
Abstract
The goal of this investigation was to explore changes in psychotherapy utilization for patients with major depressive disorder (MDD) treated in community mental health agencies across two cohorts. We used a Medicaid claims database including approximately 300,000 public sector clients. Although the use of psychotherapy alone showed a small decrease, there was a large increase in the use of combined medication and psychotherapy as a treatment for MDD. Race was a significant predictor of both treatment type received and length of treatment. African American consumers were more likely to receive psychotherapy alone than combined treatment and attended significantly fewer psychotherapy sessions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
There are many factors that have potentially influenced the utilization of psychotherapy as a treatment for major depressive disorder (MDD) in the United States, including both consumer preferences and beliefs as well as clinician biases regarding diagnosis and treatment. In addition, profound changes in the organization and financing of services for all mental disorders (Olfson et al. 2002a) over the past two decades have resulted in limits on the number of visits and the amount of reimbursement per visit for psychotherapeutic services. Further, the development of a new generation of antidepressants (serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors) has provided consumers with an easy and effective alternative to psychotherapy. The ease of dispensing medications relative to the weekly commitment of psychotherapy, as well as substantial evidence of the efficacy of these medications in treating MDD (Mulrow et al. 1999), has had a profound impact on the treatment of MDD in the community mental health system.
Changes in treatment guidelines for depression have also influenced the utilization of psychotherapy for the treatment of MDD. Although the American Psychological Association (American Psychological Association 1993) listed a number of empirically supported psychotherapies as efficacious in the treatment of MDD, the American Psychiatric Association (American Psychiatric Association 2000) specifically recommended evidence-based psychotherapies for the treatment of only mild to moderate depression. For the treatment of severe depression, psychotherapy was recommended only in combination with medication.
In order to evaluate how these variables have actually impacted the utilization of psychotherapy in the general United States population, Olfson et al. (2002b) compared the utilization of psychotherapy for participants of the 1987 National Medical Expenditure Survey to participants of the 1997 Medical Expenditure Panel Survey. Despite a steady utilization of psychotherapy of between 3.2 and 3.6% of the American population across the decade (Olfson et al. 2002a), psychotherapy as an outpatient treatment for depressive disorders significantly decreased across the decade from 71 to 61% while the utilization of medication as a treatment for depressive disorders significantly increased from 37 to 75% of those seeking outpatient services for depressive disorders (Olfson et al. 2002a). Although there was a small decrease in the utilization of psychotherapy, the most interesting finding was that the advent of newer, more effective medications for depression did not eliminate the utilization of psychotherapy as a treatment for depression, but rather had resulted in a large increase in the number of users of psychotherapy who were concurrently using an antidepressant among those with depressive disorders (23.2% in 1987 up to 45.2% by 1997).
Although the national samples evaluated by Olfson et al. 2002a suggest that psychotherapy, usually in combination with medication, is still a common treatment for depressive disorders in this country, little is known about changes in treatment modalities for MDD in the publicly funded, community mental health system. Although the community mental health system provides service to a relatively small percentage of the general population, there are a large number of individuals with the most serious mental disorders treated in this sector. Thus, the utilization trends found in the general population may not be representative of the trends in treatment settings that serve primarily minority and low income consumers on medical assistance or other forms of public support. Furthermore, though the community mental health system is charged with providing quality services, it has few resources. As a result, it is possible that these venues have been forced to alter treatment approaches to meet the financial demands of providing services to consumers of low socio-economic status.
In addition to organizational, financial, and policy variables that may influence the utilization of psychotherapy, the research literature suggests that demographic characteristics influence the types of treatment sought and received for mental disorders. It has been shown that African American consumers are less likely to seek treatment for mental disorders (Padgett et al. 1994a; Diala et al. 2000, 2001) and use fewer services than Caucasian consumers (Padgett et al. 1994a, b). Gender has also been found to predict treatment utilization among mental health services consumers. Women, especially lower income, female consumers, have identified a number of barriers to mental health service use including the unavailability of childcare and concerns about the stigma associated with mental health treatment (Alvidrez and Azocar 1999). Finally, age has also been demonstrated to be a significant factor in the utilization of mental health services, with older adults showing a preference for psychotherapy over medications as a treatment for depression (Lundervold and Lewin 1990).
To date, no studies have specifically examined treatment trends in community mental health settings where major policy changes, including a move toward deinstitutionalization and the implementation of mandated managed behavioral health programs for publicly funded clients have taken place. Our goal was to use a large Medicaid claims database to evaluate the utilization of psychotherapy as a treatment for MDD in the community mental health system in light of policy shifts and changes in treatment availability. Additionally, we sought to evaluate whether consumer demographic variables continued to influence treatments received for MDD despite these policy and organizational changes.
The current investigation has three specific goals. First, we provide descriptive results for the types and lengths of treatments received by consumers of mental health services for MDD in the community mental health system. Second, we examine whether patterns of utilization of psychotherapy and pharmacotherapy have changed among mental health consumers seeking treatment for MDD in the community mental health system from 1993 to 2003. Third, we examine whether consumer demographic variables predict the type or length of treatment received for MDD in community settings. Based on the literature reviewed above, we hypothesized that there would be a small decrease in the utilization of psychotherapy as a treatment for MDD across the decade and an increase in the utilization of combined medication and psychotherapy. We also hypothesized that African American consumers, as well as female consumers, would receive fewer sessions, and that older consumers would be more likely to receive psychotherapy alone as a treatment for MDD.
Method
The current study utilized the Penn Longitudinal Database to examine patterns of treatment utilization for MDD in the community mental health system of Philadelphia.
Data Source
The data used in this study came from Medicaid claims and eligibility records for Medicaid-eligible adult recipients in Philadelphia in 1993 and 2003. Medicaid is a principal payer of services for persons with serious mental illness and major disability and thus provides information on a large number of cases. As such, these claims are useful for conducting population-based studies and detecting variations in practice patterns. The behavioral health claims files used in these analyses contain records of all outpatient mental health services for the Medicaid eligible population. Since providers are paid based on actual visits and revenue is dependent upon information accuracy, the claims represent a reasonably accurate measure of care provided. The claims files provide both person-level, socio-demographic information and service-level information, including date of service use and diagnostic codes. Services including outpatient medication and psychotherapy visits were extracted for these analyses.
Study Participants
Study participants consisted of two cohorts of Medicaid recipients, one in 1993 and one in 2003. Prior to 1997, the majority of Medicaid recipients received behavioral healthcare services from providers who were contracted by the county mental health program and paid on a fee-for-service basis. Approximately 17% of the Medicaid enrollees in 1993 were under a Medicaid waiver demonstration program and received services through a Health Maintenance Organization which used their own behavioral health care provider network. The records of these individuals were not available for analysis. Since 1997, the Pennsylvania Department of Public Welfare has had a mandatory managed care program for all Medical Assistance recipients in the study site and assigns the management of behavioral health to a single managed care organization. The publicly funded provider network in 2003 remained the same as it was in 1993 for the first cohort, and the service providers continued to be paid on a fee-for-service basis.
Individuals between the ages of 18 and 65 who resided in Philadelphia or the surrounding region and were enrolled in the Medicaid system were eligible. We selected only individuals who received services at an outpatient psychiatric clinic for a primary diagnosis of MDD (ICD-9 code of 296). In 1993, there were 711,285 claims for psychiatric outpatient services, including 29,348 claims from 1,479 individuals between the ages of 18 and 65 treated specifically for MDD in the community mental health system of Philadelphia and the surrounding region. By 2003, there were 1,047,212 total outpatient claims, including 113,868 claims from 5,912 individuals treated for MDD in the community mental health system. The increase in Medicaid recipients was due to the inclusion of the Medicaid population living in an area that was previously under a waiver.
Seventeen outpatient sites are included in the longitudinal database. We excluded one clinic that comprised five separate sites serving predominantly Hispanic consumers due to unsolvable database coding issues. By excluding these sites, we eliminated the majority of Hispanic consumers receiving services in the community mental health system in the Philadelphia region.
Data Analysis
The service claims records included five categories of outpatient services received, including: case management, medication, group therapy, family therapy, and individual psychotherapy. For analyses of predictors of treatment type, we classified the services received into three groups: psychotherapy alone, medication alone, and combined psychotherapy and medication. Psychotherapy alone was defined as any individual who received individual psychotherapy and did not have any claims for medication sessions in the respective year. Medication alone was defined as any individual who had at least one claim for a medication session and no claims for individual psychotherapy. Combined treatment was defined as an individual who had claims for both medication and psychotherapy in a given year. Utilization of case management services was not examined. The number of sessions was calculated as the number of claims for a given service in each year examined. Therefore, the number of medication sessions for each individual is estimated by the number of medication claims in a given year, and the number of individual psychotherapy sessions is estimated by the number of claims for individual psychotherapy.
For descriptive results, the percent of patients who utilized each type of treatment was calculated for each cohort, as well as the percent of individuals receiving combined psychotherapy plus medication versus a monotherapy. In addition, the average length of medication and psychotherapy treatments received within each cohort was calculated.
Multinomial logistic regressions were used to evaluate changes in treatment types received across the cohorts as well as demographic predictors of treatment type. For these analyses, the dependent variable was treatment type, a three level categorical variable representing psychotherapy alone, medication alone, and combined treatment. The predictor variables included age, gender, race, and cohort. Race was coded as Caucasian versus African American to represent the predominant demographic groups included in this population. Although a small number of consumers of other races received services at the included sites, their services are included only in the descriptive results of types of treatment received and length of treatment. Cohort was a two level variable representing the 1993 cohort versus the 2003 cohort. Age was a two level variable using a median split of consumers age 42 and above versus consumers less than 42 years of age. Separate multinomial regressions were conducted to evaluate the interaction of each of the demographics with cohort in the prediction of the type of treatment received, controlling for the main effects of age, gender, race, and cohort. The first set of multinomial logistic regressions were conducted comparing consumers who received psychotherapy alone and those receiving medication alone to the reference group who received combined psychotherapy and medication. A second set of multinomial logistic regressions were conducted to compare consumers who received medication alone to those who received psychotherapy alone and combined treatment. Wald Chi-squares and odds ratios are presented for each main effect and interaction effect, as well as the percentage of consumers receiving each treatment by demographic group to aid interpretation of results.
Poisson regression was used to predict the number of psychotherapy session utilized by age, gender, race, and cohort since the number of psychotherapy sessions was not normally distributed. Additionally, the interactions of each demographic variable with cohort were examined, controlling for the main effects of age, race, gender, and cohort. As with the multinomial logistic regressions, race represented African American consumers versus Caucasian consumers. Wald Chi-squares were used to test the significance of each main effect and interaction effect. We present estimated marginal means of the number of psychotherapy sessions by each demographic group to aid interpretation of results in addition to the Cohen’s d effect size for all significant effects. Similar poisson regression analyses were conducted predicting the number of medication sessions received.
Results
Sample Demographics and Descriptive Results
The majority of treatment consumers across both cohorts were female with an average age of 40 in the 1993 cohort and 43 in the 2003 cohort (see Table 1). In the 1993 cohort, 50% of consumers were African American and 46.6% were Caucasian. In the 2003 cohort, 62% of consumers were African American and 32% were Caucasian.
Descriptive results for the types of treatment received by consumers of services for MDD in the Philadelphia region are presented in Table 2. The most prevalent treatments for MDD included psychotherapy and medication interventions. Whereas over 80% of consumers received psychotherapy in both the 1993 and the 2003 cohorts, 42% of consumers in 1993 and 61% of consumers in 2003 received medication for MDD. In 1993, 55% of consumers received psychotherapy alone, 6% medication alone, and 39% combined treatment for MDD. In 2003, 36% received psychotherapy alone, 13% medication alone, and 51% combined psychotherapy plus medication for the treatment of MDD. The modal number of sessions for any treatment in the community mental health system was one in both 1993 and 2003. The average number of psychotherapy sessions was 8.5(SD = 10.0) in 1993 and 9.4 (SD = 10.6) in 2003, while the number of medication sessions attended was 4.1(SD = 3.4) in 1993 and 3.4(SD = 2.4) in 2003. The median number of psychotherapy sessions was 5.0 in both 1993 and 2003. The median number of medication sessions was 3.0 in both 1993 and 2003.
Predictors of Treatment Utilization
Predictors of type of treatment received
The results of the multinomial logistic regressions predicting treatment type are presented in Table 3. There were significant changes across the cohorts in the type of treatment received. There was a significant main effect for cohort (χ 2(1) = 240.7, p < .001) as well as a significant interaction between race and cohort (χ 2(1) = 5.1, p = .024) in the prediction of treatment type comparing the utilization of psychotherapy alone to combined treatment. Overall there was a trend toward greater utilization of combined treatment for MDD by 2003 compared to 1993, but this shift was more prevalent among Caucasian consumers. In 1993, 58% of African American consumers received psychotherapy alone while 36% received combined medication and psychotherapy for the treatment of MDD. By 2003, 40% of African American consumers received psychotherapy alone and 48% received combined treatment. For Caucasian consumers, 53% received psychotherapy alone and 41% received combined treatment in 1993, while 29% received psychotherapy alone and 58% received combined treatment by 2003. Multinomial logistic regressions were computed within cohort to interpret the direction of this interaction. The odds ratio for the utilization of psychotherapy alone over combined treatment by race for the 1993 cohort was 1.18. In 1993, African American consumers were 18% more likely to receive psychotherapy than combined treatment compared to Caucasian consumers. The odds ratio for this effect in 2003 was 1.66, indicating that by 2003, African American consumers were 66% more likely to receive psychotherapy than combined treatment compared to Caucasian consumers.
There were also significant main effects for cohort predicting the utilization of medication alone compared to combined treatment (χ 2(1) = 6.5, p = .011) and the utilization of medication alone compared to psychotherapy alone (χ 2(1) = 125.8, p < .001). For the comparison of medication alone to combined treatment, there was an increase in utilization of both medication alone and combined treatment for MDD across the decade. In 1993, 6% of consumers received medication alone and 39% received combined treatment. By 2003, 13% of consumer received medication alone in the treatment of MDD while 51% received combined treatment. The odds ratio of .72 indicates that the 1993 cohort was 28% less likely to receive medication alone over combined treatment than the 2003 cohort. For the comparison of medication alone to psychotherapy alone for the treatment of MDD, there was a decrease in the utilization of psychotherapy alone and an increase in medication alone as treatments received for MDD in the community mental health system across the decade. The odds ratio of .23 indicates that the 1993 cohort was 77% less likely to receive medication alone over psychotherapy alone compared to the 2003 cohort.
Age was also a significant predictor of treatment utilization. Controlling for other predictors, there was a significant main effect for age in the prediction of utilization of psychotherapy alone over combined treatment (χ 2(1) = 117.7, p < .001) as well as in the prediction of utilization of medication alone versus psychotherapy alone (χ 2(1) = 35.2, p < .001). Older consumers were 3% less likely to receive psychotherapy alone rather than combined treatment than younger consumers. For older consumers of services (defined using a median split) for MDD, 33% received psychotherapy alone and 55% received combined treatment. In contrast, younger consumers were more evenly split between treatments with 49% receiving psychotherapy alone and 42% receiving combined treatment. Older consumers were also 3% more likely to receive medication alone over psychotherapy alone for the treatment of MDD compared to younger consumers. For older consumers, 33% received psychotherapy alone while 12% received medication alone. For younger consumers, 49% received psychotherapy alone and only 9% received medication alone for MDD.
Finally, there was a significant effect for gender on the utilization of psychotherapy alone versus combined treatment (χ 2(1) = 6.9, p = .009). Females were 18% less likely to receive psychotherapy alone compared to combined treatment than males. Thirty-four percent of females received psychotherapy alone while 55% received combined treatment. In comparison, 38% of males received psychotherapy alone while 50% percent received combined treatment.
Predictors of treatment length
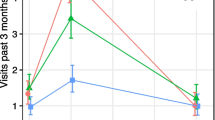
The results of the poisson regression predicting the number of psychotherapy sessions and the number of medication sessions are presented in Table 4. Cohort significantly interacted with age (χ 2(1) = 42.7, p < .001), gender (χ 2(1) = 4.3, p = .038), and race (χ 2(1) = 64.2, p < .001) in predicting the number of psychotherapy sessions received. The Cohen’s d effect size for the prediction of number of psychotherapy sessions from the age by cohort interaction was .23. Using a median split of age to examine the effect, older consumers increased from an average of 8.9 sessions (estimated marginal means controlling for all demographic main effects) in 1993 to an average of 12.8 sessions in 2003. Younger consumers showed a smaller increase in the average number of psychotherapy sessions attended, increasing from 7.7 sessions in 1993 to 10.2 sessions in 2003. The effect size for the prediction of number of psychotherapy sessions from the gender by cohort interaction was very small (d = .04). Females increased from an average of 8.7 to 11.9 across the decade, while males made a somewhat larger gain from an average of 7.9 sessions to 11.3. Race had the largest effect on changes in the number of psychotherapy sessions across the decade (Cohen’s d = .46). African American consumers showed only a small increase in the average number of psychotherapy sessions received from an average of 7.1 sessions to 8.8 sessions. Caucasian consumers received more sessions in 1993, an estimated marginal mean of 10.1 sessions, and made a larger increase across the decade to an average of 15.1 sessions.
There was a very small effect for gender in the prediction of the number of medication sessions attended (χ 2(1) = 3.9, p = .048, d = .04). Females attended an average of 3.9 sessions, while males attended an average of 3.8 sessions. There was also a significant interaction between cohort and age in the prediction of the number of medication sessions attended (χ 2(1) = 5.5, p = .019, d = .01). Using a median split of age, older consumers decreased from an average of 4.3 medication sessions to 3.7 sessions across the decade, while younger consumers remained more stable in the number of medication sessions attended, ranging from an average of 3.7 in 1993 to an average of 3.6 in 2003.
Discussion
We evaluated psychotherapy utilization among African American and Caucasian consumers of outpatient services for the treatment of MDD in the community mental health system. Contrary to our hypotheses, there does not appear to be a decrease in the utilization of psychotherapy as a treatment for MDD across the decade from 1993 to 2003, as over 80% of consumers received psychotherapy as a treatment for MDD as either a monotherapy or in combination with medication. Examination of the incidence of monotherapy versus combined treatment for MDD clarifies how policy, financial, and medication development issues may have influenced the utilization of psychotherapy as a treatment for MDD in the community mental health system. Consistent with the national results presented by Olfson et al. (2002b), there was a decrease in the utilization of psychotherapy alone to treat MDD across the decade. However, there was also a large increase in the percentage of consumers who received combined psychotherapy plus medication for the treatment of MDD. In terms of treatment length, unfortunately, the modal number of sessions attended for either psychotherapy or medication treatment was only one session. The median number of psychotherapy sessions remained stable at 5 sessions across the decade and the median number of medication sessions remained stable at 3 sessions.
These results indicate that despite advances in pharmacotherapy for depression and the development of guidelines recommending medication as the primary treatment for moderate to severe depression, psychotherapy remains a predominant treatment for MDD in the community mental health system. The current data indicate which treatments were actually received by consumers but do not explain why combined treatment has become the most prominent in community treatment. It could be that consumers are interested and seeking both medication and psychotherapy for the treatment of MDD. Although community clinics may benefit from the ease of disseminating medications as treatment for MDD, consumers might also want psychotherapy. Alternatively, it could be that providers working in these settings prefer the combined treatment approach, despite factors that encourage the use of medication alone for the treatment of MDD, given the chronic nature of the depression treated in the community setting. Future studies should seek to explore whether the move towards combined treatment for MDD in the community mental health setting has been driven by consumers, providers, or both.
Although the trend towards greater utilization of combined treatments for MDD in this community mental health sample is consistent with the national survey evaluated by Olfson et al. (2002b), evaluation of the demographic predictors of treatment utilization clarify the shifts in treatment utilization in this community sample. Racial disparities are evident in both the types of treatment received and the length of treatment across the decade examined. Although there was an overall shift toward the utilization of combined treatment for MDD in the community mental health system, Caucasian consumers made a greater shift toward combined treatment than African American consumers. Although there was a small trend in 1993 for African American consumers to receive psychotherapy over combined treatment, by 2003 African American consumers were much more likely to receive psychotherapy over combined treatment than Caucasian consumers. For consumers who received a monotherapy in both cohorts, a greater percentage of consumers received psychotherapy alone than medication alone as a treatment for MDD. However, across the decade the percentage of consumers receiving medication alone increased while the percentage of consumers receiving psychotherapy alone decreased.
This racial disparity appears to influence the length of treatments for MDD in the community mental health system as well. Although the median number of psychotherapy sessions remained stable across the decade examined, Caucasian consumers of services in 2003 received significantly more psychotherapy sessions than Caucasian consumers 10 years earlier, receiving an average of 15 sessions compared to 10 in 1993. In contrast, African American consumers received significantly fewer psychotherapy sessions on average in 1993 and made a much smaller increase in the number of psychotherapy sessions attended across the decade to an average of only 9 sessions.
This claims database cannot determine whether African American consumers are less likely to choose combined treatments for MDD or are prescribed combined medication and psychotherapy treatment less often. However, the results of the current study indicate that the organizational, policy, and research developments that have influenced an overall shift towards combined treatment for MDD among Caucasian consumers have not had the same effect on African American consumers. In addition, African American consumers continued to receive fewer treatment sessions than Caucasian consumers across the decade, indicating that African Americans are not receiving the same dose of treatment for MDD in the community system.
These results demonstrate that racial disparities exist in the type and length of treatments received for the treatment of depression. Other investigations have shown that socioeconomic factors such as lack of insurance coverage and access to services predict service utilization by African Americans. Our results indicate that even when insurance and availability of services is not an issue, a disparity still remains in the type and length of treatments received.
The findings of this study go against the long-established and well documented findings that African Americans are not initially seeking treatment services for mental health issues. Although we could not examine differential trends in seeking treatment across racial groups, we found that many African Americans in Philadelphia are initiating treatment with the behavioral health care system; however, they are not continuing treatment for as long as their Caucasian counterparts. The continuous evaluation of engagement and retention of African Americans in mental health care is necessary in order to ensure that African American consumers receive quality treatment.
These findings indicate that African Americans are more likely to receive a monotherapy (psychotherapy or medication) in the treatment of MDD, while Caucasian consumers are more likely to receive combined treatment. The literature on disparities indicates that African Americans tend not to be in the forefront of receiving new, prominent treatments (Aisenberg 2008; Brown et al. 1999), yet there is emerging literature that suggests newer evidence based treatments are effective treatments for depression in African Americans (Aisenberg 2008; Miranda et al. 2005; Schraufnagel et al. 2006). Although our analyses do not assess the use of evidence based treatments per se, our finding that African Americans are less likely to receive combined treatment and typically attend fewer sessions raises the question of whether African Americans are receiving the highest quality treatments available for depression in the community mental health system. However, these results indicate disparities in treatments received but do not directly assess outcomes of treatment. It is possible that African Americans are more cautious in committing to the combined medication and psychotherapy treatment, but are able to attain quality care by choosing the monotherapy that is right for them. Alternatively, it is possible that certain characteristics of the community mental health system discourage African American consumers from receiving the quality and quantity of treatment needed for optimal results. Future research efforts should focus on understanding the effects of treatment preference for monotherapy versus combined treatment on outcome and should evaluate the factors that contribute to attrition from services. Such studies have the potential to enhance the quality and quantity of treatments for depression across demographic groups in the community mental health system.
Contrary to our hypotheses, older consumers were not more likely to receive psychotherapy in lieu of medication for the treatment of MDD. In fact, older consumers were less likely to receive psychotherapy alone relative to medication alone and combined treatment than younger consumers. This finding can be understood in light of the overall trend toward combined treatment as the preferred treatment for MDD. More than half of older consumers received combined psychotherapy and medication as a treatment for MDD. However, younger consumers were split between the utilization of psychotherapy alone and combined treatment. For older consumers who received psychotherapy, there was a larger increase in the average number of psychotherapy sessions across the cohorts compared to younger consumers. However, older consumers received fewer medication sessions on average in 2003 compared to the earlier 1993 cohort. Older consumers were more likely to make the shift toward use of combined treatment for MDD overall, but were also more likely to receive more psychotherapy sessions and fewer medication sessions in the treatment of MDD.
Finally, gender effects further illuminate the treatment utilization shift toward combined treatment for MDD in the community mental health system. Female consumers were more likely to receive combined treatment over psychotherapy alone than male consumers. Females also had a larger increase in the average number of psychotherapy sessions received across the decade than male consumers. This may indicate that the community mental health system has improved resources for assisting females with childcare and social burdens that have been reported as barriers to service in the past.
Several limitations of this study are important to mention. Claims databases such as the one used for this project reflect only treatment sessions for which payment was sought, and do not necessarily acknowledge the recommendations of health care providers. Additionally, it is possible that there are treatment sessions received by consumers that were not adequately billed, thus resulting in an underestimate of the total number of treatments actually received. From a technical standpoint, claims databases may also have inherent system errors that distort the estimates of treatment utilization. There may also be cohort effects. This analysis evaluated treatment utilization changes using two separate cohorts representing service use in 1993 and 2003. It is possible that other factors related to these years influences the service use estimates and therefore the estimates of change in utilization. Finally, these analyses were conducted on claims databases for the Philadelphia region. Although the results should generalize to community mental health samples in other large, urban areas, it is possible that regional differences across the United States account for differences in psychotherapy utilization.
Overall, our results indicate that there have been important changes in the utilization of treatments for MDD in the community mental health system over time. Across the decade examined here, there was a shift toward combined treatment as the treatment of choice for MDD and an increase in the average number of psychotherapy sessions attended. Our results indicate that evaluations of changes in treatment utilization need to be understood in the context of demographic differences among consumers of services. Important racial disparities have been identified in the types and lengths of treatment received as well as in changes in treatment utilization over time. Although many factors have influenced a shift towards combined treatment for MDD, African American consumers of mental health services are still less likely to receive combined psychotherapy and medication treatment for MDD than Caucasian consumers and also receive significantly fewer treatment sessions.
References
Aisenberg, E. (2008). Evidence-based practice in mental health care to ethnic minority communities: Has its practice fallen short of its evidence? Social Work, 53(4), 297–306.
Alvidrez, J., & Azocar, F. (1999). Distressed women’s clinic patients: Preferences for mental health treatments and perceived obstacles. General Hospital Psychiatry, 21(5), 340–347.
American Psychiatric Association. (1993). Practice guideline for major depressive disorder in adults. American Journal of Psychiatry, 150(4), 1–26.
American Psychiatric Association. (2000). Practice guideline for the treatment of patients with Major Depressive Disorder: Second edition. American Journal of Psychiatry, 157(4), 1–45.
Brown, C., Schulberg, H., Sacco, D., Perel, J., & Houck, P. (1999). Effectiveness of treatments for major depression in primary medical care practice: A post hoc analysis of outcomes for African American and white patients. Journal of Affective Disorders, 53(2), 185–192.
Diala, C. C., Muntaner, C., Walrath, C., Nickerson, K. J., LaVeist, T. A., & Leaf, P. J. (2000). Racial differences in attitudes toward professional mental health care and in the use of services. The American Journal of Orthopsychiatry, 70(4), 455–464.
Diala, C. C., Muntaner, C., Walrath, C., Nickerson, K. J., LaVeist, T. A., & Leaf, P. J. (2001). Racial/ethnic differences in attitudes toward seeking professional mental health services. American Journal of Public Health, 91(5), 805–807.
Lundervold, D., & Lewin, L. M. (1990). Older adults’ acceptability of pharmacotherapy and behavior therapy for depression: Initial results. Journal of Applied Gerontology, 9, 211–215.
Miranda, J., Bernal, G., Lau, A., Kohn, L., Hwang, W. C., & LaFromboise, T. (2005). State of the science on psychosocial interventions for ethnic minorities. Annual Review of Clinical Psychology, 1, 113–142.
Mulrow, C. D., Williams, J. W., Jr., Trivedi, M., et al. (1999). Treatment of depression: Newer pharmacotherapies [AHCPR publication No. 99-E014]. Rockville, MD: US Department of Health and Human Services.
Olfson, M., Marcus, S. C., Druss, B., Elinson, L., Tanielian, T., & Pincus, H. A. (2002a). National trends in the outpatient treatment of depression. JAMA, 287, 203–209.
Olfson, M., Marcus, S. C., Druss, B., & Pincus, H. A. (2002b). National trends in the use of outpatient psychotherapy. American Journal of Psychiatry, 159, 1914–1920.
Padgett, D. K., Patrick, C., Burns, B. J., & Schlesinger, H. J. (1994a). Ethnicity and the use of outpatient mental health services in a national insured population. American Journal of Public Health, 84, 222–226.
Padgett, D. K., Patrick, C., Burns, B. J., & Schlesinger, H. J. (1994b). Women and outpatient mental health services: Use by Black, Hispanic, and White women in a national insured population. Journal of Mental Health Administration, 21, 347–360.
Schraufnagel, T. J., Wagner, A. W., Miranda, J., & Roy-Byrne, P. P. (2006). Treating minority patients with depression and anxiety: What does the evidence tell us? General Hospital Psychiatry, 28, 27–36.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Connolly Gibbons, M.B., Rothbard, A., Farris, K.D. et al. Changes in Psychotherapy Utilization Among Consumers of Services for Major Depressive Disorder in the Community Mental Health System. Adm Policy Ment Health 38, 495–503 (2011). https://doi.org/10.1007/s10488-011-0336-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10488-011-0336-1