
Abstract
Neighborhood social ecologies may have protective effects on depression in Latinos, after adjusting for demographic risk factors, such as nativity and length of stay in the US. This study examines the effects of neighborhood collective efficacy and linguistic isolation on depression in a heterogeneous urban Latino population from 1,468 adult respondents in Los Angeles County. We used multilevel models to analyze how major depression is associated with socioeconomic background, length of stay in the U.S., neighborhood collective efficacy and linguistic isolation among Latinos. A significant cross-level interaction effect was found between collective efficacy and foreign-born Latinos who resided in the US ≥ 15 years. We report cross-level interaction effects between linguistic isolation and nativity for U.S.-born and nativity and duration of residence for foreign-born Latinos who had lived in the U.S. at least 15 years. The moderating effects reported in this study suggest that the benefits of neighborhood collective efficacy and linguistic isolation vary by Latino subgroup and are conceptually discrete forms of social capital and offer insights for community based interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Social and behavioral sciences have increasingly turned to the study of neighborhood characteristics to determine their effects on human organization and health. A central challenge is distinguishing how social and cultural factors interact with neighborhood characteristics to affect health and illness. This article examines the association between neighborhood characteristics and depression among Latinos.
Collective Efficacy and Linguistic Isolation as Explanatory Factors in Neighborhood Studies
Two constructs are used in this study to explore three related research questions about how neighborhood characteristics affect depression. The construct of collective efficacy encompasses neighborhood social control and social cohesion (Sampson et al. 1997), and has been found to contribute to social and personal outcomes (Browning and Cagney 2002; Cohen et al. 2006). The collective efficacy measure was developed in the Chicago Human Potential Project by Sampson (Sampson 2003). Collective efficacy has been defined as the ability of neighborhoods to “realize the common values of residents” (Sampson et al. 1997). The construct derives from community participation and responsibility rooted in the commonweal, “the general welfare of the community.” Collective trust increases social control for sustaining normative values and behaviors in neighborhoods (Sastry et al. 2006). Although this is a proxy indicator for a collective social process, it is measured by obtaining self-reported information from individual respondents residing in target neighborhoods. The “Methods” section describes the well-validated scale used for this assessment.
Although the collective efficacy construct was originally applied to the control and reduction of juvenile crime, we believe the construct has implications for community depression. First, social cohesion is a marker of positive neighborhood interaction and has direct implications for individual level depression. Second, although informal social control may have primary effects on controlling deviant behaviors among both residents and non-residents, participating in these acts of informal social control fosters voluntary participation in community institutions and activities creating solidarity and social integration of new residents into the community.
Linguistic isolation as a measured variable originated in the 2000 U.S. Census. Although this is largely a demographic measure of individual households, which is then aggregated to the level of a neighborhood, it is an important proxy marker for cultural conditions within a neighborhood. Linguistic isolation is a marker for the presence of an ethnic enclave and ethnic sub-group homogeneity; in this instance, Spanish-speaking social networks. The concentration of Spanish speakers into interactive networks illustrates “chain migration” patterns of Latino immigrants who resettle in areas where relatives, friends and acquaintances reside (Portes and Zhou 1993). Participation of newcomers in linguistically and culturally compatible social networks composed of co-ethnic groups facilitates resettlement (Finch et al. 2007).
For our study, we asked three research questions:
-
1.
Are collective efficacy and linguistic isolation empirically discrete constructs?
-
2.
Does neighborhood collective efficacy offer protective effects in lowering depression after adjusting for demographic risk factors due to nativity and length of stay in the US?
-
3.
Does linguistic isolation offer protective effects in lowering depression after adjusting for demographic risk factors due to nativity and length of stay in the US?
-
4.
Is there a moderating effect between linguistic isolation and collective efficacy where the effect of these two protective factors may be conditional on one another?
Theoretical Foundation of the Study
The theoretical foundation for this study is based on a functional definition of culture: a living repository of mutual history, social facts and social expectations transmitted through interaction that affords solutions for tangible and intangible problems in living (Guerra and Knox 2008). Culture has systematic effects on world view and self-identity of individuals, and functions as an open system with continuous information and reshaping (Schensul 2009; Szapocznik and Coatsworth 1999). Culture operates through a social ecological framework. The elements of theory used to interpret this framework are derived from social and community psychology, social organization, social networks and social control, as well as social epidemiology (Kelly and Chang 2008).
Socioeconomic differences in U.S. society produce patterned differences in neighborhood environments including micro features such as families, peer groups, and distinctive ethnic social networks. Meta and macro features of a neighborhood range from local churches and commercial vendors to larger scale organizations and institutions, and ultimately extend to more remote media and government entities (Hawkins et al. 1992). Social ecological theory presumes that there are intimate domains where intense interaction and socialization occur, such as in co-ethnic social networks of family and friends. Outside of these arenas, adults and children have variable levels of shared exposure to the social contexts or ecologies. These multiple levels of social interaction are distinguishable yet functionally linked in complex patterns (Schensul 2009). More relevant to this study, socialization and social control also originate in multiple domains of the social ecology; these influences may be complementary, competitive, antagonistic, or unrelated.
Socialization is a lifespan process. Individual level change results from unique personal traits, maturation, selective personal experiences, and social affiliation patterns obtained through interactions with elements that make up the social ecology. As noted by Bronfenbrenner (1995), risk and protective factors affecting individual development, such as behavioral problems and depression, emerge directly from the processes of interaction across the different domains, or levels, of the social ecology. This includes the possibility of continuities and discontinuities across domains that result in fragmented socialization (Bronfenbrenner 1995). Multiple factors including concentrated poverty, racism, limited opportunity structure, ethnic composition, deterioration of the built environment, spatial dimensions of geographic areas, and settlement history, all influence the frequency and character of risk and protective factors. Thus, variations in characteristics of social ecologies, especially their core social assets, can be conceived to be either protective or risk enhancing for individuals and ethnic groups. In short, human groups adapt to the social ecology through selective interaction in social networks, and the ramifications of this process may be adaptive or maladaptive for human development, self-valuation, and social adjustment (Szapocznik and Coatsworth 1999).
Latinos and Depression
Using a multilevel approach, the primary goal of this study was to examine the interplay of collective efficacy and linguistic isolation as explanatory factors for reducing risk for depression among Latinos. Collective efficacy has been widely used in previous multilevel health and socio-behavioral studies (e.g., Sampson et al. 1997; Morenoff 2003) but insufficiently in studies of mental health. Linguistic isolation has been studied in Latino neighborhoods and shown to have selective protective effects against risk factors such as nativity and duration of stay for substance abuse and obesity (Park et al. 2008; Gordon-Larsen et al. 2003; Pearlman et al. 2003; Finch et al. 2000). To our knowledge neither of these factors (nativity and duration of stay) has been examined in controlled models to determine discrete or combined effects on depression in neighborhoods with significant Latino populations.
The epidemiologic research literature has shown that, despite a range of estimates regarding the prevalence of depression in Latino populations, rates of depression are lower among immigrant Latinos than among U.S.-born Latinos (Alegria et al. 2007; Vega et al. 1998b; Grant et al. 2004; Burnam et al. 1987). The lower risk for depression among immigrants has been attributed to pre-adolescent socialization in countries of origin, countries where lower depression rates have been documented. This propensity for higher risk of depression is especially notable in English-dominant speakers suggesting a positive association with social acculturation (Vega and Sribney 2008).
Of particular interest in this study is the observation that language preference is a marker for risk of behavioral health problems, such as depression, because language preference is highly correlated with proximal factors of differential socialization such as nativity, duration of residence in the U.S. for immigrants, and social network interaction patterns (Canino et al. 2008; Alegria et al. 2007; Vega et al. 1998a). Gottlieb (1978) showed that social networks have multiple functions including expressive support, resource reciprocity, and information assistance. Antonucci and Akiyama (1987) used the metaphorical “convoy model” to describe the process by which immigrants carry their cultural beliefs and practices forward to the U.S. and reinforce their culture through social network relations.
Social Control, Social Adaptation, and Depression
Social disorganization affects normative systems through disruptions in both intimate networks and social institutions that are responsible for defining behavioral expectations through processes of informal social control (Kubrin and Weitzer 2003). To the extent that informal social control is weakened, normative socialization is undermined. Behavior expectations become less predictable or even inconsistent across domains of the social ecology. Deviation from behavioral norms in both public and private behaviors increases, and established social role arrangements (e.g., marriage, family structure, and parenting roles) are destabilized. In short, the social origins of depression at a personal level are attributable to disjunctures in social expectations and social roles that are expected to supply both social capital and emotional bonds. Low social control and reduced social support may play important concomitant causal roles in depression. Together, they can cause declines in interpersonal bonds in social networks especially if reinforced by wider neighborhood disintegration (Lin 1986; Vega et al. 1991). This process is analogous to findings in research on emotional support, if absent it is a risk factor for depression and when present is protective and potentially buffering (interaction effect).
Methods
Data from the Los Angeles Family and Neighborhood Study (LAFANS) Wave 1—a longitudinal study of families in a stratified probability sample of census tracts in Los Angeles County were used in the analyses. The data were gathered in Los Angeles County where 45% of the population is Latino (nearly 4.7 million individuals of mixed Latino national origins in 2009), including Latino immigrant enclaves that have been rapidly expanding in recent decades.
The LAFANS surveys were conducted from April 2000 to January 2002 to examine questions about how neighborhoods, social conditions and family life affect a broad set of outcomes for adults and children. For the LAFANS sample, 1,652 census tracts in Los Angeles County were stratified into very poor, poor, and non-poor strata based on the proportion of residents with annual income below the poverty level. The very poor census tracts are in the top 10% of the poverty distribution, the poor census tracts are in the 60th–89th percentiles, and non-poor census tracts are in the bottom 60% of the distribution (Sastry et al. 2006). From a representative sample of 65 tracts (20 very poor, 20 poor, and 25 non-poor), 40–50 dwelling units were sampled at random, with an oversample of households with children. Within each household, LAFANS randomly sampled one adult (aged ≥ 18 years) who was interviewed in-person. This sample had a 70% response rate, which is considered to be without non-response bias based on analyses from a previous study (Pebley and Sastry 2004). Our analyses used data from the randomly sampled self-identified Latino adults in the LAFANS Wave 1 cohort, n = 1,468.
Since participants had a choice of being interviewed in either English or Spanish, extensive efforts were made to assure cross-ethnic/cross-language equivalence. English and Spanish versions of the questionnaires were developed in parallel by bilingual survey researchers and specialists. Furthermore, all survey questions were pre-tested in English and Spanish and revised accordingly, if necessary (Pebley and Sastry 2004).
Individual-Level Variables
The primary outcome was a report of physician’s diagnosis of major depression. The main individual level predictors used were the survey respondent’s age, sex, race/ethnicity, income, and education. We also included alcohol binge drinking and smoking as predictors since these are known from previous studies to be associated with health status and depression (Ruo et al. 2003; Epstein et al. 2009). We also took into account nativity (U.S.-born vs. foreign-born) and length of stay in the U.S. (categorized as <15 years and ≥15 years). We dichotomized residence in the U.S. at 15 years based on previous studies, where it was found that language shift, as well as other changes in lifestyle, tends to occur within 15 years of arrival in the U.S. (Veltman 1988; Barcenas et al. 2007). All individual-level predictors were coded as dummy variables with reference categories similar to previous studies on LAFANS (Brown et al. 2007; Brown et al. 2008).
Neighborhood-Level Variables
The neighborhood variables used in the analyses were neighborhood socioeconomic index, neighborhood collective efficacy and neighborhood linguistic isolation. Neighborhood socioeconomic index was assessed using each tract’s data obtained from the 2000 U.S. Census. The SES Index (Brown et al. 2007; Winkleby and Cubbin 2003) is the unweighted mean of the standardized values of five census tract variables that represent education (% of those aged 25+ years, without a high school degree), income (median family income), wealth (median home value), occupational status (% blue collar), and employment (% unemployed).
The neighborhood collective efficacy measure is based on previous research by Sampson et al. (1997). Collective efficacy measures the extent to which communities exhibit social cohesion and informal social control. Nine survey items were used, six of which measured social cohesion: (1) this is a close-knit neighborhood; (2) there are adults children can look up to; (3) people are willing to help their neighbors; (4) neighbors generally do not get along with each other; (5) you can count on adults to watch out that children are safe and do not get in trouble; and (6) neighbors do not share the same values. Informal social control was measured by three survey items asking respondents to estimate the likelihood that neighbors would do something if: (1) neighborhood children were skipping school and hanging out on a street corner; (2) children were spray-painting graffiti on a local building; and (3) a child was showing disrespect to an adult. For both sets of items, respondents ranked the items on a 5-point Likert scales (1 = strongly disagree, 5 = strongly agree). The nine items were reverse coded where appropriate, to indicate high scores for high collective efficacy. Finally, the nine-item collective efficacy scale was obtained by aggregating individual scores among those who shared the same census tract (Cronbach reliability = .79). It should be noted that, in terms of internal consistency, we found no significant difference in Cronbach’s alpha reliability for collective efficacy for those interviewed in Spanish (α = .78) compared to those interviewed in English (α = .80).
The measure for neighborhood linguistic isolation was a measure obtained from the 2000 Census tracts, where the U.S. Census Bureau defines linguistic isolation as living in a household in which all members aged 14 years and older speak a non-English language and none speak English “very well” (U.S. Census 2000). All the members of a linguistically isolated household were recorded as linguistically isolated, including members <14 years old who may speak only English. Based on the population counts, the proportion of linguistically isolated households in a neighborhood (i.e., census tract) was computed for all 65 LAFANS Census tracts and appended to individual observations.
In a post-hoc analysis, we also examined the survey respondent’s number of friends in the neighborhood, number of neighbors they spoke to in the past 30 days, and how close they were to their neighbors (scaled from one to five, where 1 = don’t know neighbors, 5 = close friends of neighbors). These three items comprised the neighborhood interaction intensity scale.Footnote 1
Multilevel Models
The LAFANS data used a multistage stratified sampling design where census tracts, blocks within tracts and households were sampled. In order to obtain results that are representative of the entire sample, the models were weighted to account for unequal probabilities of sample selection (Sastry et al. 2006). Weighted multilevel models were constructed to assess the association between neighborhood collective efficacy, linguistic isolation and diagnosis of major depression. At the neighborhood level, the models included neighborhood SES (very poor, poor vs. non-poor), neighborhood collective efficacy, and linguistic isolation as continuous variables. At the individual level, the models included sociodemographic characteristics (age, sex, nativity, length of stay in the US, household income, education), and health behaviors (smoking and alcohol use).
In order to explore the first research question, we examined the Latino sample in the LAFANS data. We used separate hierarchical logistic regressions with linguistic isolation alone, and in the subsequent model included collective efficacy. We then examined the effects of collective efficacy and linguistic isolation together in the same model (Table 3, model 1). In order to analyze the second research question, we examined the effects of collective efficacy on depression among U.S.-born Latinos and longer stay Latino immigrants (≥15 years) relative to shorter stay Latino immigrants (<15 years), which is the reference category (Table 3, model 3). In order to answer the third research question, we examined the effects of linguistic isolation on depression among longer stay immigrants, and U.S.-born Latinos (Table 3, model 4). To answer the fourth research question, we examined the interaction effect between collective efficacy and linguistic isolation in (Table 3, model 2). In all the models, we specify hierarchical random-intercept models (Raudenbush et al. 2006) that allow for the incorporation of both individual-level and tract-level characteristics, as well as adjust for clustering of individuals within census tracts. SAS version 9.1 (SAS Institute Inc., Cary, NC) was used to create the multilevel datasets, Stata version 10 (Stata Corp, College Station, TX) was used to run the random intercept multilevel models using GLLAMM.
Results
The sample comprised 1,468 Latino adults, of whom 205 (14%) were diagnosed with depression. The demographic characteristics of the study sample are presented in Table 1. In the preliminary bivariate analyses, females were more likely to have major depression. At the neighborhood level, collective efficacy and linguistic isolation were significantly, and negatively, associated with depression in the comparisons of neighborhood tracts. No other variables in the bivariate analyses were shown to have significantly different rates of depression.
Correlations among collective efficacy, linguistic isolation and the demographic characteristics are shown in Table 2. Significant positive correlations are interpreted as being associated to each other in the same direction. Significant negative correlations between two variables are interpreted as being associated to each other, but in the opposite direction. Collective efficacy is significantly associated with length of stay with positive correlations for immigrant Latinos who have resided in the US ≥ 15 years. This positive correlation indicates that the mean level of neighborhood collective efficacy is higher for long stay Latinos (≥15 years) compared to Latinos who have resided in the US < 15 years. Linguistic isolation is also significantly associated with length of stay with significant negative correlations for immigrant Latinos who have resided in the US ≥ 15 years. This negative correlation indicates that the mean level of neighborhood linguistic isolation is lower for longer stay Latinos (≥15 years) compared to Latinos who have resided in the US < 15 years. There is no significant correlation between collective efficacy and linguistic isolation. This result supports our first research question that collective efficacy and linguistic isolation appear to be empirically discrete constructs.
To further explore the first hypothesis, separate hierarchical logistic regressions were run with linguistic isolation alone and subsequently adding collective efficacy into the model. We then examined the effects of collective efficacy and linguistic isolation together in the model (Table 3, model 1). In the analysis, there were significant associations between neighborhood characteristics (i.e., neighborhood SES, collective efficacy, linguistic isolation) and depression (Table 3, model 1). Depression was significantly lower for persons who live in neighborhoods with high collective efficacy (OR = .97, 95% CI, .94–.99), and high linguistic isolation (OR = .68, 95% CI, .52–.88). Depression was also higher for persons living in very impoverished tracts (OR = 1.89, 95%CI, 1.07–3.36).
At the individual level, there were significant differences in depression diagnoses between US-born Latinos relative to short stay Latino immigrants (OR = 1.34, 95%CI, 1.02–2.24). However, there were no significant differences in depression diagnoses for long and short stay Latino immigrants. This model shows that if we look at the main effects, nativity is a risk factor but length of stay is not. Other individual characteristics associated with depression were female sex, age 35 to ≥65 years (reference, age 18 to <25 years), having insurance, and being a current smoker.
In order to address our second research question, we examined the interaction effects of collective efficacy on length of stay in the US and nativity. These results are shown in Table 3, models 3. Using multilevel models, we tested cross-level interactions, which are conventional interactions (cross-product terms) between individual-level and neighborhood-level factors. We report significant cross-level interaction effects in the models. In model 3, there was a significant cross-level interaction effect between Latinos who have resided in the US more than 15 years and collective efficacy. Latinos (≥15 years in US) who reside in high collective efficacy neighborhoods were less likely to have depression (OR = .90, 95% CI, .83–.97). This model shows that the length of stay is a risk factor when we examine the interaction effect (Table 3, model 3), but it was not a risk if we just examine the main effect (Table 3, model 1).
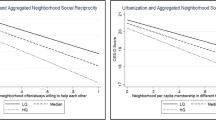
To further explore the effects of collective efficacy on U.S.-born and long-stay immigrants, we examined the three-way interaction effects of language spoken at home, collective efficacy and length of residence in the US. In Table 4, we found a significant three-way interaction effect for English language spoken × collective efficacy × foreign-born Latinos >15 years in the US (OR = .91, 95% CI, .83–.99). There was no significant three-way interaction effect of language spoken at home × collective efficacy × U.S.-born Latinos.
In order to address our third research question, we examined the interaction effects of linguistic isolation on length of stay in the US and nativity. These results are shown in Table 3, model 4. Significant interaction effects were found between linguistic isolation and length of stay, and linguistic isolation and nativity. Foreign-born Latinos (≥15 years in US) and U.S.-born Latinos who reside in neighborhoods with high linguistic isolation were less likely to have depression (OR = .35, 95% CI, .15–.82 and OR = .17, 95% CI, .05–.61, respectively).
To address the fourth hypothesis, we examined the interaction effect between collective efficacy and linguistic isolation (Table 3, model 2). The results show that the regression coefficients changed only marginally, and both linguistic isolation and collective efficacy remain statistically significant whether run separately or jointly, with and without the interaction term. No significant interaction effect between linguistic isolation × collective efficacy was found. We further examined this association using a GAM (generalized additive model) to test the main effects of both variables in the same regression model. The results showed that both variables have statistically significant main effects on depression, with no significant interaction between linguistic isolation and collective efficacy.
In order to assess model fit, the deviance statistics (Raudenbush et al. 2006) were computed for the four models in Table 3. The addition of the interaction term in model 2 for collective efficacy × linguistic isolation shows no improvement in model fit (χ2(1) = .4, p = .53). However, the addition of the interaction terms for collective efficacy in Table 3, model 3 shows a significant improvement in the model fit compared with model 1, where χ2(3) = 31.3, p < .001. There was also significant improvement in model fit when we compare model 4 with model 1, where χ2(3) = 35.1, p < .001. After adding the interaction terms in models 3 and 4, the change in the variance explained by the models were 7.0 and 7.9%, respectively, relative to model 1. There was no change in the variance explained for model 2 vs. model 1.
We also examined neighborhood interaction intensity among Latinos to further explain these findings. Latino immigrants who lived in the U.S. > 15 years and resided in high collective efficacy neighborhoods had more friends living in their neighborhood, talked to neighbors more often and felt closer to their neighbors, compared to those living in low collective efficacy neighborhoods. The neighborhood interaction intensity for high collective efficacy neighborhoods was significantly higher (8.7 vs. 7.1, p < .001) compared to low collective efficacy neighborhoods. Respondents living in neighborhoods with high linguistic isolation felt less close to their neighbors (3.4 vs. 4.3, p = .01), compared to those living in neighborhoods with lower linguistic isolation. There was no significant difference with regards to number of friends living in the neighborhood and how often they talked to neighbors. The neighborhood interaction intensity for neighborhoods with high linguistic isolation was not significantly different compared to neighborhoods with low linguistic isolation. However, Latino residents living in neighborhoods with high linguistic isolation have more relatives living in the same neighborhood compared to neighborhoods with low linguistic isolation (1.68 vs. 1.41, p = .002).
Discussion
We examined whether collective efficacy and linguistic isolation as neighborhood level constructs are protective against risk factors of nativity and duration of stay that are hypothesized to increase depression in the Latino population. Our analytic model is based on the assumption that recent immigrants have lower depression rates than Latino immigrants who have resided for longer periods of time or were born in the US, as documented in previous research (Alegria et al. 2007; Vega et al. 1998b). We tested whether our key neighborhood constructs had protective effects against demographic risk factors that are proxies for social assimilation and associated with higher population depression rates, including nativity (US-born vs. foreign-born), and length of stay among immigrant Latinos (≥15 years vs. <15 years.). Our contention is that collective efficacy is a proxy for informal social control rooted in the perception of residents that functional linkages exist across domains of the social ecology for regulating behavior and problem resolution. A key theoretical assumption is that informal social control is strengthened by closeness of social ties and robust community interaction patterns that increase neighborhood social cohesion. In turn collective efficacy increases conformity to community normative expectations and reduces social deviance, thereby reducing depression among long stay Latino immigrants in the U.S. (≥15 years).
We found a significant reduction in depression attributable to linguistic isolation for immigrants with ≥15 years of residence in the U.S. compared to immigrants with <15 years residence in the U.S. We presume this occurred because the prevalence for depression among more recent immigrants was already lower than reported by the other subgroups. As noted in the literature review, recent immigrants have the lowest rates of depression (Alegria et al. 2007; Vega et al. 1998b). Recently resettled immigrants do not interact as frequently with neighbors as do longer staying immigrants (≥15 years). These results should not be interpreted as volitional avoidance of neighbors by new immigrants,Footnote 2 but is more likely a reflection of low social integration due to inadequate command of the English language and lack of familiarity with U.S. normative expectations about citizen participation in neighborhood affairs. Linguistic isolation must also be thought of contextually (Gresenz et al. 2007). As the proportion of linguistically isolated households increases in a neighborhood, Spanish-speaking individuals are actually less isolated in that neighborhood.
The relationships between linguistic isolation, collective efficacy and depression, adjusted for the demographic risk factors, are complex because these constructs are neither static because they may change over time for both neighborhoods and individuals that reside in them, nor categorical. Collective efficacy reduced depression for longer residence Latino immigrants (e.g., >15 years of residence). It may be that they’ve had sufficient exposure in the U.S. to improve their language skills. Longer stay Latino immigrants whose primary spoken language at home was English benefited most from collective efficacy in lowering depression. This did not occur among immigrants with fewer years residing in the U.S., as their primary social ties were embedded in linguistically compatible neighborhood social networks and they had less contact with immediate neighbors. These results agree with recent research on social networks and help-seeking (Gresenz et al. 2007).
Survey data document that about 70% of California Latino immigrants report being more dominant in Spanish and only about 10% of U.S.-born Latinos are Spanish dominant (Vega and Sribney 2008). This is a critical point because it points out that Latinos receiving protective effects against depression from linguistic isolation are monolingual or to some degree bilingual. The critical distinction is that there is a larger pool of immigrants than U.S.-born Latinos who are functionally bilingual (30% vs. 10%), suggesting that it is bilingual immigrants who are most likely to receive the dual benefits of linguistic isolation and collective efficacy because they have the language skills to develop social ties across a wider range of mixed-language neighborhood networks.
It is important to study selective retention patterns in ethnic enclaves of immigrants to better understand neighborhood effects on depression. Recent research has found that Latinos who were born in the US and reside in low SES neighborhoods are at higher risk than other Latinos for mental health and substance abuse problems and other problematic health behaviors (Gil and Vega 2009; Vega and Gil 2009). In this study collective efficacy did not have any effect on depression among U.S.-born Latinos (residing in low income areas). Future research should examine the personal, social network, and other demographic characteristics of the U.S. Latino group that resides in low SES, ethnically concentrated neighborhoods. U.S.-born Latinos are likely to have different reasons for living in ethnic enclaves. Some with low educational attainment may feel more socially secure residing in primarily co-ethnic neighborhoods because they will not be socially marginalized. Recent social science research has shown a pattern of intergenerational mobility stagnation and increasing residential segregation among people of Mexican origin (Telles and Ortiz 2008). This point underscores the potential for compositional effects in this study wherein the same neighborhoods may act as collection points systematically for subgroups with very different characteristics, e.g. newcomers and natives with dissimilar risk and protective factors for depression. These systematic differences, if confirmed, may result in different causal pathways and neighborhood protective factors for depression within these subgroups (Portes and Zhou 1993).
How Culture is Activated Within the Social Ecology
Linguistically isolated neighborhoods are best characterized as enclaves where newly arrived immigrants have evolved subsocieties reinforcing their respective language and culture. Enclaves have both latent and manifest functions. Their latent functions are in the provision of a receptive cultural “comfort zone” for a population of new and long stay immigrants who wish to sustain their culture and language as a medium for meeting basic human needs and problem solving during resettlement and long term social adjustment. The manifest functions are played out in pragmatic activities of everyday living. These include establishing systems of reciprocity and formal exchange of goods and services, employment information and fostering economic opportunities, child and elder care, recreational activities, and varied faith based programs that provide normative socialization and social regulation for children and adolescents.
Within the enclave the micro and meta systems merge selectively within the greater neighborhood social ecology. The enclave is culturally bounded by language and a common culture which is given specific meaning by the resettlement experience, and other factors such as fear of detection among undocumented immigrants, which further heightens social isolation and embeddedness in homophilius social networks (Lin 1986). With the cultural transition that occurs as a result of exposure to American culture, subsequent generations of Latinos (post-immigration) may find less utility living in ethnic enclaves, especially those who become English language dominant and highly acculturated. Nonetheless, as this study reports, there is a residual protective effect for reducing depression afforded by linguistic isolation for some U.S.-born Latinos who are Spanish-speaking or bilingual. Researchers should be mindful that there are many variants in ethnic community composition, and model building and interpretability of research data will benefit with a finer level of information about these contextual factors and their interplay.
Limitations of the Study
A few cautions and limitations are pertinent to this study. This was not a stress process study so any allusion to social stress vis-à-vis exposure to environmental factors, or social adaptation, was made without benefit of measurement. The LAFANS data included a diverse set of neighborhoods based on a probability sample of all neighborhoods throughout Los Angeles County with an over-sample of poor and very poor neighborhoods. However, there are limitations inherent in the design of the study, as we used cross-sectional data where measures are based on one data point, thus making conclusions largely associational and non-causal. People in worse health, especially newer immigrants, may seek assistance from family members elsewhere or return to their nation of origin creating a selective retention that would attenuate the depression rate. The possibility of both positive selection and reverse selection may decrease the proportion of short-stay residence immigrants likely to be depressed. If true, the resulting composition effects would limit the ability to make inferences about neighborhood effects on depression for immigrants. However, in the sensitivity analyses, we did restrict the analysis to residents who lived in the area for one or more years and controlling for duration of residence produced no significant changes in the results. In addition, we have relied on doctor-diagnosed depression, which inevitably biases the sample toward greater access among U.S.-born Latinos and long-stay Latino immigrants. However, recent surveys have shown that the gap in physician care in the past 12 months among these Latinos subgroups does exist but is not highly disproportionate (Pew 2008).
In the analysis, Census tracts were used as proxy for social ecologies, encompassing communities and neighborhoods. This was based on the original design of LAFANS, where maps were examined and experts were consulted. It was concluded that census tracts most closely approximate social definitions of neighborhoods (Sastry et al. 2006), but this is merely an approximation and has its limitations. The neighborhood data which are based on available Census data is vulnerable to rapid demographic shifts, and there are potentially other neighborhood characteristics that were not examined or controlled that could elaborate or provide additional insights for some of the findings and interpretations. Finally, the bivariate relationships between linguistic isolation and depression, and collective efficacy and depression are both weak. Therefore, any moderation of these effects will also not be large.
Challenges to Social Area Research
As noted by Diez-Roux, “Differences across areas or neighborhoods are the result of macrostructural factors shaping residential segregation (e.g. economic restructuring, migration, discrimination, political decisions and public policies” (p. 1787, Diez-Roux 2001). Thus, a chain of causal elements and reciprocal effects are implicated in understanding neighborhood effects on individuals. How then do we conceptualize, and ultimately operationalize proximate factors that have variance across definable social areas and have face validity as causal agents for individual pathologies? This enigma has opened the door to rethinking the types of information needed and the technical procedures required to detect discrete effects of putatively causal factors using multilevel modeling. We believe the approach we have taken is an example of using explanatory research to identify putatively causal effects of area characteristics on depression among residents with defined characteristics (e.g. linguistic isolation and collective efficacy) (De Silva et al. 2007; Sastry et al. 2006; Diez-Roux 2001). We believe precision is gained by the use of more refined constructs and methods, including juxtaposing constructs as we have done to assess their conceptual independence and covariance with other explanatory factors. The burden of demonstrating discrete effects of social factors at the neighborhood level, and avoiding confounding, remains a major research challenge.
Conclusion
This study examined the effects of neighborhood collective efficacy and linguistic isolation on Latinos residing in an array of Los Angeles communities with mixed ethnic composition as compiled in the LAFANS database. We report that collective efficacy and linguistic isolation are empirically discrete constructs with independent effects on depression among ethnic sub-groups. Collective efficacy and linguistic isolation had differential effects on attenuating depression among long-stay Latino immigrants, and U.S.-born Latinos. Two-way interaction tests showed that collective efficacy reduced depression for long-stay immigrants, and linguistic isolation significantly reduced depression for both long-stay immigrants and U.S.-born Latinos. Short-stay Latino immigrants received no protective benefits from either construct probably because of lower overall population depression levels before their resettlement in the U.S. which were sustained during the early years after resettlement through co-ethnic social network interactions. U.S.-born Latinos received no benefit from collective efficacy, which raises very important research questions about the interaction patterns, social characteristics, and patterns of selective mobility and social adjustment occurring in this subgroup. Although short stay immigrants had a lower risk of depression, it is consistent with the Hispanic health paradox that they were also affording protective effects against risk factors for longer stay immigrants and U.S.-born Latinos.
Notes
The appropriateness of the three items to measure neighborhood interaction intensity was evaluated using exploratory factor analysis (EFA) with varimax rotation, and results indicate that all of the items loaded on one factor and had factor loadings above the criterion of 0.5. The alpha reliability coefficient of the neighborhood intensity scale was 0.66.
In general, however, it is clear that residents who have moved to a neighborhood recently are less likely to interact with neighbors due to unfamiliarity. This would clearly be the case for recent immigrants.
References
Alegria, M., Mulvaney-Day, N., Torres, M., Polo, A., Cao, Z., & Canino, G. (2007). Prevalence of psychiatric disorders across Latino subgroups in the United States. American Journal of Public Health, 97(1), 68–75.
Antonucci, T. C., & Akiyama, H. (1987). Social networks in adult life and a preliminary examination of the convoy model. Journal of Gerontology, 42(5), 519–527.
Barcenas, C. H., Wilkinson, A. V., Strom, S. S., Cao, Y., Saunders, K. C., Mahabir, S., et al. (2007). Birthplace, years of residence in the United States, and obesity among Mexican–American adults. Obesity, 15(4), 1043–1052.
Bronfenbrenner, U. (1995). Developmental ecology through space and time: A future perspective. In P. Moen, G. H. Elder, & K. Luscher (Eds.), Examining lives in context: Perspectives on the ecology of human development (pp. 619–647). Washington, DC: American Psychological Association.
Brown, A. F., Ang, A., & Pebley, A. R. (2007). The relationship between neighborhood characteristics and self-rated health for adults with chronic conditions. American Journal of Public Health, 97(5), 926–932.
Brown, A. F., Vargas, R. B., Ang, A., & Pebley, A. R. (2008). The neighborhood food resource environment and the health of residents with chronic conditions: the food resource environment and the health of residents. Journal of General Internal Medicine, 23(8), 1137–1144.
Browning, C. R., & Cagney, K. A. (2002). Neighborhood structural disadvantage, collective efficacy, and self-rated physical health in an urban setting. Journal of Health and Social Behavior, 43(4), 383–399.
Burnam, M. A., Hough, R. L., Karno, M., Escobar, J. I., & Telles, C. A. (1987). Acculturation and lifetime prevalence of psychiatric disorders among Mexican–Americans in Los Angeles. Journal of Health and Social Behavior, 28, 89–102.
Canino, C., Vega, W. A., Sribney, W. M., Warner, L. A., & Alegria, M. (2008). Social relationships, social assimilation and substance use disorders among adult Latinos in the U.S. Journal of Drug Issues, 38, 69–102.
Cohen, D. A., Finch, B. K., Bower, A., & Sastry, N. (2006). Collective efficacy and obesity: The potential influence of social factors on health. Social Science and Medicine, 62(3), 769–778.
De Silva, M. J., Huttly, S. R., Harpham, T., & Kenward, M. G. (2007). Social capital and mental health: A comparative analysis of four low income countries. Social Science and Medicine, 64(1), 5–20.
Diez-Roux, A. (2001). Investigating neighborhood and area effects on health. American Journal of Public Health, 91(11), 1783–1789.
Epstein, J. F., Induni, M., & Wilson, T. (2009). Patterns of clinically significant symptoms of depression among heavy users of alcohol and cigarettes. Preventing Chronic Disease, 6(1), A09.
Finch, B. K., Boardman, J. D., Kolody, B., & Vega, W. A. (2000). Contextual effects of acculturation on perinatal substance exposure among immigrant and native-born Latinas. Social Science Quarterly, 81(1), 421–438.
Finch, B. K., Lim, N., Perez, W., & Do, P. (2007). Toward a population health model of segmented assimilation: The case of low birth-weight in Los Angeles. Sociological Perspectives, 50(3), 445–468.
Gil, A. G., & Vega, W. A. (2009). Alcohol, Tobacco, and Other Drugs. In M. Aguirre-Molina, L. Borreall, & W. A. Vega (Eds.), Latino male health. New Brunswick, NJ: Rutgers University Press.
Gordon-Larsen, P., Harris, K. M., Ward, D. S., & Popkin, B. M. (2003). Acculturation and overweight-related behaviors among Hispanic immigrants to the US: The National longitudinal study of adolescent health. Social Science and Medicine, 57(11), 2023–2034.
Gottlieb, B. H. (1978). The development and application of a classification scheme of informal helping behaviors. Canadian Journal of Behavioural Science, 10, 105–115.
Grant, B. F., Stinson, F. S., Hasin, D. S., Dawson, D. A., Chou, S. P., & Anderson, K. (2004). Immigration and lifetime prevalence of DSM-IV psychiatric disorders among Mexican Americans and non-Hispanic Whites in the United States. Archives of General Psychiatry, 61, 1226–1233.
Gresenz, C. R., Rogowski, J., & Escarce, J. (2007). Health care markets, the safety net, and utilization of care among the uninsured. Health Services Research, 42(1 Pt 1), 239–264.
Guerra, N. G., & Knox, L. (2008). How culture impacts the dissemination and implementation of innovation: A case study of the families and schools together program (FAST) for preventing violence with immigrant Latino youth. American Journal of Community Psychology, 41, 304–313.
Hawkins, J. D., Catalano, R. F., & Millar, J. Y. (1992). Risk and protective factors for alcohol and other drug problems in adolesence and early childhood: Implications for substance abuse prevention. Psychological Bulletin, 112, 64–105.
Kelly, J. G., & Chang, J. (2008). Pluralistic inquiry for the history of community psychology. Journal of Community Psychology, 36, 675–691.
Kubrin, C. E., & Weitzer, R. (2003). New directions in social disorganization theory. Journal of Research in Crime and Delinquency, 40, 374.
Lin, N. (1986). Conceptualizing social support. In N. Lin, A. Dean, & W. Ensel (Eds.), Social support, life events, and depression (pp. 17–30). New York: Academic Press.
Morenoff, J. D. (2003). Neighborhood mechanisms and the spatial dynamics of birth weight. American Journal of Sociology, 108(5), 976–1017.
Park, Y., Neckerman, K. M., Quinn, J., Weiss, C., & Rundle, A. (2008). Place of birth, duration of residence, neighborhood immigrant composition and body mass index in New York City. International Journal of Behavioral Nutrition and Physical Activity, 5(19).
Pearlman, D. N., Zierler, S., Gjelsvik, A., & Verhoek-Oftedahl, W. (2003). Neighborhood environment, racial position, and risk of police-reported domestic violence: a contextual analysis. Public Health Reports, 118(1), 44–58.
Pebley, A. R., & Sastry, N. (2004). The Los Angeles family and neighborhood survey household questionnaires (Spanish). RAND Labor and Population Program Working Paper DRU-2400/4-LAFANS.
Pew Research Center Project. (2008). Hispanic and health care in the United States: Access, information and knowledge. Washington, DC: A Joint Pew Hispanic Center and Robert Wood Johnson Foundation Research Report.
Portes, A., & Zhou, M. (1993). The new second generation: Segmented assimilation and its variants. Annals of the American Academy of Political & Social Sciences, 530, 74–96.
Raudenbush, S. W., Bryk, A. S., Cheong, Y. F., & Congdon, R. (2006). HLM6: Hierarchical linear and nonlinear modeling. Lincolnwood, IL: Scientific Software International.
Ruo, B., Rumsfeld, J. S., Hlatky, M. A., Liu, H., Browner, W. S., & Whooley, M. A. (2003). Depressive symptoms and health related quality of life: The Heart and Soul Study. JAMA, 290(2), 215–221.
Sampson, R. J. (2003). The neighborhood context of well-being. Perspectives in Biology and Medicine, 46(3 Suppl.), S53–S64.
Sampson, R. J., Raudenbush, S. W., & Earls, F. (1997). Neighborhoods and violent crime: a multilevel study of collective efficacy. Science, 277(5328), 918–924.
Sastry, N., Ghosh-Dastidar, B., Adams, J., & Pebley, A. R. (2006). The design of a multilevel longitudinal survey of children, families, and communities: The Los Angeles Family and Neighborhood Study, RAND. Social Science Research, 35(4), 1000–1024.
Schensul, J. J. (2009). Community, culture, and sustainability in multilevel dynamic systems intervention science. American Journal of Community Psychology, 43, 241–256.
Szapocznik, J., & Coatsworth, J. D. (1999). An ecodevelopmental framework for organizing the influences on drug abuse: A developmental model of risk and protection. In M. D. Glantz & C. R. Hartel (Eds.), Drug abuse: Origins and intervention. Washington, DC: American Psychological Association.
Telles, E., & Ortiz, V. (2008). Generations of exclusion: Mexican Americans, assimilation and race. NY: Russell Sage Foundation Press.
US Census. (2000). Summary file 3. Retrieved August 10, 2009 from http://www.census.gov/Press-Release/www/2002/sumfile3.html.
Vega, W. A., Alderete, E., Kolody, B., & Aguilar-Gaxiola, S. (1998a). Illicit drug use among Mexicans and Mexican Americans in California: The effects of gender and acculturation. Addiction, 93(12), 1839–1850.
Vega, W. A., & Gil, A. G. (2009). Substance use in minority populations. In S. Loue & M. Sajatovic (Eds.), Determinants of minority mental health and wellness (pp. 313–314). NY: Springer.
Vega, W. A., Kolody, B., Aguilar-Gaxiola, S., Alderete, E., Catalano, R., & Caraveo-Anguaga, J. (1998b). Lifetime prevalence of DSM-III-R psychiatric disorders among urban and rural Mexican Americans in California. Archives of General Psychiatry, 55, 771–778.
Vega, W. A., Kolody, B., Valle, R., & Weir, J. (1991). Social networks, social support, and their relationship to depression among immigrant Mexican women. Human Organization, 50, 154–162.
Vega, W. A., & Sribney, W. (2008). Latino population demographics, risk factors and depression. In S. Aguilar-Gaxiola, E. Kramer, & T. P. Gullotta (Eds.), Depression in Latinos: Assessment, treatment and prevention (pp. 29–52). NY: Springer.
Veltman, C. (1988). Modelling the language shift process of Hispanic immigrants. International Migration Review, 22(4), 545–562.
Winkleby, M. A., & Cubbin, C. (2003). Influence of individual and neighborhood socioeconomic status on mortality among black, Mexican–American, and White women and men in the United States. Journal of Epidemiology and Community Health, 57, 444–452.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vega, W.A., Ang, A., Rodriguez, M.A. et al. Neighborhood Protective Effects on Depression in Latinos. Am J Community Psychol 47, 114–126 (2011). https://doi.org/10.1007/s10464-010-9370-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10464-010-9370-5