
Abstract
We assessed how egocentric (i.e., self-generated descriptions of a person’s social contacts) network structure and composition corresponded with reported instances of condomless receptive and insertive anal intercourse with men who were reportedly HIV-infected or of unknown HIV serostatus in a sample of black men who have sex with men (MSM) in six U.S. cities. Ratings showing a higher percentage of network members who provided social participation and medical support were positively associated with reporting condomless sex. There were also significant positive associations between stimulant use and condomless insertive and receptive anal sex. Future research should examine the social processes that underlie these associations and explore ways that social support can affect HIV prevention efforts for black MSM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Disparities in HIV infection rates among black men remain severe in the United States despite evidence of a recent reduction in national incidence [1]. Rates of new infections are especially high for black men who have sex with men (MSM), with 2015 surveillance estimates indicating that black MSM accounted for almost 39% of all new HIV infections among MSM [2,3,4,5]. In addition, HIV diagnoses among young black MSM (i.e., ages 13–24) increased 87% between 2005 and 2014 [5]. The HIV Prevention Trials Network (HPTN) 061 study, the largest prospective cohort study among black MSM from six U.S. cities, found a high overall HIV incidence (3.0%) (5.9 percent for young black MSM ≤ 30 years old) [6].
Examining the root causes of this disparity requires not only an exploration of epidemiologic factors that contribute to HIV seroconversion but also of socio-structural factors and individual behaviors that can increase exposure to HIV. For example, systemic factors such as reduced health care access (including HIV prevention and care), socioeconomic challenges, and high levels of unemployment and incarceration have been cited as potential contributors to disproportionate HIV infection rates in black MSM [3, 7]. Similarly, there is evidence that individual factors such as race/ethnicity, level of education, and sexual orientation can link to condomless anal sex, increasing risks for HIV infection [8]. However, previous researchers have also shown that examining individual risk behaviors such as substance use before or during sex use alone does not sufficiently explain HIV infection disparities in black MSM, noting comparative or lower rates of these activities when compared to non-black MSM [5, 9]. The next logical area of inquiry, given that HIV infection is often associated with social and sexual networks, is to examine the social context of sexual behavior through the lens of social networks.
Social networks, comprised of the range of people with whom a person may interact (friends, family members, sex partners) [10] can play a significant role in HIV transmission [3, 7, 11]. As the source of social capital, social support, and behavioral norms, social networks can influence whether a man engages HIV risk behavior [12]. Previous researchers have hypothesized that social support can have a protective effect on health by various pathways including modifying people’s coping mechanisms when faced with stressors, enhancing their problem solving ability, influencing their level of engagement in health behaviors, and helping to provide a sense of individual control over certain situations [13]. Further, the minority stress model describes how stress and stigma can contribute to compulsive sexual behavior and new HIV infections [14], though social support can potentially mitigate this stress [15]. However, there is limited research on how the social context or characteristics of social relationships affect protective or risk-taking behavior among black MSM, or whether there may be differential impact based on the availability of social support [3, 7, 16].
Most social network studies of HIV risk behaviors focus on factors that increase the likelihood of risk behaviors. For example, one study observed that black MSM who had at least one member of their social network condone condomless sexual intercourse had an increased likelihood of engaging in high-risk sexual behavior [4], and the perception that male peers did not think condom use was highly important contributed to condomless anal sex risk in a sample of black and Latino MSM [2]. However, some studies have focused on factors that decrease the likelihood of HIV seroconversion risk. For instance, peer support has been linked to increased HIV testing in young black MSM [17], and a previous study examined how having peer support for safer sex can reduce a person’s likelihood of engaging in condomless sex in young MSM [18]. An additional social network study determined that having peers who regularly went to school or were not heavy drinkers was associated with a decrease in sexual risk behavior in young MSM [19]. Previous research has expanded their studies beyond just enacted support to include perceived support and have shown that perceived emotional and tangible support can contribute to increased regular condom usage in some MSM [20]. Not surprisingly, findings have varied depending on the population studied and may be influenced by the context of the networks in which the study is conducted [21].
We explored how egocentric (i.e., self-generated descriptions of a person’s social contacts) network structure and composition corresponded with reported instances of condomless receptive and insertive anal intercourse with men who were reportedly HIV-infected or of unknown HIV serostatus, behaviors known to have a high risk of seroconversion. The first objective of this study was to explore how network structure and composition may vary between black MSM in the study who did and did not report recent episodes of condomless anal sex. The second objective was to examine which network features might influence HIV-related risk behavior. Our overarching study hypothesis was that increasing levels of personal support within a participant’s network would be associated with a decreased likelihood of condomless anal sex. Learning more about how functional support can impact HIV risk behavior could influence future efforts to develop HIV prevention efforts for Black MSM. Study results could yield insight on the ways social network support may impact HIV risk behavior, which could have implications on how to best utilize network support to disseminate intervention strategies such as PrEP or provide greater clarity on what types of peer networks may be at particularly elevated risk of having members acquire HIV.
Methods
This secondary analysis used data collected between 2009 and 2011 from the HPTN 061 study. Briefly, the HPTN 061 study was designed to “assess the feasibility and acceptability of a multi-component intervention to reduce HIV incidence among Black MSM” [22]. Researchers recruited Black MSM across six U.S. cities (Atlanta, GA, Boston, MA, Los Angeles, CA, New York City, NY, San Francisco, CA, and Washington, D.C.) who were at least 18 years old and reported condomless anal intercourse with a man in the last 6 months [22]. Men entered the study either through two methods: (1) by various site-based community recruitment methods (including print and online advertising, support from local organizations, and the advisement of significant informants) or (2) by being a member of the sexual network of “index participants” who were either unaware of their HIV-infected status, HIV-uninfected, or HIV-infected and having condomless sex with men who were HIV-uninfected or did not know their HIV status [22]. Men enrolled in the study received HIV and STI screening during their baseline assessment and two subsequent follow-up visits (at the 6 and 12 months measurement points). HIV status was confirmed retrospectively at the HPTN Laboratory Center (Baltimore, MD). Study organizers also offered peer health navigators to help participants obtain needed medical or psychosocial services when they were identified at any point during the study participation timeline [22].
Individual Measures and Variables
Individuals described whether they had any instances of condomless insertive or receptive anal intercourse in the past six months based on a dichotomous measure (“yes” or “no”) using an audio computer-assisted self-interview (ACASI) program. ACASI questions also assessed respondents’ alcohol and substance use behavior in the past 6 months (“yes” or “no”) including marijuana, cocaine (both powdered and smoked), and methamphetamine use. Respondents also provided demographic information including age, level of education (“less than high school graduate”, “high school graduate or GED”, or “more than high school level of education”), study site based on the six U.S. city locations, and HIV status (“HIV+”, “HIV−” or “refused HIV testing”) based on study testing results (which included a rapid test followed by confirmatory Western blot testing and subsequent quality assurance to verify HIV infection status at study enrollment).
Social Network Questionnaire
Interviewers administered an in-person social network questionnaire based on a measure validated in a previous study [23] that gathered information on some of each participant’s social contacts. First, interviewers elicited members of a person’s social network by asking men about people who provided them specific types of support (defined below). Men could choose not to list any network members when answering the questionnaire. Respondents would answer these questions and then provide the initials or nicknames of the people who met the stated criteria. After identifying the named persons as members of their social network in the elicitation section of the questionnaire, respondents answered additional questions about each social network member such as the person’s age, gender, race/ethnicity, frequency of communication, and type of relationship.
Study Analysis
Primary Outcomes
The primary outcomes of interest were two dichotomous variables describing whether the study participant had engaged in condomless receptive or insertive anal intercourse (CRAI or CIAI) with male sex partners (primary, most recent, or otherwise classified) who were reportedly living with HIV or who were of unknown HIV status in the past 6 months. Therefore, our results compare individual and network variables between those who did and did not participate in this type of condomless sex during the past 6-month time period. We used two separate outcomes as recent literature has examined how HIV risk perception and one’s ability to negotiate condom usage may differ depending on preferred sex roles in MSM [24]. Because each outcome was measured at both the initial assessment and subsequent follow-up visits, both variables were examined as repeated measures. Approximately 33% of the total number of condomless sex endorsements measured across the study included overlap between the two variables.
Network Measures
Social network size (the total number of named people who provided functional support to the participant as described below) was the sole structural measure available in this data set. Study participants answered whether contacts provided specific forms of social support (i.e., 1. “If you wanted to talk to someone about things that are very personal and private is there anybody you could talk to?” [personal/emotional], 2. “Is there anybody who would go to a medical appointment with you?” [medical], 3. “Is there anybody you know who you would ask to lend you $100 or more if you need it?” [financial], and 4. “Is there anybody that you get together with, spend time talking, relaxing or just hanging out with?” [social participation]). Network members could provide multiple forms of support, which were classified as “personal/emotional”, “medical”, “financial”, and “social participation” support based on the aforementioned social network member criteria and past literature [25].
Network composition measures quantified the amount of network contacts named in the network questionnaire that met certain relationship criteria. We believed that count data for specific network composition questions (support provision, for example) were less effective at accounting for variation in network size in statistical models and less effective at accounting for individual differences in overall network size that lead the value of one person to differ from respondent to respondent (though we have included a version of our analysis using count data in the Appendix). In our opinion, one person providing support to an individual with a network of five people was more important than one person providing support in the network of an individual with a network of fifty people. To reflect this, we chose to use proportions rather than counts in our network statistical models. We also assumed that regardless of how expansive a respondent was they were likely to report networks similar in proportion to their real networks regardless of the overall number of network members they report. This further supported our choice to use proportions in our analyses. This builds on studies of informant accuracy that suggest respondents are more effective at reporting long-term and habitual social interactions than they are at reporting specific interactions [26, 27] and that people’s networks tend to scale up proportionally from those they report [28]. Aside from disciplinary preferences, there are methodological reasons for using proportions. The most frequently used approaches to analyzing egocentric or personal network data use proportions to represent network composition [29, 30]. In multilevel models (MLM) that incorporate network data (e.g., one-to-many dyadic data analysis), it is also recommended that proportions be used to represent network composition at the respondent level. Indeed, most MLM texts would recommend that higher levels should account for lower levels using summary measures (i.e., proportions) of lower level characteristics to make sure that variances are best accounted for [31,32,33,34]. Though our analyses are not multi-level, we believed that these conventions were appropriate and followed them in our analyses.
Statistical Analysis
To assess whether there were significant differences in network measurements between people who did or did not endorse specific sexual risk behaviors during their baseline assessments, we performed non-parametric tests that did not assume a normal distribution for each variable of interest depending on whether it was a continuous (Wilcoxon–Mann–Whitney) or categorical (Kruskal–Wallis) measure. Subsequently, we fitted two mixed-effects logistic regression models to assess the relationship between each outcome (i.e., reported insertive or receptive anal sex with a positive or unknown status partner) as a repeated measure while controlling for clustering of outcomes and within-person variation. We controlled for baseline predictors including reported age, level of education, frequently endorsed substance use categories including alcohol, marijuana, and stimulants [cocaine or methamphetamine] consumed in the past 6 months, study location site, HIV status (biologically confirmed), and structural and compositional network measures. Study participants who reported zero social network members were included in the repeated measure models, though there were no significant differences between models that did or did not include these specific participants.
Results
Out of the total study sample (n = 1553), 1462 people answered questions about individual CIAI or CRAI with men living with HIV or unaware of their HIV status in the past 6 months during their first assessment. The mean age was 37.8 years old (S.D. 11.7) and almost 18% had less than a high school education. The highest percentage of participants came from New York City, NY (20.2%) followed by Atlanta, GA (18.7%), Los Angeles, CA (18.2%), Boston, MA (15.7%), Washington, D.C. (14.0%), and San Francisco, CA (13.2%). While there were no significant differences in education, there were statistically significant differences when comparing additional individual predictors at baseline by age, study location site, HIV status, and stimulant use as shown in Table 1. A greater percentage of men reported CIAI (49.4%) than CRAI (32.3%) with men who were seropositive or did not know their HIV status, and 21.4% of the sample reported both types of sexual activity. In contrast, men who reported CIAI tended to be older (mean age: 39.8 vs. 35.9 years old; p value < 0.0001) and were more likely to be stimulant users (59.1% vs. 40.9%; p-value = 0.0001). There also appeared to be study site differences when examining CIAI, with a lower percentage of men (39.0%) in Washington, D.C. endorsing this sexual activity in the past 6 months. However, there were no significant study site associations for CRAI. People who were HIV-infected reported a higher percentage of CIAI (60.1% vs. 46.1%; p-value = 0.0001) in comparison to people who were HIV-uninfected. In addition to the associations noted above, people who reported CRAI also had a younger mean age (36.7 vs. 38.4 years old; p-value = 0.007) compared to people who did not report this type of sexual activity in the past 6 months. Similar to the CIAI findings, people who were HIV-infected also reported a higher percentage of CRAI (50.6% vs. 26.1%; p-value = 0.0001) compared to people who were HIV-uninfected.
Social network size measures were identical whether men did or did not report CIAI, with identical ranges (0–15), medians (5), and interquartile ranges (3). Only 1.7% of the sample reported zero social network members. With respect to social network composition, men who reported CIAI reported significantly lower mean percentages of network members who provided “personal/emotional” (47.9% vs. 51.3%; p = 0.024). While men who endorsed CRAI had a slightly smaller social network size range (0–14) compared to me who denied this sexual activity (0–15), the medians (5) and interquartile ranges (3) were the same between these two groups. Men who reported CRAI had a significantly higher mean percentage of network members who would attend medical appointments (40.6% vs. 37.2%; p = 0.029).
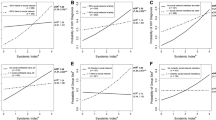
The results of the mixed-effects logistic regression models showed some similar associations when compared to bivariate analyses as seen in Table 2. Increasing age was associated with a lower likelihood of engaging in condomless receptive anal sex (AOR 0.96; 95% CI 0.94–0.97; p-value < 0.0001) while a reverse association was seen with CIAI (AOR 1.01; 95% CI 1.00–1.02; p-value = 0.026). Being located in Los Angeles was also positively associated with CRAI (AOR 1.65; 95% CI 1.04–2.63; p-value = 0.034). Stimulant use increased the odds of reporting both CIAI (AOR 1.58; 95% CI 1.22–2.06; p-value = 0.001) and CRAI (AOR 2.02; 95% CI 1.43–2.86; p-value < 0.0001); reported cannabis use was negatively associated with CRAI but only approached statistical significance (AOR 0.74; 95% CI 0.53–1.02; p-value = 0.066). Compared to people who were HIV-infected, people who were HIV-uninfected were less likely to report either CIAI (AOR 0.51; 95% CI 0.39–0.67; p-value < 0.0001) or CRAI (AOR 0.18; 95% CI 0.13–0.26; p-value < 0.0001).
Social network measures that assessed the availability of social support provided by network members showed significant associations in the multivariate models. For example, having a higher percentage of people who provided social participation support was positively associated with the odds of reporting CIAI (AOR 1.56; 95% CI 1.03–2.38; p-value = 0.037), which differed from bivariate analysis. In addition, having a higher percentage of people who provided medical support led to higher odds of engaging in CRAI (AOR 1.99; 95% CI 1.06–3.72; p-value = 0.031).
Discussion
The overall aim of this study was to examine egocentric network structure and composition related to CRAI and CIAI with men who were HIV-infected or of unknown HIV serostatus among black MSM. While there was some evidence in bivariate analysis that higher proportions of network members that provide personal/emotional support is associated with less reported CIAI, higher levels of social participation and medical support were linked to increased condomless anal sex when controlling for individual characteristics including substance use. While the increasing presence of social support in one’s network could reduce sexual risk behavior by contributing to a greater propensity towards health-promoting behavior, increased knowledge about HIV/STI prevention, or mitigating factors such as stress that can cause people to engage in condomless sex as a compensatory mechanism, these findings suggest that social support could also be linked to increased sexual risk. Reporting a higher percentage of people providing medical support could suggest that a person may be predisposed to poorer physical and/or mental health, and having a greater proportion of social contacts may be linked to a higher propensity to report sexual risk behavior in general. Both of these factors could lead to a higher reporting of condomless sex compared to people with a relative paucity of medical support or social participation network members. It is also possible that having more network members who would be willing to attend medical appointments or socialize with a study participant would increase a person’s propensity to engage in condomless sex due to having increased support for HIV/STI testing or post-exposure prophylaxis (PEP) treatment after a condomless sex event. In addition, HIV-infected men participating in serosorting behavior could have a higher frequency of condomless sex, which could also explain our medical support finding [35, 36]. Similarly, people with more medical network support members may have higher rates of STIs and require increased engagement with health care providers for treatment, which could be the result of increased condomless sex. Future research could expand on these results by using detailed surveys that assess whether receiving support from specific individuals differentially influences risk behavior among black and other MSM of color. Furthermore, examining partner characteristics in greater detail could reveal how factors such as emotional closeness, frequency of contact, age differences, or geographic proximity could influence condomless sex risk and thereby shape behavioral interventions that focus on partner choice and negotiating safer sex practices.
It is also unclear how our findings may relate to geosocial-networking (GSN) smartphone applications (apps), which have become increasingly popular among MSM populations. Recent surveys of app users showed low uptake of pre-exposure prophylaxis (PrEP) despite high awareness of this biomedical intervention [37, 38]. While there is evidence in a recent study that integrating men met through GSN apps into one’s social network contributed to increased condomless anal sex among MSM (and that perceived GSN peer norms in regards to condomless sex may contribute to this risk), there was also an increased likelihood of discussing safer sex practices and HIV testing between study participants and GSN-linked men [39]. Dating apps can potentially facilitate discussions about biomedical prevention and HIV viral suppression [40], and examining the presence of social support in GSN-established communities, especially given the possible overlap between online and in-person networks, may contribute to a greater understanding of condom usage or conversations about HIV risk among men and the sexual partners found through these applications.
While social network composition had important links to condomless sex, it is important to mention those individual predictors that also showed significant associations. In line with previous research, stimulant use was associated with increased odds of condomless sex [41, 42]. Men’s HIV status was also an important factor related to condomless sex, with men who were HIV-uninfected being less likely to report both CIAI or CRAI with men who were HIV-infected or of unknown HIV status compared to men living with HIV. This finding could be consistent with risk reduction strategies in which men who are HIV-infected engage in serosorting behavior while men who are HIV-uninfected are more likely to use condoms to avoid HIV infection [43]. In addition, the association between increasing age and a lower likelihood of reporting condomless receptive sex (and the contrasting association between older age and increased odds of condomless insertive sex) suggests that patterns of sexual risk behavior may change over the course of male sexual development [44, 45]. Potential causes of this association could include increasing sexual education over time, changes in libido, or power/financial dynamics that may contribute to decreased agency in younger MSM for condom use [46]. There may also be role expectations and power dynamics based on age in which older men are more likely to be an insertive anal sex partner compared to younger MSM [47]. Study site was also an important factor, with men located in Los Angeles having a higher propensity of reporting CRAI. Hypotheses for this site association include the possibilities that men recruited in Los Angeles were potentially engaging in more sexual risk behavior or more likely to disclose condomless receptive anal sex than men located at other sites. Further research could explore how regional differences may contribute to sexual risk behavior in black MSM.
There are some limitations to our study. Although we used outcomes as repeated measures, we cannot assess causality directly between our study predictors and condomless sex, and missing predictor data at follow-up visits limited our ability to include time-varying independent variables in our models. These findings are only associations; studies that collect longitudinal data would help us assess causal relationships. While we included HIV status as a predictor, future studies that include the perceived viral load measures of people living with HIV or of men’s sexual partners could provide additional dimensions in regards to sexual risk behavior. In addition, data about PrEP usage was not available given that the timeframe of this study was prior to FDA approval in 2012, so we could not examine how this HIV prevention method could impact men’s condom use. Our study measures also lack granularity about network relationships, which limits our ability to examine behavioral dynamics and processes that underlie social network relationships. Finally, our network measures capture study participants’ perceptions of social support, which may differ from actual support received from network members. Despite these limitations, there are also several study strengths including the large sample size, the specific focus on black MSM, and the multisite study design that contributed to geographical diversity (though study participants might not be representative of all black MSM in the United States).
Conclusions
While our study findings continue to suggest the importance of individual factors in relation to sexual risk behavior, they also highlight important social network effects. More reported social support was associated with increased condomless sex in black MSM when controlling for individual characteristics. Although this study did not explore the mechanisms of how social network support can mitigate or enhance one’s propensity to engage in condomless sex, future research should explore the contexts in which functional support can influence sexual risk in Black MSM either through changing social norms or impacting stress. Given the existing disparities in HIV infection among black MSM, there may be a role for targeting social network support in novel HIV prevention efforts for this population.
References
Hall HI, Song R, Tang T, An Q, Prejean J, Dietz P, et al. HIV trends in the United States: diagnoses and estimated incidence. JMIR Public Health Surveill. 2017;3:e8.
Carlos J-A, Bingham TA, Stueve A, Lauby J, Ayala G, Millett GA, et al. The role of peer support on condom use among Black and Latino MSM in three urban areas. AIDS Educ Prev. 2010;22:430–44.
Koblin BA, Tieu H-V, Frye V. Disparities in HIV/AIDS in black men who have sex with men. Lancet. 2012;380:316–8.
Schneider JA, Cornwell B, Ostrow D, Michaels S, Schumm P, Laumann EO, et al. Network mixing and network influences most linked to HIV infection and risk behavior in the HIV epidemic among black men who have sex with men. Am J Public Health. 2013;103:e28–36.
HIV among African American gay and bisexual men. Centers for Disease Control and Prevention. https://www.cdc.gov/hiv/pdf/group/msm/cdc-hiv-bmsm.pdf. Accessed February 6, 2017.
Koblin BA, Mayer KH, Eshleman SH, Wang L, Mannheimer S, Rio CD, et al. Correlates of HIV acquisition in a cohort of black men who have sex with men in the United States: HIV Prevention Trials Network (HPTN) 061. PLoS ONE. 2013;8:e70413.
Millett GA, Jeffries WL, Peterson JL, Malebranche DJ, Lane T, Flores SA, et al. Common roots: a contextual review of HIV epidemics in black men who have sex with men across the African diaspora. Lancet. 2012;380:411–23.
Halkitis PN, Kapadia F, Siconolfi DE, Moeller RW, Figueroa RP, Barton SC, et al. Individual, psychosocial, and social correlates of unprotected anal intercourse in a new generation of young men who have sex with men in New York City. Am J Public Health. 2013;103:889–95.
Millett GA, Flores SA, Peterson JL, Bakeman R. Explaining disparities in HIV infection among black and white men who have sex with men: a meta-analysis of HIV risk behaviors. AIDS. 2007;21:2083–91.
Neblett RC, Davey-Rothwell M, Chander G, Latkin CA. Social network characteristics and HIV sexual risk behavior among urban African American women. J Urban Health. 2011;88:54–65.
Latkin CA, German D, Vlahov D, Galea S. Neighborhoods and HIV: a social ecological approach to prevention and care. Am Psychol. 2013;68:210–24.
Amirkhanian YA. Social networks, sexual networks and HIV risk in men who have sex with men. Curr HIV/AIDS Rep. 2014;11:81–92.
Heaney CA, Israel BA. Social networks and social support. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education: theory, research, and practice. 3rd ed. San Francisco: Jossey-Bass; 2008.
Dyer TP, Regan R, Wilton L, Harawa NT, Ou SS, Wang L, et al. Differences in substance use, psychosocial characteristics and HIV-related sexual risk behavior between black men who have sex with men only (BMSMO) and black men who have sex with men and women (BMSMW) in six US cities. J Urban Health. 2013;90:1181–93.
Wong CF, Schrager SM, Holloway IW, Meyer IH, Kipke MD. Minority stress experiences and psychological well-being: the impact of support from and connection to social networks within the Los Angeles house and ball communities. Prev Sci. 2014;15:44–55.
Shah NS, Iveniuk J, Muth SQ, Michaels S, Jose J-A, Laumann EO, et al. Structural bridging network position is associated with HIV status in a younger black men who have sex with men epidemic. AIDS Behav. 2014;18:335–45.
Scott HM, Pollack L, Rebchook GM, Huebner DM, Peterson J, Kegeles SM. Peer social support is associated with recent HIV testing among young black men who have sex with men. AIDS Behav. 2014;18:913–20.
Forney JC, Miller RL, The City Project Study Team. Risk and protective factors related to HIV-risk behavior: a comparison between HIV-positive and HIV-negative young men who have sex with men. AIDS Care. 2012;24:544–52.
Tucker JS, Hu J, Golinelli D, Kennedy DP, Green HD Jr, Wenzel SL. Social network and individual correlates of sexual risk behavior among homeless young men who have sex with men. J Adolesc Health. 2012;51:386–92.
Liu H, Feng T, Liu H, Feng H, Cai Y, Rhodes AG, et al. Egocentric networks of Chinese men who have sex with men: network components, condom use norms, and safer sex. AIDS Patient Care STDs. 2009;23:885–93.
Qiao S, Li X, Stanton B. Social support and HIV-related risk behaviors: a systematic review of the global literature. AIDS Behav. 2014;18:419–41.
Mayer KH, Wang L, Koblin B, Mannheimer S, Magnus M, Rio CD, et al. Concomitant socioeconomic, behavioral, and biological factors associated with the disproportionate HIV infection burden among black men who have sex with men in 6 U. S. cities. PLoS ONE. 2014;9:e87298.
Latkin C, Yang C, Tobin K, Roebuck G, Spikes P, Patterson J. Social network predictors of disclosure of MSM behavior and HIV-positive serostatus among African American MSM in Baltimore, Maryland. AIDS Behav. 2012;16:535–42.
Goedel WC, Schneider JA, Hambrick HR, Kreski NT, Morganstein JG, Park SH, et al. Are anal sex roles associated with preferences for pre-exposure prophylaxis administration modalities among men who have sex with men? Arch Sex Behav. 2018;47:2123–33.
Latkin CA, Tieu H, Fields S, Hanscom BS, Connor M, Hanscom B, et al. Social network factors as correlates and predictors of high depressive symptoms among black men who have sex with men in HPTN 061. AIDS Behav. 2017;21:1163–70.
Killworth PD, Bernard HR. Informant accuracy in social network data. Hum Organ. 1976;1976(35):269–86.
Bernard HR, Killworth P, Kronenfeld D, Sailer L. The problem of informant accuracy: the validity of retrospective data. Annu Rev Anthropol. 1984;13:495–517.
Bernard HR, Hallett T, Iovita A, Johnsen EC, Lyerla R, McCarty C, et al. Counting hard-to-count populations: the network scale-up method for public health. Sex Transm Infect. 2016;86:11–5.
Wenzel SL, Green HD, Tucker JS, Golinelli D, Kennedy DP, Ryan G, et al. The social context of homeless women’s alcohol and drug use. Drug Alcohol Depend. 2006;105:16–23.
Nieuwbeerta P, Flap H. Crosscutting social circles and political choice: effects of personal network composition on voting behavior in The Netherlands. Soc Netw. 2000;2000(22):313–35.
Carrington PJ, Scott J, Wasserman S, editors. Models and methods in social network analysis. 1st ed. Cambridge: Cambridge University Press; 2005.
Perry BL, Pescosolido BA, Borgatti SP. Egocentric network analysis: foundations, methods, and models. 1st ed. Cambridge: Cambridge University Press; 2018.
Kashy DA, Kenny DA. Dyadic data analysis using multilevel modeling. In: Hox J, Roberts JK, editors. Handbook of advanced multilevel analysis. 1st ed. New York: Routledge; 2011.
Kenny DA, Kashy DA, Cook WL, editors. Dyadic data analysis. 1st ed. New York: The Guilford Press; 2006.
Margolis AD, Joseph H, Hirshfield S, Chiasson MA, Belcher L, Purcell DW. Anal intercourse without condoms among HIV-positive men who have sex with men recruited from a sexual networking web site, United States. Sex Transm Dis. 2014;41:749–55.
Khosropour CM, Dombrowski JC, Swanson F, Kerani RP, Katz DA, Barbee LA, et al. Trends in serosorting and the association with HIV/STI risk over time among men who have sex with men. J Acquir Immune Defic Syndr. 2016;72:189–97.
Goedel WC, Halkitis PN, Greene RE, Duncan DT. Correlates of awareness of and willingness to use pre-exposure prophylaxis (PrEP) in gay, bisexual, and other men who have sex with men who use geosocial-networking smartphone applications in New York City. AIDS Behav. 2016;20:1435–42.
Goedel WC, Halkitis PN, Greene RE, Hickson DA, Duncan DT. HIV risk behaviors, perceptions, and testing and preexposure prophylaxis (PrEP) awareness/use in Grindr-using men who have sex with men in Atlanta, Georgia. J Assoc Nurses AIDS Care. 2016;27:133–42.
Holloway IW, Pulsipher CA, Gibbs J, Barman-Adhikari A, Rice E. Network influences on the sexual risk behaviors of gay, bisexual and other men who have sex with men using geosocial networking applications. AIDS Behav. 2015;19(Suppl 2):112–22.
Newcomb ME, Mongrella MC, Weis B, McMillen SJ, Mustanski B. Partner disclosure of PrEP use and undetectable viral load on geosocial networking apps: frequency of disclosure and decisions about condomless sex. J Acquir Immune Defic Syndr. 2016;71:200–6.
Mimiaga MJ, Reisner SL, Fontaine Y-M, Bland SE, Driscoll MA, Isenberg D, et al. Walking the line: stimulant use during sex and HIV risk behavior among Black urban MSM. Drug Alcohol Depend. 2010;110:30–7.
Skeer MR, Mimiaga MJ, Mayer KH, O’Cleirigh C, Covahey C, Safren SA. Patterns of substance use among a large urban cohort of HIV-infected men who have sex with men in primary care. AIDS Behav. 2012;16:676–89.
Snowden JM, Wei C, McFarland W, Raymond HF. Prevalence, correlates and trends in seroadaptive behaviours among men who have sex with men from serial cross-sectional surveillance in San Francisco, 2004–2011. Sex Transm Infect. 2014;90:498–504.
Dariotis JK, Sonenstein FL, Gates GJ, Capps R, Astone NM, Pleck JH, et al. Changes in sexual risk behavior as young men transition to adulthood. Perspect Sex Reprod Health. 2008;40:218–25.
Pines HA, Gorbach PM, Weiss RE, Shoptaw S, Landovitz RJ, Javanbakht M, et al. Sexual risk trajectories among MSM in the United States. J Acquir Immune Defic Syndr. 2014;65:579–86.
Newcomb ME, Mustanski B. Developmental change in the effects of sexual partner and relationship characteristics on sexual risk behavior in young men who have sex with men. AIDS Behav. 2016;20:1284–94.
Dangerfield DT, Smith LR, Williams J, Unger J, Bluthenthal R. Sexual positioning among men who have sex with men: a narrative review. Arch Sex Behav. 2016;46:869–84.
Acknowledgements
Keith A. Hermanstyne received support from the UCLA-Robert Wood Johnson Clinical Scholars Program, and Kenneth B. Wells and Nina T. Harawa provided study design feedback and research mentorship on this project.
Funding
Hong-Van Tieu reports that the HPTN 061 study was funded at the New York Blood Center by NIH 1-U01-AI06946. Steven Shoptaw received support via the P30 MH058107 Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Keith A. Hermanstyne declares that he has no conflict of interest. Harold D. Green, Jr. declares that he has no conflict of interest. Hong-Van Tieu has received a research grant from Merck. Christopher Hucks-Ortiz declares that he has no conflict of interest. Leo Wilton declares that he has no conflict of interest. Steven Shoptaw reports grants from the National Institute on Mental Health during the conduct of the study and other support from Medicinova, Inc. outside of the submitted work.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of each institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hermanstyne, K.A., Green, H.D., Tieu, HV. et al. The Association Between Condomless Anal Sex and Social Support Among Black Men Who Have Sex With Men (MSM) in Six U.S. Cities: A Study Using Data from the HIV Prevention Trials Network BROTHERS Study (HPTN 061). AIDS Behav 23, 1387–1395 (2019). https://doi.org/10.1007/s10461-018-2315-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-018-2315-y