
Abstract
Secondary multiple regression analyses related disorder profile, probation officers’ mental health/substance use service referrals, and recidivism in 361 juvenile justice youths. Those with externalizing (disruptive behavior or substance use) disorder or substance offenses were most likely to receive service referrals. Substance disordered youths with service referrals had lower recidivism risk compared to counterparts without referrals; referral lowered the recidivism odds to approximately that for youths without a substance use disorder. Providing juvenile justice youths with systematic mental health assessment and linking those with substance use disorder to mental health and substance use services likely reduces recidivism risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Rates of mental health disorder are known to be high in youths in contact with the juvenile justice system (e.g., Colins et al. 2010; Teplin et al. 2002; Vermeiren et al. 2006; Wasserman et al. 2010). About two-thirds of incarcerated youth have at least one diagnosable psychiatric disorder. For example, in a multi-site study with almost 10,000 youths in a range of juvenile justice settings, almost 65 % of incarcerated juveniles and 60 % of detained juveniles met criteria for one or another disorder (Wasserman et al. 2010). At earlier points in justice system processing, such as court or probation intake, rates are lower, but still exceed those in the general population. For example, 35 % of those in system intake settings (such as probation intake) report one or another mental health disorder (Wasserman et al. 2010), whereas prevalence rates are approximately 15 % for adolescents in the general population (e.g., Roberts et al. 1998). Co-morbidity has been identified in over half of those in juvenile justice settings (Vermeiren et al. 2006), further highlighting their high mental health service needs.
Despite high mental health need, service access among justice-involved youths is generally low. For example, among juvenile detainees, only 40 % of those with substance use disorder and only 34 % of those with anxiety, mood, or disruptive behavior disorders had received earlier treatment in their communities (Novins et al. 1999). As further documentation of their unmet service need (Flisher et al. 1997), in one study of incarcerated youths, only 6 % received a referral to mental health services (Rogers et al. 2001). In another, among youths in various juvenile justice settings referred to juvenile courts, the court’s decision included a mental health referral for only 2 % of female and 4.5 % of male youths (Breda 2003). More recently, we found that only 14 % of juvenile probationers had been receiving mental health or substance use services in their communities prior to intake, and mental health/substance needs were newly identified in only about 25 % at probation intake (Wasserman et al. 2008), as compared to rates of disorder of approximately 35 % for youths in similar settings, and based on a similar uniform assessment (Wasserman et al. 2010). Finally, lifetime use of mental health services in incarcerated youths is lower than in counterparts in the community (Pumariega et al. 1999).
Beyond its necessity as a first step in intervention, identification of mental health status adds unique information to the prediction of recidivism above and beyond usual juvenile justice risk indicators, such as offending characteristics and demographics (Colins et al. 2009, 2011; Hoeve et al. in press; McReynolds et al. 2010; Schubert et al. 2011; Vermeiren et al. 2002; Wierson and Forehand 1995). However, links between specific disorder profiles and recidivism have been inconsistent. For example, in one study, youths with substance use disorder were more likely to commit more future substance offenses (Colins et al. 2010), while in another, substance disordered youths were less likely to re-offend (Wierson and Forehand 1995).
In several studies, relying on large sample sizes, substance use disorder with or without additional disorders has been consistently associated with elevated risk for juvenile recidivism (McReynolds et al. 2010; Schubert et al. 2011). An earlier study (Hoeve et al. in press) found that youths with substance use disorder were more likely to commit further property crimes while still juveniles, compared to counterparts without substance use disorder. Those results were consistent with the proposition that substance use causes further illegal activity (Bennett et al. 2008), as users of illicit substances are more likely to commit property crimes to obtain those substances (Goldstein 1985). That study also found that youths with substance use disorder were more likely to commit more serious re-offenses over time (Hoeve et al. in press). Thus, identifying youths with substance use disorder and referring them to specialized and effective interventions might be expected to decrease their risk for an escalating pattern of future juvenile offenses.
Studies demonstrating that mental health or substance use services can lower risk are rare indeed. While randomized controlled trials of family-focused interventions for juvenile delinquents (e.g., Multisystemic Therapy; Borduin et al. 1995; Henggeler 1999) have demonstrated effectiveness in reducing offending behavior, these programs do not consistently offer mental health components, nor do they necessarily screen for mental health concerns. In the single randomized control trial of mental health diversion for juvenile probationers that we could identify (Cuellar et al. 2006), those identified with a disorder on a standardized assessment were assigned either to a state-run mental health diversion program or to a waitlist control. Participating local specialized mental health agencies offered treatment services (e.g., individual or family therapy, medication monitoring, crisis management) and client advocacy. Diverted youths were significantly less likely to recidivate in the following year, even adjusting for demographics and offense characteristics, such as prior offending. Re-arrest dropped to 68 per 100 youth (as compared to 154 arrests per 100 youth in waitlist controls), demonstrating that mental health intervention may prevent or delay juvenile recidivism.
In sum, although disorder, particularly substance use disorder, likely increases recidivism risk and service needs are high among justice system youths, their access to mental health and substance abuse services remains low. Research on the extent to which mental health services reduce recidivism in youths in juvenile justice settings is very rare. Given that those with substance use disorder are at particularly high risk for recidivism (Hoeve et al. in press; McReynolds et al. 2010; Schubert et al. 2011), services targeting the co-occurring mental health and substance use problems of substance disordered youth would be expected to lower recidivism. Considering a formal service referral from a probation officer as an index of service access (Wasserman et al. 2008), the present study examines the contributions of disorder and service referral to juvenile recidivism.
We proceed in two steps. First, we examine which features contribute to receiving mental health and substance abuse service referrals. Next, we examine whether the substance use disorder/recidivism link is moderated by receipt of a service referral. We adjust for demographics (age, gender and ethnicity), and for prior offending, both of which features have been associated with recidivism (e.g., Cottle et al. 2001). In our earlier work, we reported gender differences in both disorder prevalence (girls endorsed higher rates of internalizing disorder; e.g., Wasserman et al. 2010) and in the disorder-recidivism association (e.g., McReynolds et al. 2010).
Method
Subjects
Youths undergoing probation or detention intake in Jefferson (n = 491), Mobile (n = 174), and Montgomery (n = 119) counties participated in a collaboration with the Center for the Promotion of Mental Health in Juvenile Justice (CPMHJJ) between 2002 and 2006. Following either a systematic universal or randomized (by day of the week) sampling protocol, depending on county, 784 youths referred to juvenile justice agencies (491 at probation intake and 293 in detention) reported on mental health status. Data from youths were previously examined in a study of the contribution of baseline disorder to recidivism (Hoeve et al. in press) and were included in the National Archive of Mental Health in Juvenile Justice, contributing to reports of the prevalence of psychiatric disorder across a range of juvenile justice settings (Wasserman and McReynolds 2011; Wasserman et al. 2010). For 575 youths, data were also available on disposition and probation officer’s mental health/substance abuse service referral. For 361 of these, we obtained information on full juvenile offense history, through December 13, 2007. As reported earlier (Hoeve et al. in press), differences between matched and non-matched youths were no different from chance, considering a range of demographic, mental health, and offense characteristics, suggesting that the impact of selective attrition was limited. Below, we report on the 361 youths with complete data on disorder, offense history and service referral.
Procedures
Before baseline, probation officers received a one-day training that included background information on mental health problems in youths in juvenile justice settings, and on how to interpret results of standardized assessments. At baseline, youths completed an audio computer-assisted diagnostic self-interview (V-DISC; Wasserman et al. 2002) soon after intake into either their county’s probation or detention system. Next, the assigned probation officer reviewed the V-DISC clinical report, along with other materials, and then made a dispositional recommendation to the judge. While they were able to incorporate V-DISC screening results into their decision making protocols, they were not required to do so. Probation officers completed a Mental Health Tracking Form for each youth, recording demographics and recommendations for mental health/substance use services. The de-identified assessment, demographic, and disposition data were sent to CPMHJJ.
A little over a year after the close of data collection (14 months), the AL Administrative Office of the Courts (AAOC) attempted to match individual youths’ assessment data to their cumulative juvenile justice records, relying on agency case number, date of birth, gender, race, county, and admit date at baseline. For each matched youth, AAOC provided the date and type of all charges, beginning with the first complaint through December 13, 2007. After AAOC returned the offense dataset to CPMHJJ, data were matched to baseline assessment results and again de-identified.
Measures
Mental Health Disorder
Youths self-assessed mental health status on the Voice Diagnostic Interview Schedule for Children (V-DISC). The V-DISC measures 20 disorders in four clusters [substance use (SUD), disruptive behavior (DBD), anxiety (ANX), and affective (AFF) disorder] based on past-month symptoms according to the DSM-IV, except for SUD and conduct disorder, which are based on symptoms within the past 12 and 6 months respectively. The V-DISC utilizes an audio computer-assisted self-interview format and has been widely used in juvenile justice settings (e.g., Wasserman et al. 2005, 2004, 2009). Finally, DISC algorithms define “subthreshold” youths as those who endorse at least half of the criteria needed for a diagnosis (Ko et al. 2004).
We created measures to denote youths who had mental health concerns: internalizing (anxiety or affective: INT alone), DBD alone, internalizing and disruptive behavior disorder (INT + DBD), substance use disorder with or without a co-occurring disorder (any SUD). We denoted youths who had at least one mental health disorder in any domain as demonstrating “any disorder”.
Service Referral
Probation officers recorded recommendations for mental health and substance abuse services to the court (disposition recommendation), as well as whether the court’s final disposition plan/program included services to address mental health/substance abuse issues. Because, consistent with earlier findings (Vilhauer et al. 2004), probation officers’ and court recommendations were highly correlated (here κ = .77; 88.6 % agreement), we only report on service recommendations from probation officers. Probation officers noted that families refused the service referral in only two instances. Because in almost 90 % of all cases, probation officers’ service recommendations were incorporated into court-ordered disposition plans, we considered probation officer service recommendations as markers of service access.
Cumulative Offense History
Complaint data (date and charge) were used as an indication of actual offending. Two types of offense data were available. Prior offenses included charges before the baseline mental health assessment (including the current offense). Subsequent offenses were charges after baseline up to age 18. We also present descriptive information separately on youths’ current offense, although analyses aggregated current offenses into prior offenses. For each youth, we calculated the number of months after the baseline mental health assessment for which offense records were reviewed, through 12/13/2007 (the “censor date”) or age 18 years, whichever came first (average length of follow-up = 18.5 months). Because no determination could be made of their seriousness, charges that referenced administrative actions (e.g., miscellaneous filing or dispositional hearing) were not examined.
Juvenile recidivism was defined dichotomously as whether or not there was any subsequent offense by age 18 years. As in an earlier study (Hoeve et al. in press), models adjusted for prior offense severity. Analyses considered the further outcomes of offense severity and frequency constructs for descriptive purposes (see Hoeve et al. in press, for a description of these constructs).
Data Analysis
First, we examined contributors to receipt of a mental health or substance abuse service referral, via logistic regression, considering those demographic and offense characteristics that had been found significantly associated in bivariate analyses. These analyses employed the full sample, because service referrals were noted both for youths who reported and those who did not report a disorder.
Approximately 40 % of youths who did not meet criteria for a disorder on the V-DISC nonetheless received service referrals (92 out of 220, see Table 1). In post hoc analyses, we examined why these youths had received referrals. Those with subthreshold mood disorders [χ2(1) = 6.3, p < .05] or subthreshold substance use disorders [χ2(1) = 10.0, p < .01] were significantly more likely to receive a referral, suggesting that, for the 19 of the 92 V-DISC-“negative” youths positive for these or for some other disorder(s), probation officers may have been attending to less severe (though still treatment-worthy) mental health or substance use concerns. Beyond this, service referrals for those not meeting criteria for a disorder on the V-DISC likely reflected impairments other than mental health problems. The reasons for service referral among juveniles not meeting criteria for a V-DISC disorder were unknown and likely quite variable. Accordingly, analyses predicting recidivism from receipt of service referral considered only those meeting criteria for one or another V-DISC disorder, as the reason for their referral was most definitive. We had a particular interest in substance disordered youths, given their very high recidivism risk (Hoeve et al. in press; McReynolds et al. 2010; Schubert et al. 2011).
For analyses predicting recidivism, we proceeded in a series of steps. In order to identify covariates for the analyses on SUD, service referral and recidivism, we first predicted recidivism from a model that included only demographic and offense characteristics. Only prior offense seriousness, gender and months reviewed were retained in final models. The first model predicted recidivism from demographic and offense features alone, including prior offense severity, number of months post-baseline of available offense data, and gender. The second model examined further contributions of substance use disorder, service referral and the substance use disorder by service referral interaction.
We found no evidence for multicollinearity in multivariate models; the variance inflation factors (VIF) were low, i.e. between values 1 and 2 for the model predicting service referral and between 1 and 3.5 for the model predicting recidivism.
Although analyses controlled for the length of follow up (months reviewed), incarceration might have further limited opportunity for offending during follow-up, so that incarcerated and non-incarcerated youths would have varied in their opportunity to reoffend. We examined regression results without youths who experienced a time in secure care after baseline. Altogether, 19 youths had been incarcerated during follow-up, either for the current offense, or for some future offense committed while a juvenile. When we removed youths incarcerated subsequent to baseline from analysis, results were essentially unchanged (available upon request).
Results
Sample Characteristics
Table 1 presents sample characteristics. At baseline the average juvenile was 15 years old; most were male and non-white. Almost half were from Jefferson County (n = 244), about a fifth from Montgomery County (n = 73), and a little over 10 % from Mobile County (n = 44). Current offenses were most commonly person-related (e.g., assault), followed by property, substance and weapon offenses. About twenty percent could not be classified into any of these offense categories (e.g., traffic offenses).
Of the 361 youths, almost 40 % (n = 141, 39 %) reported one or another disorder (Table 1). Internalizing disorders were most frequent (about 40 % of those who reported a disorder), followed by comorbid INT and DBD. About 35 % of disordered youths (n = 49) reported substance use disorder with or without a co-occurring disorder.
Predicting Service Referral
Table 1 presents bivariate associations between demographic/offense characteristics and service referral, via bivariate analyses, for the full sample. Almost half (n = 173, 48 %) received a mental health/substance abuse service referral in his/her disposition plan. Youths who received service referrals were on average a little older than counterparts not receiving referrals [t(359) = -2.6, p < .05]. The association between race and service referral was marginally significant [χ2(1) = 2.8, p < .10], with white youths slightly more likely to be referred than non-whites. Probation officers were more likely to recommend mental health/substance abuse services for youths charged with substance offenses [χ2(4) = 31.3, p < .001] than for youths with other types of current offenses.
Expectably, youths meeting criteria for a disorder were significantly more likely to get a service referral [χ2(4) = 17.5, p < .01], although about 40 % of those reporting a disorder did not receive a service referral. The likelihood of receiving a referral varied by disorder type. Among disordered youths, about two-thirds to three quarters of those with either SUD (32 of 49, 65 %), or with comorbid INT and DBD (19 of 25, 76 %) received a disposition recommendation that included mental health or substance abuse services. In contrast, only half of those with DBD alone (6 of 12) received a service referral. Of those youths endorsing INT alone only 44 % received mental health/substance abuse service referrals (24 of 55).
In predicting service referrals for the full sample, the first model, considering age and type of offense only, was significant [Table 2; χ2(2) = 32.7, p < .001; Nagelkerke R 2 = .12]. Youths who had committed substance offenses were more than one and a half times more likely than those charged with other offenses to receive referrals. Considering disorder profiles, in the second model [χ2(6) = 48.8, p < .001; Nagelkerke R 2 = .17], contributions of age and substance offense were essentially unchanged, and there was a small improvement in explained variance attributed to disorder. Compared to non-disordered youth, those reporting DBD with comorbid INT were about 5 times, and those reporting SUD with or without another disorder were about twice as likely to receive a service referral, compared to those with no disorder.
Predicting Recidivism
We next examined the degree to which receiving a mental health/substance abuse service referral impacted recidivism. Almost 40 % of the total sample and 48 % of those with a disorder recidivated as juveniles. Adjusting for demographic and offense features and for the number of months reviewed, youths with SUD were somewhat more likely to recidivate than not, while those with another disorder were somewhat less likely to recidivate than not (differences were not significant; predicted probabilities of recidivism: .56 for SUD versus .45 for other disorders). Table 3 presents results of analyses predicting juvenile recidivism in youths endorsing one or more baseline disorder. Model 1 considered demographic and offense characteristics only [χ2(3) = 25.6, p < .001; Nagelkerke R 2 = .22]. Youths whose records were reviewed for longer periods post-baseline were slightly more likely to commit additional offenses than those whose records were reviewed for shorter periods. Males were almost three times as likely as females to commit subsequent juvenile offenses.
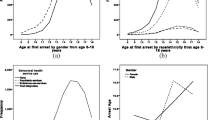
Considering service-related features and adjusting for the same set of demographic and offense characteristics [Model 2; χ2(6) = 31.2, p < .001; Nagelkerke R 2 = .27], both SUD and the SUD by service referral interaction were significantly related to recidivism. Substance disordered youths were over four times as likely to recidivate compared to youths with some other disorder. We found a significant SUD x referral interaction, indicating that the effect of referral on recidivism was significantly different for substance disordered youths, compared to those with some other disorder (Fig. 1). More specifically, among those with SUD, those who received a service referral were 66 % less likely to recidivate, compared to those without a referral (OR = .34). Adjusting for other features, the predicted probability of recidivism for youths with SUD who received a service referral was .44, compared to .71 for those with SUD who did not receive a referral. The predicted probability of recidivism for youths with a disorder other than SUD who received a service referral was .54, compared to .34 for those with a disorder other than SUD who did not receive a referral. Thus, substance disordered youths were more likely to recidivate if they did not receive a service referral, compared to either substance disordered youths with service referrals (OR = 3.0) or to youths with some other disorder either with (OR = 2.0) or without service referrals (OR = 1.5). Among substance disordered youths, service referral lowered the odds of recidivism to approximately that for youths without a substance use disorder. Adding the interaction term to the model significantly improved the model [χ2(1) = 4.8, p < .05].

Odds of recidivism for disordered youths with and without substance use disorder and with and without a service referral
Discussion
In this study of disorder characteristics, service referral and recidivism in juvenile probationers and detainees, those with externalizing (disruptive behavior and substance use) disorder or substance offenses were most likely to receive a service referral. Service referral moderated the association between substance use disorder and recidivism. To our knowledge, this is the first longitudinal investigation to show that service referrals may reduce recidivism risk among substance disordered youths. Formal service recommendations included in disposition plans by gatekeeper probation officers are, effectively, service referrals. Although in most service sectors, referral does not always result in access, given the agreement between probation officers’ and courts’ final disposition plans, here, recommendations in probation officers disposition plans likely stand as proxies for service access. In earlier work with review of juvenile probation service charts, 73 % of youths referred to mental health and substance abuse providers were noted to have accessed services (Wasserman et al. 2008).
Who Receives a Service Referral?
Those with profiles indicative of disruptive behavior and substance use disorders were considerably more likely to receive a service referral, as were those whose current charges reflected substance offenses. About 75 % of those with either substance use disorder with or without another disorder, or with comorbid disruptive behavior and internalizing disorder received service referrals. In contrast, only about 40 % of those with internalizing disorder alone received referrals.
Most earlier studies of service referral or access in youths in contact with the juvenile justice system have considered only the contributions of demographics and offense characteristics, revealing inconsistent associations with referral (e.g., Breda 2003; Carney and Buttell 2003; Grijalva et al. 2008; Gunter-Justice and Ott 1997; Rogers et al. 2001). For example, in one study, referred youths were more likely to be male (Pullmann and Heflinger 2009), while they were more likely to be female in another (Lopez-Williams et al. 2006). Study-specific associations between disorder and demographics may have been behind these discrepancies, so that these discrepancies may have resulted from their not measuring disorder in participants. Some have examined the further contribution of global mental health indicators (Lopez-Williams et al. 2006; Teplin et al. 2005), rather than specific disorder profiles, and found that “major mental disorder”, measured on the DISC 2.3 (Teplin et al. 2005), and higher number of “warning” scores on the MAYSI-2 (Lopez-Williams et al. 2006), were related to service enrollment.
Two earlier studies of justice system youths examined the more specific contributions of disorder characteristics to service referral. In one, decisions about which detainees received referrals were determined by consent decree, identifying those disorders that were to result in referrals. That set of disorders did not include either substance use or disruptive behavior disorder (Rogers et al. 2006), so that comparability with the present investigation is limited. An earlier chart review study (Wasserman et al. 2008) considered probation officers’ recorded identification of juvenile probationers’ mental health and substance use needs. Compared to rates identified by universal screening on the V-DISC in neighboring counties in the same state, probation officers identified internalizing problems at only about 5 % of the expected rate. In contrast, they identified disruptive or substance use problems at about half the expected rate. Similar results appear in studies examining other gatekeepers in other service sectors. Both parents (Weiss et al. 1997) and teachers (Summers et al. 1973) are more likely to identify externalizing than internalizing behavior, and the presence of an adolescent’s externalizing disorder may interfere with parents’ noticing commonly comorbid internalizing concerns (Weiss et al. 1997).
A possible explanation for the under-identification of those with internalizing problems is that gatekeepers often do not base their decisions on results provided by comprehensive mental health screening instruments, instead relying on “proxy variables” (Lopez-Williams et al. 2006) with weaker associations with mental health needs. Service referral in juvenile justice settings is often found to be related to other known factors that are not systematically related to mental health need, including demographic features and offense history (e.g., Breda 2003; Carney and Buttell 2003; Grijalva et al. 2008; Gunter-Justice and Ott 1997; Rogers et al. 2001).
In the present study, however, mental health status, measured with the V-DISC, was available prior to probation officers’ decisions about service referrals. While they were able to incorporate screening results into their decision making protocols, they were not required to do so. Nevertheless, even with this information available, internalizing mental health problems remained unmet.
Overall, however, rate of service referral was high compared to earlier studies: here almost half of the total sample received service referrals, compared to referral rates of 4.4 % in court-processed youths (in court-processed youths, setting undefined; Pullmann and Heflinger 2009), 6 % in detainees (Rogers et al. 2001), and 28 % in probationers in another state (Wasserman et al. 2008). Given the absence of explicit decision rules regarding which youth get a referral, it is unclear how juvenile justice gatekeepers utilize available assessment results. In an earlier study, cooperative agreements between probation and mental health agencies, training for probation officers, systematic mental health screening and explicit referral algorithms, together resulted in significantly increased service access: referred youths were almost three times more likely to access mental health or substance abuse services, compared to baseline (Wasserman et al. 2009).
Does Service Referral Reduce Recidivism?
In the present study recidivism risk for those with substance use disorder decreased threefold if they received a service referral. Considering probation officers’ service referrals as proxies for service access, these youths likely received treatment, which in turn, may have reduced their symptoms and ultimately lowered their recidivism risk. The positive impact of mental health and substance use service access is consistent with earlier findings that mental health diversion services can effectively prevent or delay recidivism in juvenile probationers (Cuellar et al. 2006). In the present study, the moderating effect of service referral was not found for youths with conditions other than substance use disorder. Comparable to other investigations (McReynolds et al. 2010; Schubert et al. 2011), we found that substance use disordered youths were more likely (here, 4.5 times as likely) to recidivate than those with other disorders. Expectably, service referral did not decrease the (already low) recidivism risk in youths with other disorders, although it may positively impact other outcomes such as suicide risk.
Although we adjusted statistically for other potential contributors to recidivism, we did not control for other important factors by random assignment of youths to service referral/no referral conditions. An experimental study would better establish to what extent reductions in juvenile recidivism might be attributable to mental health or substance abuse services. Earlier work (Cuellar et al. 2006), however, relying on randomized assignment, showed very similar results.
Study Limitations
Indication of actual service access was not available. However, because service referrals were, in most cases, incorporated into court-ordered disposition plans, it is likely that probation officers’ referrals operated as markers for service access. Another limitation is that we relied on self-reports of youths only. Disorder was measured by youth self-report, and parent reports were not available. Diagnostic agreement between youths and other informants (i.e., parents) is generally low (e.g., Colins et al. 2008; Ko et al. 2004). However, in our earlier work with the same diagnostic measure and a similar youth population, we found that youths reported more symptoms than parents, and that parents contributed little new information compared to that ascertained from youth report alone (Ko et al. 2004).
Referral data were unavailable for a considerable portion of the baseline sample, so that the sample size at follow up was reduced, and perhaps contributing to the relatively wide confidence intervals noted here. Moreover, it would have been interesting to examine the effect of service referral and substance use disorder on severity of re-offenses. An earlier study (Hoeve et al. in press) found that SUD with or without another disorder was associated with more serious re-offenses; we observed similar results for all (dichotomous, frequency and seriousness) measures of recidivism. For this reason, and because our present sample size was reduced because referral data were often unavailable, here our focus is on any juvenile recidivism, defined dichotomously.
We have confined our efforts to predicting juvenile recidivism, although examination of influences of service referral on adult recidivism would also be of interest. In addition to the above limitation (limited availability of referral data), data on adult criminal offending were also limited (only 340 of 700 baseline youths were old enough at follow up to be considered adults). As a result, we lacked power to examine whether service referral moderated the association between disorder and young adult recidivism. Future research should focus on longer term effects of service access in juvenile justice youths.
We did not measure certain other features that may have contributed to service referral. In earlier work, those whose probation officers had more knowledge about mental health, or who resided in a county without a shortage of available mental health professionals, were more likely to receive a mental health referral (Wasserman et al. 2008). Across a range of service sectors including the juvenile justice system, providers with training in and knowledge of mental health resources are more likely to recognize youths’ mental health problems and provide youths with services (Stiffman et al. 2000). Other organizational features, such as good relationships and frequent contact between justice staff and mental health providers also contribute to receipt of service referral (Pullmann and Heflinger 2009). Finally, other concerns may contribute to service referral decisions, such as family conflict or youths’ social functioning.
Policy Implications
Identification and referral to mental health or substance abuse services should be based on universal and comprehensive screening, instead of relying on factors that are unsystematically related to mental health, such as demographics or offense history. Standards for needs assessment in juvenile justice settings underscore the importance of mental health screening and assessment for identifying youths with substance use disorder and mental health problems (Skowyra and Cocozza 2006; Wasserman et al. 2003).
Those with one or another internalizing disorder were most likely to remain unidentified and consequently, the least likely to access services. Although youths with anxiety or mood disorders do not have elevated recidivism risk, their service needs should nonetheless be addressed. The prevalence of internalizing disorders in youths in juvenile justice settings is considerable (e.g., 23.2 % at system intake and 36.0 % in detention; Wasserman et al. 2010). Moreover, their elevated rates of mood disorder place juvenile system youths at increased suicide risk (Gray et al. 2002; Nolen et al. 2008). Youths with comorbid internalizing and disruptive behavior disorder are at increased risk for persistent offending into adulthood (Copeland et al. 2007; Hoeve et al. in press). Problems with both disruptive behavior and depressive symptoms may operate synergistically, resulting in a worsening course of behavior (Loeber and Keenan 1994).
Approximately 40 % of youths who did not meet criteria for a disorder on the V-DISC nonetheless received service referrals. It is possible that these youths received referrals for a disorder at the subthreshold level. We found that subthreshold mood disorders and subthreshold substance use disorders were significantly more likely to receive a referral. Service referrals for those not meeting criteria for a disorder on the V-DISC may also have reflected impairments for conditions other than diagnostic ones. In an earlier study (Wasserman et al. 2009) of probation officers’ mental health decision making, approximately half of juvenile probationers who received a service referral despite not reporting clinical disorder on the V-DISC) were referred for a problem not specific to a diagnosis, such as family conflict.
Several factors may improve the accuracy of service referral in juvenile justice youths. For example, organizational and systems features, such as probation officers’ knowledge of mental health resources, improving relations between gatekeepers and mental health providers, and improving availability of mental health services, all contribute to the accuracy of service referral in justice system youths (Colwell et al. 2012; Pullmann and Heflinger 2009; Stiffman et al. 2000; Wasserman et al. 2008) and adults (Fletcher et al. 2009). In earlier work, cooperative agreements between probation and mental health agencies, training for probation officers and systematic mental health screening, together resulted in significantly increased service access: referred youths were almost three times more likely to access mental health or substance abuse services, compared to those seen before such interventions were implemented (Wasserman et al. 2009).
Although the New Freedom Commission (U.S. Department of Health and Human Services, 2003) recommended that research on referral decisions should be a major priority, the research base describing contributors to referral decision making and to service access remains limited. As the healthcare system strives for increased efficiency, longitudinal research on contributors to and consequences of services access is key.
Information from scientifically sound mental health and substance abuse screening can contribute to the identification of those juveniles most likely to engage in a future course of offending. Identifying substance disordered youths and referring them to appropriate services decreases their recidivism risk. The present findings underscore the importance of universal comprehensive screening for mental health and substance use problems, (i.e., youths should all receive the same assessment, that can identify need across a range of conditions), adequate referral to mental health and substance use services and access to effective treatment for justice system youths.
References
Bennett, T., Holloway, K., & Farrington, D. (2008). The statistical association between drug misuse and crime: A meta-analysis. Aggression and Violent Behavior, 13, 107–118.
Borduin, C. M., Mann, B. J., Cone, L. T., Henggeler, S. W., Fucci, B. R., Blaske, D. M., et al. (1995). Multisystemic treatment of serious juvenile offenders: Long-term prevention of criminality and violence. Journal of Consulting and Clinical Psychology, 63, 569–578.
Breda, C. S. (2003). Offender ethnicity and mental health service referrals from juvenile courts. Criminal Justice and Behavior, 30, 644–667.
Carney, M. M., & Buttell, F. P. (2003). Predicting attrition to prevent service gaps in serving juvenile offenders. Journal of Offender Rehabilitation, 37, 67–79.
Colins, O., Vermeiren, R., Schuyten, G., & Broekaert, E. (2009). Psychiatric disorders in property, violent, and versatile offending detained male adolescents. American Journal of Orthopsychiatry, 79, 31–38.
Colins, O., Vermeiren, R., Schuyten, G., Broekaert, E., & Soyez, V. (2008). Informant agreement in the assessment of disruptive behavior disorders in detained minors in belgium: A diagnosis-level and symptom-level examination. Journal of Clinical Psychiatry, 69(1), 141–148.
Colins, O., Vermeiren, R., Vahl, P., Markus, M., Broekaert, E., & Doreleijers, T. A. H. (2011). Psychiatric disorder in detained male adolescents as risk factors for serious recidivism. Canadian Journal of Psychiatry, 56, 44–50.
Colins, O., Vermeiren, R., Vreugdenhil, C., Van den Brink, W., Doreleijers, T., & Broekaert, E. (2010). Psychiatric disorders in detained male adolescents: A systematic literature review. Canadian Journal of Psychiatry, 55, 255–263.
Colwell, B., Villarreal, S. F., & Espinosa, E. M. (2012). Preliminary outcomes of a preadjudication diversion initiative for juvenile justice involved youth with mental health needs in Texas. Criminal Justice and Behavior, 39, 447–460.
Copeland, W. E., Miller-Johnson, S., Keeler, G., Angold, A., & Costello, E. J. (2007). Childhood psychiatric disorders and young adult crime: A prospective, population-based study. American Journal of Psychiatry, 164, 1668–1675.
Cottle, C. C., Lee, R. J., & Heilbrun, K. (2001). The prediction of criminal recidivism in juveniles: A meta-analysis. Criminal Justice and Behavior, 28, 367–394.
Cuellar, A. E., McReynolds, L. S., & Wasserman, G. A. (2006). A cure for crime: Can mental health treatment diversion reduce crime among youth? Journal of Policy Analysis and Management, 25, 197–214.
Fletcher, B. W., Lehman, W. E., Wexler, H. K., Melnick, G., Taxman, F. S., & Young, D. W. (2009). Measuring collaboration and integration activities in criminal justice and substance abuse treatment agencies. Drug and Alcohol Dependence, 101, 191–201.
Flisher, A. J., Kramer, R. A., Grosser, R. C., Alegria, M., Brid, H. R., Bourdon, K. H., et al. (1997). Correlates of unmet need for mental health services by children and adolescents. Psychological Medicine, 27, 1145–1154.
Goldstein, J. P. (1985). The drugs/violence nexus: A tripartite conceptueal framework. Journal of Drug Issues, 15, 493–506.
Gray, D., Achilles, J., Keller, T., Tate, D., Haggard, L., Rolfs, R., et al. (2002). Utah youth suicide study, phase I: Government agency contact before death. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 427–434.
Grijalva, F. E., Ford, J. D., Docherty, A. R., Fricker-Elhai, A. E., & Elhai, J. D. (2008). Sociodemographic associations with mental health and residential care utilization among juvenile delinquents. Psychological Services, 5, 153–160.
Gunter-Justice, T. D., & Ott, D. A. (1997). Who does the family court refer for psychiatric services? Journal of Forensic Science, 42, 1102–1104.
Henggeler, S. W. (1999). Multisystemic Therapy: An overview of clinical procedures, outcomes, and policy implications. Child Psychology and Psychiatry Review, 4, 2–10.
Hoeve, M., McReynolds, L. S., McMillan, C., & Wasserman, G. A. (in press). The influence of mental health disorders on severity of re-offending in juveniles. Criminal Justice and Behavior.
Ko, S. J., Wasserman, G. A., McReynolds, L. S., & Katz, L. M. (2004). Contribution of parent report to Voice DISC-IV diagnosis among incarcerated youths. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 868–877.
Loeber, R., & Keenan, K. (1994). Interaction between conduct disorder and its comorbid conditions: Effects of age and gender. Clinical Psychology Review, 14, 497–523.
Lopez-Williams, A., Stoep, A. V., Kuo, E., & Stewart, D. G. (2006). Predictors of mental health service enrollment among juvenile offenders. Youth Violence and Juvenile Justice, 4, 266–280.
McReynolds, L. S., Schwalbe, C. S., & Wasserman, G. A. (2010). The contribution of psychiatric disorder to juvenile recidivism. Criminal Justice and Behavior, 37, 204–216.
Nolen, S., McReynolds, L. S., DeComo, R. E., John, R., Keating, J. M., & Wasserman, G. A. (2008). Lifetime suicide attempts in juvenile assessment center youth. Archives of Suicide Research, 12, 111–123.
Novins, D. K., Duclos, C. W., Martin, C., Jewett, C. S., & Manson, S. M. (1999). Utilization of alcohol, drug, and mental health treatment services among American Indian adolescent detainees. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 1102–1108.
Pullmann, M. D., & Heflinger, C. A. (2009). Community determinants of substance abuse treatment referrals from juvenile courts: Do rural youths have equal access? Journal of Child and Adolescent Substance Abuse, 18, 359–378.
Pumariega, A. J., Atkins, D. L., Rogers, K., Montgomery, L., Nybro, C., Caesar, R., et al. (1999). Mental health and incarcerated youth II: Service utilization. Journal of Child and Family Studies in Higher Education, 8, 205–215.
Roberts, R. E., Attkisson, C. C., & Rosenblatt, A. (1998). Prevalence of psychopathology among children and adolescents. American Journal of Psychiatry, 155, 715–725.
Rogers, K. M., Pumariega, A. J., Atkins, D. L., & Cuffe, S. P. (2006). Conditions associated with identification of mentally ill youths in juvenile detention. Community Mental Health Journal, 42, 25–40.
Rogers, K. M., Zima, B. T., Powell, E., & Pumariega, A. J. (2001). Who is referred to mental health services in the juvenile justice system? Journal of Child and Family Studies, 10, 485–494.
Schubert, C. A., Mulvey, E. P., & Glasheen, C. (2011). Influence of mental health and substance use problems and criminogenic risk on outcomes in serious juvenile offenders. Journal of the American Academy of Child and Adolescent Psychiatry, 50, 925–937.
Skowyra, K. R., & Cocozza, J. J. (2006). Blueprint for Change: A comprehensive model for the identification and treatment of youth with mental health needs in contact with juvenile justice system. Delmar: National Center for Mental Health and Juvenile Justice.
Stiffman, A. R., Hadley-Ives, E., Doré, P., Polgar, M., Horvath, V. E., Striley, C., et al. (2000). Youths’ access to mental mealth services: The role of providers’ training, resource connectivity, and assessment of need. Mental Health Services Research, 2, 141–154.
Summers, D. A., Faucher, T., & Chapman, S. B. (1973). A note on nonprofessional judgments of mental health. Community Mental Health, 9, 169–177.
Teplin, L. A., Abram, K. M., McClelland, G. M., Dulcan, M. K., & Mericle, A. A. (2002). Psychiatric disorders in youth in juvenile detention. Archives of General Psychiatry, 59, 1133–1143.
Teplin, L. A., Abram, K. M., McClelland, G. M., Washburn, J. J., & Pikus, A. K. (2005). Detecting mental disorder in juvenile detainees: Who receives services. American Journal of Public Health, 96, 1773–1780.
Vermeiren, R., Jespers, I., & Moffitt, T. E. (2006). Mental health problems in juvenile justice populations. Child and Adolescent Psychiatric Clinics of North America, 15, 333–351.
Vermeiren, R., Schwab-Stone, M., Ruchkin, V., De Clippele, A., & Deboutte, D. (2002). Predicting recidivism in delinquent adolescents from psychological and psychiatric assessment. Comprehensive Psychiatry, 43, 142–149.
Vilhauer, J. S., McReynolds, L. S., Wasserman, G. A., & Wahl, R. (2004). Probation officers’ mental health knowledge and practices. Perspectives, 28(3), 28–32.
Wasserman, G. A., Jensen, P. S., Ko, S. J., Cocozza, J., Trupin, E., Angold, A., et al. (2003). Mental health assessments in juvenile justice: Report on the consensus conference. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 751–761.
Wasserman, G. A., & McReynolds, L. S. (2011). Contributors to traumatic exposure and posttraumatic stress disorder in juvenile justice youths. Journal of Traumatic Stress, 24, 422–429.
Wasserman, G. A., McReynolds, L. S., Ko, S. J., Katz, L. M., & Carpenter, J. R. (2005). Gender differences in psychiatric disorders at juvenile probation intake. American Journal of Public Health, 95, 131–137.
Wasserman, G. A., McReynolds, L. S., Ko, S. J., Katz, L. M., Cauffman, E., Haxton, W., et al. (2004). Screening for emergent risk and service needs among incarcerated youth: Comparing MAYSI-2 and voice DISC-IV. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 629–639.
Wasserman, G. A., McReynolds, L. S., Lucas, C. P., Fisher, P., & Santos, L. (2002). The voice DISC-IV with incarcerated male youths: Prevalence of disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 314–321.
Wasserman, G. A., McReynolds, L. S., Musabegovic, H., Whited, A. L., Keating, J. M., & Huo, Y. (2009). Evaluating project connect: Improving juvenile probationers’ mental health and substance use service access. Administration and Policy in Mental Health and Mental Health Services Research, 36, 393–405.
Wasserman, G. A., McReynolds, L. S., Schwalbe, C. S., Keating, J. M., & Jones, S. A. (2010). Psychiatric disorder, comorbidity, and suicidal behavior in juvenile justice youth. Criminal Justice and Behavior, 37, 1361–1376.
Wasserman, G. A., McReynolds, L. S., Whited, A. L., Keating, J. M., Musabegovic, H., & Yanling, H. (2008). Juvenile probation officers’ mental health decision making. Administration and Policy in Mental Health and Mental Health Services Research, 35, 410–422.
Weiss, B., Jackson, E. W., & Susser, K. (1997). Effect of co-occurrence on the referability of internalizing and externalizing problem behavior in adolescents. Journal of Clinical Child Psychology, 26, 198–204.
Wierson, M., & Forehand, R. (1995). Predicting recidivism in juvenile delinquents: The role of mental health diagnoses and the qualification of conclusion by race. Behaviour Research and Therapy, 33, 63–67.
Acknowledgments
This work was supported by the Carmel Hill Fund and by a Marie Curie grant of the European Union awarded to Machteld Hoeve (FP7-PEOPLE-2010-IOF, project 274337).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hoeve, M., McReynolds, L.S. & Wasserman, G.A. Service Referral for Juvenile Justice Youths: Associations with Psychiatric Disorder and Recidivism. Adm Policy Ment Health 41, 379–389 (2014). https://doi.org/10.1007/s10488-013-0472-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10488-013-0472-x