
Abstract
The effects of false positive and false negative physiological feedback (vaginal photoplethymograph response print-out) on women's sexual arousal were examined. Participants included women without sexual dysfunction (n=16) and women with Sexual Arousal Disorder (SAD; n=15). Measures of subjective sexual arousal, physiological sexual arousal (vaginal pulse amplitude), expectancies, affect, and anxiety were obtained in response to viewing an erotic film. Results indicated that false positive feedback significantly increased subjective levels of sexual arousal, whereas false negative feedback significantly decreased subjective levels of sexual arousal in both groups. Sexually functional women had overall higher expectancies for sexual arousal than women with SAD. Unexpectedly, false positive feedback did not significantly impact physiological sexual arousal in sexually functional women; however, it resulted in significantly decreased responses in physiological sexual arousal in women with SAD. False negative feedback had no significant effect on physiological sexual response in sexually functional women or women with SAD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In a number of laboratory studies, it has been shown that men without sexual dysfunction respond to erotic cues with positive affect, positive expectancies, and perceived control of erectile response, whereas men with a history of sexual dysfunction respond to erotic cues with negative affect, negative expectancies, and perceived lack of control of erectile response (Abrahamson, Barlow, & Abrahamson, 1989; Abrahamson, Barlow, Sakheim, Beck, & Athanasiou, 1985; Barlow, 1986). These findings have been explained in terms of a positive feedback loop whereby expectancies are shaped by an individual's recollections of past sexual experiences (Barlow, 1986). In Barlow's model, individuals with sexual dysfunction have responded unsuccessfully, whereas sexually functional individuals have responded successfully in past sexual scenarios and, thus, approach sexual scenarios with expectancies and affective responses congruent with their past experiences. While this model was initially derived to explain male sexual patterns, intuitively it seems to also represent female sexual patterns and has been applied as such by a number of researchers and theorists (e.g., Laan, Everaerd, Van Aanhold, & Rebel, 1993; Meston & Gorzalka, 1996; Palace & Gorzalka, 1990). That is, critical components of Barlow's model, including affect and expectancies, have also been shown to play an important role in the female sexual response (e.g., Heiman, 1980; Laan, Everaerd, van Bellen, & Hanewald, 1994; Palace & Gorzalka, 1990; Wiegel, Scepkowski, & Barlow, 2006).
Based on Barlow's model of sexual functioning, Bach, Brown, and Barlow (1999) aimed to further understand the cognitive aspects involved in sexual arousal by investigating the effects of false negative physiological feedback on efficacy expectancies and subsequent sexual arousal. Sexually functional men were randomly assigned to receive either false negative feedback or no feedback regarding their sexual arousal responses. Men who received feedback evidenced lowered expectancies for sexual arousal, which led to a significant decline in physiological sexual arousal. False feedback did not significantly affect subjective arousal, which is surprising given that most laboratory studies of sexual responding in men show a high concordance between erectile and self-reported sexual arousal (e.g., Heiman, 1977; Janssen & Everaerd, 1993). Levels of negative affect were also not significantly changed, suggesting that affect and expectancies for sexual arousal may operate independently in men without sexual concerns.
Adding a further dimension to the picture, Weisberg, Brown, Wincze, and Barlow (2001) found that attributions for sexual arousal responses (or lack thereof) can also impact sexual responding. In this study, sexually functional men were given false negative physiological feedback after viewing erotic films, and were given either an external (i.e., poor films) or an internal (i.e., problematic thoughts about sex) attribution for their supposed lack of response. Participants who were given false feedback with an internal attribution evidenced lower erectile responses and reported lower subjective arousal during subsequent erotic films, whereas participants given false negative feedback with an external attribution appeared relatively unaffected. Self-reported ratings of affect, expectancies, and perceived control of erectile responses were not significantly affected by the feedback manipulation. Hence, findings in sexually functional men suggest that negative feedback can impair sexual arousal and the mechanisms involved may include attributions and expectancies, but not necessarily affective responses. Based on Barlow's model, one would expect negative feedback to have an even more deleterious impact on responding in men with erectile dysfunction but, to our knowledge, there are no published studies which report on the effects of false feedback in men with sexual dysfunction.
To our knowledge, the first study to investigate the effects of false feedback in women was conducted by Palace (1995) and reported modifying dysfunctional patterns of sexual responding through the use of autonomic arousal (exposure to a fear-evoking film) and false positive physiological feedback. False physiological feedback included showing the participants a pre-recorded graph from the vaginal photoplethysmograph which showed a vasocongestive (vaginal blood volume) response similar to sexually functional women. Results indicated that both autonomic arousal and false positive physiological feedback significantly increased expectancies for sexual arousal, physiological sexual arousal, and subjective ratings of sexual arousal. The finding of an increase in both physiological and subjective arousal is noteworthy, given that most laboratory studies of arousal induction in women with sexual concerns show a low concordance between these measures (e.g., Laan & Everaerd, 1995; Meston, 2000). Participants in this study were women with mixed sexual problems, including sexual desire, arousal, orgasm, and/or pain disorders. Palace did not examine sexual response patterns separately by sexual dysfunction, which is unfortunate as this may have provided further insight into the role of expectancies on sexual responding. For example, expectations for arousal would be expected to differ substantially between women with SAD versus women who experience pain, but not arousal difficulties during intercourse.
Sipski, Rosen, Alexander, and Hamer (2000) investigated the effects of both false positive and false neutral feedback (vaginal response print-outs) in women with varying degrees of spinal cord injury and able-bodied women. All participants showed increased subjective ratings of sexual arousal following the administration of positive feedback. Physiological sexual arousal also increased following positive feedback in able-bodied participants and those with less severe degrees of spinal cord injury (SCI sensory scores of 0–23).
With regard to false negative feedback on sexual responses in women, Delizonna et al. (2001) presented sexually functional women with false negative physiological feedback, as well as either an external or an internal attribution for their supposed lack of sexual arousal response to the films. Unlike Weisberg et al.'s (2001) findings in men, false negative feedback did not significantly affect physiological or subjective arousal in women regardless of the type of attribution given (Delizonna et al., 2001).
Hence, findings in women suggest that false positive feedback enhances physiological and subjective sexual arousal in able-bodied, sexually functional women and in women with heterogeneous sexual concerns, and that expectancies may play a role in this effect. However, false negative feedback does not seem to substantially impact physiological or subjective arousal in sexually functional women. To fully understand the degree to which Barlow's (1986) model of sexual functioning can be applied to women's sexual responding, the following questions remain unexplored: (1) To what degree would negative feedback impact sexual responses in women with SAD? (2) To what degree would positive feedback impact sexual responses in women with SAD? (3) To what degree do factors such as affect, expectancies, attributions, and perceived control mediate these effects?
The purpose of the present study was to begin answering these questions by investigating the impact of both false positive and false negative feedback on subsequent sexual responding in both sexually functional women and women with SAD. The rationale for recruiting women with SAD was two-fold. First, given that the feedback is specific to sexual arousal responses, we felt it would be important to investigate the effects of feedback in a population of women with primary concerns specific to this stage of sexual responding. Second, unlike desire and orgasm concerns, both physiological and subjective levels of sexual arousal can be measured with relative ease and accuracy in a laboratory setting. We hypothesized that false positive feedback would have a greater facilitatory impact on both physiological and subjective sexual responding among sexually functional women as compared to women with SAD, and that false negative feedback would have a greater inhibitory impact on physiological and subjective sexual responding among women with SAD as compared to sexually functional women. The former of these hypotheses was based on the notion that for women with no history of sexual difficulties, positive feedback would be consistent with their past sexual experiences, and thus be more believable and more likely to be incorporated into their present sexual experience and subsequently enhance sexual arousal. The latter of these hypotheses was based on the notion that for women with a history of sexual arousal difficulties, negative feedback would be more consistent with their past sexual experiences, and thus more likely to be incorporated into their current experience and subsequently decrease sexual arousal. Based on Barlow's model of sexual functioning, we predicted that false physiological feedback would impact sexual responding through changes in expectancies, negative and positive affect, and anxiety. This study extends past research of this nature by: (1) examining sexual responses in sexually functional women and in a sample of women who meet Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000) criteria for SAD, and (2) examining the impact of both false positive feedback and false negative feedback on sexual responses in the same sample of women.
Method
Participants
Participants were 32 women recruited via local community and university advertisements. Women who responded to the advertisements were given a detailed description of the experiment, screened for inclusion/exclusion criteria, and told the purpose of the experiment was to investigate the effects of brief visual stimuli (which may include erotic content) on emotional and physiological responses.
All participants were evaluated for current sexual functioning status using the Female Sexual Function Index (FSFI; Rosen et al., 2000) and through DSM-IV-TR based (American Psychiatric Association, 2000) clinical interviews conducted via telephone by a female doctoral student in clinical psychology with previous training and work experience in DSM-IV-TR-based diagnostic assessments. Interviews began with a thorough semi-structured assessment of possible sexual concerns based on the DSM-IV-TR criteria for sexual dysfunction. The interviewer asked all callers whether they had received previous psychological diagnoses from a health care provider, including mood disorders, anxiety disorders, psychotic disorders, and/or eating disorders. Women who responded affirmatively to prior psychological diagnoses were disqualified from participating. Sixteen women were categorized as sexually functional based on the criteria of: (1) no self-report of any current sexual concerns or distress during clinical interviews, and (2) scoring within the normative range of healthy controls on the FSFI; 15 women were categorized as having SAD based on the criterion of: (1) meeting DSM-IV-TR criterion for SAD as self-reported during clinical interviews, and (2) scoring within the range of women with SAD on the FSFI on both the arousal and lubrication domains. Although all of the women included in the SAD group indicated sexual arousal concerns as their primary sexual concern during telephone interviews, many of the women indicated concerns with other areas of sexual functioning, including low sexual desire, difficulties with orgasm, and pain related to sexual activity. This is consistent with past research indicating a high degree of overlap of sexual dysfunctions in women (e.g., Wiegel, Meston, & Rosen, 2005). Specifically, of the 15 women included in the SAD group, 11 of these women fell within the dysfunctional range on the Desire subscale of the FSFI, seven within the dysfunctional range for the Orgasm subscale of the FSFI, and two within the dysfunctional range of the Pain subscale of the FSFI. Further exclusion criteria included: under the age of 18; currently pregnant; and currently receiving any medications known to affect vascular or sexual functioning, including antidepressants and anti-hypertensives. Six women were excluded during the screening process because they did not meet the inclusion criteria.
A t-test indicated that women with SAD were significantly older than sexually functional women, t(29)=−2.30, p=.03. A chi-square analysis indicated that the two groups did not differ significantly on level of education, and a likelihood ratio analysis indicated that the two groups did not differ significantly on race. T-tests verified significant differences between groups for each subscale and total score of the FSFI (see Table 1). Given that all of the women included in the clinical group met DSM-IV-TR criteria for SAD as established through clinical interviews, it is not surprising that that the largest group differences on the FSFI subscales were for the Arousal and Lubrication domains. The existence of desire and orgasm concerns among these women is consistent with literature that indicates a high comorbidity of desire, arousal, and orgasm disorders in women (e.g., Wiegel et al., 2005). See Table 1 for demographic variables and FSFI means (± SD) by group.
Measures
Subjective ratings
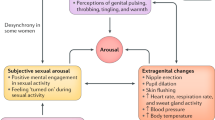
Subjective levels of sexual arousal and affect were measured using our Subjective Ratings Scale, a modified version of Heiman and Rowland's (1983) film scale. The scale consisted of 15 items measuring physical sexual arousal (4 items), mental sexual arousal (2 items), positive affect (4 items), negative affect (4 items), and anxiety (1 item). Participants rated each of the items on a 7-point Likert scale according to the degree to which they experienced the sensations. Two versions of this scale were used: (1) A pre-film version which included the prompt, “Right now, I feel” and (2) A post-film version which included the prompt, “During the last film, I felt.” Subjective physical sexual arousal was defined by the following four items: warmth in genitals, genital wetness or lubrication, genital pulsing or throbbing, and any genital feelings. Subjective mental sexual arousal was defined by the following two items: sexually aroused and sexually turned-off (reverse-scored).
Physiological sexual arousal
Physiological responding was measured using a vaginal photoplethysmograph to detect changes in vaginal pulse amplitude (VPA) (Sintchak & Geer, 1975). VPA is a measure of short-term changes in vaginal wall engorgement (Rosen & Beck, 1988) and has been found to be a sensitive measure of sexual arousal in women. Vaginal pulse amplitude was sampled at a rate of 60 samples per sec during the entire 3 min of neutral film and 5 min of erotic film, band-pass filtered (0.5–30 Hz), and recorded using the software package AcqKnowledge III, Version 3.2 (BIOPAC Systems, Inc., Santa Barbara, CA) and a Model MP100WS data acquisition unit (BIOPAC Systems, Inc.) on a Dell Pentium computer. Using the same procedures as previous studies of this nature (e.g., Meston & Heiman, 1998), psychophysiological artifacts related to movement or contractions of the pelvic muscles were deleted using the computer software program following visual inspection of the data. VPA scores (in mV) were computed for both the neutral and erotic films by averaging across the entire 180 sec of the neutral and 300 sec of the erotic film stimuli at each of the four test periods (pre-positive feedback, post-positive feedback, pre-negative feedback, and post-negative feedback). Percent-change scores from neutral-to-erotic film segments were computed for each experimental condition for use in subsequent VPA analyses.
Sexual functioning
The FSFI (Rosen et al., 2000) was used to assess for current levels of sexual functioning. The FSFI is composed of 19 items divided into factor-analytic derived subscales: desire (2 items), arousal (4 items), lubrication (4 items), orgasm (3 items), satisfaction (3 items), and pain (3 items). Rosen et al. reported inter-item reliability values within the acceptable range for sexually functional women (Cronbach's alpha=0.82–0.92), as well as for women with diagnosed SAD (Cronbach's alpha=0.89–0.95). Test-retest reliabilities assessed using a four week interval ranged between Pearson's r=0.79–0.86. In a recent study, Wiegel et al. (2005) provided strong evidence of discriminant validity between women with and without sexual dysfunction for FSFI total score and each subscale score, although a high degree of overlap was present across various diagnostic groups.
Expectancies
Expectancies for sexual arousal were assessed using the following question, “If you were in an ideal sexual situation, how aroused do you think that you could get right now?” Participants were asked to score this item on a 7-point Likert scale with “1” indicating “not at all” and “7” indicating “intensely.”
Stimulus materials
Films. Film stimuli consisted of four audiovisual films (referred to here as Film Sequence A, B, C, and D) each of which included: (a) a 1 min display of the word “relax,” (b) 3 min of a travel film (neutral stimuli), and (c) 5 min of an erotic film. The erotic stimuli depicted a heterosexual couple engaging in foreplay and sexual intercourse and have previously been shown to induce sexual arousal in women in our laboratory (e.g., Meston, 2004). Film sequences were counterbalanced across participants.
Experimental manipulation
False physiological feedback. Participants were randomly assigned to receive either false positive feedback first or false negative feedback first. All participants received both positive and negative feedback. The false feedback consisted of the female experimenter telling the participant (via the intercom) immediately after viewing Film A or C (depending on whether appointment 1 or 2) the following statement: “I am getting the preliminary record of your physiological response to the films on the computer right now. I am going print it out and I will come into the room and show it to you.” At this point, the female experimenter entered the room and showed the participant a pre-recorded analog chart depicting either an extremely heightened response (positive feedback condition) or a lack of any response at all (negative feedback condition). The female experimenter then told both groups:
Ok. Here is the print out that I am getting on the computer from the vaginal photoplethysmograph. I thought that you might be interested in seeing what it looks like so far. As I told you earlier, the vaginal probe records vaginal pulse amplitude. When a woman becomes sexually aroused, there is an increase in blood flow to the vagina. This is called “vasocongestion.” When a person is sexually aroused, thus more blood flow, these changes are reflected in the peaks you see here on the print-out. The higher the amplitude of the waves, meaning the higher the peaks you see here (experimenter pointing to the analog chart), the higher the level of sexual arousal. Conversely, the lower peaks indicate lower levels of sexual arousal.
The false positive feedback first group was then told:
You have shown an enormous response to the erotic film as you can see here by the increase in the peaks (on the analog chart) when the film changed from the neutral portion to the erotic portion. Actually right here in the print-out (experimenter pointing to the highest peak), you reached the highest level of arousal that the computer is set to record for this study. Having seen many physiological responses, I imagine that if the computer was able to record a wider range of responses that these peaks would have gone much higher. I also printed out what an average response looks like so that you could compare them and as you can tell, you responded well above average. This is good and what we like to see, so let's see how you respond to the next film. Do you have any questions?
The false negative feedback group was told:
Are you having trouble becoming aroused? The print-out from the computer shows that you aren't really responding to the erotic portion of the film as you can see by the chart here which shows no change in peaks from the neutral film to the erotic film. I also printed out what an average response looks like so that you could compare them and as you can tell, you responded below average. Let's see how you respond to the next film. Do you have any questions?
Design and procedure
A flow diagram outlining the procedures of the experimental session is depicted in Fig. 1. Following initial telephone screening interviews, women who qualified based on the inclusion criteria participated in two experimental sessions (approximately 1 hour each), scheduled 1–2 days apart. All sessions were conducted by an all-female research staff

Flow diagram of the methodology. Note. FSFI= Female Sexual Function Index, N–E= neutral-erotic stimuli; left side of figure represents Session 1 and right side of figure represents Session 2. This figure represents the positive feedback first condition; however, order of feedback administration was counterbalanced across participants and conditions
When the participant arrived, she was shown the laboratory and given a review of the general experimental procedures. The laboratory room used for data collection had an adjoining, private, and locked participant room. An intercom system allowed for communication between the participant and experimenter at all times throughout the experimental session. A television was positioned in the participant room with a recliner in front of it so that participants could sit comfortably while having a full view of the screen.
Participants were advised of their complete privacy and given verbal instructions on how to insert the vaginal probe. The orientation and depth of probe insertion was standardized using a 9×2 cm rubber position shield (Instrumentation Department of the Academic Medical Hospital in Amsterdam) which was attached to the cable at a distance of 5 cm from the center of the probe. Participants were instructed to insert the probe until the position shield was in contact with their labia. Participants were asked to remain as still as possible throughout the films in order to minimize potential movement artifacts. Participants were then instructed on the sequence of questionnaires, which were labeled and placed in completion order. The experimenter then left the room and instructed the participants to complete initial questionnaires, including a demographic questionnaire, the FSFI, expectancies for arousal, and the pre-film Subjective Ratings Scale.
After completing the questionnaires, participants were asked to insert the vaginal probe and notify the experimenter via the intercom system when they were ready to begin. Following a 10 min habituation period, Film Sequence A began on the T.V. screen. Pre-feedback percent increases in VPA were assessed during Film Sequence A and at the end of the sequence participants immediately completed the first post-film Subjective Ratings Scale. At this point, the experimenter gave the participant either false positive feedback first or false negative feedback first (dependent on random group assignment). After a 10 min resting period (in order to allow time for arousal responses to return to baseline), participants completed the expectancies for arousal question. Then, Film Sequence B began and participants immediately completed the second post-film Subjective Ratings Scale after the film.
In order to help control for potential practice and/or boredom effects associated with a repeated-measure design, the experimental session was divided into two separate appointments scheduled approximately 1–2 days apart. Thus, participants only received one type of feedback during each appointment. The exact methodological sequence was repeated for Film Sequences C and D during the second appointment. Participants who received positive feedback after Film Sequence A now received negative feedback after Film Sequence C and vice versa. Following Film Sequence D, participants were debriefed and informed regarding the actual purpose of the study through the following statement:
The information given to you regarding your arousal responses during this study was false and did not accurately reflect your actual responses. The same feedback was given verbatim to all participants. I will tell you more about why we gave you the false feedback. However, first I would like to ask you whether you felt suspicious of the feedback at any point during the study?
After this, the reason for using deception was explained and participants were paid $50 for participation. Given that participants were not debriefed until completion of the entire experiment, as per IRB requirements and in an attempt to minimize potential distress in response to receiving feedback, no more than two days was allowed to pass between each appointment.
Manipulation check
In order to assure the credibility of the false feedback, the experimenter asked participants during the debriefing interview whether they had been suspicious of the feedback. One participant indicated that she had not believed the feedback and, thus, her data were excluded from all analyses. The remaining 31 women stated that they had accepted the feedback as reflections of their own arousal responses.
Results
Order effects
In order to determine whether the order of feedback sequence significantly affected outcome variables, initial 2 (Group) ×2 (Feedback: Pre-feedback vs. Post-feedback) ×2 (Order of Feedback Administration: Positive Feedback first vs. Negative Feedback first) MANOVAS were conducted. Because feedback sequence order was not shown to affect subjective levels of sexual arousal, VPA, expectancies, positive or negative affect, or subjective levels of anxiety, this variable was excluded from further analyses.Footnote 1
Subjective responses
Data sampling and reduction
For each variable, a pre-feedback score was calculated by subtracting initial pre-film Subjective Ratings Scale scores (baseline responses) from post-film Subjective Ratings Scale scores after viewing the first film sequence (no feedback). Post-feedback scores were calculated by subtracting initial pre-film Subjective Ratings Scale scores from post-film Subjective Ratings Scale scores after viewing the second film sequence (post-feedback; see Fig. 1 for details). Thus, in order to control for the potential influence of feedback on baseline measures of arousal, the initial pre-film baseline responses obtained from the Subjective Ratings Scale were used in the calculation of difference scores of both the pre- and post- feedback subjective ratings scores. Each score was based on an average value of all questions included within each variable (e.g., subjective physical sexual arousal was defined by four questions on the Subjective Ratings Scale; thus, scores for subjective physical arousal were based on the average value of these four questions).
Subjective reports of sexual arousal
Effects of positive feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feed-back) repeated measures ANOVA indicated a significant main effect of positive feedback on subjective physical sexual arousal, F(1, 29)=5.47, p=.03, and subjective mental sexual arousal, F(1, 29)=5.95, p=.02, such that following positive feedback, participants reported significantly higher levels of sexual arousal. No significant main effects for group or interactions were found.
Effects of negative feedback
A 2 (Group)×2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA revealed a significant main effect of negative feedback on subjective physical sexual arousal, F(1, 29)=18.7, p<.001, and subjective mental sexual arousal, F(1, 29)=13.4, p=.001, such that following negative feedback, participants reported significantly lower levels of subjective sexual arousal. No significant main effects for group or interactions were found (see Fig. 2).

Mean difference scores of (+/− SEM) subjective ratings of mental and physical sexual arousal. Note. SH=Sexually health women, SAD=women with sexual arousal disorder; A=subjective mental sexual arousal, B=subjective physical sexual arousal
Physiological results
Manipulation check
To verify that the erotic films facilitated VPA responding, a 2 (Group) ×2 (Film Type: Neutral vs. Erotic) ×4 (Film Sequence A, B, C or D) MANOVA was conducted on VPA peak-to-peak values within each experimental condition (positive feedback and negative feedback). Results revealed a main effect of Film Type indicating a significant increase in VPA responses across all films with exposure to the erotic stimulus, F(1, 29)=6.08, p<.05. There were no significant main effects for film sequence (all ps>.05), and no significant interactions between group and overall physiological response to the erotic film. These findings indicate that the experimental films were effective in eliciting sexual responding.
Effects of positive feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA was used to examine whether administration of positive feedback affected VPA responses. The Group×Feedback interaction was significant, F(1, 29)=4.35, p=.05. Follow-up univariate analyses indicated that VPA responses of sexually functional women did not significantly change following positive feedback, F(1, 15)<1; however, women with SAD showed a decreased response in VPA following positive feedback, F(1, 14)=4.99, p=.04. There were no significant main effects of feedback or group.
Effects of negative feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA revealed no significant main effects for administration of feedback or group and no significant interactions were found (see Fig. 3).

Mean VPA percent change values (+/− SEM) across feedback conditions
Expectancies
Effects of positive feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA indicated that feedback did not significantly affect reported expectancies, however results did reveal a significant main effect for group where sexually functional women reported significantly higher levels of expectancies for sexual arousal than women with SAD, F(1, 29)=13.24, p=.001.
Effects of negative feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA indicated that feedback did not significantly affect reported expectancies, however results did reveal a significant main effect of group where sexually functional women reported significantly higher levels of expectancies for sexual arousal than women with SAD, F(1, 29)=11.45, p=.002.
Affect
Effects of positive feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA indicated that positive feedback did not significantly affect levels of positive affect or negative affect. Sexually functional women and women with SAD did not significantly differ on self-reported levels of positive affect or levels of negative affect and no significant interactions were found.
Effects of negative feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA revealed a significant main effect of negative feedback on positive affect, F(1, 29)=7.4, p=.01, such that, following negative feedback, women reported lower levels of positive affect. However, administration of negative feedback did not have a significant impact on levels of negative affect. Sexually functional women and women with SAD did not significantly differ on self-reported levels of positive affect and no significant interactions were found.
Anxiety
Effects of positive feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA indicated no significant main effects for group or positive feedback administration and no significant interactions were found.
Effects of negative feedback
A 2 (Group) × 2 (Feedback: Pre-feedback vs. Post-feedback) repeated measures ANOVA indicated no significant main effect of negative feedback administration, however did reveal a significant main effect for group, F(1, 29)=15.3, p=.001, such that women with SAD reported significantly higher levels of anxiety than sexually functional women. No significant interactions were found.
Discussion
In an effort to further understand the applicability of Barlow's (1986) model of sexual dysfunction to women, this study examined the effects of false positive and false negative physiological feedback on sexual arousal in sexually functional women and women with SAD. Based on Barlow's model of sexual functioning, we hypothesized that false positive feedback would have a greater facilitatory effect on sexual arousal among sexually functional women as compared to women with SAD, and that false negative feedback would have a greater inhibitory effect on sexual arousal among women with SAD as compared to sexually functional women.
Consistent with our hypotheses, false positive feedback increased subjective levels of physical and mental sexual arousal in sexually functional women. Inconsistent with our hypotheses, false positive feedback also increased subjective physical and mental sexual arousal in women with SAD and there were no significant differences between groups in the amount of increase. The finding of increases in subjective arousal in women with SAD was consistent with Palace's (1995) findings in a heterogeneous sample of women with sexual dysfunction and Sipski et al.'s (2000) findings in a group of women with spinal cord injuries.
Palace (1995) posited that the increased levels of subjective sexual arousal following positive feedback were mediated by the change in expectancies of arousal. In the present study, subjective physical and mental sexual arousal significantly increased following positive feedback in both groups, whereas there were no significant changes in expectancies following feedback. This suggests that either the increases in subjective physical and mental sexual arousal noted here were mediated by changes in mechanisms other than expectancies, or that the measure we used to assess expectancies was not sensitive or specific enough to detect the changes that occurred across feedback conditions. With regard to the latter explanation, expectancies for arousal were measured by asking participants, “If you were in an ideal sexual situation, how aroused do you think that you could get right now?” Reference to an “ideal situation” was used based on the assumption that the laboratory is not the ideal situation for becoming sexually aroused for most women. It is likely that this question was not an adequate measure for the construct of expectancies. Further, false physiological feedback was presented as a “relative” indicator of sexual arousal, meaning that it was ranked relative to how other women who have participated in laboratory studies have responded (i.e., “I also printed out what an average response looks like so that you compare them …”). Thus, assessment of expectancies relative to how other women have responded may have been more effective for detecting changes in expectancies across conditions in the present study.
The finding that, among women with SAD, positive feedback increased subjective, but decreased physiological levels of sexual arousal is intriguing. In a recent study that compared relations between subjective and physiological sexual arousal in women with and without SAD, Meston, Rellini, and McCall (2005) found that women with SAD had significantly weaker relationships between these components of sexual arousal as compared to sexually functional women. Possibly, women with an arousal disorder may be less likely than sexually functional women to attend to or detect genital cues, or they may be equally as likely to detect the cues but be less likely to interpret them as being psychologically arousing. These questions are worthy of further investigation. Knowing the extent to which a woman who suffers from an arousal disorder is impacted psychologically by changes in genital response has clear relevance for cognitive-behavioral interventions.
In the present study, sexually functional women had significantly greater expectancies for sexual arousal than did women with SAD and, in the negative feedback condition, women with SAD reported overall higher levels of anxiety than did sexually functional women. Both of these findings were consistent with Barlow's (1986) model of sexual dysfunction, which posits that individuals with sexual dysfunction approach sexual scenarios with lower expectations for arousal and higher levels of anxiety. Inconsistent with Barlow's model was that the impact of false feedback on subjective arousal was not associated with changes in anxiety, negative affect, or expectancies.
It is possible that lack of changes in negative affect and anxiety with feedback was related to the fact that women may not have been concerned with attaining an average level of VPA response during the experimental assessment. That is, a laboratory setting such as that used in the present study may not evoke the same level of performance concerns as does a real-life sexual scenario and, hence, would not have the same level of impact on mood. It is also possible that demand or performance-related concerns associated with physiological sexual arousal are more important and salient in men as compared to women. That is, a performance-related concern for a woman may be more tied to her behavioral responses in sexual scenarios (e.g., appearing interested, attractive, or “turned on”) than to a specific physiological response which is more the case with male erections. From a purely anatomical standpoint, this would make sense given that, unlike women, men are unable to perform sexually without the presence of a visible physiological response (i.e., erection). Future studies of this nature might consider examining the impact of more behavioral (e.g., whether the woman appears “sexy”) versus physiological (e.g., vaginal responding) feedback on subsequent sexual responses in women.
Consistent with our hypotheses and with predictions based on Barlow's model, false negative feedback led to decreased subjective physical and mental sexual arousal responses in women with SAD. Negative feedback also resulted in decreased reports of subjective physical and mental sexual arousal in sexually functional women and decreased ratings of positive affect in both groups of women. The finding that false negative feedback affected sexually functional women was inconsistent with the findings of Delizonna et al. (2001) in which bogus negative feedback had no effect on physiological (VPA) sexual arousal, subjective sexual arousal, or affect. These discrepant findings may be explained by the fact that specific attributions were given to women for their low arousal responses in Delizonna et al.'s (2001) study, but not in the present study.
Contrary to predictions, false positive feedback did not significantly impact physiological sexual arousal in sexually functional women and resulted in decreased responses in physiological sexual arousal in women with SAD. It is possible that for women with SAD, being informed that they were highly aroused caused some anxiety as this information violated their schematic of having trouble with sexual arousal. Although there were no group differences in anxiety in the positive feedback condition, in the negative feedback condition women with SAD did report significantly higher levels of anxiety than sexually functional women. False negative feedback did not significantly affect physiological sexual responses in sexually functional women or women with SAD. These findings suggest that, even though the feedback given pertained specifically to a physiological sexual response, the impact was more apparent at a subjective level. Thus, it is possible that receiving this type of feedback affected women's personal cognitions surrounding sexual arousal (e.g., “I feel like less of a woman because I didn't respond adequately”), but did not directly impact their genital responses. Rellini, McCall, Randall, and Meston (2005) reported huge variability between women in the degree to which subjective sexual arousal impacts genital arousal. That is, even though a woman may experience a change in subjective sexual arousal, this does not necessarily correspond with changes in physiological sexual arousal. Further, recent research indicates that the impact of subjective sexual arousal on physiological sexual arousal may be more related to whether women are attending to genital cues than whether they are experiencing subjective levels of sexual arousal (Meston, 2003). Whether this could explain the desynchrony between subjective sexual arousal and VPA responses following the administration of false positive feedback in women with SAD is a topic for further study (for a review of the literature examining the psychophysiological assessment of sexual arousal in women, see Janssen, 2002; Laan, Everaerd, & Evers, 1995; Meston, 2000; Prause & Janssen, 2006).
A potential limitation to this study was that the experimenter entering the room to provide the false feedback and ending the feedback scripts with the statement “Let's see how you respond to the next film” could have prompted demand characteristics rendering the study's hypotheses transparent. However, given that during the debriefing interviews only one participant reported that she had not believed the false feedback, it is unlikely that this was the case. We chose this methodology to be consistent with previous studies of this nature (e.g., Bach et al., 1999; Palace, 1995) and because we felt that providing visual “evidence” to support the false feedback would help to strengthen any potential subsequent effects of the feedback. The authors note that the positive feedback, which was stated as an “enormous” response, could have been interpreted by participants as atypical and thus regarded as something other than positive. Also, the false positive feedback was longer (i.e., more words) than the false negative feedback and, hence, could have been interpreted as more extreme. Although it is possible that subtle differences in the feedback wording could account for the counterintuitive finding that positive feedback decreased VPA responses in women with SAD, one would expect that, if this were the case, subjective reports of sexual arousal would have also decreased and not increased, with false positive feedback among this group of women. Future studies that obtain information from participants pertaining to how they interpreted and explained the feedback may provide further insight into how the process of receiving feedback affects subsequent sexual responses.
One aspect of the design methodology worth noting is what constituted a baseline measure of subjective responding. We used responses to the pre-film scale (prior to viewing the first film sequence) to calculate both the pre-feedback and post-feedback subjective response values (see Subjective Results for details). It is possible that this baseline measure may have been lower than had we taken another subjective measure following feedback, but prior to viewing the second film sequence. That is, difference score values for subjective responding may have been artificially magnified given that our baseline values did not take into account the fact that women had already viewed one erotic film. Given that approximately 20 minutes of time had passed before viewing the second film sequence, and based on past research using a repeated-measures design which indicate that women return to baseline levels in less time than this (e.g., Laan, Everaerd, & Evers, 1995), we believe that residual arousal from viewing the previous film had most likely subsided. We felt that it was important to use a baseline value based on the feedback instructions as opposed to residual arousal (from previous film) as this was central to our primary hypothesis, which was to examine how a feedback manipulation specifically affected women's subsequent responses.
It should also be noted that, while comparable to other psychophysiological studies of this nature (e.g., Bach et al., 1999; Meston, 2004), the sample size for the present study was small. Post-hoc power analyses examining the effects of false feedback across groups indicated a range in power from .25 to .98 for subjective responses (see Table 2 for effect sizes and power for subjective data). While these power results were comparable to those reported by Weisberg et al. (2001) (i.e., .11 to .58) in a sample of 52 men, we note that the power to detect interactions (i.e., differential impact of feedback on sexually functional women and women with SAD) would be lower, as this reduces the number of participants within each comparison group. Additionally, it should be noted that there were several trends found in the data and it is possible that had we used a larger sample, these findings might have reached significance. Another limitation related to sample size was the inclusion of both pre- and post-menopausal women in this sample. Although it is possible that different arousal mechanisms were involved for these two groups of women, given the small number of women included in the post-menopausal sample, we were unfortunately unable to conduct separate analyses.
In conclusion, findings from the current study suggest that false feedback regarding physiological sexual responding may impact women's reports of subjective sexual arousal in a direction consistent with predictions based on Barlow's (1986) model. By contrast, false feedback did not impact women's physiological sexual arousal in a manner consistent with predictions based on Barlow's model. From a theoretical standpoint, this calls into question whether genital responding is a meaningful indicator of a woman's sexual self-efficacy. It may be the case that information about one's sexual performance is more likely to impact subsequent psychological (i.e., subjective reports) and behavioral (e.g., acting confident, sexy, open, and relaxed) indices of responding in women than a physiological index, as may be more the case in male sexual responding. Future researchers using the feedback paradigm to examine female sexual responding might consider investigating the effects of feedback on specific behavioral outcomes. Additionally, future research might also examine the potential clinical implications of this study by examining the effects of partner feedback on sexual arousal in a more natural setting.
Notes
Given the significant difference in age between the two groups, all analyses were initially conducted with age added as a co-variate. Results were not substantially altered when age was accounted for; thus, the results presented in the article did not take age into account.
References
Abrahamson, D. J., Barlow, D. H., & Abrahamson, L. S. (1989). Differential effects of performance demand and distraction on sexually functional and dysfunctional males. Journal of Abnormal Psychology, 98, 241–247.
Abrahamson, D. J., Barlow, D. H., Sakheim, D. K., Beck, J. G., & Athanasiou, R. (1985). Effects of distraction on sexual responding in functional and dysfunctional men. Behavior Therapy, 16, 503–515.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Bach, A. K., Brown, T. A., & Barlow, D. H. (1999). The effects of false negative feedback on efficacy expectancies and sexual arousal in sexually functional males. Behavior Therapy, 30, 79–95.
Barlow, D. H. (1986). The causes of sexual dysfunction: The role of anxiety and cognitive interference. Journal of Consulting and Clinical Psychology, 54, 140–148.
Delizonna, L. L., Wiegel, M., Scepkowski, L., Jensen, J. M., Ramsawh, H. J., Brown, T. A., et al. (2001, October). Causal attributions and female sexual arousal: The impact of attributions for a bogus arousal difficulty on sexual arousal, cognitions, and affect. Paper presented at the annual meeting of the Female Sexual Function Forum, Boston, MA.
Heiman, J. R. (1977). A psychophysiological exploration of sexual arousal patterns in females and males. Psychophysiology, 14, 266–274.
Heiman, J. R. (1980). Female sexual response patterns: Interactions of physiological, affective, and contextual clues. Archives of General Psychiatry, 37, 1311–1316.
Heiman, J. R., & Rowland, D. L. (1983). Affective and physiological sexual response patterns: The effects of instructions on sexually functional and dysfunctional men. Journal of Psychosomatic Research, 27, 105–116.
Janssen, E. (2002). Psychophysiological measurement of sexual arousal. In M. W. Wiederman & B. E. Whitley (Eds.), Hand- book for conducting research on human sexuality (pp. 139–171). Mahwah, NJ: Lawrence Erlbaum Associates.
Janssen, E., & Everaerd, W. (1993). Determinants of male sexual arousal. Annual Review of Sex Research, 4, 211–245.
Laan, E., & Everaerd, W. (1995). Habituation of female sexual arousal to slides and film. Archives of Sexual Behavior, 24, 517–541.
Laan, E., Everaerd, W., & Evers, A. (1995). Assessment of female sexual arousal: Response specificity and construct validity. Psy- chophysiology, 32, 476–485.
Laan, E., Everaerd, W., Van Aanhold, M., & Rebel, M. (1993). Performance demand and sexual arousal in women. Behaviour Research and Therapy, 31, 25–35.
Laan, E., Everaerd, W., van Bellen, G., & Hanewald, G. (1994). Women's sexual and emotional responses to male- and female-produced erotica. Archives of Sexual Behavior, 23, 153–169.
Lynch, J. J., & Paskewitz, D. A. (1971). On the mechanisms of the feedback control of human brain wave activity. Journal of Nervous and Mental Disease, 153, 205–217.
Matsui, T., Okada, A., & Inoshita, O. (1983). Mechanism of feedback affecting task performance. Organizational Behavior & Human Performance, 31, 114–122.
Meston, C. M. (2000). The psychophysiological assessment of female sexual function. Journal of Sex Education and Therapy, 25, 6–16.
Meston, C. M. (2003, October). Determinants of women's subjective sexual arousal. Paper presented at the Annual Meeting of the International Society for the Study of Women's Sexual Health (ISSWSH), Amsterdam, The Netherlands.
Meston, C. M. (2004). The effects of hysterectomy on sexual arousal in women with a history of benign uterine fibroids. Archives of Sexual Behavior, 33, 31–42.
Meston, C. M., & Gorzalka, B. B. (1996). The effects of immediate, delayed, and residual sympathetic activation on physiological and subjective sexual arousal in women. Behaviour Research and Therapy, 34, 143–148.
Meston, C. M., & Heiman, J. R. (1998). Ephedrine-activated sexual arousal in women. Archives of General Psychiatry, 55, 652–656.
Meston, C. M., Rellini, A. H., & McCall, K. (October, 2005). The sensitivity of continuous laboratory measures of physiological and subjective sexual arousal for diagnosing women's sexual dysfunction. Poster presentation at the meeting of the International Society for the Study of Women's Sexual Health (ISSWSH), Las Vegas, Nevada.
Morokoff, P. J., & Heiman, J. R. (1980). Effects of erotic stimuli on sexually function and dysfunctional women: Multiple measures before and after sex therapy. Behaviour Research and Therapy, 18, 127–137.
Mosch, S. C. (2000). Personality correlates and mechanisms of maladaptive responding to negative feedback during cognitive testing. Dissertation Abstracts International, 61(6), 3286B.
Palace, E. M. (1995). Modification of dysfunctional patterns of sexual response through automatic arousal and false physiological feedback. Journal of Consulting and Clinical Psychology, 63, 604–615.
Palace, E. M., & Gorzalka, B. B. (1990). The enhancing effects of anxiety on arousal in sexually dysfunctional and functional women. Journal of Abnormal Psychology, 99, 403–411.
Prause, N., & Janssen, E. (2006). Blood flow: Vaginal photoplethysmography. In I. Goldstein, C. M. Meston, S. R. Davis, & A. M. Traish (Eds.), Women's sexual function and dysfunction: Study, diagnosis and treatment (pp. 359–367). London, UK: Taylor & Francis.
Rellini, A., McCall, K. M., Randall, P. K., & Meston, C. M. (2005). The relationship between self-reported and physiological measures of female sexual arousal. Psychophysiology, 42, 116–124.
Rosen, R. C., & Beck, J. G. (1988). Patterns of sexual arousal: Psychophysiological processes and clinical applications. New York: Guilford Press.
Rosen, R., Brown, C., Heiman, J., Leiblum, S., Meston, C., Shabsigh, R., et al. (2000). The female sexual function index (FSFI): A multi-dimensional self-report instrument for the assessment of female sexual function. Journal of Sex & Marital Therapy, 26, 191–208.
Schmidt, K., & Kleinbeck, U. (1990). Effects of goals and feedback on performance: Mediating mechanisms and structures of information processing. In P. J. Drenth & J. A. Sergeant (Eds.), European perspectives in psychology, Vol. 3: Work and organizational, social and economic, cross-cultural (pp. 55–66). Oxford, England: John Wiley & Sons.
Shah, P. J., O’Carroll, R. E., Rogers, A., Moffoot, A. P., & Ebmeier, K. P. (1999). Abnormal response to negative feedback in depression. Psychological Medicine, 29, 63–72.
Sintchak, G., & Geer, J. H. (1975). A vaginal plethysmograph system. Psychophysiology, 12, 113–115.
Sipski, M. L., Rosen, R., Alexander, C. J., & Hamer, R. (2000). A controlled trial of positive feedback to increase sexual arousal in spinal cord injuries. Neurorehabilitation, 15, 145–153.
Weisberg, R. B., Brown, T. A., Wincze, J. P., & Barlow, D. H. (2001). Causal attributions and male sexual arousal: The impact of attributions for a bogus erectile difficulty on sexual arousal, cognitions, and affect. Journal of Abnormal Psychology, 110, 324–334.
Wiegel, M., Meston, C. M., & Rosen, R. C. (2005). The Female Sexual Function Index (FSFI): Cross-validation and development of clinical cutoff scores. Journal of Sex and Marital Therapy, 31, 1–20.
Wiegel, M., Scepkowski, L. A., & Barlow, D. H. (2006). Cognitive and affective processes in female sexual dysfunctions. In I. Goldstein, C. M. Meston, S. R. Davis, & A. M. Traish (Eds.), Women's sexual function and dysfunction: Study, diagnosis and treatment (pp. 85–92). London, England: Taylor & Francis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McCall, K.M., Meston, C.M. The Effects of False Positive and False Negative Physiological Feedback on Sexual Arousal: A Comparison of Women with or without Sexual Arousal Disorder. Arch Sex Behav 36, 518–530 (2007). https://doi.org/10.1007/s10508-006-9140-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-006-9140-5