
Abstract
Although antiretroviral therapy (ART) is vital to people living with HIV (PLWH) by suppressing the virus and in turn preventing onward HIV transmission and reducing AIDS-related morbidity and mortality, the rates of optimal ART adherence continuously remain low. Disclosure of HIV status is considered to be a critical predictor of ART adherence. However, few studies have explored the mechanisms underlying the association between disclosure and medication adherence. The current study aims to examine the mediating role of social support and self-efficacy underlying the relationship between HIV disclosure to family members and ART adherence. PLWH in China provided data on HIV disclosure, ART adherence, perceived social support on medication adherence, adherence self-efficacy, and social-demographic information. The path analyses revealed that disclosure to family members had significant indirect effects on adherence via social support and self-efficacy. Our findings suggested that HIV disclosure might positively affect ART adherence through two psychosocial pathways: social support and self-efficacy. Future intervention to improve medication adherence among PLWH should consider targeting these two factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There are approximately 36.9 million people living with HIV (PLWH) globally, among whom 1.8 million are newly infected with HIV in 2017 [1]. The use of antiretroviral therapy (ART) dramatically improves health outcomes and prolongs life expectancy of PLWH [2]. With the increasing coverage of ART, 21.7 million PLWH have initiated ART by the end of 2017 [1]. Adherence to ART regimen is essential for sustained viral suppression [3], which prevents onward HIV transmission to others [4] and reduces AIDS-related mortality [5]. Optimal adherence, which is often considered as 95% or more of prescribed doses taken [6,7,8], is linked to better inhibition of viral mutation thereby avoiding evolution of drug resistant viruses [9]. Unfortunately, the adherence rates continue to remain low with only 61%–83% across various cultural settings [10,11,12]. Given the importance of optimal adherence, a better understanding of influential factors of medication adherence becomes pressing and urgent.
ART adherence is influenced by many factors, including personal attributes, institutional resources, treatment related factors, and psychosocial factors [13]. One of the key and complex predictors is disclosure of HIV diagnosis [14], which refers to revealing personal HIV seropositive status to others. For PLWH, HIV disclosure might be an important step in engaging in HIV care [15]. A previous study found that greater disclosure was significantly related with better adherence after controlling other relevant variables [16]. Another study also found that participants who disclosed to more than two family members and/or steady partners were more likely to take all of the prescribed doses in the past 4 days [17]. Family members were more likely to become targets of disclosure, and sometimes the initial targets [18]. For example, among 76 men living with HIV who had disclosed to at least one person, 62% disclosed to a family member and 21% to a friend [19]. Among 314 women living with HIV who had disclosed, 56.4% of them first disclosed to either parents or husbands [20]. Furthermore, a longitudinal study of HIV-positive mothers reported that a lack of disclosure to family members at baseline predicted missed medical appointments at follow-up, while no significant relationship was found between general disclosure and ART adherence [21]. The disclosure target preference in family members might be due to the emotional support and positive responses that PLWH could receive [18]. Thus, in anticipation of supportive responses, disclosure to family members might be a key factor in improving and maintaining ART adherence [16, 22, 23]. Although research investigating pathways underlying disclosure to family members and ART adherence is limited, some of the psychosocial variables that are associated with disclosure may also influence ART adherence, both theoretically and empirically.
According to the Disclosure Processes Model [14, 24], social support is a potential mediator explaining the effect of disclosure on adherence. The model posits that multiple processes exist between disclosure and various long-term outcomes. Specifically, disclosure has effect on social, contextual, dyadic (e.g., spousal or family relationship), and clinical outcomes (e.g. medication adherence) through three possible mediation processes, including alleviation of inhibition, changes in social information, and social support [14]. Consistent with the theoretical framework, qualitative data from 152 HIV infected adults suggested that disclosure and adherence could influence each other, in which social support was speculated as an active element [25]. On one hand, HIV disclosure, especially to family members [26], has been associated with social support across ethnicity, gender and sexual orientation [27,28,29,30,31]. On the other hand, a number of cross-sectional studies reported that high levels of perceived social support were linked with optimal ART adherence [32,33,34,35,36]. Although few studies have directly explored the mediation role of social support, these existing empirical data generally support the premise of the theoretical conjecture that disclosure might benefit adherence through augmenting social support [14]. Meanwhile, comparing with general social support, medication-specific social support might be a proximal predictor of ART adherence. Researchers argue that general social support is more useful in predicting psychological outcomes rather than behavioral outcomes but specific social support may work in the opposite direction [37]. Consistent with this line of reasoning, a study found that medication-specific social support significantly influenced ART adherence, while general social support did not [38].
Self-efficacy might be another potential mediator underlying the association between disclosure and ART adherence. According to the Social Cognitive Theory, individuals who have higher self-efficacy to perform health promoting behavior are more likely to do so [39, 40]. Although few, if any, research has directly explored the mediation role of self-efficacy between disclosure and ATR adherence, studies have proved that self-efficacy is associated with ART adherence as well as disclosure [41,42,43]. Compared with general self-efficacy, the association with ART adherence is especially solid for medication-specific self-efficacy [44]. Medication self-efficacy refers to an individual belief that oneself will be able to take medication as prescribed. Medication self-efficacy has been evidenced as a stronger predictor of ART adherence in comparison with key sociodemographic variables (e.g., age), treatment-related factors (e.g., duration of ART), disease-related conditions (e.g., CD4 cell count), interpersonal correlates (e.g., social support), and other behavioral predictors (e.g., current substance use) [45]. The significant association between medication self-efficacy and ART adherence has been reported in a number of studies [44,45,46]. Considering the theoretical basis and empirical evidence, it is plausible to hypothesize that treatment self-efficacy might play a mediation role between disclosure and adherence.
The serial mediating effect of social support and self-efficacy between disclosure and ART adherence has not been established, while it might possibly exist. The Social Cognitive Theory indicates that social support is likely to engender self-efficacy beliefs, which in turn improve health outcomes [47]. Align with the theory, two cross-sectional studies suggested that social support was indirectly associated with ART adherence through self-efficacy [48, 49]. However, whether disclosure might impact adherence through social support and self-efficacy successively still needs to be clarified. Testing serial (“chain”) mediation is necessary since it might uncover complex mechanisms between disclosure and adherence in future studies [50]. Given the theoretical backdrop and empirical findings, serial mediation effect of social support and self-efficacy may exist between the relationship of disclosure and adherence. However, these mediational chains have not been empirically tested to date. Meanwhile the impact of potential serial mediators has also not been fully examined. The main purpose of the present study is to explore whether medication social support and treatment adherence self-efficacy mediate the relationship between disclosure to family members and ART adherence.
Two main hypothesized models are proposed to investigate mechanisms linking disclosure and adherence. First, social support and self-efficacy serve as individual mediators. With parallel models in which two mediators do not interact with each other [51], social support and self-efficacy are hypothesized to be predicted by the disclosure and to then predict ART adherence separately (i.e., disclosure → social support → ART adherence; disclosure → self-efficacy → ART adherence). Second, social support and self-efficacy function in a sequential chain of mediators between disclosure and ART adherence (i.e., disclosure → social support → self-efficacy → ART adherence).
Method
Study Sites
Data were drawn from a cross-sectional survey designed to explore psychosocial and behavioral factors related to mental and physical health among PLWH [52]. The survey started in October 2012 and lasted for 10 months in Guangxi Autonomous Region (Guangxi) in China. Guangxi was ranked first in 2012 in number of newly reported HIV/AIDS cases among 34 provinces and autonomous regions in China [53]. From all of 17 cities and 75 counties, the top 2 cities and 10 counties in terms of the number of cumulative HIV/AIDS cases were selected as study sites. The selected study sites had about 43% of total reported cases in Guangxi in 2012 [34].
Participants
Approximately 10% of the reported HIV/AIDS cases at each participating site were randomly recruited by the staff at the local centers for disease control and prevention (CDC). About 90% of recruited cases gave their consent to attend the study. Among the 2987 PLWH who participated in the study, parents (N=1254) who had children of 5 to 16 years old were asked to complete an additional section on HIV disclosure. The current study sample consisted of 874 (69.70%) of these parents who initiated ART and provided data regarding ART adherence.
Survey Procedure
Based on participants’ personal preference or literacy level, about three quarters (77.78%) of the current study sample completed the survey via face-to-face interviews, whereas the rest of participants completed the survey on their own. To assure confidentiality, the survey was conducted in private offices of local community health centers or HIV clinics where participants received medical care. The entire survey took about 75–100 min to complete. After completion, each participant received a five-dollar-worth household item for compensation for their time. The research protocol was approved by Institutional Review Boards at both Wayne State University in the United States and Guangxi CDC in China.
Measures
Disclosure to Family Members
One multiple-response question was administered to assess participants’ disclosure to their family members (i.e., “Whom have you told about your HIV infection?”). Fourteen options were provided, including spouse/steady sexual partners, casual sexual partners, father, mother, brothers, sisters, grandparents, adult children, minor children, other relatives, friends, co-workers or bosses, others, or no one. Following a similar procedure in the existing study [15], a continuous variable was created by counting the number of positive (“yes”) response to options of family member (e.g., spouse, parents, siblings, grandparents, and children). The possible scores of disclosure to family members ranged from 0 to 8 with a higher score indicating a higher level of disclosure to family members.
Medication Social Support
Medication-specific social support was measured with an 8-item scale [38] to identify how often participants received help for their medication taking over a three-month period (e.g., “Someone reminded you to take your medicine”) on a 5-pont scale ranging from “never” (0) to “always” [4]. The responses to all 8 items in the scale were averaged to form an index of medication-specific social support. The index score ranged from 0 to 4 with a higher score indicating a higher level of medication social support. A previous study showed that the scale has a high reliability and a good construct validity [33]. Cronbach α was 0.92 for the scale in the current study.
Treatment Adherence Self-efficacy
Self-efficacy of treatment adherence was assessed with a 12-item scale used in a previous study [46]. The scale consists of statements that reflect participants’ confidence of following directions on medication, controlling side effects, and managing treatment-related health problems. These statements were rated on 5-point Likert response ranging from 1 (completely not sure) to 5 (completely sure). A composite score was calculated by summing the responses to 12 items. The composite scores ranged from 12 to 60 with a higher score indicating better self-efficacy on HIV treatment adherence. Cronbach α was 0.92 for the scale in the current study.
ART Adherence
Five items were employed to assess adherence to ART. The first two items asked participants if they had missed any dose in the past weekend/ever before with responses being recorded to reflect an adherence (1 = not missed, 0 = missed). The other three items inquired the total number of prescribed doses and the number of doses that participants actually took within three specific time windows (i.e., past 3 days, past weekend, or past month). The responses to each of these items were first converted into percentage of doses taken as scheduled and then dichotomized into 1 (≥ 95% of prescribed doses) or 0 (< 95%). The threshold of 95% is used in current study as the existing literature suggested that 95% as the optimal level of adherence to sustain viral suppression [3] and to avoid evolution of drug resistant viruses [9]. An adherence index score was generated by summing the dichotomous scores of the five items to reflect an optimal adherence (score=5) or suboptimal adherence (score < 5).
Potential Covariates
Data on the following covariates that were identified in a previous study [50] were collected and included in the final path analysis.
Demographic Information
Participants were asked to provide information on their age, gender, ethnicity, marital status, residence status, employment status, education in years, monthly household income, drug use, duration since diagnosis, and HIV infection among other family members.
Depression
Depressive symptoms were assessed with the short 10-item version of the Center for Epidemiological Studies Depression Scale (CESD-10) [54]. Each CESD-10 item was rated on a 4-point scale (0 = never, 1 = sometime, 2 = often, and 3 = always). A total score ranging from 0 to 30 was created with higher scores indicating a higher depressive symptom (Cronbach α = 0.78).
Stigma
HIV-related stigma was assessed using 14 items with a 4-point scale (1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree) [55]. A composite score was calculated by summing the scores of 14 items. The HIV-related stigma scale had a Cronbach’s α of 0.93 in the current study.
Data Analysis
First, independent-samples t test or χ2 test was performed to examine the differences of demographic variables, treatment factors, and psychological factors between optimal adherence group and suboptimal adherence group. All the covariates that were significantly different between adherence groups (e.g., age, ethnicity, data collection mode, and income), as well as predictors of adherence that were identified in previous studies (e.g., stigma, depression), were included in the further path analysis.
Second, the correlation coefficients were calculated among main study variables. Finally, path analyses of both parallel mediation and serial mediation models were conducted using PROCESS for SPSS [51], providing estimates of path coefficients (β) and bootstrapped 95% confidence intervals (95% CI) for indirect effects based on 5000 resamples. In addition, an alternative model with reversed pathways was tested with the same procedure. Due to smaller variances accounted by the alternative model, only results from the originally hypothesized models were reported. Among the 874 participants in the current analysis, 678 (77.57%) had complete data (i.e., non-missing) in any of the study variables. The maximum percentage of missing responses for any single variable was less than 5%. The expectation maximization method was used to impute missing data [56]. All statistical analyses were performed using SPSS 24.0. A p value of less than 0.05 was employed to indicate statistical significance
Results
Sample Characteristics
As shown in Table 1, the average age of the study sample (n = 874) was 37.23 years old (SD = 5.90). The majority of the participants were male (57.67%), of Han ethnicity (71.05%), married (78.56%), and living in rural area (71.79%). The rates of unemployment, part-time job and full-time job were 17.55, 37.61 and 44.84%, respectively. Their average years of formal schooling were about 7.16 years (SD = 2.67). More than half of the participants reported less than 1000 Chinese yuan (or approximately 159 US dollars) of household income per month, which was less than half of that for the local population at the provincial level [57]. The average length of HIV diagnosis was 45.07 months (SD = 28.43). About one half (51.83%) of the participants reported that at least one other family member was also infected with HIV.
Group Differences by Adherence
About half of the participants (n = 468, 53.55%) were considered having optimal adherence, while the others (n = 406, 46.45%) were considered as having suboptimal adherence. Table 1 presents the differences of key variables between two adherence groups. Most of the variables (e.g., gender, ethnicity, marital status, residence status, work status, education in years, household income, duration since diagnosis, other HIV infection in family, depression, HIV stigma, disclosure to family members, social support to treatment) did not significantly differ between the adherence groups (all ps > 0.05). Compared to participants in suboptimal group, those in the optimal group were older (37.64 vs. 36.76 years, p < 0.05) and had a lower proportion of drug use (17.20% vs. 23.08%, p < 0.05). Moreover, participants in the optimal group had a higher proportion of completing the survey via face-to-face interview than those in suboptimal group (81.41% vs. 73.58%, p < 0.05) and a higher score of self-efficacy (47.10 vs. 45.09, p < 0.01).
Associations Among Main Study Variables
As displayed in Table 2, disclosure to family members was positively associated with drug use (r = 0.11, p < 0.01), social support (r = 0.13, p < 0.01) and self-efficacy (r = 0.15, p < 0.01). Social support had a positive relationship with treatment self-efficacy (r = 0.19, p < 0.01). ART adherence also showed a significantly positive correlation with treatment self-efficacy (r = 0.25, p < 0.01). In addition, the disclosure to family member was negatively associated with participants’ age (r = − 0.16, p < 0.01).
Path Analysis
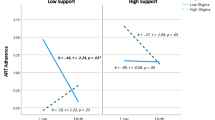
The results of final parallel mediation models (e.g., estimates of path coefficients, percentage of variance explained in each key variable) were presented in Fig. 1a (social support model) and Fig. 1b (self-efficacy model). The results of the serial mediation model were presented in Fig. 1c.

Path analysis model for the direct and indirect effects of disclosure to immediate family members on medication adherence via social support and adherence self-efficacy. Potential confounding variables which were significantly associated with ART adherence were controlled in the model as covariates, including age, ethnicity, monthly household income, data collection mode, depression, and stigma. Correlations between covariates and ART adherence have been omitted for reasons of presentation simplicity. The solid line and dashed line indicated significant and non-significant path coefficients, respectively. *p < 0.05; **p < 0.01
As shown in Table 3, the parallel mediation analysis indicated that the mediating effect of social support (Fig. 1a) was not significant (β = 0.005, 95% CI [− 0.001, 0.01]), while self-efficacy (Fig. 1b) was a significant mediator of the relationship between disclosure and adherence (β = 0.03, 95% CI [0.01, 0.05]). The parallel models explained 1.74% and 3.22% of the variance in social support and self-efficacy, respectively. The social support model and self-efficacy model explained 2.12% and 8.22% of the variance in ART adherence, respectively.
Serial mediation analysis (Fig. 1c) showed that the hypothesized model with both direct and indirect paths from disclosure to adherence accounted for 1.74% variances in social support, 6.04% variances in self-efficacy and 8.22% in ART adherence. The direct effect of disclosure on adherence was not significant (β = − 0.04, 95% CI [− 0.09, 0.004]), so was the direct effect of social support on adherence (β = 0.01, 95% CI [− 0.07, 0.08]), while self-efficacy showed a significant direct effect on adherence (β = 0.04, 95% CI [0.03, 0.05]). As shown in Table 3, the indirect effect of the serial mediation from disclosure to adherence via social support and self-efficacy was significant (β = 0.004, 95% CI [0.002, 0.01]).
Discussion
The results of the present study indicate a potential indirect effect of disclosure of HIV status to family members on ART adherence, through both individual mediators and serial mediators. The findings suggested that disclosure was positively associated with adherence self-efficacy, which is related to a better adherence. The pathway suggests that adherence self-efficacy plays an important role in disclosure-adherence association. As adherence self-efficacy reflects one’s confidence to deal with health problems related to treatment, adhere to ART regimen, and manage side effects [46], high self-efficacy might help augment the benefits of disclosure and buffer the possible and often unexpected negative effects of disclosure on adherence, which in turn amplify the overall advantage of disclosure on adherence. This finding is consistent with previous studies, in which medication self-efficacy acted as a protector to alleviate negative influence of stigma on quality of life [52] and was introduced as a facilitator to ART adherence [46].
The indirect path from disclosure to adherence via medication-specific social support and adherence self-efficacy is also significant. The combined indirect effect of social support and self-efficacy suggests that disclosure might give rise to greater social support, which leads to better self-efficacy, which finally positively impacts disclosure. Given that mediating effect of social support alone between disclosure and adherence is not significant in current study, the significant mediating role of social support and self-efficacy may imply an interlinked effect. Instead of operating separately, social support aroused by disclosure might be conducive to adherence only when it facilitates self-efficacy. Should it be the case, self-efficacy would be a more immediate cause than social support and social support would be in vain if oneself have no confidence to adhere. This finding is consistent with previous study in which treatment adherence self-efficacy was found to mediate the relationship between general social support and adherence [48]. The same study also showed that the association between general social support and self-efficacy was no longer significant when patient satisfaction with healthcare providers was taken into consideration, which suggested that social support from a healthcare provider was more important than general support in enhancing self-efficacy [48]. In line with this evidence, our finding also implies that treatment or adherence specific social support and self-efficacy might be better indicators in studies related to ART treatment, compared with general social support and self-efficacy.
In consistent with some previous studies, the direct path between disclosure and adherence was not significant. This result suggests a possibility of both positive and negative effects of disclosure. On the one hand, disclosure is beneficial when it alleviates depression and anxiety [58], enhances social support [28] and releases the stress of secrecy [59]. On the other hand, disclosure (especially those that are unplanned, or culturally or developmentally inappropriate) could be harmful when it disrupts relationships with families or communities [60], evokes partner violence [61], increases the perceptions of stigma [14], and leads to psychological distress [62]. Our result provides evidence to support the notion that not all the disclosures necessarily appear to benefit adherence [63]. In addition, disclosure could be associated with adherence through different pathways, in which mechanisms are complex and diverse.
The results extend our understanding about how disclosure of HIV status is related with ART adherence by uncovering the role of social support towards treatment adherence and self-efficacy in taking medications and managing the disease. The findings might have several implications for future interventions aimed at improving ART adherence. First, the present study suggests possible efforts which may bolster the effectiveness of various existing interventions of ART adherence. For example, a cognitive-behavioral therapy-based intervention was developed in order to facilitate adherence [59]. The intervention contained 12 sessions to discuss difficulties and progresses in adherence and to generate strategies to solve the problems. The present study implies that the existing intervention of adherence might by further enhanced by adding sessions targeting disclosure management, perceived social support, and self-efficacy enhancement. Second, the results suggest a chain relationship among disclosure, social support and self-efficacy, which indicate that disclosure management may help to improve social support [26, 64] and then self-efficacy [65] in a row. This finding may also contribute to intervention improvement. While some interventions solely targeted on disclosure [43] or social support [66] as a means of improving ART adherence, our results indicate that further interventions may combine or integrate the efforts in managing disclosure, improving social support and self-efficacy, so the intervention motivating disclosure could also be efficacious to energize social support and self-efficacy and improve adherence at the same time.
Inevitably, this study has some limitations. First, questions concerning HIV are always sensitive so that the responses would be influenced by social desirability [67], especially when questions are presented via face-to-face interviews compared to self-administered survey [68]. Social desirability might account for the difference in adherence between participants who completed survey via face-to-face interview and participants who completed questionnaires by themselves. Besides the bias produced by social desirability, self-report may result in overestimation of adherence because of the inaccuracy in recalling times of medicine taking over a long retrospective window (e.g. 30 days) [69]. However, although self-report is subject to social desirability and recall bias, it is generally considered a valid assessment technique of adherence that associates steadily and consistently with biological markers of medical treatment such as viral load and CD4 count [38, 65, 70]. Even so, it is suggested to combine different measurements of adherence, such as electric monitoring and self-report, to improve the assessment accuracy in future research [70].
Second, our findings should be considered preliminary. Although some of the pathways were significant, the percentage of variance explained in each key variable by the serial mediation model was small (e.g., 1.74% in social support, 6.04% in self-efficacy, and 8.22% in ART adherence). The insufficient variances explained suggest that there may be other important factors besides social support and self-efficacy that impact ART adherence. As a matter of fact, existing literature has suggested numerous factors that may impact adherence, including psychological symptoms [71], stigma [72], frequency of religious attendance [73], financial status [74], even demographics such as age [75], gender [76] and ethnicity [77]. Third, our data were derived from a cross-sectional survey, where causal inference cannot be generated. Although we tested an alternative model with reversed pathways and found less variance that would be accounted by the model, we still could not rule out the reverse-causality. The preliminary nature of this study suggests the potential tenuousness of the effect. For future research, longitudinal and prospective research is needed to evaluate causal relationships and to examine further impacts that disclosure may have on adherence over time.
In summary, the results of the current study indicated a role of social support and self-efficacy in mediating the relationship between HIV disclosure to family members and medication adherence among PLWH. Though the indirect effect was small, the findings extend our understanding of the relationship among disclosure, social support, self-efficacy, and ART adherence, which could be critical for improvement and implementation of future interventions with an ultimate goal of improving ART adherence among PLWH in China and other cultural settings.
References
The United Nations Joint Programme on HIV/AIDS. UNAIDS data 2017. http://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf. Accessed 2018.
Maile R, Roger L, Sterne JAC, Sonia HD, Robins JM, Caroline S, et al. The effect of combined antiretroviral therapy on the overall mortality of HIV-infected individuals. AIDS. 2010;24(1):123–37.
Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30.
Vernazza PL, Eron JJ, Fiscus SA, Cohen MS. Sexual transmission of HIV: infectiousness and prevention. AIDS. 1999;13(2):155–66.
Wood E, Hogg RS, Yip B, Harrigan PR, O’Shaughnessy MV, Montaner JS. Is there a baseline CD4 cell count that precludes a survival response to modern antiretroviral therapy? AIDS. 2003;17(5):711–20.
Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14:365.
Biressaw S, Abegaz WE, Abebe M, Taye WA, Belay M. Adherence to antiretroviral therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatr. 2013;13:132.
Cluver LD, Hodes RJ, Toska E, Kidia KK, Orkin FM, Sherr L, et al. ‘HIV is like a tsotsi. ARVs are your guns’: associations between HIV-disclosure and adherence to antiretroviral treatment among adolescents in South Africa. AIDS. 2015;29(Suppl 1):57–65.
Massad LS, Evans CT, Wilson TE, Golub ET, Goparaju L, Howard A, et al. Intermediate highly active antiretroviral therapy adherence thresholds and empirical models for the development of drug resistance mutations. J Acquir Immune Defic Syndr. 2008;47(3):397–402.
Brown JL, Littlewood RA, Vanable PA. Social-cognitive correlates of antiretroviral therapy adherence among HIV-infected individuals receiving infectious disease care in a medium-sized northeastern US city. AIDS Care. 2013;25(9):1149–58.
Cederfjall C, Langius-Eklof A, Lidman K, Wredling R. Self-reported adherence to antiretroviral treatment and degree of sense of coherence in a group of HIV-infected patients. AIDS Patient Care STDS. 2002;16(12):609–16.
Godin G, Gagne C, Naccache H. Validation of a self-reported questionnaire assessing adherence to antiretroviral medication. AIDS Patient Care STDS. 2003;17(7):325–32.
Fogartya L, Rotera D, Larsona S, Burkea J, Gillespieb J, Levy R. Patient adherence to HIV medication regimens: a review of published and abstract reports. Patient Educ Couns. 2002;46:93–108.
Chaudoir SR, Fisher JD, Simoni JM. Understanding HIV disclosure: a review and application of the disclosure processes model. Soc Sci Med. 2011;72(10):1618–29.
Qiao S, Li X, Stanton B. Disclosure of parental HIV infection to children: a systematic review of global literature. AIDS Behav. 2013;17(1):369–89.
Stirratt MJ, Remien RH, Smith A, Copeland OQ, Dolezal C, Krieger D, et al. The role of HIV serostatus disclosure in antiretroviral medication adherence. AIDS Behav. 2006;10(5):483–93.
Spire B, Carrieri P, Sopha P, Protopopescu C, Prak N, Quillet C, et al. Adherence to antiretroviral therapy in patients enrolled in a comprehensive care program in Cambodia: a 24 month follow-up assessment. Antivir Ther. 2008;13(5):697–703.
Serovich JM, Craft SM, Yoon HJ. Women’s HIV disclosure to immediate family. AIDS Patient Care STDS. 2007;21(12):970–80.
Ko NY, Lee HC, Hsu ST, Wang WL, Huang MC, Ko WC. Differences in HIV disclosure by modes of transmission in Taiwanese families. AIDS Care. 2007;19(6):791–8.
Sowell RL, Seals BF, Phillips KD, Julious CH. Disclosure of HIV infection: how do women decide to tell? Health Educ Res. 2003;18(1):32–44.
Mellins CA, Kang E, Leu CS, Havens JF, Chesney MA. Longitudinal study of mental health and psychosocial predictors of medical treatment adherence in mothers living with HIV disease. AIDS Patient Care STDS. 2003;17(8):407–16.
Wouters E, van Loon F, van Rensburg D, Meulemans H. Community support and disclosure of HIV serostatus to family members by public-sector antiretroviral treatment patients in the Free State Province of South Africa. AIDS Patient Care STDS. 2009;23(5):357–64.
Malcolm SE, Ng JJ, Rosen RK, Stone VE. An examination of HIV/AIDS patients who have excellent adherence to HAART. AIDS Care Psychol Socio-Med Aspects AIDS/HIV. 2003;15(2):251–61.
Qiao S, Li X, Stanton B. Theoretical models of parental HIV disclosure: a critical review. AIDS Care. 2013;25(3):326–36.
Klitzman RL, Kirshenbaum SB, Dodge B, Remien RH, Ehrhardt AA, Johnson MO, et al. Intricacies and inter-relationships between HIV disclosure and HAART: a qualitative study. AIDS Care. 2004;16(5):628–40.
Kalichman SC, DiMarco M, Austin J, Luke W, DiFonzo K. Stress, social support, and HIV-status disclosure to family and friends among HIV-positive men and women. J Behav Med. 2003;26(4):315–32.
Vyavaharkar M, Moneyham L, Corwin S, Tavakoli A, Saunders R, Annang L. Hiv-disclosure, social support, and depression among HIV-infected African American women living in the rural southeastern United States. AIDS Educ Prev. 2011;23(1):78–90.
Zea MC, Reisen CA, Poppen PJ, Bianchi FT, Echeverry JJ. Disclosure of HIV status and psychological well-being among Latino gay and bisexual men. AIDS Behav. 2005;9(1):15–26.
Qiao S, Li X, Zhou Y, Shen Z, Tang Z, Stanton B. Factors influencing the decision-making of parental HIV disclosure: a socio-ecological approach. AIDS. 2015;29(Suppl 1):S25–34.
Lin X, Chi P, Zhang L, Zhang Y, Fang X, Qiao S, et al. Disclosure of HIV serostatus and sexual orientation among HIV-positive men who have sex with men in China. Community Ment Health J. 2016;52(4):457–65.
Qiao S, Li X, Zhou Y, Shen Z, Tang Z. Interpersonal factors associated with HIV partner disclosure among HIV-infected people in China. AIDS Care. 2016;28(Suppl 1):37–43.
Catz SL, Kelly JA, Bogart LM, Benotsch EG, McAuliffe TL. Patterns, correlates, and barriers to medication adherence among persons prescribed new treatments for HIV disease. Health Psychol. 2000;19(2):124–33.
Gonzalez JS, Penedo FJ, Antoni MH, Duran RE, McPherson-Baker S, Ironson G, et al. Social support, positive states of mind, and HIV treatment adherence in men and women living with HIV/AIDS. Health Psychol. 2004;23(4):413–8.
Huynh AK, Kinsler JJ, Cunningham WE, Sayles JN. The role of mental health in mediating the relationship between social support and optimal ART adherence. AIDS Care. 2013;25(9):1179–84.
Woodward EN, Pantalone DW. The role of social support and negative affect in medication adherence for HIV-infected men who have sex with men. J Assoc Nurses AIDS Care. 2012;23(5):388–96.
Waddell EN, Messeri PA. Social support, disclosure, and use of antiretroviral therapy. AIDS Behav. 2006;10(3):263–72.
Darbes LA, Lewis MA. HIV-specific social support predicts less sexual risk behavior in gay male couples. Health Psychol. 2005;24(6):617–22.
Lehavot K, Huh D, Walters KL, King KM, Andrasik MP, Simoni JM. Buffering effects of general and medication-specific social support on the association between substance use and HIV medication adherence. AIDS Patient Care STDS. 2011;25(3):181–9.
Bandura A. Social foundations of thought and action: a social cognitive theory. Upper Saddle River: Prentice-Hall; 1987. p. 169–71.
Bandura A. Social cognitive theory and exercise of control over HIV infection. New York: Springer; 1994. p. 25–59.
Brown MJ, Serovich JM, Kimberly JA, Umasabor-Bubu O. Disclosure and self-efficacy among HIV-positive men who have sex with men: a comparison between older and younger adults. AIDS Patient Care STDS. 2015;29(11):625–33.
Kalichman SC, Nachimson D. Self-efficacy and disclosure of HIV-positive serostatus to sex partners. Health Psychol. 1999;18(3):281–7.
Machtinger EL, Lavin SM, Hilliard S, Jones R, Haberer JE, Capito K, et al. An expressive therapy group disclosure intervention for women living with HIV improves social support, self-efficacy, and the safety and quality of relationships: a qualitative analysis. J Assoc Nurses AIDS Care. 2015;26(2):187–98.
Archiopoli A, Ginossar T, Wilcox B, Avila M, Hill R, Oetzel J. Factors of interpersonal communication and behavioral health on medication self-efficacy and medication adherence. AIDS Care. 2016;28(12):1607–14.
Colbert AM, Sereika SM, Erlen JA. Functional health literacy, medication-taking self-efficacy and adherence to antiretroviral therapy. J Adv Nurs. 2013;69(2):295–304.
Zhang L, Li X, Lin Z, Jacques-Tiura AJ, Xu J, Zhou Y, et al. Side effects, adherence self-efficacy, and adherence to antiretroviral treatment: a mediation analysis in a Chinese sample. AIDS Care. 2016;28(7):919–26.
Bandura A. Self-efficacy: the exercise of control. J Cogn Psychother 2005;13(2):75–8.
Diiorio C, McCarty F, Depadilla L, Resnicow K, Holstad MM, Yeager K, et al. Adherence to antiretroviral medication regimens: a test of a psychosocial model. AIDS Behav. 2009;13(1):10–22.
Cha E, Erlen JA, Kim KH, Sereika SM, Caruthers D. Mediating roles of medication-taking self-efficacy and depressive symptoms on self-reported medication adherence in persons with HIV: a questionnaire survey. Int J Nurs Stud. 2008;45(8):1175–84.
Tomfohr LM, Pung MA, Dimsdale JE. Mediators of the relationship between race and allostatic load in African and White Americans. Health Psychol. 2016;35(4):322–32.
Hayes AF. Introduction to mediation, moderation and conditional process analysis: a regression-based approach. New York: Guilford; 2013.
Zhou G, Li X, Qiao S, Shen Z, Zhou Y. Influence of side effects on ART adherence among PLWH in China: the moderator role of ART-related knowledge. AIDS Behav. 2018;22(3):961–70.
Ministry of Health of the People’s Republic of China. 2012 China AIDS Response Progress Report. http://ghdx.healthdata.org/record/china-aids-response-progress-report-2012. Accessed 2012.
Kohout FJ, Berkman LF, Evans DA, Cornoni-Huntley J. Two shorter forms of the CES-D (Center for Epidemiological Studies Depression) depression symptoms index. J Aging Health. 1993;5(2):179–93.
Berger BE, Ferrans CE, Lashley FR. Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res Nurs Health. 2001;24(6):518–29.
Lipira L, Williams EC, Huh D, Kemp CG, Nevin PE, Greene P, et al. HIV-related stigma and viral suppression among African-American women: exploring the mediating roles of depression and ART nonadherence. AIDS Behav. 2018. https://doi.org/10.1007/s10461-018-2301-4.
National Bureau of Statistics of China. China Statistical Yearbook. http://www.stats.gov.cn/tjsj/ndsj/2013/indexch.htm. Accessed 2013.
Hays RB, McKusick L, Pollack L, Hilliard R, Hoff C, Coates TJ. Disclosing HIV seropositivity to significant others. AIDS. 1993;7(3):425–31.
Katz IT, Ryu AE, Onuegbu AG, Psaros C, Weiser SD, Bangsberg DR, et al. Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis. J Int AIDS Soc. 2013;16(3 Suppl 2):18640.
Clum GA, Czaplicki L, Andrinopoulos K, Muessig K, Hamvas L, Ellen JM, et al. Strategies and outcomes of HIV status disclosure in HIV-positive young women with abuse histories. AIDS Patient Care STDS. 2013;27(3):191–200.
Gielen AC, McDonnell KA, Burke JG, O’Campo P. Women’s lives after an HIV-positive diagnosis: disclosure and violence. Matern Child Health J. 2000;4(2):111–20.
Comer LK, Henker B, Kemeny M, Wyatt G. Illness disclosure and mental health among women with HIV/AIDS. J Commun Appl Soc Psychol. 2000;10(6):449–64.
Li X, de Wit J, Qiao S, Sherr L. HIV disclosure to children in low-and middle-income countries: towards effective interventions. AIDS. 2015;29(Suppl 1):S1–5.
Ortiz CE. Disclosing concerns of Latinas living with HIV/AIDS. J Transcult Nurs. 2005;16(3):210–7.
Simoni JM, Kurth AE, Pearson CR, Pantalone DW, Merrill JO, Frick PA. Self-report measures of antiretroviral therapy adherence: a review with recommendations for HIV research and clinical management. AIDS Behav. 2006;10(3):227–45.
Simoni JM, Pantalone DW, Plummer MD, Huang B. A randomized controlled trial of a peer support intervention targeting antiretroviral medication adherence and depressive symptomatology in HIV-positive men and women. Health Psychol. 2007;26(4):488–95.
McCallum EB, Peterson ZD. Investigating the impact of inquiry mode on self-reported sexual behavior: theoretical considerations and review of the literature. J Sex Res. 2012;49(2–3):212–26.
Richman WL, Weisband S, Kiesler S, Drasgow F. A meta-analytic study of social desirability distortion in computer administered questionnaires, traditional questionnaires, and interviews. J Appl Psychol. 1999;84(5):754–75.
Levine AJ, Hinkin CH, Marion S, Keuning A, Castellon SA, Lam MM, et al. Adherence to antiretroviral medications in HIV: differences in data collected via self-report and electronic monitoring. Health Psychol. 2006;25(3):329–35.
Pearson CR, Simoni JM, Hoff P, Kurth AE, Martin DP. Assessing antiretroviral adherence via electronic drug monitoring and self-report: an examination of key methodological issues. AIDS Behav. 2007;11(2):161–73.
MacDonell KK, Jacques-Tiura AJ, Naar S, Fernandez MI, Team ATNP. Predictors of self-reported adherence to antiretroviral medication in a multisite study of ethnic and racial minority HIV-positive youth. J Pediatr Psychol. 2016;41(4):419–28.
Elwell K. Facilitators and barriers to treatment adherence within PMTCT programs in Malawi. AIDS Care. 2016;28(8):971–5.
Dalmida SG, McCoy K, Koenig HG, Miller A, Holstad MM, Thomas T, et al. Examination of the role of religious and psychosocial factors in HIV medication adherence rates. J Relig Health. 2017;56(6):2144–61.
Langebeek N, Gisolf EH, Reiss P, Vervoort SC, Hafsteinsdottir TB, Richter C, et al. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: a meta-analysis. BMC Med. 2014;12:142.
Cockerham L, Scherzer R, Zolopa A, Rimland D, Lewis CE, Bacchetti P, et al. Association of HIV infection, demographic and cardiovascular risk factors with all-cause mortality in the recent HAART era. J Acquir Immune Defic Syndr. 2010;53(1):102–6.
Yildiz Sevgi D, Gunduz A, Altuntas Aydin O, Mete B, Sargin F, Kumbasar Karaosmanoglu H, et al. Adherence to antiretroviral therapy in Turkey: results from the ACTHIV-IST Study Group. AIDS Res Hum Retroviruses. 2017;33(12):1192–8.
Daskalopoulou M, Lampe FC, Sherr L, Phillips AN, Johnson MA, Gilson R, et al. Non-disclosure of HIV status and associations with psychological factors, ART non-adherence, and viral load non-suppression among people living with HIV in the UK. AIDS Behav. 2017;21(1):184–95.
Acknowledgements
The authors want to thank other team members at University of South Carolina and Guangxi CDC for their efforts in instrument development and data collection and data management.
Funding
The study was supported by National Institutes of Health (NIH) [Grant Nos. R01HD074221, R01AA018090 and R21AI122919] and National Nature Science Foundation of China (NSFC) [Grant No. 71673146]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or NSFC.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no of conflict of interest.
Ethical Approval
The study protocol received review and approval from the Institutional Review Boards at Guangxi CDC in China and Wayne State University in the United States.
Informed Consent
Informed consent was obtained from all participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mi, T., Li, X., Zhou, G. et al. HIV Disclosure to Family Members and Medication Adherence: Role of Social Support and Self-efficacy. AIDS Behav 24, 45–54 (2020). https://doi.org/10.1007/s10461-019-02456-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-019-02456-1