
Abstract
Increasing HIV testing frequency in gay and bisexual men (GBM) is critical to reducing the time between HIV infection and diagnosis. Using anonymous national behavioural surveillance data (2013–2018) from 43,753 surveys of Australian GBM, we examined HIV testing frequency trends and factors differentiating PrEP-users, non-PrEP-users reporting two or more tests in the previous year, and non-PrEP-users reporting less frequent testing. The proportion tested at least annually increased from 64.4% in 2013 to 70.8% in 2018 (p-trend < 0.001), and from 73.9% to 84.6% among the 51.6% of men classified as higher-risk. Among higher-risk men, having two or more tests in the previous year increased from 48.0% to 69.3% (p-trend < 0.001). Among higher-risk non-PrEP-users, it increased from 47.2% to 54.8% (p-trend < 0.001), however, there was a decrease since 2016 (p-trend < 0.001). Among PrEP-users, it increased from 82.1% in 2013 to 97.3% in 2018 (p-trend < 0.001). Non-PrEP-using higher-risk men having less frequent tests reported lower risk than PrEP-users and non-PrEP-using men reporting two or more tests in the previous year. However, recent risk behaviour was not uncommon: nearly half reported condomless sex; one-fifth reported receptive condomless sex with ejaculation; over half reported group sex; one-quarter used drugs for the purposes of sex; and one-fifth had more than ten sex partners. Efforts are needed to encourage frequent testing and PrEP use among non-PrEP-users who are at higher-risk.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Australia’s guidelines for HIV and sexually transmitted infection (STI) testing published in 2014 recommended that sexually active gay, bisexual, and other men who have sex with men (GBM) be tested for HIV at least once per year. The guidelines recommended more frequent testing, up to four times per year, for GBM who had condomless anal intercourse (CLAI), more than ten sexual partners, group sex or drugs for the purposes of sex in the previous 6 months [1, 2]. These guidelines were recently updated to recommend quarterly HIV testing for all GBM [3]. Additionally, PrEP-users are required to have quarterly HIV tests to continue receiving prescriptions under Australian PrEP guidelines [4]. These clinical guidelines are supported by Australia’s current national HIV strategy, which aims to “improve the frequency, regularity and targeting of testing for priority populations and decrease rates of late diagnosis” (p. 26) [5].
Increasing HIV testing frequency in high-risk populations such as GBM is critical to reducing the time between HIV infection and diagnosis—the period in which viral loads are high [6] and prior to the reduction in sexual risk behaviour that is typically observed after HIV diagnosis [7, 8]. Men with undiagnosed infection contribute disproportionately to new HIV transmissions [9]. With the introduction and promotion of biomedical HIV prevention—particularly PrEP—and the associated rapid changes in sexual behaviour observed in gay communities [10, 11], frequent testing has become more essential. It is the gateway to both PrEP initiation and early initiation of treatment to reduce the risk of onwards transmission, as well as other non-condom-based strategies such as strategic positioning and serosorting.
Over recent years, strategies to increase HIV testing in Australian GBM have included: text message clinic testing appointment reminders [12]; provision of HIV test results by telephone and removing the need for pre- and post-test counselling [13]; rapid HIV testing [14]; ‘express clinics’ within publicly-funded sexual health centres [15]; peer-led, community-based HIV testing sites [16,17,18,19], including in-language services for recently-arrived migrants from Asia [20]; online-facilitated home sampling [21]; social marketing to mobilise demand for testing [22]; and the introduction of HIV self-testing [23]. Scale-up of PrEP could also be considered as such a strategy, given that access to prescriptions is tied to frequent testing [3]. Over the long term, HIV testing frequency among Australian GBM has increased: the proportion of non-HIV-positive men in Australia getting tested in the previous 12 months increased from 56.1% in 2000 to 64.8% in 2015 [24]. However, previous reports showed GBM did not test as frequently as recommended in the national guidelines [25,26,27].
The rapid rollout of PrEP in Australia is likely to have been accompanied by increased testing frequency in PrEP-users. It is likely to become increasingly important to stratify HIV testing data by PrEP status to assess testing frequency among GBM susceptible to HIV infection and to ensure rates of testing among PrEP-users do not mask rates in non-users. Using national, repeated, cross-sectional gay community-based behavioural surveillance data, this analysis therefore had three aims: (1) To examine trends in HIV testing frequency among non-HIV-positive GBM, stratifying by PrEP use; (2) To examine trends in HIV testing frequency among non-HIV-positive men defined as ‘higher-risk’ according to the national HIV/STI testing guidelines, stratifying by PrEP use; and (3) To determine, within higher-risk GBM, demographic and behavioural factors differentiating PrEP-users, non-PrEP-users reporting two or more tests in the previous year, and non-PrEP-users reporting fewer than two tests in the previous year.
Methods
Procedures and Participants
Details of the Australian national behavioural HIV surveillance system for GBM, the Gay Community Periodic Surveys (GCPS), have been previously described [24, 28]. Briefly, the GCPS used time-location sampling in seven states and territories annually or biennially to recruit GBM at gay venues, events, sex-on-premises, and clinics. Face-to-face recruitment was undertaken by trained staff who invited men to self-complete a paper questionnaire. Recruiters recorded refusals among eligible men, with a typical response rate among eligible men of 70%. In most cities from 2014 onwards, face-to-face recruitment occurred over 2 weekends, followed by a week of online recruitment driven by paid Facebook advertising. In Tasmania, recruitment occurred solely online. Overall, online recruitment accounted for approximately one-fifth of the GCPS sample (15.3% in 2014 to 26.2% in 2018). Community-based organisations were central to promotion and recruitment in each round.
Participants were eligible if they: were aged at least 18 years (face-to-face recruitment) or 16 years (online recruitment), were male (including male-identified cisgender and transgender participants), had sex with a man in the past 5 years and/or identified as gay or bisexual, and lived in Australia. The surveys were anonymous, and men could complete the surveys in multiple survey rounds; thus, it was not possible to determine the number of unique GBM participating. Ethical approval was received from the Human Research Ethics Committee of the University of New South Wales (UNSW) and two community organisations.
Measures and Variable Definition
Details of the GCPS measures have been previously described [24, 28]. Frequency of HIV testing was assessed since 2013 with the question, ‘How many HIV tests have you had in the last 12 months?’ with the response options ‘none’, ‘one’, ‘two’, ‘three to four’ or ‘five or more’. For this analysis, the latter categories were combined into ‘three or more’ tests or ‘two or more’ tests. ‘Frequent testers’ and ‘non-frequent testers’ were defined as those reporting two or more HIV tests or fewer than two tests in the previous year, respectively. ‘PrEP-users’ were defined as those reporting any use of prescribed or non-prescribed PrEP in the last 6 months. Respondents were classified as ‘higher-risk’ (according to the national HIV/STI guidelines) if they were sexually active and reported one or more of the following in the previous the 6 months: any condomless anal intercourse with casual male partners (CLAIC), group sex, more than ten male sex partners, and using recreational drugs for sex [1]. Covariates were selected for inclusion in the analysis based on previous associations with HIV testing, use of clinical services, and uptake of or disparities in HIV prevention. Demographic factors included age, country of birth, education, employment, and HIV status [29,30,31,32]. We included factors associated with connection to gay identity and community, including sexual identity, social engagement, location of residence, and PrEP awareness [30, 32]. Social engagement with other gay men was measured with a two-item scale, assessing number of gay male friends and amount of time spent socially with gay men [28, 32]. Participants reported their postcode or suburb of residence. All postcodes were categorised as a ‘gay suburb’ (where greater than 10% of men living in that postcode were estimated to be gay-identified) or not [33]; postcode of residence has previously been found to be associated with PrEP uptake [29]. Sexual behaviour and STI covariates were included to determine the levels of potential HIV risk across the groups.
Analysis
We used survey data from all Australian jurisdictions from 2013 to 2018. Surveys were conducted in New South Wales (NSW), Victoria, and Queensland annually, and less frequently elsewhere (South Australia: 2014, 2016; Western Australia: 2014, 2016, 2017; Australian Capital Territory [ACT]: 2015, 2017; Tasmania: 2014, 2016, 2018). HIV-positive men and men with missing data on key variables were excluded from the analysis.
The analysis is presented in three parts. First, the ‘full sample’ includes all surveys completed by non-HIV-positive men from 2013 to 2018, used to examine trends in surveys among all non-HIV-positive GBM. Second, the ‘higher-risk sample’ includes surveys completed by those recommended to have frequent HIV testing (that is, more than one and up to four HIV tests per year) under the 2014 testing guidelines, which was used to examine trends from 2013 to 2018 in surveys among higher-risk GBM. Third, the ‘cross-sectional higher-risk sample’ is a subset of the abovementioned higher-risk sample, where data were restricted to the most recent available survey round for each Australian state/territory (2018 for NSW, Victoria, Queensland, South Australia, and Tasmania; and 2017 for Western Australia and ACT). This sample was used to examine factors differentiating three groups: (1) non-PrEP-users who were non-frequent testers (fewer than two HIV tests in the previous year); (2) non-PrEP-users who were frequent testers (two or more HIV tests in the previous year; and (3) PrEP-users.
Data were analysed using Stata 14.2 (Stata Corporation, College Station, Texas, USA). Statistical significance was set at p < 0.05 (two-tailed). Trends in HIV testing over time in the full sample and higher-risk sample were assessed with generalised linear models (logistic regression). Trends were assessed for three outcome variables (with various stratifications): ever having been tested for HIV (dichotomous yes/no variable), having been tested for HIV in the previous year (dichotomous yes/no variable), and number of tests in the previous year (this variable had four response options: none, one, two, and three or more. Each response option was tested separately; a dichotomous yes/no dummy variable was created and used as the outcome variable for each level). In these models, calendar year was the independent variable. Trends were assessed for two time periods: (1) the full 6-year period (2013–2018) for which the HIV testing frequency data were available; and (2) the most recent 3 years of data (2016–2018). The year 2016 was selected as the reference year for the second of these trend analyses as it was the year during which rapid increases in PrEP use began via large-scale clinical trials (which started at different points during 2016). Statistical significance of trends is reported as ‘p-trend’; we also report odds ratios (OR) and 95% confidence intervals (95% CI) for these trends. As the surveys were anonymous, it was not possible to adjust for individuals appearing in multiple years, including potential classification as non-PrEP-users in one year and PrEP-users in a subsequent year. In the cross-sectional higher-risk sample, factors differentiating the three groups were assessed using bivariate and multivariate multinomial logistic regression models. The reference group for these models was non-PrEP-using non-frequent testers. Multivariate models controlled for survey year and state/territory. We report p-values for the bivariate associations, and adjusted relative risk ratios (aRRR), 95% CI and p-values for the multivariate associations.
Results
Between 2013 and 2018, 49,283 GCPS surveys were completed. After excluding surveys completed by HIV-positive men (n = 3997) and men with missing data on key variables (n = 1533), 43,753 survey responses remained (full sample). The mean number of responses per year was 7292 (± 1174; range = 5404 [2013] to 8535 [2016]). Among the surveys across all included years, the median age was 32 (interquartile range [IQR] = 26–43). Most surveys were from participants who were born in Australia (70.9%), were HIV-negative (86.7%), identified as gay (88.5%), and were in full-time employment (64.5%). Over half of the surveys were from men with university-level education (51.6%). Overall, 8.1% (n = 3544) of surveys were from men who took PrEP in the previous 6 months, increasing from 1.5% of the full sample in 2013 to 20.9% in 2018 (OR 1.96, 95% CI 1.91–2.02, p-trend < 0.001), with the largest increase between 2016 (n = 392, 4.6%) and 2017 (n = 1263, 15.1%). Most PrEP was prescribed (85–95%) and thus most likely to be daily use.
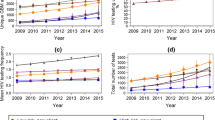
In the full sample, having ever been tested for HIV increased between 2013 and 2018 in the surveys among all men (OR 1.10, 95% CI 1.08–1.12, p-trend < 0.001), non-PrEP-users (OR 1.05, 95% CI 1.03–1.07, p-trend < 0.001), and PrEP-users (OR 1.63, 95% CI 1.39–1.91, p-trend < 0.001), but there was no increase in the last 3 years (OR 1.05, 95% CI 1.00–1.10, p-trend = 0.066; OR 0.95, 95% CI 0.91–1.00, p-trend = 0.063; and OR 0.95, 95% CI 0.57–1.57, p-trend = 0.832, respectively; Table 1 and Fig. 1). In 2018, 88.4% of non-PrEP-users had ever been tested, compared to 99.1% of men on PrEP. Having an HIV test in the last 12 months increased in the surveys among all men and among PrEP-users (OR 1.02, 95% CI 1.02–1.03, p-trend < 0.001; and OR 1.56, 95% CI 1.35–1.81, p-trend < 0.001), but not among non-PrEP-users (OR 1.00, 95% CI 1.00–1.00, p-trend = 0.844). Indeed, over the last 3 years, annual testing decreased in the surveys among non-PrEP-users (OR 0.96, 95% CI 0.95–0.97, p-trend < 0.001). In all men, the proportion of surveys among men reporting two or more HIV tests in the previous year increased from 37.0% in 2013 to 50.4% in 2018 (OR 1.07, 95% CI 1.06–1.08, p-trend < 0.001), while in surveys among PrEP-users it increased from 81.3% in 2013 to 96.5% in 2018 (OR 1.02, 95% CI 1.01–1.03, p-trend < 0.001). In surveys from men not using PrEP, the increase was smaller, from 36.3% in 2013 to 38.2% in 2018 (OR 1.01, 95% CI 1.01–1.02, p-trend < 0.001) and decreased in the last 3 years from 42.9% in 2016 (OR 0.94, 95% CI 0.92–0.96, p-trend < 0.001).

HIV testing trends (2013–2018) in a all non-HIV-positive men, b non-PrEP-users, and c PrEP-users
The respondents in just over half of the surveys (n = 22,596, 51.6%) were classified as higher-risk and thus were recommended to have frequent HIV testing (ranging from 50.2% in 2013 to 53.2% in 2018). The non-mutually exclusive reasons for classification as higher-risk were: any CLAIC (49.2%); any drug use for sex (29.9%); more than ten sex partners (36.9%); and any group sex (58.3%). PrEP use was reported in 13.8% (n = 3123) of the surveys among higher-risk GBM, increasing from 2.5% in 2013 to 34.1% in 2018 (p-trend < 0.001), with the largest increase between 2016 (n = 356, 8.7%) and 2017 (n = 1133, 25.8%).
In the higher-risk sample, ever having had an HIV test increased from 88.3% in 2013 to 94.3% in 2018 (OR 1.19, 95% CI 1.16–1.22, p-trend < 0.001), with no change over the past 3 years (OR 0.92, 95% CI 0.74–1.01, p-trend = 0.070; Table 2 and Fig. 2). In surveys among non-PrEP-users, ever being tested rose from 88.1% in 2013 to 94.8% in 2016 (OR 1.05, 95% CI 1.04–1.06, p-trend < 0.001), and decreased to 91.8% in 2018 (OR 0.79, 95% CI 0.72–0.86, p-trend < 0.001). In surveys among PrEP-users, it increased from 97.0% in 2013 to 99.3% in 2018 (OR 1.67, 95% CI 1.38–2.01, p-trend < 0.001). Having an HIV test in the previous 12 months increased in surveys completed by all higher-risk men (73.9–84.6%; OR 1.03, 95% CI 1.03–1.04, p-trend < 0.001), non-PrEP-users (73.4–77.2%; OR 1.02, 95% CI 1.01–1.02, p-trend < 0.001), and PrEP-users (92.5–98.8%; OR 1.56, 95% CI 1.32–1.85, p-trend < 0.001); there was no change in the last 3 years in all men and PrEP-users, while annual testing in surveys among non-PrEP-users decreased from 2016 to 2018 (OR 0.97, 95% CI 0.96–0.98, p-trend < 0.001). Having two or more tests in the previous year increased from 48.0% of surveys among all higher-risk men in 2013 to 69.3% in 2018 (OR 1.09, 95% CI 1.08–1.10, p-trend < 0.001). In surveys among higher-risk non-PrEP-users, it increased from 47.2% in 2013 to 54.8% in 2018 (OR 1.04, 95% CI 1.03–1.05, p-trend < 0.001), however, there was a decrease since 2016 (OR 0.95, 95% CI 0.93–0.97, p-trend < 0.001). Among surveys completed by PrEP-users, it increased from 82.1% in 2013 to 97.3% in 2018 (OR 1.55, 95% CI 1.38–1.75, p-trend < 0.001).

HIV testing trends nn among non-HIV-positive higher risk GBM, in a all men, b non-PrEP-users, and c PrEP-users
Figure 3 shows surveys among the higher-risk men who had two or more tests in the previous year. The proportion who were PrEP-users increased from 4.2% in 2013 to 47.9% in 2018 (OR 1.82, 95% CI 1.77–1.87, p-trend < 0.001; Fig. 3a). Since 2016, the increase in absolute number of surveys from higher-risk men having two or more tests was entirely among PrEP-users (Fig. 3b).

Among higher risk GBM who reported having two or more HIV tests in the previous year, a proportion and b absolute number of PrEP-users versus non-PrEP-users
A comparison of non-PrEP-using non-frequent testers (n = 1362), non-PrEP-using frequent testers (n = 1666), and PrEP-users (n = 1445) in the cross-sectional higher-risk sample (n = 4473) is presented in Table 3. Of the non-PrEP-using non-frequent testers, 50.4% (n = 686) reported no HIV tests and 49.6% (n = 676) reported one test in the previous year, respectively. Over half (n = 864, 51.9%) of non-PrEP-using frequent testers reported three or more tests. First, compared to the higher-risk non-PrEP-using non-frequent testers, the non-PrEP-using frequent testers were more likely to be slightly younger (aRRR 0.98, 95% CI 0.97–0.99), have higher partner numbers (e.g. aRRR for greater than 20 partners 2.27, 95% CI 1.72–3.00), be aware of PrEP availability (aRRR 1.24, 95% CI 1.02–1.52), report recent CLAIC (aRRR 1.22, 95% CI 1.00–1.49) and occasional receptive CLAIC with ejaculation (aRRR 1.50, 95% CI 1.17–1.93), have had an STI diagnosis in the previous year (aRRR 3.65, 95% CI 2.89–4.61); and be less likely to have unknown serostatus (aRRR 0.06, 95% CI 0.04–0.09). There were no statistically significant differences in sexual identity, country of birth, education, employment, living in a ‘gay suburb’, group sex, and drug use for sex. Second, compared to the higher-risk non-PrEP-using non-frequent testers, the PrEP-users were more likely to be slightly younger (aRRR 0.99, 95% CI 0.98–1.00), have a university degree (aRRR 1.26, 95% CI 1.03–1.53), be in full-time employment (aRRR 1.29, 95% CI 1.05–1.59), live in a ‘gay suburb’ (aRRR 1.57, 95% CI 1.25–1.97), be socially engaged with other gay men (aRRR 1.25, 95% CI 1.17–1.34), know about PrEP availability (aRRR 5.90, 95% CI 4.14–8.40), report more sexual partners (e.g. aRRR for more than 20 partners 4.13, 95% CI 3.03–5.64) and group sex (aRRR for occasional group sex 1.39, 95% CI 1.13–1.72; aRRR for frequent group sex 2.29, 95% CI 1.59–3.30), report recent CLAIC (aRRR 2.53, 95% CI 1.97–3.26) and receptive CLAIC with ejaculation (aRRR for occasional receptive CLAIC with ejaculation 3.02, 95% CI 2.30–3.96; aRRR for frequent receptive CLAIC with ejaculation 2.63, 95% CI 1.85–3.75), and have had an STI diagnosis in the previous year (aRRR 6.53, 95% CI 5.11–8.36); and were less likely to have unknown serostatus (aRRR 0.11, 95% CI 0.07–0.19). Country of birth, sexual identity and drug use for the purposes of sex were not significantly associated.
Discussion
Data from repeated surveys indicate that HIV testing frequency among Australian GBM has increased over time. Between 2013 and 2018, having two or more HIV tests in the previous year increased substantially in surveys among all men and among GBM classified as higher-risk under the Australian testing guidelines [1]. The increase in the proportions reporting three or more tests in the previous year accounted for most of these changes. Yet despite these increases, nearly one-third of the higher-risk men in 2018 had fewer than two tests in the previous year.
Most of the increase in HIV testing frequency was concentrated in the surveys completed by PrEP-users. In several Australian jurisdictions, large-scale PrEP implementation trials were initiated during 2016 [29, 34, 35]. In our data, by 2018, having two or more tests in the previous year was reported by more than 95% of PrEP-users and few PrEP-users reported no tests (< 2% since 2016). Among the surveys completed by higher-risk non-PrEP-using men, there was a 16% increase in those reporting two or more tests in the previous year between 2013 and 2018, but there was a 9% decrease since 2016. Since 2016, the increase in the two or more tests category was completely attributable to PrEP-users (Fig. 3b), coincident with the rapid scale-up of PrEP via the trials. It is likely that the apparent decrease in frequent testing in higher-risk non-PrEP-users is due to frequent testers initiating PrEP (that is, moving from the non-PrEP-using category in one year to the PrEP-using category in a later year); due to the anonymous nature of the GCPS, it is not possible to determine the PrEP initiation and usage patterns of individuals over time. However, the key point remains: the majority of higher-risk non-PrEP-using men in the most recent data did not have the recommended two or more tests in the previous year.
Within higher-risk men recommended for frequent testing, we aimed to determine demographic and behavioural factors differentiating three mutually exclusive groups of GBM (non-PrEP-using non-frequent testers, non-PrEP-using frequent testers, and PrEP-users). PrEP-users have been well-characterised by previous research indicating that the ‘riskiest’ and most sexually active men have been well-targeted for PrEP in Australia [11, 36] and PrEP uptake is associated with social engagement with gay friends, living in suburbs with high concentrations of gay men, and markers of higher socioeconomic status [36]; our analysis reconfirmed these findings. A novel aspect of our analysis demonstrated that for many sociodemographic and behavioural factors, there were ‘stepped’ gradations between the three groups examined. For example, PrEP-users were typically the most socially connected to other gay men, non-PrEP-using non-frequent testers were the least connected, and non-PrEP-using frequent testers were somewhere in the middle. This ‘stepped’ pattern (or its reverse) was observed for most of the variables examined in the multivariate model. Thus, those who reported more frequent HIV testing did appear to be at greater need of it, given their sexual practices, compared to those who reported fewer tests.
However, although these non-PrEP-using non-frequent testers reported less prevalent and less frequent risk behaviours than the other two groups, they were all still classified as higher-risk according to the guidelines. Furthermore, risk behaviours were not uncommon: nearly half reported CLAIC in the last 6 months; nearly one-fifth reported receptive CLAIC with ejaculation; over half reported group sex; one-quarter used drugs for the purposes of sex; one-fifth had more than 10 sex partners in the last 6 months; and 9% were diagnosed with an STI in the previous year. Half of these men reported no tests in the previous year. Given the risk behaviours reported, and the low frequency of testing, if infected with HIV, these men are unlikely to be diagnosed soon after infection. This has implications not only for their own health due to delayed HIV treatment initiation [37], but also the increased risk of transmission to others [38], particularly if they have sex in networks with lower PrEP use (such as men living in the outer suburbs of Australia’s large cities and those less connected to gay community [29]).
Even in a country that has achieved the UNAIDS 90-90-90 targets [39, 40] and relatively high use of PrEP among high-risk GBM [10], there is still room for improvement in HIV testing frequency. The virtual elimination of HIV transmission will not be achieved with long delays between HIV infection and diagnosis given that men with undiagnosed infection contribute disproportionately to new HIV transmissions [9].
Several implications arise from our findings. First, observed increases in HIV testing frequency in settings with widespread PrEP uptake may be misleading. As HIV testing is a requirement of PrEP programs, scale-up of PrEP is likely to thus coincide with increased testing frequency at a population level. If such increases are concentrated among adherent PrEP-users (who are no longer at risk of acquiring HIV), this may mistakenly give the impression that HIV testing coverage and frequency are increasing among HIV-susceptible GBM in whom testing is arguably most needed. In our data, frequent HIV testing among surveys completed by higher-risk men increased significantly since PrEP rollout started during 2016, but these increases disappeared when the surveys from PrEP-users were excluded. Our results are supported by clinical data on HIV testing frequency reported in the NSW government’s publicly-available HIV data reports. The observed increase in average number of tests per year per GBM has been solely concentrated among PrEP-users: while PrEP-using GBM had on average 4.5 HIV tests per year at the end of 2018, non-PrEP-using high-risk GBM had an average of 2.2 tests per year—and testing frequency among these men has not increased since 2013 [21]. It would be helpful if other jurisdictions in Australia and elsewhere reported on HIV testing frequency among higher-risk populations, as it appears that most do not include such data [40,41,42,43,44,45,46]. However, if they do so, they should ensure to disaggregate PrEP-users from non-PrEP-users.
Second, greater efforts are needed in GBM community education to improve men’s knowledge of the HIV/STI testing guidelines and encourage increased testing frequency among higher-risk GBM. For the most part, testing frequency among PrEP-users is managed ‘automatically’ since they must be tested to obtain their quarterly PrEP prescription. Research has shown relatively low rates of PrEP cessation in Australian GBM who start it, especially among those engaging in CLAIC and frequent sexual activity [47]. Thus, it is important to focus efforts to increase HIV testing frequency on higher-risk non-PrEP-using men susceptible to HIV infection. This may have the added benefit of providing opportunities to initiate more GBM onto PrEP.
Third, given the already high levels of HIV testing generally, it is equally if not more important to continue implementing innovative testing models to increase the convenience of and reduce barriers to testing. Our data indicated that in the last 2 years, around 10% of the surveys in higher-risk non-PrEP-using GBM were in those who had never been tested, and over one-fifth were in those who had not had a test in the previous 12 months. Further effort must be put into understanding why such men do not test and offer testing innovations to counter identified barriers. It is also important to note that intensified efforts to increase testing have not been implemented consistently across Australian states/territories; jurisdictions that have not yet implemented testing innovations may learn from others that have done so. Additionally, in the context of widespread PrEP use, there can be competition for available clinic appointments and stress on services to meet demand. It is important that non-PrEP-users are accommodated within clinics, given that they remain at greater risk for HIV infection.
Our analysis is subject to some limitations. The GCPS targets GBM who are socially and sexually engaged with each other, primarily in metropolitan areas. This is consistent with guidelines for behavioural surveillance [48], which recommend the tracking of populations at increased risk of HIV. However, it is unlikely to be a representative sample of Australian GBM, as it had comparatively fewer men who identified as bisexual and men from regional areas as would be expected in a representative sample of Australian GBM [49]. Due to the anonymous nature of the surveys, individual GBM may have completed the survey in multiple years and it was not possible to determine the number of unique respondents. Statistically, this means that some responses from the same individuals across survey rounds were treated as independent. However, the anonymous nature of many HIV behavioural surveillance systems is well-established, and is consistent with guidelines acknowledging that anonymity encourages greater honesty [48]. Recall bias may have led to overestimations in the testing frequency estimates. Self-report may have led to social desirability bias, although this is unlikely given the surveys were anonymous.
Conclusions
Although Australian behavioural surveillance data showed an increase in HIV testing frequency among GBM, the observed increases since 2016 have been almost entirely due to the increase in testing by PrEP-users. There is a critical need to ensure that HIV testing data is disaggregated by PrEP use and level of sexual risk, especially in surveillance reports used to guide HIV testing and prevention responses. Although higher-risk non-PrEP-using men who did not test frequently appeared to be at somewhat lower HIV risk (compared to PrEP-users and to non-PrEP-users who had two or more tests per year), risk behaviours and high levels of sexual activity were not uncommon and thus, new HIV infections may lead to transmission clusters driven by undiagnosed men. Further efforts are required to encourage frequent testing among higher-risk GBM and to reduce barriers to testing.
References
STIs in Gay Men Action Group. Australian sexually transmitted infection and HIV testing guidelines 2014. Sydney, NSW: STIs in Gay Men Action Group; 2014.
Templeton DJ, Read P, Varma R, Bourne C. Australian sexually transmissible infection and HIV testing guidelines for asymptomatic men who have sex with men 2014: a review of the evidence. Sex Health. 2014;11(3):217–29.
STIs in Gay Men Action Group. Australian sexually transmitted infection and HIV testing guidelines 2019. Sydney, NSW: STIs in Gay Men Action Group; 2019.
Wright E, Grulich A, Roy K, et al. Australasian society for HIV, viral hepatitis and sexual health medicine HIV pre-exposure prophylaxis: clinical guidelines. J Virus Erad. 2017;3(3):168–84.
Australian Government Department of Health. Eighth national HIV strategy, 2018–2022. Canberra, ACT: Australian Government Department of Health; 2018.
Skarbinski J, Rosenberg E, Paz-Bailey G, et al. Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA Intern Med. 2015;175(4):588–96.
Prestage G, Brown G, Allan B, Ellard J, Down I. Impact of peer support on behavior change among newly diagnosed Australian gay men. J Acquir Immune Defic Syndr. 2016;72(5):565–71.
Khosropour CM, Dombrowski JC, Kerani RP, Katz DA, Barbee LA, Golden MR. Changes in condomless sex and serosorting among men who have sex with men after HIV diagnosis. J Acquir Immune Defic Syndr. 2016;73(4):475–81.
Gray RT, Wilson DP, Guy RJ, et al. Undiagnosed HIV infections among gay and bisexual men increasingly contribute to new infections in Australia. J Int AIDS Soc. 2018;21(4):e25104.
Holt M, Lea T, Mao L, et al. Community-level changes in condom use and uptake of HIV pre-exposure prophylaxis by gay and bisexual men in Melbourne and Sydney, Australia: results of repeated behavioural surveillance in 2013–17. Lancet HIV. 2018;5(8):e448–e556.
Hammoud MA, Vaccher S, Jin F, et al. HIV pre-exposure prophylaxis (PrEP) uptake among gay and bisexual men in Australia and factors associated with the non-use of PrEP among eligible men: results from a prospective cohort study. J Acquir Immune Defic Syndr. 2019;81(3):e73–e84.
Bourne C, Knight V, Guy R, Wand H, Lu H, McNulty A. Short message service reminder intervention doubles sexually transmitted infection/HIV re-testing rates among men who have sex with men. Sex Transm Infect. 2011;87(3):229–31.
Australian Government Department of Health and Ageing. National HIV testing policy v.10. Canberra, ACT: Australian Government Department of Health and Ageing; 2011.
Conway DP, Guy R, Davies SC, et al. Rapid HIV testing is highly acceptable and preferred among high-risk gay and bisexual men after implementation in Sydney sexual health clinics. PLoS ONE. 2015;10(4):e0123814.
Knight V, Ryder N, Guy R, Lu H, Wand H, McNulty A. New Xpress sexually transmissible infection screening clinic improves patient journey and clinic capacity at a large sexual health clinic. Sex Transm Dis. 2013;40(1):75–80.
Lee E, Mao L, Bavinton BR, Prestage G, Holt M. Which gay and bisexual men attend community-based HIV testing services in Australia? An analysis of cross-sectional national behavioural surveillance data. AIDS Behav. 2020;24:387–94.
Leitinger D, Ryan KE, Brown G, et al. Acceptability and HIV prevention benefits of a peer-based model of rapid point of care HIV testing for Australian gay, bisexual and other men who have sex with men. AIDS Behav. 2018;22:178–89.
Selvey LA, Slimings C, Adams E, Manuel J. Incidence and predictors of HIV, chlamydia and gonorrhoea among men who have sex with men attending a peer-based clinic. Sex Health. 2018;15(5):451–9.
Minas BC, Giele CM, Laing SC, et al. Early diagnosis of HIV among men who have sex with men in Western Australia: impact of a peer-led sexually transmissible infection testing service. Sex Health. 2015;12(4):360–3.
Barber L. Sydney gets rapid HIV testing clinic for Chinese-speaking gay and bi men. Star Observer. https://www.starobserver.com.au/news/national-news/new-south-wales-news/sydney-gets-rapid-hiv-testing-clinic-for-chinese-speaking-gay-and-bi-men/176553. Accessed 5 Feb 2019.
NSW Ministry of Health. NSW HIV strategy 2016–2020: quarter 4 and annual HIV data report 2018. Sydney, NSW: NSW Ministry of Health; 2019.
Pedrana A, Hellard M, Guy R, et al. Stop the drama Downunder: a social marketing campaign increases HIV/sexually transmitted infection knowledge and testing in Australian gay men. Sex Transm Dis. 2012;39(8):651–8.
Therapeutic Goods Association. Public Summary: Atomo Diagnostics Pty Ltd—Atomo HIV self test—HIV1/HIV2 antibody IVD, kit, immunochromatographic test (ICT), rapid Canberra, ACT: Therapeutic Goods Association, Australian Government Department of Health; 2018. https://www.ebs.tga.gov.au/servlet/xmlmillr6?dbid=ebs/PublicHTML/pdfStore.nsf&docid=5D22760703DE6366CA258353003CCFC1&agid=(PrintDetailsPublic)&actionid=1. Accessed 5 Feb 2019.
Holt M, Lea T, Mao L, et al. Adapting behavioural surveillance to antiretroviral-based HIV prevention: reviewing and anticipating trends in the Australian Gay Community Periodic Surveys. Sex Health. 2017;14(1):72–9.
Guy R, Goller J, Spelman T, et al. Does the frequency of HIV and STI testing among men who have sex with men in primary care adhere with Australian guidelines? Sex Transm Infect. 2010;86(5):371–6.
Wilkinson AL, El-Hayek C, Spelman T, et al. “Seek, test, treat” lessons from Australia: a study of HIV testing patterns from a cohort of men who have sex with men. J Acquir Immune Defic Syndr. 2015;69(4):460–5.
Wilkinson AL, El-Hayek C, Spelman T, et al. A ‘test and treat’ prevention strategy in Australia requires innovative HIV testing models: a cohort study of repeat testing among ‘high-risk’ men who have sex with men. Sex Transm Infect. 2016;92(6):464–6.
Zablotska IB, Kippax S, Grulich A, Holt M, Prestage G. Behavioural surveillance among gay men in Australia: methods, findings and policy implications for the prevention of HIV and other sexually transmissible infections. Sex Health. 2011;8(3):272–9.
Grulich AE, Guy R, Amin J, et al. Population-level effectiveness of rapid, targeted, high-coverage roll-out of HIV pre-exposure prophylaxis in men who have sex with men: the EPIC-NSW prospective cohort study. Lancet HIV. 2018;5(11):e629–e637637.
Witzel TC, Melendez-Torres G, Hickson F, Weatherburn P. HIV testing history and preferences for future tests among gay men, bisexual men and other MSM in England: results from a cross-sectional study. BMJ Open. 2016;6(9):e011372.
den Daas C, Doppen M, Schmidt AJ, de Coul EO. Determinants of never having tested for HIV among MSM in the Netherlands. BMJ Open. 2016;6(1):e009480.
Bavinton BR, Brown G, Hurley M, et al. Which gay men would increase their frequency of HIV testing with home self-testing? AIDS Behav. 2013;17(6):2084–92.
Callander D, Mooney-Somers J, Keen P, et al. Australian ‘gayborhoods’ and ‘lesborhoods’: A new method for estimating the number of adult gay men and lesbian women living in each Australian postcode. Int J Geogr Inf Sci. 2020. https://doi.org/10.1080/13658816.2019.1709973.
Ryan KE, Mak A, Stoove M, et al. Protocol for an HIV pre-exposure prophylaxis (PrEP) population level intervention study in Victoria Australia: the PrEPX study. Front Public Health. 2018;6:151.
Hoornenborg E, Krakower DS, Prins M, Mayer KH. Pre-exposure prophylaxis for men who have sex with men and transgender persons in early adopting countries: a narrative review. AIDS. 2017;31(16):2179–91.
Holt M, Lea T, Bear B, et al. Trends in attitudes to and the use of HIV pre-exposure prophylaxis by Australian gay and bisexual Men, 2011–2017: implications for further implementation from a diffusion of innovations perspective. AIDS Behav. 2019;23:1939–50.
Insight Start Study Group. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373(9):795–807.
Bavinton BR, Pinto AN, Phanuphak N, et al. Viral suppression and HIV transmission in homosexual male serodiscordant couples: an international, prospective, observational, cohort study. Lancet HIV. 2018;5(8):e438–e447447.
Keen P, Gray RT, Telfer B, et al. The 2016 HIV diagnosis and care cascade in New South Wales, Australia: Meeting the UNAIDS 90-90-90 targets. J Int AIDS Soc. 2018;21(4):e25109.
Institute K. HIV, viral hepatitis and sexually transmissible infections in Australia: annual surveillance report 2018. Sydney, NSW: Kirby Institute, UNSW; 2018.
Victorian Department of Health and Human Services. HIV quarterly surveillance report: April-June 2019. Melbourne, VIC: Victorian Department of Health and Human Services; 2019.
Queensland Department of Health. HIV in Queensland 2018. Brisbane, QLD: Communicable Diseases Branch, Queensland Department of Health; 2020.
Western Australia Department of Health. Quarterly surveillance report: notifiable sexually transmissible infections and blood-borne Viruses in Western Australia, period ending 30 September 2019. Perth, WA: Public Health and Clinical Services, Western Australia Department of Health; 2019.
Public Health England. HIV in the United Kingdom: towards zero HIV transmission by 2030–2019 report—data to end of December 2018. London: Public Health England; 2019.
San Francisco Department of Public Health. HIV epidemiology annual report 2018. San Francisco, USA: HIV Epidemiology Section, San Francisco Department of Public Health; 2019.
Public Health—Seattle & King County and the Washington State Department of Health. HIV/AIDS epidemiology report and community profile 2019, Volume 88. Seattle: Public Health—Seattle & King County and the Washington State Department of Health; 2019.
Ryan KE, Asselin J, Lal L, Nguyen L, et al. Results from a large Australian PrEP demonstration study: Discontinuation and subsequent HIV and other sexually transmitted infection risk. 10th International AIDS Society Conference on HIV Science. Mexico City, Mexico; 2019.
UNAIDS/WHO. Guidelines for second generation HIV surveillance. Geneva: UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance; 2000.
Grulich AE, de Visser RO, Badcock PB, et al. Homosexual experience and recent homosexual encounters: the Second Australian Study of Health and Relationships. Sex Health. 2014;11(5):439–50.
Acknowledgements
The Centre for Social Research in Health and The Kirby Institute receive funding from the Australian Government Department of Health and Ageing. The Gay Community Periodic Surveys are funded by state and territory health departments. BRB and AEG are supported by National Health and Medical Research Council (NHMRC) research fellowships.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bavinton, B.R., Grulich, A.E., Broady, T. et al. Increases in HIV Testing Frequency in Australian Gay and Bisexual Men are Concentrated Among PrEP Users: An Analysis of Australian Behavioural Surveillance Data, 2013–2018. AIDS Behav 24, 2691–2702 (2020). https://doi.org/10.1007/s10461-020-02826-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-020-02826-0