
Abstract
This study investigated the psychohysiological patterns associated with cell phone text messaging (texting). Twelve college students who were very familiar with texting were monitored with surface electromyography (SEMG) from the shoulder (upper trapezius) and thumb (abductor pollicis brevis/opponens pollicis); blood volume pulse (BVP) from the middle finger, temperature from the index finger, and skin conductance (SC) from the palm of the non-texting hand; and respiration from the thorax and abdomen. The counter-balanced procedure consisted of a 2 min pre-baseline, 1 min receiving text messages, 2 min middle baseline, 1 min sending text messages and 2 min post-baseline. The results indicated that all subjects showed significant increases in respiration rate, heart rate, SC, and shoulder and thumb SEMG as compared to baseline measures. Eighty-three percentage of the participants reported hand and neck pain during texting, and held their breath and experienced arousal when receiving text messages. Subjectively, most subjects were unaware of their physiological changes. The study suggests that frequent triggering of these physiological patterns (freezing for stability and shallow breathing) may increase muscle discomfort symptoms. Thus, participants should be trained to inhibit these responses to prevent illness and discomfort.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
More and more people use small digital devices such as cell phones, personal digital assistants (PDAs) and iPod™. The use of these devices has lead to a public concern over the possible harmful physiological effects. Although long term effects of cell phone use has not been studied, ongoing cell phones use may cause headaches, impaired concentration and memory, discomfort, muscle fatigue in deltoid and thenar muscles, and sleep interruption or disturbance in adolescents and adults (Balikci et al. 2005; Chany et al. 2007; Santini et al. 2001; Szyjkowska et al. 2005; van den Bulck 2003). Cell phone text messaging may also increase psychological discomfort. Smith and Williams (2004) reported that subjects reported lowering levels of belonging, control, self-esteem, and meaningful existence as well as worsening of moods when text-messaging was used as the vehicle for communication during an experiment. Although none of these studies measured physiological changes that occurred during cell phone text messaging, we previously had observed that people tended to stabilize their body (become rigid) and held their breath or shallow breathed when they entered data and/or read the LCD screen (Peper et al. 2003; Peper and Harvey 2008).
These physiological patterns appear similar to those observed during computing and mousing and are correlated with musculoskeletal discomfort/disorders reported by working-age adults, college students and children using computer (Burke and Peper 2002; Hupert et al. 2004; Jacobs and Baker 2002; Jenkins et al. 2007). Fifty-four percentage of college students experienced computer-use-related musculoskeletal symptoms and 62% of these students who were surveyed also experienced functional limitations (Jenkins et al. 2007). The purpose of this study is to explore the relationship between cell phone text messaging, psychophysiological patterns, subjective experiences and discomfort.
Methods
Participants
Twelve college students (11 right-hand dominant, 11 female and 1 male, average age 21.8 years (SD = 1.7), range 19–24 years old) were very familiar with text messaging. 41.7% participants text messaged for more than 4 years, 41.7% of the participants text messaged in classrooms during class lectures, 83.3% text messaged in their own rooms, 58.3% played computer games, and all extensively used computers.
Equipment
The BioGraph Infiniti™ version 3.1.5 (Thought Technology Ltd., Montreal, Quebec, Canada) was used to collect psychophysiological data with a sampling rate of 256 samples per second from the participants. Sensors placement and equipment settings were as follows:
-
Respiration was monitored with strain gauges placed around the chest underneath the axilla and above the breasts for thoracic recording and around the abdomen and above the umbilicus for abdominal recording.
-
Blood volume pulse (BVP) was monitored from the palmar side of the distal phalange of participants’ middle finger of non-texting hand.
-
Finger temperature (TEMP) was monitored from the medial side of the distal phalanx of index finger of non-texting hand.
-
Skin conduction (SC) was monitored with two electrodes placed on the palm (thenar and hypothenar eminences) from non-texting hand.
-
Surface Electromyography (SEMG) was monitored with Myoscan Pro sensors using Triode™ electrode with the bandpass filter set between 100 and 200 Hz. The SEMGs were recorded from the centre of the right upper trapezius and thumb (abductor pollicis brevis/opponens pollicis).
Questionnaire
The questionnaire assessed demographic data, experience with text messages (i.e., How many years have you text messaged? What type of messages do you text?), muscle symptoms and intensity (i.e., Where do you experience muscle symptoms while text messaging? Rate your intensity of the symptom from 1 to 10). The subjective experiences associated with pre-baseline, sending text message, receiving text message and post-baseline conditions were assessed (i.e., Rate your level of stress, relaxation and concentration on a graded intensity scale from 1 to 10).
Procedure
The participants sat in a quiet room and filled out the demographic questionnaire. After the sensors were attached and the cell phone was placed in front of them the following sequential conditions were monitored: 2 min pre-baseline, 1 min receiving text messages, 2 min middle baseline, 1 min sending text messages and 2 min post-baseline (the sending and receiving text messaging conditions were counterbalanced). After the recording, they then filled out the subjective questionnaire.
Data Analysis
The physiological data was scored for artifacts and one author (Lin) eliminated segments containing artifacts using standardised guidelines. Heart rate derived from the BVP signal and respiration rate were visually scored only during artifact free periods. The physiological, demographic and subjective rating data were statistically analysed using SPSS 13.0.
Results
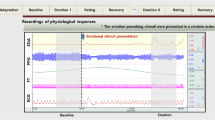
When typing text messages, 83% of the participants reported experiencing some hand and neck pain. When receiving text messages, they reported feeling increased arousal and vigilance and their heart rate, SC, and SEMG increased. At the onset of receiving the text message, they held their breath and then continued to breathe shallowly and rapidly. When sending text messages, breathing became shallow and rapid, heart rate, SC, and SEMG increased. In the post-baseline conditions following texting, the physiological signals returned to same physiological values as during the pre-baseline condition as shown by a representative subject’s recording in Fig. 1.

Representative physiological recording during receiving and sending text messages
There were significant differences in respiration rate (t = −3.61, P < .01; t = 3.86, P < .01, respectively) between pre-baseline (13.7 ± 3.2) and sending (18.1 ± 4.4), effect size for Cohen’s d is 0.36; sending (18.1 ± 4.4) and post-baseline (13.6 ± 2.5), effect size for Cohen’s d is 0.37. The pattern of respiration rate was shown in Fig. 2.

Respiratory rate during pre-baseline, receiving, sending and post-baseline
There were significant differences in SEMG trapezius (t = −3.84, P < .01; t = −5.30, P < .001, respectively) between pre-baseline (2.8 ± 0.9) and sending (7.9 ± 4.3), effect size for Cohen’s d is 0.58; pre-baseline (2.8 ± 0.9) and receiving (10.8 ± 5.0), effect size for Cohen’s d is 0.90; and there were significant differences in SEMG hand (t = −10.60, P < .001; t = −8.57, P < .001, respectively) between pre-baseline (0.8 ± 0.7) and sending (32.7 ± 10.4), effect size for Cohen’s d is 2.19; pre-baseline (0.8 ± 0.7) and receiving (19.3 ± 7.9), effect size for Cohen’s d is 1.27. The patterns of SEMG_trapezius and SEMG_hand were shown in Fig. 3.

SEMG_trapezius and SEMG_thumb activity during receiving and sending text messages
There was significant differences in SC (t = −2.34, P < .05) between pre-baseline (4.2 ± 4.5) and sending (9.3 ± 11.0), effect size for Cohen’s d is 0.18. The pattern of SC was shown in Fig. 4.

Skin conductance during pre-baseline, receiving, sending and post-baseline
There were significant differences in heart rate (t = − 2.23, P < .05; t = 2.91, P < .05, respectively) between pre-baseline (78.6 ± 9.4) and sending (82.1 ± 7.9), effect size for Cohen’s d is 0.12; sending (82.1 ± 7.9) and post-baseline (77.4 ± 9.3), effect size for Cohen’s d is 0.16. The pattern of heart rate was shown in Fig. 5.

Heart rate during pre-baseline, receiving, sending and post-baseline
There was a correlation between the intensity of symptoms and respiration rate when receiving text messages (r = −.65, P < .05). All other correlations suggest a non-significant trends between symptoms and physiological measures. Temperature recordings were not analysed because of the high room temperature during the summer season in Taiwan. Participants who reported increasing intensity of symptoms had higher pre- and post- SEMG activity as well as higher SC levels during sending and receiving. Finally, there were correlations between age and time in playing computer games (r = −.62, P < .05) and intensity of symptoms and time in playing computer games (r = .65, P < .05).
There were significant differences in the subjective stress experience (t = −2.61, P < .05 and t = 3.08, P < .01; t = 2.55, P < .05, respectively) between sending text messages (4.2 ± 2.4) and pre-baseline (2.8 ± 1.4), sending text messages (4.2 ± 2.4) and post-baseline (2.8 ± 1.5), and receiving text messages (4.3 ± 2.9) and post-baseline (2.8 ± 1.5). There were significant differences in the relaxation feeling (t = 2.26, P < .05; t = −3.34, P < .01; t = −2.73, P < .05, respectively) between pre-baseline (6.8 ± 2.1) and receiving (5.6 ± 3.2), sending text messages (5.6 ± 2.8) and post-baseline (7.3 ± 2.2), and receiving text messages (5.6 ± 3.2) and post-baseline (7.3 ± 2.2). There was significant difference in concentration (t = −2.84, P < .05) between pre-baseline (6.3 ± 1.6) and sending text messages (8.1 ± 1.5).
Discussion
When texting all participants showed significant increases in heart rate, SC, and shoulder and hand SEMG as compared to pre-baseline measures. Respiration rate increased significantly when sending text messages while the average respiration rate did not change when receiving text messages because the average respiration rate included breath holding and rapid shallow breathing. For many participants, receiving text messages evoked arousal as indicated by breath holding or shallow breathing and increased muscle tension and skin conductance. These physiological changes were consistent with their subjective reports of feeling increased stress, when they received a text message.
While sending text messages, the participants would unknowingly stabilize their trunk so that they could perform fine motor movements. The task of focusing on a small digital screen and composing a text message demanded significant covert effort and concentration. They were unaware of their muscle tension and respiratory changes and higher baseline SEMG level were correlated with higher intensity of self-reported discomfort. Also, participants who experience symptoms during texting also played the most computer games. The cell phone and other small digital devices such as PDAs, iPhone™, iPod™, Game Boy, portable DVD players, or computers all demand concentration and vigilance. To perform fine motor movements necessary to manipulate the controls of the devices, participants automatically and unconsciously stabilize their trunks, tighten their necks and shoulders and breathe shallowly as well as thrust their heads forward in order to read the small screen. This immobilized position combined with increased sympathetic arousal, neck and shoulder tension and shallow breathing, if triggered frequently, could contribute to developing musculoskeletal disorders, pain or repetitive strain injury (Peper et al. 2003). This response may have long term health consequences especially as more children operate digital devices instead of spending time playing and performing large body movements. The preliminary findings are based upon 12 participants and long term epidemiological and physiological studies need to done to investigate the relationships between physiology discomfort/symptoms, gender and the use of small handheld digital devices with LCD screens. Finally, we suggest that young people need to be trained to be become aware of covert neck and shoulder tension and shallow breathing while receiving and sending text messages and learn to relax their neck and shoulders and breathe slower to prevent future illness.
References
Balikci, K., Ozcan, I. C., Balik, D. T., & Balik, H. H. (2005). A survey study on some neurological symptoms and sensations experienced by long term users of mobile phones. Pathologie Biologie, 53, 30–34. doi:10.1016/j.patbio.2003.12.002.
Burke, A., & Peper, E. (2002). Cumulative trauma disorder risk for children using computer products: Results of a pilot investigation with a student convenience sample. Public Health Reports, 117, 350–357.
Chany, A. M., Marras, W. S., & Burr, D. L. (2007). The effect of phone design on upper extremity discomfort and muscle fiatgue. Human Factors, 49(4), 602–618. doi:10.1518/001872007X215683.
Hupert, N., Amick, B. C., Fossel, A. H., Coley, C. M., Robertson, M. M., & Katz, J. N. (2004). Upper extremity musculoskeletal symptoms and functional impairment associated with computer use among college students. Work: Journal of Prevention Assessment & Rehabilitation, 23(2), 85–93.
Jacobs, K., & Baker, N. A. (2002). The association between children’s computer use and musculoskeletal discomfort. Work: Journal of Prevention Assessment & Rehabilitation, 18(3), 221–226.
Jenkins, M., Menéndez, C. C., Amick, B. C., Tullar, J., Hupert, N., Robertson, M. M., et al. (2007). Undergraduate college students’ upper extremity symptoms and functional limitations related to computer use: A replication study. Work: Journal of Prevention Assessment & Rehabilitation, 28(3), 231–238.
Peper, E., & Harvey, R. (2008). From technostress to technohealth. Japanese Journal of Biofeedback Research, 35(2), 27–34.
Peper, E., Wilson, V. S., Gibney, K. H., Huber, K., Harvey, R., & Shumay, (2003). The integration of electromyography (sEMG) at the workstation: Assessment, treatment and prevention of repetitive strain injury (RSI). Applied Psychophysiology and Biofeedback, 28(2), 167–182. doi:10.1023/A:1023818810766.
Santini, R., Seigne, M., Bonhomme-Faivre, L., Bouffet, S., Defrasne, E., & Sage, M. (2001). Symptoms experienced by users of digital cellular phones. Pathologie Biologie, 49(3), 222–226. doi:10.1016/S0369-8114(01)00132-8.
Smith, A., & Williams, K. D. (2004). R U there? Ostracism by cell phone text messages. Group Dynamics: Theory, Research, and Practice, 8(4), 291–301. doi:10.1037/1089-2699.8.4.291.
Szyjkowska, A., Bortkiewicz, A., Szymczak, W., & Makowiec-Dabrowska, T. (2005). Subjective symptoms related to mobile phone use–a pilot study. Polski Merkuriusz Lekarski, 19(112), 529–532.
van den Bulck, J. (2003). Text messaging as a cause of sleep interruption in adolescents, evidence from a cross-sectional study. Journal of Sleep Research, 12(3), 263. doi:10.1046/j.1365-2869.2003.00362.x.
Acknowledgments
We thank Ms. Marisa Cortex for her significant help in doing the research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lin, IM., Peper, E. Psychophysiological Patterns During Cell Phone Text Messaging: A Preliminary Study. Appl Psychophysiol Biofeedback 34, 53–57 (2009). https://doi.org/10.1007/s10484-009-9078-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-009-9078-1