
Abstract
The present study explored the relationship between compulsive sexual behavior (CSB) and unprotected anal intercourse (UAI) for men who have sex with men (MSM) across a number of ethnic/racial groups and who used the Internet to seek sexual partners. A sample of 2,716 MSM (512 Asian, 445 Black, 683 Latino, 348 Other, 728 White) completed on online survey that collected information about their sexual behaviors with partners met online and offline. The survey also included the Compulsive Sexual Behavior Inventory (CSBI). Consistent with the notion that CSB is a stable trait, higher scores on the CSBI were associated with greater odds for engaging in UAI, regardless of the context in which sex partners were met (online or offline). Differences in median CSB scores were generally similar across racial and ethnic groups. The median CSB score was significantly higher for HIV-positive participants than for HIV-negative participants. HIV-prevention interventions are needed among MSM, but should take into account that some may be resistant to risk reduction strategies because of CSB.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A growing body of literature suggests an association between compulsive sexual behavior (CSB) and HIV risk behaviors, most notably unprotected anal intercourse with multiple partners (Coleman, Miner, Ohlerking, & Raymond, 2001; Kalichman & Rompa, 1995; Miner, Coleman, Center, Ross, & Rosser, 2007; Parsons, Bimbi, & Halkitis, 2001; Reece, Plate, & Daughtry, 2001). CSB has been defined as a syndrome characterized by the experience of sexual urges, sexually arousing fantasies, and sexual behaviors that are recurrent, intense, and a distressful interference in one’s daily functioning (Coleman, 1991; Coleman, Raymond, & McBean, 2003). CSB has also been referred to in the literature as sexual addiction (Carnes, 1991), sexual impulsivity (Barth & Kinder, 1987), or paraphilia-related disorder (Kafka, 1997, 2000). Individuals with CSB often perceive their sexual behavior to be excessive, but are unable to control it; they act out impulsively and/or are plagued by intrusive, obsessive thoughts and driven behaviors (Carnes, 1983, 1989, 1991; Coleman, 1991; Coleman et al., 2003; Kafka, 1991). CSB can cause emotional suffering and potentially lead to social, ethical, and legal sanctions and increased health risks, such as HIV infection (Coleman, 1992, 2003; Kalichman & Rompa, 1995, 2001; Reece et al., 2001).
Understanding that CSB might be a stable trait, researchers have developed scales attempting to measure the construct and found it to be correlated with sexual risk behavior. One such scale, the Sexual Compulsivity Scale (SCS), showed a correlation of high SCS scores with low in self-esteem and sensation seeking (Kalichman et al., 1994). Moreover, higher SCS scores were predictive of higher rates of unprotected sex, greater numbers of sex partners, and greater use of cocaine in HIV-positive men (Benotsch, Kalichman, & Kelly, 1999). Similar associations between high SCS scores and unprotected sexual behavior were reported for samples of male and female college students (Dodge, Reece, Cole, & Sandfort, 2004) and HIV-positive individuals (Kalichman & Rompa, 2001).
Although both men and women of any sexual orientation can suffer from CSB, there is particular interest in the relationship between CSB and HIV risk behaviors in men who have sex with men (MSM) (Reece et al., 2001). In the U.S., MSM remain the population at greatest risk for HIV (Centers for Disease Control and Prevention, 2007). Rates of safer sex among MSM have declined since the late-1990s (Ekstrand, Stall, Paul, Osmond, & Coates, 1999; Guenther-Grey et al., 2005; Katz et al., 1998; Mansergh et al., 2002). In the area of HIV prevention for MSM, it is a national priority to understand factors that may be fueling their renewed engagement in high-risk sexual behavior (CDC, 2001a, b). One such factor may be CSB. Reece et al. (2001), for example, found associations among MSMs level of sexual compulsivity and all of the following: their likelihood to participate in high-risk sexual behavior, their perceived level of responsibility to disclose HIV serostatus to sexual partners, and whether they had disclosed their HIV status to a sexual partner in their most recent act of unprotected intercourse (Reece, 2003; Reece et al., 2001).
Another emerging and unresolved issue is what relationship, if any, exists among CSB, unprotected anal intercourse (UAI), and online (vs. “offline”) sex seeking and dating. The Internet alone has been identified as a risk environment for MSM (Bull & McFarlane, 2000; Bull, McFarlane, & Reitmeijer, 2001; Horvath, Bowen, & Williams, 2006; Hospers, Harterink, van den Hoek, & Veenstra, 2002; Klausner, Wolf, Fischer-Ponce, Zolt, & Katz, 2000; McFarlane, Bull, & Rietmeijer, 2000). Features such as accessibility, affordability, anonymity, and acceptability contribute to the Internet’s popularity and, potentially, its risk (Cooper, 1998; Cooper, Crepaz, & Marks, 2001). On the one hand, these factors can reduce isolation and develop social skills in users, making the Internet a healthy dating environment (Cooper, Boise, Mahue, & Greenfield, 1999; Leiblum, 1997). On the other hand, the Internet offers nearly instant access to large numbers of potential sexual partners, some of whom may be seeking unsafe sexual experiences and with relative anonymity. Benotsch, Kalichman, and Cage (2002) found that MSM who used the Internet as a venue for seeking sexual partners (compared to men who did not) reported a greater number of sexual partners and a greater likelihood to have engaged in unprotected anal intercourse (see also Horvath et al., 2006; Tikkanen & Ross, 2000). Parsons et al. (2001) also found that CSB was associated with higher frequency of engaging in HIV sexual risk behaviors among gay/bisexual male escorts who advertised on the Internet. MSM using the internet for seeking sexual partners also reported greater use of methamphetamines and having more sexual partners (Shernoff, 2006). While men using the internet to seek sexual partners have a riskier sexual behavior profile than their counterparts, we are still uncertain to what extent the Internet may increase risk behavior beyond that which occurs when men meet partners in offline venues (Liau, Millett, & Marks, 2006). We need more study of online versus online sex-seeking behavior to resolve this question.
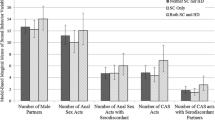
In a previous study of Latino MSM recruited via the internet, we looked for risk factors associated with unsafe sex. We found that men who scored high on the Compulsive Sexual Behavior Inventory (CSBI) (Coleman et al., 2001) and the amount of time seeking sex on the internet showed significant independent associations with unsafe sex. When these two factors were fit into a logistic regression, we found a two-factor model predicted engaging in unsafe sex. A significantly greater proportion of participants with higher scores of CSB reported having UAI with their most recent online sex partners than those with lower CSB, with similar results found for partners met offline. Latino MSM with high CSBI scores had significantly more lifetime male sexual partners, significantly more male sex partners in the last 3 months, and significantly more unprotected sex in the last 3 months than Latino MSM with low CSBI scores (Miner et al., 2007).
In the present study, we further explored the relationship between CSB and risk for unsafe sex in online and offline liaisons for MSM who use the Internet to seek sex with other men. We had two primary research questions. First, does the relationship between CSB and UAI remain among an ethnically diverse sample of Internet-using men who have sex with men? Second, does the relationship between CSB and UAI exist after controlling for key demographic factors?
Method
Participants
The research was carried out with institutional review board approval. Eligible participants were English-speaking men over the age of 18 years who self reported having had sex with another man at least once in their lifetime. This included men who self-identified as homosexual, bisexual or heterosexual. Participants had to be living in the United States, one of its territories or a U.S. military installation abroad. All races and ethnicities were invited to participate; however, the goal was to recruit 750 participants for each of five categories: Asian, Black, Latino, White, and Other. Limits were placed on enrollment when these strata were filled.
From September to November 2005, website banner advertisements for our online survey were placed on Gay.com, Latino.gay.com, and PlanetOut.com. In Leaderboard Ads and chat rooms, four advertisements were displayed, each with pictures of different races and age groups and with the text “University of Minnesota, Men’s Internet Sex Study, Earn $10—Click here now.”
The study website’s welcome page gave Internet users the following options: continue on to eligibility, resume an unfinished survey, learn more about the study, or learn about the research team. If the user chose to learn more about the study or the research team, a modal window was displayed that allowed him to view the information without accidentally closing the welcome window. Users who chose to continue were taken to an eligibility page that described the purpose of the study and payment information. Those who indicated meeting the eligibility criteria were then taken to the consent process. Payment was initially set at $10 for completing a valid survey. Because recruitment of some racial groups was slow, the amount of compensation was later increased to $20. Participants could select from a choice of payment options (Paypal, check, donation to charity, no payment). Each participant created a username and password to access the survey.
A total of 7,547 MSM passed eligibility and 6,076 enrolled and completed the human consent process. Of the 4,859 participants who started the survey, 3,035 (62%) completed it. (A priori, we chose to only use completed surveys to avoid problems of missing data and because we had sufficient complete surveys). We excluded an additional 319 (10.5%) surveys which failed to pass our de-duplication and cross-validation protocol. Thus, the final sample was comprised of 2,716 surveys. By design, a broad representation of racial and ethnic backgrounds was obtained (Table 1). Participants were young (M = 29 years; SD = 8.3) and most were sexually attracted only to men. The percentage who self-identified as HIV-positive was low (4.4%). Mean years of education was 15.5 (SD = 2.9). Mean income was US $38,475 (SD = US $93,594). Most men reported a moderate level of religiosity (Mdn = 3, M = 2.5, SD = 1.22). Few had ever been married or had children at the time of survey completion. Most men lived in metropolitan areas of the U.S., with representation from all regions. Thirteen percent of the sample self-reported being non-U.S. citizens.
Measures
The 45-min, 170-item online survey assessed participants’ sexual behaviors with partners met online and offline. The survey was adapted from that used in a previous study of Latino MSM by this research group (Ross, Rosser, Stanton, & Konstan, 2004). Participants were asked questions about their HIV status and their sexual behavior and, in particular, with their most recent online and offline sexual partner. For the purposes of this study, the participants’ risky sexual behaviors (e.g., unprotected anal intercourse) were assessed over the preceding 12 months.
The survey included 28 items from the Compulsive Sexual Behavior Inventory (CSBI) (Miner et al., 2007). Each item was scored from 1 to 5 indicating “never” to “very frequently.” A total score can range from 22 to 110. The instrument has a two factor structure, with one factor measuring behavioral discontrol and the other measuring interpersonal violence and abusive sexual behavior.Footnote 1 An example of a item relating to control is “Have you felt unable to control your sexual behavior?” An item relating to the violence factor is, “Have you forced anyone against his or her will to have sex?” These two factors show construct validity as a measure of the hypersexuality, behavioral discontrol, indulgent, and callous behavioral aspects of CSB Individuals with higher scores have shown to have significantly more lifetime male sex partners, significantly more male sex partners in the last 3 months, and significantly more unprotected sex in the last 3 months than those with low scores (Miner et al., 2007). The confirmatory factor analysis performed in that study provided evidence for the importance of both subscales is that the control and violence subscales each showed the relationship with hypersexuality and unsafe sexual behavior and there was little association between the two subscales. It appears that each subscale makes an independent and important contribution to the associations of the CSBI with hypersexuality and unsafe sex. Thus, the total CSBI score was used for analysis in this study.
Results
Differences in CSB Scores by Participant Characteristics
Participants’ CSB scores ranged from 22 to 90 with a median of 42 (M = 43.9, SD = 11.8). In bivariate analyses, several demographic factors were significantly related to CSB score. Higher CSB scores were associated with being HIV-positive (M = 46.98, SD = 12.09 vs. 43.77, SD = 11.75; t(2635) = 2.89, p < .01), not exclusively attracted to men (M = 46.06, SD = 11.45 vs. 42.75, SD = 11.78; t(2644) = 6.99, p < .001), never having been married to a woman (M = 46.02, SD = 12.88 vs. 43.77, SD = 11.70; t(2632) = 2.45, p < .05), and being a non-U.S. citizen (M = 46.02, SD = 11.76 vs. 43.59, SD = 11.76; t(2634) = 3.58, p < .001). Men who resided in rural areas had significantly higher CSB scores than men from more densely populated areas, F(4, 2679) = 7.01, p < .01. Finally, compared to men who reported that they did not consider themselves religious at all, men who endorsed being very religious had significantly higher CSB scores, F(2, 2693) = 7.01, p < .001.
Differences in CSB Scores by UAI with Most Recent Partner
Forty-nine percent (1330/2716) of participants reported having had anal intercourse with their most recent online male sexual partner. Of these, 26% (347/1330) reported having UAI with this partner. Mean CSB score was significantly higher for men who reported engaging in UAI with their most recent online partner (M = 47.31, SD = 12.75) than men who did not (M = 43.85, SD = 11.75), t(1298) = 4.43, p < .001. Forty percent (1083/2716) of participants reported having had anal intercourse with their most recent offline partner. Of these, 28% (301/1083) reported having UAI with this partner. The mean CSB score was significantly higher for men who reported engaging in UAI with their most recent offline partner (M = 45.40, SD = 12.22) than men who did not (M = 43.32, SD = 11.81), t(1081) = 2.53, p < .05.
Adjusted Multiple Logistic Regression Model for CSB Score and UAI
Results for the adjusted multiple logistic regression model are shown in Table 2. When adjusted for demographics (age, ethnicity, sexual attraction, HIV-status, education, income, occupation, religiosity, marital status, child status, residence, and U.S. citizenship), CSB was significantly related to UAI during the most recent sexual episode with both the last online and offline partner. For each unit increase in CSB score, the odds that a participant would engage in UAI rose by 1.02 (95% CI = 1.01, 1.03). The total CSB score coefficients for the most recent online and offline partner were tested for equality, adjusting for the covariation in the outcome measure. The difference between the adjusted effect of CSB on UAI between online and offline was negligible, χ2(1) = 0.80.
Figure 1 illustrates the predicted probability of UAI for every increase in 10 points in the CSBI for the five major race and ethnicity groups. The overall pattern was similar among race and ethnic groups, with White participants at slightly elevated risk and Latino participants at lowest risk among the groups.

Predicted probability of UAI by total CSB score percentile. Age set at median; sexual attraction, HIV-status, education, income, occupation, religiosity, marital status, child status, residence, and U.S. citizenship set at modal category. Asian and bi- or multiracial lines overlap. While the trend was the same for all racial/ethnic group, UAI for Latino online sexual partners was significantly lower (see Table 2)
Discussion
In this online survey study of MSM, higher CSBI scores were associated with a greater probability of engaging in UAI, even after adjusting for sociodemographic factors. This association held regardless of the context in which sex partners were met (online or offline). Further, differences in median CSB scores were similar across racial and ethnic groups.
Our results suggest that addressing CSB should be considered a part of HIV-prevention efforts strategy for MSM. This finding has been echoed by a number of investigators who examined the association between online sex seeking and CSB (e.g., Benotsch et al., 2002). Despite widespread knowledge of HIV risks and safer sex strategies, in recent years the U.S. MSM population is experiencing increases in risky sexual behavior and STI infections (CDC, 2005). One reason why HIV prevention efforts for MSM may be failing (Gross, 2003) is that current prevention programming does not address CSB in MSM. General HIV prevention interventions (e.g., public awareness campaigns, HIV testing, and counseling) are unlikely to modify personality traits or clinical syndromes. There are a number of HIV prevention interventions for MSM that are endorsed by the CDC (2008): three focus on sexual negotiation skills training (Kelly, St. Lawrence, Hood, & Brasfield, 1989; Valdiserri et al., 1989); four use counseling and motivational interviewing to enhance knowledge, self efficacy, and skills (Choi et al., 1996; Dilley et al., 2002; The Explore Study Team, 2004; Wolitski, Gomez, & Parsons, 2005); and two are community level interventions designed to influence community norms regarding the acceptability of safer sex (Kegeles, Hays, & Coates, 1996; Kelly et al., 1991). All of these efforts focus on behavioral “states” rather than “traits.” Because CSB is, by definition, a description of longer-term sexual behavior patterns experienced as outside of voluntary control, neither approach is promising to address the sexual health concerns of MSM with CSB.
If this is a clinical syndrome (and this is still being debated), access to CSB treatment should be considered (Coleman, 1991, 1992, 2003). There is certainly a danger of possible overpathologization but lack of recognition of this type of problem could be just as serious. Because CSB has also been shown to be associated with other psychiatric problems, these issues need to be addressed in HIV prevention as well (Black, Kehrberg, Flumerfelt, & Schlosser, 1997; Raymond, Coleman, & Miner, 2003).
Although the primary purpose of this study was to determine the degree to which CSB predicted UAI after adjusting for key sociodemographic factors, we also found that several sociodemographic factors independently predicted UAI. Some of these factors are documented covariates of risk behavior, such as HIV-positive status and lower income (NIMH Multisite HIV Prevention Trial Group, 1998). Regional differences in UAI were also noted, with the highest rates reported for MSM from the West or Northwest. This may be related to higher rates of amphetamine and methamphetamine use in these regions (Koblin et al., 2003). The association between U.S. citizenship and unprotected intercourse has, to our knowledge, not been shown in prior studies. Compared to White participants, Hispanic/Latino ethnicity was associated with lower UAI within online partnerships, despite surveillance data showing over-representation of this group in the HIV/AIDS epidemic in the U.S. (CDC, 2007). A previous study of Latino MSM found that higher percentages of participants engaged in sexual negotiations and serostatus disclosure with their online partners than with partners met offline; condom use rates were notably higher among Latino MSM who negotiated and/or disclosed (Carballo-Dieguez, Miner, Dolezal, Rosser, & Jacoby, 2006). Thus, the Internet may provide a safe venue for negotiating safer sex preferences, particularly for persons who face high levels of stigma, as do many Hispanic and Latino MSM.
The percentage of MSM in our sample who reported being HIV positive (<5%) was lower than that typically reported in offline studies. This is likely due to greater participation by younger men and men living outside of urban epicenters. Notably, however, HIV-positive participants in our study had significantly higher median CSBI scores than HIV-negative participants. They might be at elevated risk for transmitting HIV through unsafe sexual practices with on- and offline partners. Because of the nature of CSB, researchers designing interventions for HIV-positive MSM may find their risk behavior less amenable to change. Since most HIV positive men are sexually active and likely to be seeking partners on the Internet, more research is needed to understand them, their rates of CSB, and other associated risk factors.
Since there is no clinical criteria that has been widely established for CSB, we have to be cautious in interpreting higher scores on the CSB as indicative of some kind of psychopathology. While an association was found between higher scores on the CSBI and UAI, it is important to recognize that almost 75% of the sample was not engaging in UAI. Others who were may have been practicing serosorting and lowering risk for transmission. However, these findings do raise a concern which should be taken into account in addressing the possibility of MSM engaging in sex in a compulsive fashion and increasing the likelihood of HIV transmission.
This was a convenience sample and cannot be said to be representative of MSM. The data was collected over the internet with all of the advantages and disadvantages (including non-completers and duplicates) which are inherent in this type of research (for a fuller discussion of this, see Pequegnat et al., 2007). Our protocol attempts to reduce some of those inherent problems through validity checks. Given these limitations, this study strength is that it is one of the largest and demographically diverse studies of MSM to have been conducted in the U.S. The year of study needs to be considered given that we assessed a “snapshot” of behavior. Shifts in behaviors could occur with changes in the Internet, the sociocultural climate, and the progression of the pandemic. Because this study was cross-sectional, causality cannot be inferred. The current study relied on self-report of behaviors. The CSBI is a “paper and pencil” instrument with all of the limitations these types of instruments have. Although UAI occurred, we do not know the full context of the behavior. UAI may have occurred with seroconcordant partners, which many MSM appear to use as a risk reduction strategy (Marks et al., 1994).
Higher CSBI scores were associated with unprotected anal intercourse-in both online and offline sexual liaisons-among MSM from a variety of racial/ethnic backgrounds. Individuals with who identify traits of CSB comprise a small but important subgroup of MSM to consider as a vector for HIV transmission. Existing HIV risk reduction programs for MSM focus on behavioral skills building and changing community norms, but these strategies may not be helpful to individuals who score high on measures of CSB given the dynamics and complex nature of CSB. Psychoeducational approaches could be helpful, as could alerting people with CSB to seek more comprehensive assessment and treatment. Given the high use of the Internet for seeking sexual partners, this venue could be a good venue for intervention.
Notes
A copy of the full instrument is available from B. R. Simon Rosser, HIPS Program, Division of Epidemiology, University of Minnesota School of Public Health, 1300 South Second St., Minneapolis, MN 55454.
References
Barth, R. J., & Kinder, B. N. (1987). The mislabeling of sexual impulsivity. Journal of Sex and Marital Therapy, 13, 15–23.
Benotsch, E. G., Kalichman, S., & Cage, M. (2002). Men who have met sex partners via the internet: Prevalence, predictors, and implications for HIV prevention. Archives of Sexual Behavior, 31, 177–183.
Benotsch, E. G., Kalichman, S. C., & Kelly, J. A. (1999). Sexual compulsivity and substance use in HIV-seropositive men who have sex with men: Prevalence and predictors of high-risk behaviors. Addictive Behaviors, 24, 857–868.
Black, D. W., Kehrberg, L. L. D., Flumerfelt, D. L., & Schlosser, S. S. (1997). Characteristics of 36 subjects reporting compulsive sexual behavior. American Journal of Psychiatry, 154, 243–249.
Bull, S. S., & McFarlane, S. (2000). Soliciting sex on the Internet: What are the risks for sexually transmitted diseases and HIV? Sexually Transmitted Diseases, 27, 545–550.
Bull, S. S., McFarlane, S., & Reitmeijer, C. (2001). HIV and sexually transmitted risk behaviors among men seeking sex with men on-line. American Journal of Public Health, 91, 988–999.
Carballo-Dieguez, A., Miner, M., Dolezal, C., Rosser, B. R., & Jacoby, S. (2006). Sexual negotiation, HIV-status disclosure, and sexual risk behavior among Latino men who use the internet to seek sex with other men. Archives of Sexual Behavior, 35, 473–481.
Carnes, P. (1983). Out of the shadows: Understanding sexual addiction. Minneapolis, MN: CompCare Publishers.
Carnes, P. (1989). Contrary to love: Helping the sexual addict. Center City, MN: Hazelden Information and Educational Services.
Carnes, P. (1991). Don’t call it love: Recovering from sexual addiction. New York: Bantam.
Centers for Disease Control and Prevention (CDC). (2001a). Taking action to combat increases in STDs and HIV risk among men who have sex with men. Atlanta, GA: Author.
Centers for Disease Control and Prevention (CDC). (2001b). No turning back. Atlanta, GA: Author.
Centers for Disease Control and Prevention (CDC). (2005). Trends in HIV/AIDS diagnoses-33 states, 2001–2004. Morbidity and Mortality Weekly Report, 54, 1149–1153.
Centers for Disease Control and Prevention (CDC). (2007). HIV/AIDS Surveillance Report, 2007 (Vol. 19). Atlanta, GA: Author.
Centers for Disease Control and Prevention (CDC). (2008). Compendium of HIV prevention interventions with evidence of effectiveness. Accessed June 14, 2000 at http://cdc.gov/hiv/topics/prev_prog/rep/resources/initiatives/compendium.htm.
Choi, K.-H., Lew, S., Vittinghoff, E., Catania, J. A., Barrett, D. C., & Coates, T. J. (1996). The efficacy of brief group counseling in HIV risk reduction among homosexual Asian and Pacific Islander men. AIDS, 10, 81–87.
Coleman, E. (1991). Compulsive sexual behavior: New concepts and treatments. Journal of Psychology and Human Sexuality, 4, 37–52.
Coleman, E. (1992). Is your patient suffering from compulsive sexual behavior? Psychiatric Annals, 22, 320–325.
Coleman, E. (2003). Compulsive sexual behavior: What to call it, how to treat it? SIECUS Report, 31(5), 12–16.
Coleman, E., Miner, M., Ohlerking, F., & Raymond, N. (2001). Compulsive Sexual Behavior Inventory: A preliminary study of reliability and validity. Journal of Sex and Marital Therapy, 27, 325–332.
Coleman, E., Raymond, N., & McBean, A. (2003). Assessment and treatment of compulsive sexual behavior. Minnesota Medicine, 86(7), 42–47.
Cooper, A. (1998). Sexuality and the Internet: Surfing into the new millennium. CyberPsychology & Behavior, 1, 187–193.
Cooper, A., Boies, S., Mahue, M., & Greenfield, D. (1999). Sexuality and the internet: The next sexual revolution. In F. Muscarella & L. Szuchman (Eds.), The psychological science of sexuality: A research based approach (pp. 519–545). New York: Wiley.
Cooper, A., Crepaz, N., & Marks, G. (2001). Are negative affective states associated with HIV sexual risk behaviors? A meta-analytic review. Health Psychology, 20, 291–299.
Dilley, J. W., Woods, W. J., Sabatino, J., Lihatsh, T., Adler, B., Casey, S., et al. (2002). Changing sexual behavior among gay male repeat testers for HIV: A randomized, controlled trial of a single-session intervention. Journal of Acquired Immune Deficiency Syndromes, 30, 177–186.
Dodge, B., Reece, M., Cole, S. L., & Sandfort, T. G. M. (2004). Sexual compulsivity among heterosexual college students. Journal of Sex Research, 41, 343–350.
Ekstrand, M., Stall, R., Paul, J. P., Osmond, D. H., & Coates, T. (1999). Gay men report high rates of unprotected anal sex with partners of unknown or disconcordant HIV status. AIDS, 13, 1525–1533.
Gross, M. (2003). The second wave will drown us. American Journal of Public Health, 93, 872–881.
Guenther-Grey, C., Varnell, S., Weiser, J., Mathy, R., O’Donnell, L., Stueve, A., et al. (2005). Community intervention trial for youth study team: Trends in sexual risk-taking among urban young men who have sex with men, 1999–2002. Journal of the National Medical Association, 97, 38S–43S.
Horvath, K. J., Bowen, A. M., & Williams, M. L. (2006). Virtual and physical venues as contexts for HIV risk among rural men who have sex with men. Health Psychology, 25, 237–242.
Hospers, H. J., Harternick, P., van den Hoek, K., & Veenstra, J. (2002). Chatters on the internet: A special target group for HIV prevention. AIDS Care, 14, 539–544.
Kafka, M. P. (1991). Successful antidepressant treatment of nonparaphilic sexual addictions and paraphilias in men. Journal of Clinical Psychiatry, 52, 60–65.
Kafka, M. P. (1997). Hypersexual desire in males: An operational definition and clinical implications for males with paraphilias and paraphilia-related disorders. Archives of Sexual Behavior, 26, 505–526.
Kafka, M. P. (2000). The paraphilia-related disorders: Nonparaphilic hypersexuality and sexual compulsivity/addiction. In S. R. Leiblum & R. C. Rosen (Eds.), Principles and practice of sex therapy (pp. 471–503). New York: Guilford.
Kalichman, S. C., Adair, V., Rompa, D., Multhauf, K., Johnson, J., & Kelly, J. (1994). Sexual sensation seeking: Scale development and predicting AIDS-risk behavior among homosexually active men. Journal of Personality Assessment, 62, 385–397.
Kalichman, S. C., & Rompa, D. (1995). Sexual sensation seeking and sexual compulsivity scales: Reliability, validity, and predicting HIV risk behavior. Journal of Personality Assessment, 65, 586–601.
Kalichman, S. C., & Rompa, D. (2001). The Sexual Compulsivity Scale: Further development and use with HIV-positive persons. Journal of Personality Assessment, 76, 379–395.
Katz, M. H., McFarland, W., Guillin, V., Fenstersheib, M., Shaw, M., Kellogg, T., et al. (1998). Continuing high prevalence of HIV and risk behaviors among young men who have sex with men: The Young Men’s Survey in the San Francisco Bay area in 1992 to 1993 and in 1994 to 1995. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 19, 178–181.
Kegeles, S. M., Hays, R. B., & Coates, T. J. (1996). The Mpowerment project: A community-level HIV prevention intervention for young MSM. American Journal of Public Health, 86, 1129–1136.
Kelly, J. A., St. Lawrence, J. S., Diaz, Y. E., Stevenson, L. Y., Hauth, A. C., Brasfield, T. L., et al. (1991). HIV risk behavior reduction following intervention with key opinion leaders of population: An experimental analysis. American Journal of Public Health, 86, 1442–1445.
Kelly, J. A., St. Lawrence, J. S., Hood, H. V., & Brasfield, T. L. (1989). Behavioral intervention to reduce AIDS risk activities. Journal of Consulting and Clinical Psychology, 57, 60–67.
Klausner, J. D., Wolf, W., Fischer-Ponce, L., Zolt, I., & Katz, M. H. (2000). Tracing syphilis outbreak through cyberspace. Journal of the American Medical Association, 284, 447–449.
Koblin, B. A., Chesney, M. A., Husnik, M. J., Bozeman, S., Celum, C. L., Buchbinder, S., et al. (2003). High-risk behaviors among men who have sex with men in 6 US cities: Baseline data from the EXPLORE study. American Journal of Public Health, 93, 926–932.
Leiblum, S. R. (1997). Sex and the net: Clinical implications. Journal of Sex Education and Therapy, 22, 21–28.
Liau, A., Millett, G., & Marks, G. (2006). Meta-analytic examination of online sex-seeking and sexual risk behavior among men who have sex with men. Sexually Transmitted Diseases, 33, 576–584.
Mansergh, G., Marks, G., Colfax, G. N., Guzman, R., Rader, M., & Buchbinder, S. (2002). ‘Barebacking’ in a diverse sample of men who have sex with men. AIDS, 16, 653–659.
Marks, G., Ruis, M. S., Richardson, J. L., Reed, D., Mason, H. R. C., Sotelo, M., et al. (1994). Anal intercourse and disclosure of HIV infection among seropositive gay and bisexual men. Journal of Acquired Immune Deficiency Syndrome, 7, 866–869.
McFarlane, S., Bull, S. S., & Reitmeijer, C. (2000). The Internet as a newly emerging risk environment for sexually transmitted diseases. Journal of the American Medical Association, 284, 443–446.
Miner, M., Coleman, E., Center, B., Ross, M., & Rosser, B. R. S. (2007). The Compulsive Sexual Behavior Inventory: Psychometric properties. Archives of Sexual Behavior, 36, 579–587.
NIMH Multisite HIV Prevention Trial Group. (1998). NIMH multisite HIV prevention trial: Reducing HIV sexual risk behavior. Science, 280, 1889–1894.
Parsons, J. T., Bimbi, D., & Halkitis, P. N. (2001). Sexual compulsivity among gay/bisexual male escorts who advertise on the Internet. Sexual Addiction & Compulsivity, 8, 101–112.
Pequegnat, W., Rosser, B. R. S., Bowen, A. M., Bull, S. S., DiClemente, R. J., Bockting, W. O., et al. (2007). Conducting Internet-based HIV/STD prevention survey research: Considerations in design and evaluation. AIDS and Behavior, 11, 05–521.
Raymond, N. C., Coleman, E., & Miner, M. H. (2003). Psychiatric comorbidity and compulsive/impulsive traits in compulsive sexual behavior. Comprehensive Psychiatry, 44, 370–380.
Reece, M. (2003). Sexual compulsivity and HIV serostatus disclosure among men who have sex with men. Sexual Addiction & Compulsivity, 10, 1–11.
Reece, M., Plate, P. L., & Daughtry, M. (2001). HIV prevention and sexual compulsivity: The need for an integrated strategy of public health and mental health. Sexual Addiction & Compulsivity, 8, 157–167.
Ross, M. W., Rosser, B. R. S., Stanton, J., & Konstan, J. (2004). Characteristics of Latino men who have sex with men on the internet who complete and drop out of an internet-based sexual behavior survey. AIDS Education and Prevention, 16, 526–537.
Shernoff, M. (2006). Condomless sex: Gay men, barebacking, and harm reduction. Social Work, 51, 106–113.
The EXPLORE Study Team. (2004). Effects of a behavioural intervention to reduce acquisition of HIV infection among men who have sex with men: The EXPLORE randomised controlled study. Lancet, 364, 41–50.
Tikkanen, R., & Ross, M. W. (2000). Looking for sexual compatibility: Experiences among Swedish men in visiting Internet gay chat rooms. CyberPsychology & Behavior, 3, 605–616.
Valdiserri, R. O., Lyter, D. W., Leviton, L. C., Callahan, C. M., Kingsley, L. A., & Rinaldo, C. R. (1989). AIDS prevention in homosexual and bisexual men: Results of a randomized controlled trial evaluating two risk reduction interventions. AIDS, 3, 21–26.
Wolitski, R. J., Gomez, C. A., & Parsons, J. T. (2005). Effects of a peer-led behavioral intervention to reduce HIV transmission and promote serostatus disclosure among HIV-seropositive gay and bisexual men. AIDS, 19(Suppl. 1), S99–S110.
Acknowledgements
This study was funded by the National Institutes of Mental Health Center for Mental Health Research on AIDS, grant number 5 R01 MH063688-05. All research was carried out with the approval of the University of Minnesota Institutional Review Board, study number 0405S59661. The authors wish to acknowledge the assistance of Dr. Willo Pequegnat, project officer at NIMH, and Dr. Anne Marie Weber-Main for her critical review and editing of drafts of this article.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Coleman, E., Horvath, K.J., Miner, M. et al. Compulsive Sexual Behavior and Risk for Unsafe Sex Among Internet Using Men Who Have Sex with Men. Arch Sex Behav 39, 1045–1053 (2010). https://doi.org/10.1007/s10508-009-9507-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-009-9507-5