
Abstract
Despite the potential for sexual health communication to be leveraged for HIV prevention among youth experiencing homelessness (YEH), there has yet to be a rigorous examination of individual and network or relational characteristics associated with sexual health communication in this group of young people. Cross-sectional survey and social network data from 1014 YEH aged 14–25 recruited in Los Angeles, California, were utilized to assess individual and network or relational characteristics associated with communication regarding condom use and HIV testing among YEH. Results suggest that social networks are key to understanding sexual health communication; YEH’s engagement in sexual health communication was significantly related to the composition of their networks. To increase testing and decrease new HIV cases, a prudent strategy would be to train existing social network members (e.g., staff members, home-based peers, or partners) as agents of change in naturally occurring social networks of YEH.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
HIV Risk Behaviors Among Youth Experiencing Homelessness (YEH)
An estimated 1.3–1.7 million youth experience at least one night of homelessness each year [27]. These young people face numerous challenges and negative outcomes including poor physical, emotional, and sexual health [25, 35, 36]. In particular, research has documented higher rates of sexual health issues among youth experiencing homelessness (YEH) compared to their housed peers [7, 49]. An estimated 30–60% of female YEH, for example, have experienced a pregnancy, and 23–46% of YEH have had a sexually transmitted infection (e.g., chlamydia, gonorrhea [7, 25, 35, 41]. Notably, YEH are also 3–9 times more likely to acquire HIV than their housed peers [50]. Yet studies have suggested that YEH at the highest risk of HIV and STI may not undergo regular (or any) HIV testing, even though the Centers for Disease Control and Prevention recommends it as a primary strategy to prevent the spread of HIV [8]. Furthermore, studies have suggested that 40–70% of YEH engage in condomless sex [30]. Undoubtedly, effective HIV and sexual health protective strategies are critically needed to address these risk behaviors in this group of vulnerable young people.
Sexual Health: The Role of Social Network Relationships and Communication
Various studies have identified the noteworthy role of communication when it comes to safer sexual health practices among youth [56, 57]. A meta-analysis including more than 15,000 adolescents demonstrated a moderate effect size between communication and condom use, indicating that youth who engaged in sexual communication with their dating partners reported more condom use in their sexual encounters [57]. However, sexual health communication also occurred outside of partnered relationships, in other relationship types and the broader social network [56].
Social networks of YEH, in particular, are composed of relationships unique to their circumstances [3, 13, 44]. Social networks include partnered relationships and street-based peers (i.e., peers whom YEH met after becoming homeless); home-based peers (i.e., peers before YEH became homeless [44]; staff members from shelters and drop-in centers [3]; casual and serious partners [55]; parents [13]; and other relatives or family members [2]. These diverse sets of social network members (SNMs) are sources of communication, knowledge acquisition, and HIV risk behavior reinforcement [1]. However, the patterns and consequences of health communication may differ across SNMs. For example, a study by Craddock et al. [13] found that Black YEH who spoke with their parents about sex were 4 times more likely to get tested for HIV and almost 3 times more likely to use condoms. Likewise, another study found that talking to a sexual partner about condoms or safe-sex practices was associated with a greater likelihood of engaging in condomless sex [4], perhaps suggesting that not all communication is protective. Taken together, these studies reiterate the importance of understanding communication with a wide variety of SNMs.
Correlates of Sexual Health Communication: Key Individual and Network or Relational Factors
Although social networks are critical sources of communication regarding numerous issues, including sexual health topics [1], there is little research about the people with whom YEH communicate about sexual health topics or the individual and social network or relational factors associated with such communication. Individual factors refer to the characteristics of the participant (e.g., age, gender, behaviors, etc.), whereas network or relational characteristics refer to the nature of relationships between participants and their SNMs (e.g., relationship type, quality, and duration [19]. Understanding the role of individual and network or relational characteristics in sexual health communication about condom use and HIV testing may provide significant information for designing and disseminating more effective HIV preventive interventions. For example, in designing sexual health campaigns, targeted messaging strategies (i.e., audience segmentation) have to be developed for different audiences based on their needs, attitudes, social norms, and knowledge regarding the behavior [28]. YEH are not a homogeneous group and interventions are likely to be more effective if they reflect this group’s heterogeneity. Similarly, in disseminating sexual health interventions, it is very important to determine which channels increase the efficiency of information dissemination [52]. Especially regarding interpersonal communication about sexual health, it has been noted that the messenger is as important as the message. Therefore, knowing the people with whom YEH discussed sexual health topics can inform message delivery strategies.
No study to our knowledge has investigated the relationship between individual characteristics and communication about condom use and HIV testing among YEH. However, studies conducted with housed young people helped provide a framework for the current investigation. For instance, a study conducted with a nationally representative sample of housed adolescents found that youth who were older, had more years of education, or had parents who were better educated were more likely to report engaging in sexual health communication [26]. Similarly, studies have found that substance use can negatively affect sexual communication [17, 58]. Gender has also been linked to sexual health communication, with women being more likely than men to engage in sexual health communication [53]. Taken together, these studies indicate that demographic and behavioral correlates are important in understanding variance in sexual health communication and need to be better understood in the context of sexual health communication among YEH.
Relatedly, research addressing how network or relational factors contribute to sexual health communication among both housed youth and YEH is lacking. Because communication is naturally a relational or network phenomenon [43], it is important to understand how network structure and relationships influence sexual health communication. For example, networks shape the size and composition of groups and limit the people with whom youth communicate about sexual health topics. As previously mentioned, social networks of YEH are composed of members specific to YEH such as staff members, street peers, home peers, serious partners, causal partners, and relatives [55]. No study to date has examined how the composition of these networks affects sexual health communication patterns among YEH. Knowing with whom youth speak about sexual health topics might help us design interpersonal communication strategies that can leverage these naturally occurring networks. For instance, if we find that YEH are communicating with their partners about sexual health topics, it would be prudent to tailor interventions to focus on educating these young people on the most effective means of having these conversations with their partners. This is especially important because previous research [23] has found differentials in gender-based norms and power surrounding sexual decision-making, with women more likely to capitulate to their male partners. Therefore, engaging these young people around issues of empowerment and effective strategies for negotiating safer sex could improve sexual health.
Social network analysis, in particular, allows us to consider relationship quality by assessing relationship characteristics such as homophily and length of relationship. Homophily is the tendency of people to bond and associate with others who are similar in behaviors, beliefs, and attitudes [34]. Research has suggested that homophily may facilitate communication because of shared identity and interests [18], and therefore might influence sexual health communication. For example, studies have demonstrated that women are likely to talk to other women about sexual health topics [6, 21]. Similarly, studies have found that sexual identity plays a critical role in how people form friendships and whether sexual topics are discussed [32]. Extant research has also indicated that HIV prevention programs with more homophilous participants tend to be more effective that programs with less homophilous participants [14]. In the context of sexual health communication among YEH, we don’t yet know if homophily drives discussions about sexual health topics. Additionally, as noted, because different homophilous characteristics (e.g., gender, sexual identity, race, etc.) can drive sexual health communication, it is also important to investigate which of these dimensions is most important in understanding sexual health communication.
Also, relationships characterized by longevity are a key indicator of the strength of ties [24]. Individuals in strong relationships are more likely to exchange information of depth and richness [29]. Indeed, one study [47] found that length of time in a relationship was associated with sexual communication among women, but not men. Knowing which aspects of relationship quality influence whether YEH broach sexual health topics could indicate important entry points in HIV preventive and sexual risk-reduction interventions.
Current Study
To date, most studies have only considered the relationship between sexual health communication and sexual or HIV risk; this study responded to a call by Valente and Fosados [52] to investigate network mechanisms through which interpersonal communication about health issues are shared and received. Understanding with whom YEH discuss sexual health issues and the individual and network factors associated with such communication is important for the development of health promotion and risk reduction models for this population. Accordingly, this study’s primary aims were to investigate individual and network or relational characteristics associated with communication regarding condoms and HIV testing among participants to inform social network-based HIV interventions geared toward YEH.
Methods
Four waves of cross-sectional data were collected from YEH aged 14–25 at three drop-in centers in Los Angeles, California, between October 2011 and June 2013. All youths accessing services at these agencies during the data collection period were invited to participate. Informed consent was obtained from youths aged 18 or older, and informed assent was obtained from youths aged 14–17 years old. The institutional review board of University of Southern California approved all survey items and procedures and waived parental consent because homeless youths younger than 18 are unaccompanied minors. Participants received $20 in cash or gift cards as compensation for their time.
All surveys were conducted in a private space at the agency. The survey consisted of two distinct parts: (a) an audio computer-assisted self-interview (ACASI) and (b) a face-to-face social network interview (F2F-SNI).
ACASI allows participants to enter answers to questions privately into a computer as they read questions silently on the computer screen, listen to the questions being read to them through headphones, or both. After responses are entered, the computer selects the next questions to be answered based on preprogrammed skip patterns. ACASI reduces nonresponse rates to sensitive questions about potentially socially undesirable activities, such as sexual behaviors, illicit substance use behaviors, and criminal activity [20, 38].
The F2F-SNI [42] was designed to elicit information about the participants’ social networks. In this format, the participants were asked to visualize their personal networks on a specialized iPad app, which consisted of participants clicking circles on the screen, with one circle representing the respondent and lines connecting to other circles that represented their network alters. The visual stimulus provided by the F2F-SNI has been shown to enhance the respondent’s ability to focus on providing a large quantity of social network data while simultaneously reducing participant burden [42, 44]. Additionally, the current study employed multiple elicitation questions in the social network interview to prevent recall bias.
During the F2F-SNI exercise, youths were asked to name every person with whom they interacted—known in social network terminology as alters—during the previous month. The following prompt was first read: “Think about the last month. Who have you interacted with? These can be people you interacted with in person, on the phone, or through the Internet.” After youth stopped nominating social connections, an additional 15 prompts to solicit nominees were read, as follows: “These might be friends; family; people you hang out with/chill with/kick it with/have conversations with; people you party with—use drugs or alcohol with; boyfriend/girlfriend; people you are having sex with; baby mama/baby daddy; case worker; people from school; people from work; old friends from home; people you talk to, on the phone or by email; people from where you are staying/squatting with; people you see at this agency; and other people you know from the street.” The interviewer then asked questions regarding the characteristics of each alter (SNM). Questions sought each alter’s first and last name, nickname or street name, age, race, gender, length known (i.e., how many days and years the respondent had known the alter), and if the alter was a family member, peer, sex partner, etc. After the attributes of each alter were coded, questions regarding the participant’s perceptions of each alter’s behaviors, including drug and sex behaviors, were asked.
This analysis included data from 1014 homeless youths aged 14–25 years who completed both the social network interview and survey questionnaire.
Primary Outcome Variables
Sexual Health Communication
There were two sexual health communication questions. To assess communication about condom use, participants were asked, “Have you talked about condoms, or practicing safer sex in the past 30 days?” To assess communication about HIV testing, they were asked, “Have you talked about getting an HIV test in the past 30 days?” Responses were dichotomized (1 = yes, 0 = no).
Demographic Characteristics
Demographic variables included age; gender (male vs. female); race (White, Latinx, mixed race, and other [i.e., Asian, Native Hawaiian, Pacific Islander, Native American, or Alaska Native] vs. Black); and sexual orientation (heterosexual vs. lesbian, gay, bisexual, or queer). Youths experiencing literal homelessness were defined as those who indicated that they were currently staying in a shelter (i.e., emergency or temporary), a stranger’s home, hotel, motel, street, beach, tent or campsite, abandoned building, car, or bus vs. those living with their biological family, foster family, relative, friend, group home, sober-living facility, transitional-living program, or own apartment but still spending considerable time on the streets.
Behavioral Characteristics
Drug use variables were dichotomized and assessed recent use (during the prior 30 days) of methamphetamine, cocaine, injection drugs, and heroin. Response options were “1 or more times” (coded as 1) or “0 times” (coded as 0).
Sexual behavior variables assessed sex with condoms (condom use during last sexual encounter), concurrent sex (sex with more than one partner in 1 week period), exchange sex (exchanged sex for money, drugs, a place to stay, food or meals, or anything else), and recent HIV test (during the past 3 months). Responses were dichotomized (1 = yes, 0 = no).
SNM Characteristics
SNM variables assessed relationship quality (years known; 1 = 2 or more vs. 0 = less than 2 years) and relationship type (relative, staff member, serious partner, and casual partner; 1 = yes, 0 = no). To assess relationship types, participants were asked the following questions about each SNM: “Who is a relative?” “Who is a case worker or agency staff member or volunteer?” “Who is a sexual partner?” and “Who is a serious partner?” Participants were allowed to make selections for each question if it applied to that SNM. The home-based peer variable was created by asking, “Who did you know from home, before you became homeless?” and “Who would you call a friend?” If SNMs were nominated as someone youth knew from home and as a friend, they were considered a home-based peer. If youth nominated an SNM as a friend whom they met when they were homeless, the SNM was considered a street-based peer. Frequencies were run and variables were recoded to ensure each variable relationship type was mutually exclusive (1 = yes, 0 = no).
Homophily was dichotomized and defined as identifying as the same gender (gender homophily), same race (race homophily), or same sexual orientation (sexual orientation homophily) regarding each SNM (1 = yes, 0 = no).
Data Analyses
Statistical analyses proceeded in two stages: (a) calculation of descriptive statistics to assess demographic, behavioral, and network-related characteristics in our sample; and (b) multilevel modeling (hierarchical linear modeling) to understand how individual characteristics (e.g., age, race, drug use, and sexual risk behaviors) and SNM characteristics (i.e., years known, gender homophily, sexual orientation homophily, and network relationship type) were associated with the two kinds of sexual health communication (i.e., condom use and HIV testing).
Multivariable multilevel logistic regression models were utilized to assess correlates of sexual health communication. Multilevel logistic regression models are used to analyze variance in outcomes when data are nested (e.g., predictor variables are at a different hierarchical level [54]. In this case, members of each YEH network share variances according to the YEH with whom they are associated. The two communication outcomes were treated as dichotomous outcomes and regressed on social network-level measures (i.e., measures that varied across SNMs) and individual-level measures (i.e., measures that only varied across participants). Individual-level measures were created based on standard individual responses to survey items.
All multivariable multilevel logistic regression analyses were restricted to participants without missing data for the variables included in the models. Therefore, the sample sizes for the multivariable multilevel logistic regression models (i.e., communication about condom use or HIV testing) are smaller than the study’s total sample size. Although HIV status was not examined in the analyses, it should be noted that 2% of the participants (n = 20) identified as testing positive for HIV. All analyses were carried out in SAS version 9.4. Random-intercept logistic regressions were fitted using PROC GLIMMIX.
Results
Descriptive Statistics of Participants
Individual-level descriptive statistics are presented in Table 1. Average age for youth in this sample was 21.28 (range 14–25, SD 2.06). The majority of youth identified as White (38%), followed by Black (24%), mixed race (19%), Latinx (13%), and other (4%). Approximately 34% of the youth reported experiencing literal homelessness. Approximately three quarters of youth identified as heterosexual (76%) and male (73%). Regarding drug use, meth was reported to be the most commonly used substance (25%), followed by cocaine (16%), heroin (11%), and injection drugs (11%). Regarding sexual risk behaviors, 47% of youth had used a condom during their last sexual encounter, 37% had concurrent sexual partners, 17% reported ever participating in exchange sex, and 48% had a recent HIV test (i.e., in the last 3 months). As for sexual health communication, 28% of youth reported communicating about condom use and 24% reported communicating about testing for HIV.
Descriptive Statistics of Social Networks
Social network descriptive statistics are presented in Table 2. A total of 9981 SNMs were nominated, with youth nominating an average of 9.13 SNMs each. Forty-seven percent of youth reported knowing their network members for more than 2 years. Seventy-four percent of SNMs nominated were of the same sexual orientation, 56% were of the same gender and 57% were of the same race as the nominating youth. Regarding relationship type, the majority of youth listed street-based peers (32%), followed by relatives (20%), home-based peers (12%), serious partners (6%), and casual partners (4%).
Multilevel Multivariable Model of Communication About Condoms
Table 3 presents results from the multilevel multivariable model assessing communication about condoms. Regarding demographic and behavioral characteristics, race, homelessness type, and condom use at last sexual encounter were significant correlates of communication regarding condoms. Specifically, White identified youth had 61% decreased odds of talking about condom use with SNMs (OR 0.39; 95% CI 0.18, 0.82) compared to youth who identified as Black. Youth who reported literal homelessness had nearly 3 times the odds of talking about condom use with SNMs (OR 2.88; 95% CI 1.54, 5.38). Additionally, youth who reported meth use had decreased odds of talking about condom use with SNMs (OR 0.47; 95% CI 0.23, 0.97) compared to those who did not report meth use. Furthermore, youth who reported condom use at last sex had nearly 3 times the odds of talking with SNMs about condoms (OR 2.59; 95% CI 1.46, 4.61) than youth who did not report condom use at last sex, and youth who reported ever participating in exchange sex had more than 2 times the odds of reporting talking about condoms with SNMs (OR 2.29; 95% CI 1.05, 5.00) compared to youth who did not report participating in exchange sex.
Regarding network-level findings, several relationship types were significantly associated with communication about condoms. Youth had 68% increased odds of talking with SNMs whom they had known for 2 or more years about condom use (OR 1.68; 95% CI 1.20, 2.17), and 26% increased odds of communicating about condom use with SNMs who were homophilous in gender (OR 1.26; 95% CI 1.03, 1.55). Youth had almost 22 times the odds of communicating about condom use with their serious partners (OR 21.82; 95% CI 14.91, 31.92), and 9 times the odds of communicating about condoms with their casual partners (OR 8.85; 95% CI 5.62, 13.94) compared to their street-based peers. Findings indicated that youth had about 4 times the odds of talking to home-based peers about condoms (OR 4.33; 95% CI 3.09, 6.08) and 3 times the odds of talking with relatives about condom use (OR 3.26; 95% CI 2.40, 4.43) compared to street-based peers.
Multilevel Multivariable Model of Communication About HIV Testing
Findings from the multivariable model assessing communication about HIV testing are also presented in Table 3. Regarding demographic and behavioral characteristics, our findings indicated that White-identifying youth had decreased odds of talking about HIV testing with SNMs (OR 0.31; 95% CI 0.15, 0.65) compared to Black youth and if YEH were recently tested for HIV (OR 0.13; 95% CI 0.06, 0.28), whereas they had increased odds of talking with SNMs about HIV testing if they reported literal homelessness (OR 2.32; 95% CI 1.26, 4.25).
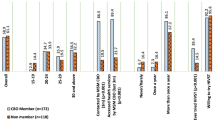
Among network-level variables, youth had 22 times the odds of talking about HIV testing with a serious partner (OR 21.58; 95% CI 14.71, 31.65); 5 times the odds of talking about HIV testing with a staff member (OR 4.85; 95% CI 3.17, 7.40); and 4 times odds of reporting communicating about HIV testing with a casual partner (OR 4.27; 95% CI 2.67, 6.81) compared to street-based peers. Results indicated that youth had nearly 4 times the odds of talking with their home-based peers about HIV testing (OR 3.51; 95% CI 2.45, 5.01) and had 66% increased odds of talking with their relatives about HIV testing (OR 1.66; 95% CI 1.20, 2.30) compared to street-based peers.
Discussion
To the best of our knowledge, this was the first study to investigate demographic, behavioral, and social network or relational factors associated with communication regarding condom use and HIV testing among YEH. Our findings indicate that these factors are key to understanding communication about these topics and have important implications for how interventions are designed.
We found that a little more than a quarter of the youth (28%) sampled in this study indicated talking about condom use; a lower proportion of youth (24%) reported having a conversation regarding HIV testing. These low rates should be concerning and indicate that sexual health communication is an issue that requires urgent attention in this group of youth. Previous studies have shown that communicating about sexual health can be a protective factor regarding unwanted pregnancies, sexually transmitted infections, and HIV [56, 57]. Although it is difficult to discern from our data why such sexual health communication patterns exist, studies conducted with housed youth have identified many barriers to sexual health communication, including discomfort or stigma surrounding conversations focused on sexual topics [5, 37, 33] and lack of access to reproductive health services [16].
Composition of networks was critical to understanding patterns of sexual health communication among our participants. Three SNM relationship types in particular were key in understanding youths’ communication about both condom use and HIV testing: serious partners, casual partners, and home-based peers. Youth were significantly more likely to talk about condom use and HIV testing with serious partners or casual partners in their networks compared to their street-based peers. This finding is promising, because more than 90% of newly diagnosed HIV infections are attributed to sexual contact [9]. Although communicating about condom use and HIV testing with a serious or casual partner does not imply that these youth are implementing the behavior (i.e., using condoms or getting tested for HIV), previous research has indicated that talking about these actions and knowledge of preventive behaviors may lead to higher rates of preventive behavior implementation [3, 13, 51, 56, 57]. These results indicate the potential to harness sexual health communication relationships with current partners for sexual or social network-based HIV preventive interventions geared toward YEH. However, further examination is needed to understand the context in which these conversations are occurring and the types of information that is being shared between YEH and their partners to better determine what is needed to increase effectiveness of HIV interventions designed for YEH (e.g., communication self-efficacy, clear and assertive communication strategies).
Youth were significantly more likely to talk about condom use and HIV testing with home-based peers than street-based peers. This is surprising considering that street-based peers made up 32% of all SNMs, whereas home-based peers only made up about 12% of all SNMs. These results suggest that youth may have stronger relationships with their home-based peers and are perhaps more comfortable talking about highly sensitive topics such as sexual health with peers they knew before becoming homeless (i.e., home-based peers). Indeed, studies have found that YEH are increasingly using social media or other technologies (e.g., cell phones) to communicate with home-based peers about sexual health topics, even when they might be geographically distant [45]. Street-based peers, on the other hand, are typically local and more often a source of instrumental support—providing protection or access to resources needed while on the street, instead of informational and emotional support [31, 48]. These results highlight the importance of differentiating home-based peers from street-based peers when examining peer networks of YEH and developing peer-based HIV interventions. Additionally, this suggests that home-based peers might be more salient intervention agents in the context of sexual health communication campaigns relative to other network members.
Not surprisingly, our findings indicate that youth who reported having a staff member in their network were more likely to report talking about HIV testing. Drop-in centers in Los Angeles have HIV testing available to youth and offer a monetary incentive for being tested. Because of these reasons, staff members often encourage youth at drop-in centers to be tested, perhaps partly explaining this association. Although this finding is promising, our study also indicates that very few YEH (less than 6%) nominated a staff member in their network. Future interventions, therefore, would be well served by increasing agency outreach to YEH to ensure they have more opportunities to communicate with staff members, who can inform them of these accessible and free testing opportunities.
In addition to network composition, relationship quality was also significantly associated with communication about condoms and safe sex. Youth were significantly more likely to talk with SNMs they had known for 2 years or more about condom use. As noted, this is probably a reflection of the stronger relationships that youth have with people they have known longer. It is therefore important that YEH have more opportunities to engage with people whom they can trust and communicate with about such sensitive topics.
Youth who identified as White were significantly less likely to talk about both condom use and HIV testing compared to Black youth. This may be due to a perceived low risk of contracting HIV [46] induced by a high representation of HIV campaign ads featuring Black and sexual minority community members [10, 15]. Although these communities may have higher rates of HIV [11], targeted campaigns may be sending an unintended message to White heterosexual-identifying youth, including those experiencing homelessness, that they are not at risk of HIV. Santa Maria et al. [46] found in their study examining HIV risk perceptions among homeless adults that 61% of White homeless adults felt they were at low risk of HIV, which was significantly higher than homeless adults who identified as a minority race. This perceived low risk and the lack of communication regarding HIV risk behaviors can set the stage for a possible HIV outbreak in the networks of these White youth, similar to those found in Indiana [12] and Seattle [22]. However, because there is very little research examining perceived HIV risk among White YEH or YEH in general, qualitative research should be conducted with YEH from various racial backgrounds to determine any cultural differences regarding HIV risk perceptions and factors associated with risk perceptions of YEH.
Youth who reported having sex with a condom during their last sexual encounter were significantly more likely to talk about condom use with their SNMs. This is a promising finding, meaning that youth who are using condoms are talking about it. However, because this was a cross-sectional study, we could not determine causality. Therefore, we cannot imply that communication about condom use in this study led to condom use. Also notable is the higher proportion of condom use (47%) compared to communication about condom use (28%) among these YEH. The lower frequency of communication about condom use compared to condom use during last sex may be due to temporal ordering of the variables. Our communication variables were based on the past 30 days; however, it is possible that some youths’ last sexual encounter occurred beyond the last 30 days or it may indicate that youth have been having sex with the same sexual partner for longer than 30 days. Thus, once they make decisions about condom use with their sexual partners, condom use conversations dissipate, hence the lower frequency of communication about condom use. Nevertheless, our findings highlight that if YEH are using condoms, they are more likely to talk about condom use, thus bolstering the case for sexual health communication campaigns.
An encouraging finding is that youth experiencing literal homelessness were more likely to talk about condom use and HIV testing compared to youth not experiencing literal homelessness. This may indicate that either YEH or their SNMs recognize that YEH are at increased risk of HIV, and thus they are communicating about these HIV prevention topics. However, this also indicates that YEH who do not identify as literally homeless may not be talking about these topics to the same extent as youth who are experiencing literal homelessness. Although there is no clear explanation for this observation, it may be that YEH who are spending more time on the streets (i.e., literally homeless) do not experience as much pressure to curtail conversations about HIV prevention topics. In essence, YEH who do and do not identify as literally homeless may simply find themselves navigating environments with different communication norms and may perceive different risks for violating such norms.
A surprising finding in our data is that YEH who were recently tested for HIV were significantly less likely to talk about HIV testing. This may be explained using two distinctive perspectives. HIV and HIV-related behaviors are very stigmatized, so people may not want to discuss their testing history with their SNMs [40], particularly if they felt they would be judged based on the perception that they engaged in risky behaviors. This perception of not being “clean” may also prevent YEH from having conversations with SNMs about HIV testing. An alternative explanation could be the temporal ordering of the variables. Our communication variables were based on the past 30 days, whereas HIV testing was based on the past 3 months. Therefore, it is possible that YEH who had been tested 3 months prior to data collection were not having conversations about HIV testing when they were responding to the communication questions in our study. Because we do not know the context of these conversations, we cannot determine whether any of these explanations accurately explicate our findings. Future studies should examine the context surrounding communication about HIV testing and testing behaviors in social networks of youth who have experienced homelessness.
Limitations
Because this study was one of the first to investigate in detail the network mechanisms through which interpersonal communication about health issues are shared and received, there are some limitations to this analysis. The study took place at three drop-in centers in Los Angeles County, restricting generalizability to YEH who live in other areas. Moreover, the cross-sectional nature of the data prohibited forming causal arguments. Regarding communication, the quality, tone, and overall content of the conversations are unknown; we are unsure of who initiated these conversations and the means used to have these conversations; and because these are perceptual data, we have no way of knowing whether these conversations happened. Future studies should examine if these conversations are taking place and should take a comprehensive look at the context of homeless youths’ conversations regarding sexual health with their SNMs and the means used to have these conversations. Additionally, because both the social network and survey data were self-reported and used a 30-day recall period, there is potential for recall bias, which could have affected the accuracy of their responses. However, a recent meta-analysis found that shorter time periods produce more reliable recall [39]. Additionally, the current study employed multiple elicitation questions in the social network interview to prevent recall bias. Although network composition was found to be an important factor for condom use and HIV testing communication, the interaction of YEH’s race and their social network composition was not considered. Future studies should consider the associations of YEH’s race and their social network composition (e.g., how many peers vs. relatives in their network) and whom YEH speak with about sexual health topics to gain an understanding of how YEH sexual health communication may differ based on social network composition and dynamics.
Conclusion
Understanding sexual health communication is important in the development of health promotion and risk reduction models for YEH. Our results offered some promising findings. Youth were significantly more likely to talk about condom use and HIV testing if they listed at least one serious partner or casual partner, youth who used condoms were talking about condom use, and youth who were connected to staff members were conversing about HIV testing. However, there is much room for improvement regarding HIV prevention efforts in social networks of YEH. To decrease the incidence of new HIV cases and increase testing, we should further examine how to train preexisting SNMs (e.g., staff members, home-based peers, or partners) as agents of change. By increasing communication about HIV protective behaviors (e.g., condom use and HIV testing) in social networks of youth who are homeless, we may see changes in behaviors disseminated through the networks of these youth.
References
Bandura A. On integrating social cognitive and social diffusion theories. Commun Innov. 2006. https://doi.org/10.4135/9788132113775.n5.
Barman-Adhikari A, Bowen E, Bender K, Brown S, Rice E. A social capital approach to identifying correlates of perceived social support among homeless youth. Child Youth Care Forum. 2016;45(5):691–708. https://doi.org/10.1007/s10566-016-9352-3.
Barman-Adhikari A, Craddock J, Bowen E, Das R, Rice E. The relative influence of injunctive and descriptive social norms on methamphetamine, heroin, and injection drug use among homeless youths: the impact of different referent groups. J Drug Issues. 2018;48(1):17–35. https://doi.org/10.1177/0022042617726080.
Barman-Adhikari A, Hsu HT, Begun S, Portillo AP, Rice E. Condomless sex among homeless youth: the role of multidimensional social norms and gender. AIDS Behav. 2017;21(3):688–702. https://doi.org/10.1007/s10461-016-1624-2.
Barth KR, Cook RL, Downs JS, Switzer GE, Fischhoff B. Social stigma and negative consequences: factors that influence college students’ decisions to seek testing for sexually transmitted infections. J Am Coll Health. 2002;50:153–9. https://doi.org/10.1080/07448480209596021.
Becker S. Couples and reproductive health: a review of couple studies. Stud Family Plan. 1996;27(6):291–306.
Begun S. The paradox of homeless youth pregnancy: a review of challenges and opportunities. Soc Work Health Care. 2015;54:444–60. https://doi.org/10.1080/00981389.2015.1030058.
Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB, Clark JE. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. Morb Mortal Wkly Rep. 2006;55(14):1–17.
Centers for Disease Control and Prevention. HIV surveillance report, 2016 ed., vol. 28. Retrieved from http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. 2017.
Centers for Disease Control and Prevention. Effective interventions: HIV prevention that works. Retrieved from https://effectiveinterventions.cdc.gov/docs/default-source/general-docs/16-0817-hip-overview-factsheet.pdf?sfvrsn=4. 2016.
Centers for Disease Control and Prevention. HIV in the United States and dependent areas. Retrieved from: https://www.cdc.gov/hiv/pdf/statistics/overview/cdc-hiv-us-ataglance.pdf. 2019.
Conrad C, Bradley HM, Broz D, Buddha S, Chapman EL, Galang RR, et al. Community outbreak of HIV infection linked to injection drug use of oxymorphone—Indiana, 2015. MMWR Morb Mortal Wkly Rep. 2015;64(16):443.
Craddock JB, Rice E, Rhoades H, Winetrobe H. Are parental relationships always protective? A social network analysis of Black, Latino, and White homeless youth and sexual risk-taking behaviors. Prev Sci. 2016. https://doi.org/10.1007/s11121-016-0684-x.
Dearing JW, Rogers EM, Meyer G, Casey MK, Rao N, Campo S, Henderson GM. Social marketing and diffusion-based strategies for communicating with unique populations: HIV prevention in San Francisco. J Health Commun. 1996;1(4):343–63.
Drumhiller K, Murray A, Gaul Z, Aholou TM, Sutton MY, Nanin J. “We Deserve Better!”: perceptions of HIV testing campaigns Among Black and Latino MSM in New York City. Arch Sex Behav. 2018;47(1):289–97.
Fothergill K, Feijoo A. Family planning services at school-based health centers: findings from a national survey. J Adolesc Health. 2000;27:166–9. https://doi.org/10.1016/S1054-139X(00)00122-1.
Freimuth VS, Hammond SL, Edgar T, McDonald DA, Fink EL. Factors explaining intent, discussion and use of condoms in first-time sexual encounters. Health Educ Res. 1992;7(2):203–15. https://doi.org/10.1093/her/7.2.203.
Fulginiti A, Pahwa R, Frey LM, Rice E, Brekke JS. What factors influence the decision to share suicidal thoughts? A multilevel social network analysis of disclosure among individuals with serious mental illness. Suicide Life-Threat Behav. 2016;46(4):398–412.
Fulginiti A, Rice E, Hsu HT, Rhoades H, Winetrobe H. Risky integration: a social network analysis of network position, exposure, and suicidal ideation among homeless youth. Crisis. 2016;37(3):184. https://doi.org/10.1027/0227-5910/a000374.
Ghanem KG, Hutton HE, Zenilman JM, Zimba R, Erbelding EJ. Audio computer assisted self-interview and face to face interview modes in assessing response bias among STD clinic patients. Sex Transm Infect. 2005;81(5):421–5.
Gillespie BJ, Frederick D, Harari L, Grov C. Homophily, close friendship, and life satisfaction among gay, lesbian, heterosexual, and bisexual men and women. PLoS ONE. 2015;10(6):e0128900.
Golden MR, Lechtenberg R, Glick SN, Dombrowski J, Duchin J, Reuer JR, et al. Outbreak of human immunodeficiency virus infection among heterosexual persons who are living homeless and inject drugs—Seattle, Washington, 2018. Morb Mortal Wkly Rep. 2019;68(15):344.
Gómez CA, Marin BV. Gender, culture, and power: barriers to HIV-prevention strategies for women. J Sex Res. 1996;33(4):355–62.
Granovetter M. The strength of weak ties: a network theory revisited. Sociol Theory. 1983. https://doi.org/10.2307/202051.
Halcón LL, Lifson AR. Prevalence and predictors of sexual risks among homeless youth. J Youth Adolesc. 2004;33:71–80. https://doi.org/10.1023/A:1027338514930.
Hall KS, Moreau C, Trussell J. Determinants of and disparities in reproductive health service use among adolescent and young adult women in the United States, 2002–2008. Am J Public Health. 2012;102(2):359–67. https://doi.org/10.2105/AJPH.2011.300380.
Hammer H, Finkelhor D, Sedlak AJ. Runaway/thrownaway children: National estimates and characteristics (NCJ Publication No. 196469). Retrieved from https://www.ncjrs.gov/pdffiles1/ojjdp/196469.pdf. 2002.
Hawkins RP, Kreuter M, Resnicow K, Fishbein M, Dijkstra A. Understanding tailoring in communicating about health. Health Educ Res. 2008;23(3):454–66.
Jha Y, Welch E. The relationship between multiplexity and academic productivity in six fields of science and engineering. Georgia Institute of Technology. 2009.
Kennedy DP, Tucker JS, Green HD Jr, Golinelli D, Ewing B. Unprotected sex of homeless youth: results from a multilevel analysis of individual, social network, and relationship factors. AIDS Behav. 2012;16:2015–32. https://doi.org/10.1007/s10461-012-0195-0.
Kennedy MC, Jansson M, Benoit C, Magnuson D, Scramstad J, Hallgrimsdottir H. Social relationships and social support among street-involved youth. J Youth Stud. 2017;20:1328–45. https://doi.org/10.1080/13676261.2017.1333582.
Logan JD. Applied mathematics. Hoboken: Wiley; 2013.
Mathur S, Mullinax M, Santelli JS. Prevention of sexually transmitted infections among adolescents. International handbook on adolescent health and development. Cham: Springer; 2017. p. 183–205.
McPherson M, Smith-Lovin L, Cook JM. Birds of a feather: homophily in social networks. Ann Rev Sociol. 2001;27(1):415–44.
Milburn NG, Batterham P, Ayala G, Rice E, Solorio R, Desmond K, et al. Discrimination and mental health problems among homeless minority young people. Public Health Rep. 2010;125(1):61–7.
Molino AC. Characteristics of help-seeking street youth and non-street youth. In: Paper presented at the 2007 National Symposium on Homelessness Research, Chicago, IL. Retrieved from https://aspe.hhs.gov/system/files/pdf/180451/report.pdf. (2007).
Morris JL, Lippman SA, Philip S, Bernstein K, Neilands TB, Lightfoot M. Sexually transmitted infection related stigma and shame among African American male youth: implications for testing practices, partner notification, and treatment. AIDS Patient Care STDs. 2014;28:499–506. https://doi.org/10.1089/apc.2013.0316.
Morrison-Beedy D, Carey MP, Tu X. Accuracy of audio computer-assisted self-interviewing (ACASI) and self-administered questionnaires for the assessment of sexual behavior. AIDS Behav. 2006;10(5):541–52.
Napper LE, Fisher DG, Reynolds GL, Johnson ME. HIV risk behavior self-report reliability at different recall periods. AIDS Behav. 2010;14(1):152–61.
Prestage G, Mao L, McGuigan D, Crawford J, Kippax S, Kaldor J, Grulich AE. HIV risk and communication between regular partners in a cohort of HIV-negative gay men. AIDS Care. 2006;18(2):166–72.
Rew L. Sexual health practices of homeless youth: a model for intervention. Issues Compr Pediatric Nurs. 2001;24:1–18. https://doi.org/10.1080/119-01460860151062424.
Rice E, Barman-Adhikari A, Milburn NG, Monro W. Position-specific HIV risk in a large network of homeless youths. Am J Public Health. 2012;102(1):141–7. https://doi.org/10.2105/AJPH.2011.300295.
Rice E, Comulada S, Green S, Arnold EM, Rotheram-Borus MJ. Differential disclosure across social network ties among women living with HIV. AIDS Behav. 2009;13:1253–61. https://doi.org/10.1007/s10461-009-9554-x.
Rice E, Kurzban S, Ray D. Homeless but connected: the role of heterogeneous social network ties and social networking technology in the mental health outcomes of street-living adolescents. Community Ment Health J. 2012;48(6):692–8. https://doi.org/10.1007/s10597-011-9462-1.
Rice E, Lee A, Taitt S. Cell phone use among homeless youth: potential for new health interventions and research. J Urban Health. 2011;88:1175–82. https://doi.org/10.1007/s11524-011-9624-z.
Santa Maria D, Hernandez D, Arlinghaus K, Gallardo K, Maness S, Kendzor D, et al. Current age, age at first sex, age at first homelessness, and HIV risk perceptions predict sexual risk behaviors among sexually active homeless adults. Int J Environ Res Public Health. 2018;15(2):218.
Saul J, Norris FH, Bartholow KK, Dixon D, Peters M, Moore J. Heterosexual risk for HIV among Puerto Rican women: does power influence self-protective behavior? AIDS Behav. 2000;4(4):361–71. https://doi.org/10.1023/A:1026402522828.
Smith H. Searching for kinship: the creation of street families among homeless youth. Am Behav Sci. 2008;51:756–71. https://doi.org/10.1177/0002764207311986.
Solorio MR, Rosenthal D, Milburn NG, Weiss RE, Batterham PJ, Gandara M, Rotheram-Borus MJ. Predictors of sexual risk behaviors among newly homeless youth: a longitudinal study. J Adolesc Health. 2008;42:401–9. https://doi.org/10.1016/j.jadohealth.2007.09.023.
Tevendale HD, Lightfoot M, Slocum SL. Individual and environmental protective factors for risky sexual behavior among homeless youth: an exploration of gender differences. AIDS Behav. 2009;13:154–64. https://doi.org/10.1007/s10461-008-9395-z.
Tyler KA. Homeless youths’ HIV risk behaviors with strangers: investigating the importance of social networks. Arch Sex Behav. 2013;42(8):1583–91. https://doi.org/10.1007/s10508-013-0091-3.
Valente TW, Fosados R. Diffusion of innovations and network segmentation: the part played by people in promoting health. Sex Transm Dis. 2006;33(7 Suppl):S23–31. https://doi.org/10.1097/01.olq.0000221018.32533.6d.
Van der Straten A, Catania JA, Pollack L. Psychosocial correlates of health-protective sexual communication with new sexual partners: the National AIDS Behavioral Survey. AIDS Behav. 1998;2(3):213–27. https://doi.org/10.1023/A:1022137817863.
Wasserman S, Faust K. Social network analysis: methods and applications. Cambridge: Cambridge University Press; 1994.
Wenzel S, Holloway I, Golinelli D, Ewing B, Bowman R, Tucker J. Social networks of homeless youth in emerging adulthood. J Youth Adolesc. 2012;41(5):561–71. https://doi.org/10.1007/s10964-011-9709-8.
Widman L, Choukas-Bradley S, Helms SW, Golin CE, Prinstein MJ. Sexual communication between early adolescents and their dating partners, parents, and best friends. J Sex Res. 2014;51:731–41. https://doi.org/10.1080/00224499.2013.843148.
Widman L, Noar SM, Choukas-Bradley S, Francis DB. Adolescent sexual health communication and condom-use: a meta-analysis. Health Psychol. 2014;33:1113–24. https://doi.org/10.1037/hea0000112.
Wight D. Impediments to safer heterosexual sex: a review of research with young people. AIDS Care. 1992;4(1):11–23. https://doi.org/10.1080/09540129208251616.
Funding
This study was funded by NIMH (R01 MH093396).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All the authors of this study have no conflict of interest to report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Craddock, J.B., Barman-Adhikari, A., Combs, K.M. et al. Individual and Social Network Correlates of Sexual Health Communication Among Youth Experiencing Homelessness. AIDS Behav 24, 222–232 (2020). https://doi.org/10.1007/s10461-019-02646-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-019-02646-x