelity that is associated with IPV. In terms of potential interventions to reduce marital violence, it may be necessary to build couple communication skills that foster more open discussions around sex and extramarital sexual partnerships. These same skills could be invoked to resolve conflict or disagreements before a situation escalates to physical violence. Couple-focused approaches such as these have been relatively effective at decreasing unprotected sex and increasing condom use in couples across a variety of different settings (Burton, Darbes, & Operario, 2010). During a time of limited funding for HIV prevention in Africa, couple-based interventions that strengthen core relationship dynamics could be leveraged to simultaneously address issues related to both violence and risky sexual behavior.
While IPV can have many different consequences on health, the threat of HIV infection is of great concern in southern Malawi. Both extramarital sexual partnerships and violence are widely recognized as fueling the HIV/AIDS epidemic in this region (Halperin & Epstein, 2004; Jewkes et al., 2010). The violence perpetuated by marital partners in response to infidelity is not limited to women, but also includes their male partners—who are largely neglected in this body of research. Coercive sex with a partner who is potentially engaging in an extramarital partnership has serious implications for HIV transmission, especially if it occurs during marriage when condom use is likely to be low (Chimbiri, 2007). Although the probability of HIV transmission from women to men (versus from men to women) is significantly lower due to biological differences (Chersich & Rees, 2008), this may still be an important overlooked transmission pathway for married men. In summary, the findings in this study illustrate that risk for IPV goes beyond individual-level perceptions or risk factors. Future studies in sub-Saharan Africa should continue to explore the couple-level context of IPV in order to gain broader understandings of how sexual partners mutually affect each other’s experiences of violence and in turn, their shared risk for HIV.
Notes
Refer to http://projects.pop.psu.edu/tlt for more information about the TLT dataset, to request data access, and for replication files.
References
Agresti, A., & Finlay, B. (2009). Statistical methods for the social sciences (4th ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
Alio, A. P., Clayton, H. B., Garba, M., Mbah, A. K., Daley, E., & Salihu, H. M. (2010). Spousal concordance in attitudes toward violence and reported physical abuse in African couples. Journal of Interpersonal Violence, 26, 2790–2810.
Anglewicz, P. A., Bignami-Van Assche, S., Clark, S., & Mkandawire, J. (2008). HIV risk among currently married couples in rural Malawi: What do spouses know about each other? AIDS and Behavior, 14, 103–112.
Archer, J. (2000). Sex differences in aggression between heterosexual partners: A meta-analytic review. Psychological Bulletin, 126, 651–680.
Babcock, J., Waltz, J., Jacobson, N. S., & Gottman, J. M. (1993). Power and violence: The relationship between communication patterns, power discrepancies, and domestic violence. Journal of Consulting and Clinical Psychology, 61, 40–50.
Balmer, D. H., Gikundi, E., Kanyotu, M., & Waithaka, R. (1995). The negotiating strategies determining coitus in stable heterosexual relationships. Health Transition Review, 5, 85–95.
Blanc, A. (2001). The effect of power in sexual relationships on sexual and reproductive health: An examination of the evidence. Studies in Family Planning, 32, 189–213.
Boonzaier, F. (2005). Woman abuse in South Africa: A brief contextual analysis. Feminism and Psychology, 15, 99–103.
Burton, J., Darbes, L. A., & Operario, D. (2010). Couples-focused behavioral interventions for prevention of HIV: Systematic review of the state of evidence. AIDS and Behavior, 14, 1–10.
Campbell, J. (2002). Health consequences of intimate partner violence. Lancet, 359, 1331–1336.
Chersich, M. F., & Rees, H. V. (2008). Vulnerability of women in southern Africa to infection with HIV: Biological determinants and priority sector interventions. AIDS, 22(Suppl. 4), S27–S40.
Chimbiri, A. M. (2007). The condom is an ‘intruder’ in marriage: Evidence from rural Malawi. Social Science and Medicine, 64, 1102–1115.
Choi, S. Y. P., & Ting, K.-F. (2008). Wife beating in South Africa: An imbalance theory of resources and power. Journal of Interpersonal Violence, 23, 834–852.
Cohen, C. R. (1998). Statistical power analysis for the behavioral sciences (rev ed.). Hillsdale, NJ: Erlbaum.
Coleman, D. H., & Straus, M. A. (1986). Marital power, conflicts, and violence in a nationally representative sample of American couples. Violence and Victims, 1, 141–157.
Conroy, A. A. (2013). Gender, power, and intimate partner violence: A study on couples from rural Malawi. Journal of Interpersonal Violence, 29, 866–888.
Cornwall, A. (2002). Spending power: Love, money, and the reconfiguration of gender relations in Ada-Odo, Southwestern Nigeria. American Ethnologist, 29, 963–980.
Dunkle, K. L., Jewkes, R. K., Brown, H. C., Gray, G. E., McIntyre, J. A., & Harlow, S. D. (2004). Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. Lancet, 363, 1415–1421.
Dunkle, K. L., Jewkes, R., Nduna, M., Jama, N., Levin, J., Sikweyiya, Y., et al. (2007). Transactional sex with causal and main partners among young South African men in the rural Eastern Cape: Prevalence, predictors, and associations with gender-based violence. Social Science and Medicine, 65, 1235–1248.
Dworkin, S. L., Treves-Kagan, S., & Lippman, S. A. (2013). Gender-transformative interventions to reduce HIV risks and violence with heterosexually-active men: A review of the global evidence. AIDS and Behavior, 17, 2845–2863.
Fonck, K., Leye, E., Kidula, N., Ndinya-Achola, J., & Temmerman, M. (2005). Increased risk of HIV in women experiencing physical partner violence in Nairobi, Kenya. AIDS and Behavior, 9, 335–339.
Frieze, I. H. (1983). Investigating the causes and consequences of marital rape. Signs, 8, 532–553.
Gage, A. J., & Hutchinson, P. L. (2006). Power, control, and intimate partner violence in Haiti. Archives of Sexual Behavior, 35, 11–24.
Garcia-Moreno, C., Jansen, H. A., Ellsberg, M., Heise, L., & Watts, C. H. (2006). Prevalence of intimate partner violence: Findings from the WHO multi-country study on women’s health and domestic violence. Lancet, 368, 1260–1269.
Gass, J. D., Stein, D. J., Williams, D. R., & Seedat, S. (2011). Gender differences in risk for intimate partner violence among South African adults. Journal of Interpersonal Violence, 26, 2764–2789.
Glynn, J. R., Caraël, M., Buvé, A., Musonda, R. M., & Kahindo, M. (2003). HIV risk in relation to marriage in areas with high prevalence of HIV infection. Journal of Acquired Immune Deficiency Syndromes, 33, 526–535.
Halperin, D. T., & Epstein, H. (2004). Concurrent sexual partnerships help to explain Africa’s high HIV prevalence: Implications for prevention. Lancet, 364, 4–6.
Hatcher, A. M., Romito, P., Odero, M., Bukusi, E. A., Onono, M., & Turan, J. M. (2013). Social context and drivers of intimate partner violence in rural Kenya: Implications for the health of pregnant women. Culture Health & Sexuality, 15, 404–419.
Helleringer, S., & Kohler, H. P. (2007). Sexual network structure and the spread of HIV in Africa: Evidence from Likoma Island, Malawi. AIDS, 21, 2323–2332.
Higgins, J. A., Hoffman, S., & Dworkin, S. L. (2010). Rethinking gender, heterosexual men, and women’s vulnerability to HIV/AIDS. American Journal of Public Health, 100, 435–442.
Hox, J. J., & Kreft, I. G. G. (1994). Multilevel analysis methods. Sociological Methods and Research, 22, 283–299.
Jewkes, R. (2002). Intimate partner violence: Causes and prevention. Lancet, 359, 1423–1429.
Jewkes, R., Dunkle, K. L., Nduna, M., Levin, J., Jama, P. N., Khuzwayao, N., … Duvvury, N. (2006). Factors associated with HIV sero-positivity in young, rural South African men. International Journal of Epidemiology, 35, 1455–1460.
Jewkes, R. K., Dunkle, K., Nduna, M., & Shai, N. (2010). Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: A cohort study. Lancet, 376, 41–48.
Karakurt, G., & Cumbie, T. (2012). The relationship between egalitarianism, dominance, and violence in intimate relationships. Journal of Family Violence, 27, 115–122.
Karamagi, C. A. S., Tumwine, J. K., Tylleskar, T., & Heggenhougen, K. (2006). Intimate partner violence against women in eastern Uganda: Implications for HIV prevention. BMC Public Health, 6(4), 1–12. doi:10.1186/1471-2458-6-284.
Kelley, H. H., & Thibalt, J. W. (1978). Interpersonal relations: A theory of interdependence. New York: Wiley.
Kenny, D. A., Kashy, D. A., & Cook, W. L. (2006). Dyadic data analysis. New York: Guilford Press.
Kim, J. Y., & Motsei, M. (2002). “Women enjoy punishment”: Attitudes and experiences of gender-based violence among PHC nurses in rural South Africa. Social Science and Medicine, 54, 1243–1254.
Koenig, M. A., Lutalo, T., Zhao, F., Nalugoda, F., Kiwanuka, N., Wabwire-Mangen, F., … Gray, R. (2004). Coercive sex in rural Uganda: Prevalence and associated risk factors. Social Science and Medicine, 37, 859–872.
Koenig, M. A., Lutalo, T., Zhao, F., Nalugoda, F., Wabwire-Mangen, F., Kiwanuka, N., … Gray, R. (2003). Domestic violence in rural Uganda: Evidence from a community-based study. Bulletin of the World Health Organization, 81(1), 53–60.
Krishnan, S., Rocca, C. H., Hubbard, A. E., Subbiah, K., Edmeades, J., & Padian, N. S. (2009). Do changes in spousal employment status lead to domestic violence? Insights from a prospective study in Bangalore, India. Social Science and Medicine, 70, 136–143.
Lary, H., Maman, S., Katebalila, M., & Mbwambo, J. (2004). Exploring the association between HIV and violence: Young people’s experiences with infidelity, violence, and forced sex in Dar es Salaam, Tanzania. International Family Planning Perspectives, 30, 200–206.
Leach, M. (1991). Locating gendered experience: An anthropologist’s view from a Sierra Leonian village. IDS Bulletin, 22, 44–50.
Malamuth, N. M., Sockloskie, R. J., Koss, M. P., & Tanaka, J. S. (1991). Characteristics of aggressors against women: Testing a model using a national sample of college students. Journal of Consulting and Clinical Psychology, 59, 670–681.
Maman, S., Mbwambo, J. K., Hogan, N. M., Kilonza, G. P., Campbell, J. C., Weiss, E., et al. (2002). HIV-positive women report more life-time partner violence: Findings from a voluntary counselling and testing clinic in Dar es Salaam, Tanzania. American Journal of Public Health, 92, 1331–1337.
Mbweza, E., Norr, K. F., & McElmurry, B. (2008). Couple decision making and use of cultural scripts in Malawi. Journal of Nursing Scholarship, 40, 12–19.
Morrell, R., Jewkes, R., Lindegger, G., & Hamlall, V. (2013). Hegemonic masculinity: Reviewing the gendered analysis of men’s power in South Africa. South African Review of Sociology, 44, 3–21.
National Statistical Office & ICF Macro. (2011). Malawi Demographic and Health Survey. Calverton, MD: NSO and ICF Macro.
Ntaganira, J., Muula, A. S., Masaisa, F., Dusabeyezu, F., Siziya, S., & Rudatsikira, E. (2008). Intimate partner violence among pregnant women in Rwanda. BMC Women’s Health, 8(17), 1–17. doi:10.1186/1472-6874-8-17.
Parikh, S. (2009). Modern wives, men’s infidelity, and marriage. In J. S. Hirsch, H. Wardlow, D. J. Smith, H. M. Phinney, S. Parikh, & C. A. Nathanson (Eds.), The secret: Love, marriage, and HIV (pp. 168–196). Nashville, TN: Vanderbilt University Press.
Peters, P. E. (1997). Against the odds: Matriliny, land and gender in the shire highlands of Malawi. Critique of Anthropology, 17, 189–210.
Pulerwitz, J., Gortmaker, S. L., & DeJong, W. (2000). Measuring relationship power in HIV/STD research. Sex Roles, 42, 637–660.
Reniers, G. (2003). Divorce and remarriage in rural Malawi. Demographic Research (Special Collection 1, Article 6), 173-206. doi:10.4054/DemRes.2003.S1.6.
Schatz, E. (2002). Numbers and narratives: Making sense of gender and context in rural Malawi. Unpublished doctoral dissertation, University of Pennsylvania, Philadelphia, PA.
Schatz, E. (2005). ‘Take your mat and go’! Rural Malawian women’s strategies in the HIV/AIDS era. Culture, Health & Sexuality, 7, 479–492.
Scorgie, F., Kunene, B., Smit, J. A., Manzini, N., Chersich, M. F., & Preston-Whyte, E. M. (2009). In search of sexual pleasure and fidelity: Vaginal practices in KwaZulu-Natal, South Africa. Culture, Health & Sexuality, 11, 267–283.
Sikweyiya, Y., & Jewkes, R. (2009). Force and temptation: Contrasting South African men’s accounts of coercion into sex by men and women. Culture, Health & Sexuality, 11, 529–541.
Simpson, A. (2007). Learning sex and gender in Zambia: Masculinities and HIV/AIDS risk. Sexualities, 10, 173–188.
Smith, D. J. (2009). Gender inequality, infidelity, and the social risks of modern marriage in Nigeria. In J. S. Hirsch, H. Wardlow, D. J. Smith, H. M. Phinney, S. Parikh, & C. A. Nathanson (Eds.), The secret: Love, marriage, and HIV (pp. 84–107). Nashville, TN: Vanderbilt University Press.
Swidler, A., & Watkins, S. C. (2007). Ties of dependence: AIDS and transactional sex in rural Malawi. Studies in Family Planning, 38, 147–162.
Tawfik, L., & Watkins, S. C. (2007). Sex in Geneva, sex in Lilongwe, and sex in Balaka. Social Science and Medicine, 64, 1090–1101.
van der Straten, A., King, R., Grinstead, O., Serufilira, A., & Allen, S. (1995). Couple communication, sexual coercion and HIV risk reduction in Kigali, Rwanda. AIDS, 9, 935–944.
Vyas, S., & Watts, C. (2009). How does economic empowerment affect women’s risk of intimate partner violence in low and middle income countries? A systematic review of published evidence. Journal of International Development, 21, 577–602.
Watkins, S. C. (2004). Navigating the AIDS epidemic in rural Malawi. Population and Development Review, 30, 673–705.
Watkins, S. C., & Swidler, A. (2012). Working misunderstandings: Donors, brokers, and villagers in Africa’s AIDS industry. Population and Development Review, 38(Suppl.), 197–218.
Watts, C., Keogh, E., Ndlovu, M., & Kwaramba, R. (1998). Withholding of sex and forced sex: Dimensions of violence against Zimbabwean women. Reproductive Health Matters, 6, 57–65.
Were, E., Curran, K., Delany-Moretlwe, S., Nakku-Joloba, E., Mugo, N. R., Kiarie, J., et al. (2011). A prospective study of frequency and correlates of intimate partner violence among African heterosexual HIV serodiscordant couples. AIDS, 25, 2009–2018.
Wood, K., & Jewkes, R. (1997). Violence, rape, and sexual coercion: Everyday love in a South African township. Gender and Development, 5, 41–46.
Zablotska, I. B., Gray, R. H., Koenig, M. A., Serwadda, D., Nalugoda, F., Kigozi, G., … Wawer, M. (2009). Alcohol use, intimate partner violence, sexual coercion and HIV among women aged 15-24 in Rakai, Uganda. AIDS and Behavior, 13, 225–233.
Acknowledgments
This research was supported by grants F31-MH093260 and T32-MH19105 from the National Institutes of Mental Health and grant R01-HD058366 from the National Institute of Child Health and Human Development. Special thanks to Sara Yeatman, Monica Longmore, and several anonymous reviewers for their valuable feedback on earlier versions of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Conroy, A.A. Marital Infidelity and Intimate Partner Violence in Rural Malawi: A Dyadic Investigation. Arch Sex Behav 43, 1303–1314 (2014). https://doi.org/10.1007/s10508-014-0306-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-014-0306-2