
Abstract
We developed an innovative home-based HIV self-testing (HIVST) service that included mailing of a free HIVST kit, and providing online real-time instructions and pre-test/post-test counseling (HIVST-OIC). The present parallel-group and non-blinded randomized controlled trial was conducted to evaluate the efficacy of promoting HIVST-OIC in increasing HIV testing rate among 430 men who have sex with men (MSM), with access to online live-chat applications in Hong Kong. At month 6, as compared to the control group, the intervention group reported significantly higher prevalence of HIV testing of any type (89.8 vs. 50.7%; relative risk (RR): 1.77; p < 0.001). Among those who have taken up any HIV testing in the last six months, significant between-group difference was found in multiple male sex partnerships (34.2 vs. 47.7%, RR: 0.72; p = 0.021). HIVST-OIC has a strong potential in increasing prevalence of HIV testing and reducing sexual risk behaviors. Implementation research is warranted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
HIV testing is one of the four global HIV prevention strategies recommended by the World Health Organization (WHO) [1]. Specifically, the WHO recommends men who have sex with men (MSM) with high risk behaviors take up HIV testing every 6–12 months [2]. The United States Center for Disease Control and Prevention (U.S. CDC) recommends all sexually active MSM get tested every 3–6 months [3]. HIV testing and counseling (HTC) can reduce risk behaviors [4, 5].
HIV testing has become even more important, as antiretroviral treatment (ART) with good adherence can reduce risk of HIV transmission by >90% [6]. The WHO (2015) recommends provision of ART to all people living with HIV (PLWH) [7]. Achievement of the 90–90–90 target (90% detection, 90% on ART, and 90% viral suppression) by 2020 would put HIV under control globally by 2030 [8]; HIV testing rate is a prerequisite to the target [9]. Among MSM in Hong Kong, HIV prevalence increased from 4.08% in 2011 [10] to 5.85% in 2014 [11], but prevalence of HIV testing in the last year only ranged from 24.0 to 40.1% [12, 13]. Only 12.7% of those who had never and 37.2% of those who had ever taken up HIV testing intended to take up HIV testing in the next six months [14, 15]. Improvement is warranted.
HIV self-testing (HIVST) can potentially remove obstacles against HIV testing among MSM (e.g., inconvenience and perceived stigma originated from service providers [16, 17]). The 2014 WHO guideline was supportive of HIVST [18], and a new one for HIVST was recently released in December 2016 [19]. HIVST kits showed high sensitivity and specificity (>99%) [20]. An oral fluid test was approved by the U.S. FDA in 2012 [21]. In Hong Kong, HIVST kits are available at pharmaceutical stores or on the Internet. At least 16 countries (e.g., United Kingdom, U.S., Canada, etc.) also have policies endorsing HIVST [22,23,24,25,26]. There was high acceptability of HIVST among MSM (e.g., 72.8% in mainland China, 80% in the U.S., and 86.5% in France) [27], but prevalence of HIVST use was 17.0 and 26.2% among MSM in the U.S. [28] and mainland China [29]. Among Hong Kong MSM, it was only 3.6 to 6.0% [15, 30]; they usually received HIV testing at non-governmental organizations (NGOs) (45.5%) and governmental clinics (27.9%) [30]. About half of them were willing to take up HIVST [30]; 64.8% would take up HIV testing if given choices in time and venue [12]. It is feasible and warranted to promote HIVST among MSM.
To our knowledge, five single-arm pilot studies tested feasibility of delivering different modes of home-based HIVST services among MSM in China [31] and the U.S. [32,33,34], and transgender women in the U.S. [35]. All studies reported high acceptability of HIVST [31,32,33, 35]. Researchers provided free HIVST kits to users on-site [32, 33, 35] or via mail [33]. Only one randomized controlled trial (RCT) tested the efficacy of supplying HIVST kits in increasing prevalence of overall HIV testing among MSM, and reported higher frequency of HIV testing in the intervention group [36]. One study involved pre-test counseling and optional but delayed post-test counseling through social networking apps [31]. One small pilot of 20 MSM in the U.S. involved real-time instruction, interpretation of testing results, and post-test counseling [34]. There are concerns that HIVST users may skip pre-test/post-test counseling, potentially causing problems in procedures and linkage to care [37]; a review reported that self-testers’ consistently wished for pre-test/post-test counseling in HIVST to be included [37]. Given the wide availability of online live-chat applications and smartphones (96% of Hong Kong population possessed a smartphone) [38], home-based HIVST can be integrated with online counseling.
We developed an innovative home-based HIVST service, which included mailing a free HIVST kit and providing online real-time instructions and pre-test/post-test counseling (HIVST-OIC) via online live-chat applications to users. The HIV testing experience was hence similar to that of HTC offered by many NGOs. Videos were produced to promote HIV testing and HIVST-OIC; audio-visual approach has been used effectively in health promotion programs [39, 40]. Design of health promotion materials was based on perceived benefits and barriers, two constructs of the Health Belief Model (HBM) [41]. We also promoted HIVST-OIC in the intervention group by conducting brief motivational interviewing (MI) over the phone. MI focuses on the individuals’ concerns and perspectives, explores and resolves ambivalence, and moves the person towards change [42]. It is evident that MI, including brief ones of about 15 min, can change various types of health-related behaviors [43,44,45]. It has been used in combination with other intervention components [42, 46]. Thus, evidence-based and theory-based intervention components were used.
The objective of this RCT was to evaluate the relative efficacy of the health promotion between the intervention and control groups in increasing prevalence of overall HIV testing rate (HIV testing of any type) among MSM in Hong Kong within a 6-month follow-up period. In the control group, we promoted traditional HIV testing in general without mentioning HIVST. In the intervention group, in addition to the health promotion received by the control group, we promoted the new HIVST-OIC service through multiple means and provided the HIVST-OIC service to interested participants. Secondary objectives included evaluating between-group differences in prevalence of condomless anal intercourse (CAI) and multiple sex partnerships among testers.
Methods
Study Design
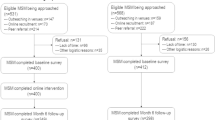
A parallel-group and non-blinded RCT was conducted. Two 10-min telephone surveys were conducted at baseline and six months afterwards by blinded interviewers (See Fig. 1). Up to five calls were made at different timeslots during weekdays/weekends before considering a case as loss-to-follow-up. Additional questions were asked for process evaluation in a telephone survey conducted at Month 3. Information on the clinical trial protocol is available at: https://rfs1.fhb.gov.hk/app/fundedsearch/projectdetail.xhtml?id=1332. We did not register for this trial on other sites. The funding was provided by Health and Medical Research Fund (ref# 11120791), Food and Health Bureau, Hong Kong SAR, China.

Consort flow diagram
Participants
Inclusion criteria were: (1) Hong Kong Chinese speaking males aged ≥18 years old, (2) anal intercourse with ≥1 man in the last six months, (3) willingness to leave contact information (mobile and/or electronic) with us and be followed up at Month 6, (4) access to online live-chat applications (e.g. Line, WhatsApp, and Skype), and (5) no intention to leave Hong Kong for one month consecutively within the next six months. Exclusion criteria were: (1) diagnosed as HIV positive, and (2) HIV testing in the last six months.
Development of the Health Promotion Materials
A panel of three MSM volunteers, two epidemiologists, one psychologist, one health communication expert, two experienced NGO workers and one video producer, was formed. A literature review and a discussion group that involved five MSM were conducted to guide the design of the two videos for promoting HIV testing in general and for promoting HIVST-OIC. The videos were filmed by a professional team, reviewed by three other MSM, and finalized by the panel.
Recruitment Procedures
We recruited participants via outreach in gay-friendly venues (e.g., bars, clubs and saunas), advertisements displayed on websites frequently visited by MSM, and referrals made by the participants. Fieldworkers confirmed eligibility, briefed prospective participants about the study, and assured them anonymity, right to quit at any time, and that refusals would not affect their rights to use any services. Verbal instead of written informed consent was obtained to maintain anonymity, and the fieldworkers signed forms pledging adoption of proper procedures. Upon completion of each of the three surveys and the online health promotion session, a HK $50 (US $8) supermarket coupon was mailed to the participants in plain envelops. Ethics approval was obtained from the institutional Survey and Behavioural Research Ethics Committee and the Clinical Research Ethics Committee.
We approached 857 MSM and invited 583 eligible ones to participate in the study; 430 (73.8%) completed the baseline survey and intervention with informed consent (online: 194; gay venues: 219; participants’ referrals: 17).
The Baseline Survey and Random Allocation Process
Appointments were made to conduct the 10-min baseline telephone survey. After completing the baseline survey, participants were randomized 1:1 to either the intervention group or the control group. Computer-generated randomization allocation codes were produced and sealed in opaque envelopes by a research staff with no involvement in recruitment or baseline survey. One envelope was drawn and opened by the fieldworker. The fieldworker then informed the participant which group he was assigned to. Block randomization with block size of eight was used.
The Control Group
After randomization took place, the control group watched a 3-min online video that promoted HIV testing in general. The contents included: (1) one MSM peer introducing some potential benefits of taking up HIV testing in general, such as it would help to detect HIV infection earlier, increase trust between sex partners and reduce psychological burden, (2) the WHO recommendation for MSM with risk behaviors to take up HIV testing every six months, (3) one MSM peer demonstrating the procedures for HIV testing provided by NGOs, which portrayed caring, supportive, and non-judgmental administrators, regardless of the users’ test results, and (4) a list of such NGOs. Participants were then encouraged to take up HIV testing.
The Intervention Group
Health Promotion Components
-
(1)
In addition to the video shown to the control group, the intervention group watched an online video promoting HIVST-OIC for an additional 4 min. In the video, a local MSM narratively discussed about the benefits and barriers of HIVST-OIC, demonstrated its procedures, and emphasized on availability of immediate online support. Narrative interventions were effective in changing behaviors [47].
-
(2)
Well-trained fieldworkers performed MI for about 15 minutes over the phone to promote HIVST-OIC.
Procedures for Performing HIVST-OIC
-
(1)
Interested participants were mailed a free HIVST kit in a plain envelope. They then made appointments with the fieldworkers to perform HIV testing, based on HIVST-OIC procedures. For those who did not have live-chat application (e.g. Line, WhatsApp, or Skype), the fieldworkers helped them install one and taught them how to use it.
-
(2)
Through video chat, using these live-chat applications, the HIV testing administrator, an experienced registered nurse who was familiar with the sub-culture of local MSM, provided the participants with verbal instructions on how to use the HIVST kit. Standard-of-care pre-test counseling was also provided by the administrators, which took about 10–15 minutes to complete and covered the following topics: (i) knowledge on HIV prevention, (ii) risk assessment, and (iii) an explanation of the procedure and benefits of HIV testing. Participants were guaranteed confidentiality. No recording was made and participants could choose not to show their face during the process.
-
(3)
Participants performed the HIVST, under online and real-time supervision provided by the administrator. It took about 20 minutes to know the test result. Users showed the test result visually to the administrator. Standard-of-care post-test counseling was delivered by the administrator, which lasted for about 15–25 minutes and covered the following topics: (i) explanation of the HIV testing results, (ii) reminders for those who received negative results, about the risk of HIV infection, and assistance for setting up specific goals for consistent condom use, and (iii) psychological support for those who received positive results, and a reminder that they must take up free confirmatory HIV testing provided by the Department of Health.
-
(4)
To ensure linkage, the research staff accompanied participants who received a positive test result to the collaborating NGOs and/or Department of Health, if desired. One HIV positive case was detected. He was immediately counseled by the administrator, confirmed positive at the Department of Health and received proper services.
Fidelity Assessments
The fieldworkers waited on the phone while the participants watched the video (or called back), asked them three simple questions about the video, and recorded the starting/ending time of the MI as verification.
Measures
Outcomes and Confounders
Potential confounders included socio-demographics, sexual orientation, utilization of HIV prevention services, previous testing experience, and anal intercourse with regular male sex partner (RP: defined as those who were in a stable relationship that did not involve transactional sex) and non-regular male sex partner (NRP: defined as men who were not RP and did not involve transactional sex) assessed at baseline. The primary outcome was whether the participant had taken up at least one of the following types of HIV testing within the 6-month follow-up period, including: (i) the HIVST-OIC, (ii) self-purchased HIVST not offered by us, (iii) HIV antibody testing at NGOs, (iv) HIV antibody testing offered by governmental clinics and (v) testing performed at private clinics or private laboratories. The assessment counted testing conducted both locally and overseas. The primary outcome was thus the overall prevalence instead of that limited to the use of HIVST. Secondary outcomes were CAI with men and multiple male sex partnerships in the last three months (among testers only).
Process Evaluation
Process evaluation of health promotion and online implementation of HIVST-OIC was conducted at Month 3. Participants in both groups were asked: (1) whether the content of the health promotion was clear, (2) whether the materials were attractive to them, and (3) whether the health promotion had increased their understanding on the importance of regular HTC and their willingness to take up HIV testing. Participants in the intervention group were asked an additional question about their satisfaction of the MI session.
Users of the HIVST-OIC were asked whether they were satisfied with the logistics of implementation and performance of the HIV testing administrator. They were also asked about the usefulness of the HIVST-OIC in helping them understand HIV testing, preparing them to take up such testing, and reducing their risk behaviors. In the end, they were asked whether they would use HIVST-OIC again under two different cost scenarios (free and HK $100/episode) and recommend it to their peers in the next year.
Sample Size Planning
According to previous data, the prevalence of HIV antibody testing of any type among MSM in Hong Kong in the last year was about 40% [12]. Since we were evaluating the testing rate in the last six months, we hence expected half of the 40% (i.e. 20%) would be tested in the last six months in the absence of intervention, assuming an even distribution as seasonal effect of HIV testing is not apparent. In this study, as participants in the control group were exposed to a simple intervention, we expected the uptake of HIV testing would be higher than 20% and would increase to 25%. The sample size of 150 per group would allow us to detect a between-group difference in the primary outcome of 15% or above (α = 0.05, 2-sided test with statistical power of 0.8; PASS). Taking into account an expected drop-out rate of 30% at month 6 (primary outcome) [48], a sample size of 215 per group was required. The total sample size would be 430.
Statistical Analysis
Baseline between-group differences were compared by using Chi square test. Intention-to-treat analysis was conducted for outcome analyses. Relative risk (RR), absolute risk reduction (ARR) and number needed to treat (NNT) statistics were used to test between-group differences in the binary primary and secondary outcomes assessed at Month 6. Within-group differences were tested by using McNemar test. We used SPSS version 16.0; p values <0.05 were considered as statistically significant.
Results
Descriptive Statistics
Over half of the participants were 18–30 years old (63.1%), currently single (80.7%), had attended university (81.4%), were employed full-time (77.7%), and identified themselves as gay (89.3%). Regarding HIV-related characteristics, 73.0% and 43.3% had had anal intercourse with RP and NRP in the last three months; 44.0 and 38.1% had had multiple male sex partnerships and CAI with men in the last three months, respectively; 84.2% had utilized some HIV-related prevention services in the last six months. Among all participants, 67.2% had taken up HIV testing in the last three years (1–3 episodes: 54.7%; 4–6 episodes: 11.4%; >6 episodes: 1.2%). Only 1.2% had utilized HIVST, while 49.3, 9.3 and 7.7% had used HIV testing services provided by local NGOs, the government hospitals/clinics, and private facilities in the last three years, respectively (Table 1). The baseline differences in all of the aforementioned characteristics between the intervention and control groups were all statistically non-significant (p = 0.32–1.00, see Table 1). Hence, no adjustment was required for subsequent analyses of primary/secondary outcomes.
The loss-to-follow-up rate in the intervention group and the control group was 6.0 and 10.7%, respectively. All except one baseline measurement were non-significant when the two groups were compared (HIV-related prevention service utilization). We do not present results of such comparisons.
Primary Outcome
Participants in the intervention group reported significantly higher prevalence of HIV testing of any type at Month 6 (89.8 vs. 50.7%; RR: 1.77, 95% CI 1.54, 2.03; NNT: 2.56, 95% CI 2.13, 3.20; p < 0.001). Similar significant between-group differences in the primary outcome were detected within subgroups of those with and without CAI, multiple male sex partners, and experience in HIV testing in the last three years (Table 2).
Secondary Outcomes
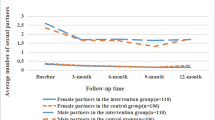
Among those who had taken up HIV testing during the 6-month follow-up period, a significant between-group difference at Month 6 was found in multiple male sex partnerships (intervention: 34.2% vs. control: 47.7%; RR: 0.72, 95% CI 0.54, 0.95; p = 0.021), but not in CAI (intervention: 27.5% vs. control: 33.9%, p = 0.237) (Table 3).
Statistically significant reductions in prevalence of CAI (Month 6 vs. baseline: p = 0.002) and multiple male sex partnerships (Month 6 vs. baseline: p = 0.040) were found within the intervention group but not within the control group (Month 6 vs. baseline; p = 0.078 for CAI and p = 0.327 for multiple male sex partnerships, respectively) (Table 3).
Validation of Primary Outcome for the Intervention Group
At Month 6, self-reported prevalence of taking up HIVST in the intervention and control groups was 87.9 versus 2.3% (p < 0.001). The number of self-reported HIVST in the intervention group was equivalent to that administrated by our staff (both n = 189). Since almost all participants of the intervention group who had taken up HIV testing of any type during the follow-up period had taken up observable HIVST-OIC (189 out of 193), the primary outcome (HIV testing of any type) of the intervention group has been validated.
Other Types of HIV Testing
During the follow-up period, prevalence of HIV testing taken up at NGOs (15.8 vs. 43.7%; p < 0.001), governmental clinics (2.8 vs. 4.7%; p = 0.308), and private settings (1.4 vs. 3.7%; p = 0.127) was reported for the intervention group and the control group. Furthermore, 16.4% of the intervention group had taken up facility-based HIV testing (not HIVST) during the follow-up period.
Process Evaluations (Data Not Given in Tables)
Health Promotion for HIV Testing
Among those in the intervention group (n = 200) and the control group (n = 198) that participated in the process evaluation, 94 and 81.3% believed that the content of the health promotion was clear, respectively. The intervention group was more likely than the control group to find the materials attractive (51.5 vs. 33.4%, p < 0.001), and believed that the health promotion had increased their understanding on the importance of regular HTC (81.0 vs. 69.2%, p = 0.032) and willingness to take up HIV testing (69.0 vs. 43.9%, p < 0.001). In the intervention group, 85% were satisfied with the MI session.
The HIVST-OIC Service
More than 80% of the HIVST-OIC users in the intervention group were satisfied with the logistics of implementation (89.5%), performance of the HIV testing administrator (96.5%), and usefulness of the HIVST-OIC in helping them understand HIV testing (86.7%) and preparing them to take up such testing (80.3%); 71.4% believed the service was effective in reducing their risk behaviors. About 3/4 (78.5 and 75%) expressed a desire to use this service again and would recommend it to their peers in the next year; 47.8% would pay for HIVST-OIC at the cost of HK $100/episode in the next six months.
Fidelity Assessments
All participants were able to answer the questions about the video correctly. The time duration of the MI ranged from 11 to 18 minutes.
Discussion
About nine-tenths (89.8%) of the intervention group’s participants had taken up HIV testing of any type (87.8% for HIVST-OIC) at month 6, representing a large ARR of 39.1%. Participants were at high risk, as 38.1% had had CAI in the last three months. The high efficacy of the intervention group in promoting overall HIV testing, compared to the control group, applied to both those with and without sexual risk behaviors. The ARR for overall testing rate was also very large (>40%) among those who had not taken up HIV testing in the last three years. This group of testers might not use existing testing facilities, but found this new option appealing. HIVST-OIC can hence potentially increase testing rate and reduce risk behaviors among at-risk MSM. As mentioned, the WHO and the U.S. CDC recommend MSM to take up HIV testing on a regular basis [2, 3]. As about 75% of the intervention group indicated that they would like to use HIVST-OIC again in the next year, the new service may also be able to increase the currently low regular HIV testing rate among MSM [14, 15, 49].
The sample characteristics, such as prevalence of CAI (38.1 vs. 39.0%), age (18–30 years old: 63.1 vs. 55.5%), education level (attained university: 81.4 vs. 68.2%) and employment status (employed full-time: 77.7 vs. 74.4%), were comparable to those of other local surveys [49, 50]. Based on these similarities, we contend that applicability of HIVST-OIC can be generalized to local MSM.
About half (50.7%) of participants in the control group had taken up HIV testing at month 6. Since we did not offer the option of HIVST-OIC to them, most of them used the existing types of testing, mainly at NGOs. As compared to the control group, a new option of HIV testing (HIVST-OIC) was offered to the participants in the intervention group. Since this option can remove potential barriers of NGO-based testing such as embarrassment and inconvenience, many users of HIV testing at NGOs might switch to HIVST-OIC. The use of HIVST may potentially substitute the use of traditional HTC offered by NGOs and the government [51]. The substitution could be large if HIVST-OIC becomes widely available.
However, as the between-group difference in overall testing rate was about 40%, a large expansion of testing was also observed on top of substitution. The HIVST-OIC could attract MSM who are not willing to use HIV testing at NGOs. Furthermore, lack of counseling is not an issue as it is part of HIVST-OIC. It is encouraging that the intervention group but not the control group showed significant reductions in risk behaviors, and the statistically significant between-group difference in prevalence of multiple sex partnership favored the intervention group. Given this evidence, NGOs may consider reallocating some of their resources from facility-based HTC service to establish and scale up HIVST-OIC services.
Given the impressive responses in the control group, the online video-based interventions were able to promote both traditional facility-based HTC and HIVST. As MI was offered only to the intervention group and was found effective in changing behaviors [43,44,45], it is possible that it further increased the intervention group’s testing rate. Also, the receipt of the HIVST kit by itself was a very strong cue to action [41]. Previous studies presenting HIVST kit alone were able to increase HIV testing [36, 52]. Similar approaches should be tested in other countries and for other key populations. Future studies may provide a third arm of HIVST-OIC promotion in the absence of MI to better discern effective components. It is a limitation that we could not identify the exact mechanism accounting for the large effect size, but the components of this study can be easily integrated with each other.
Only one HIV positive case was detected among HIVST-OIC users; the HIV prevalence (0.5%) was lower than the reported figure of 5.85% (2014) [11]. Sampling bias may exist but might not be able to explain the large difference, as the background characteristics and prevalence of sexual risk behaviors of the participants were comparable to that of the local MSM [48, 49, 53, 54]. Given the high sensitivity/specificity of the test kit, the false negative rate should be very low. We performed an independent small validation exercise for 20 newly diagnosed HIV positive MSM and 20 HIV negative MSM; accuracy of testing results was 100%. The low prevalence cannot be explained and might be due to randomness.
Strength and Limitation
This study had the strength of an RCT design, innovativeness, low drop-out rate, well validated primary outcome, and good process evaluation results. Since the HIVST kit and the HIVST-OIC service were provided for free and over 96% of Hong Kong people have access to the Internet, we believed the intervention would work well among less a privileged population with fewer resources. Although the HIVST kit was free, resources are involved for future implementation. Currently, local NGOs are also providing free HTC services to users and resources required for HIVST-OIC may be comparable or slightly higher. About half of the HIVST-OIC users indicated that they would use partially funded HIVST-OIC at HK $100/episode. Implementation study may test effectiveness of the new service model under different pricing. Many HIVST services are unsupported or less supported by service providers. The very good outcome of HIVST-OIC justifies additional resources to be allocated to support HIVST, as many existing facility-based HTC services also involve manpower for counseling. Cost-effectiveness analysis and implementation research are warranted.
This study has some limitations. First, a high percentage of the control group self-reported use of facility-based HTC; such responses might have been over-reported due to social desirability. Second, the health promotion was limited to MSM who had access to online live-chat applications. It is justifiable as penetration of smartphone has been increasing sharply in many countries. Third, probability sampling was not feasible for this study in the absence of a sampling frame. Like most RCTs, the participants were recruited by convenient sampling and selection bias was likely. The RCT design ensured good internal validity [55]. However, caution should be exercised when generalizing the results to other Chinese cities. Fourth, we did not collect information on those who refused to participate in the study. Moreover, attrition bias might exist. However, since those who dropped out did not differ from those who were followed up in terms of baseline characteristics, and the attrition rate was low and did not differ between groups (6.0% in the intervention group and 10.7% in the control group), we expected the attrition bias was small. Furthermore, we did not study problems faced with self-test manipulation or unintended harm in this study. Since we provided HIVST-OIC to the users, we did not expect they would not have serious problems related to self-test manipulation (e.g., incorrect procedures due to a lack of clear instructions) or unintended harm (e.g., psychological burden due to misinterpreting a self-test result or due to a lack of linkages to either post-test counseling or treatment). Lastly, it is true that RCT do not allow us to understand the actual preferred mode of HIV testing due to randomization, and how to reach out potential participants for promotion of HIV testing. In the intervention group, we provided post-test counseling to enable participants to interpret the clinical meaning of the testing result correctly, but we did not know about participants’ interpretations of the testing results with reference to their daily life. A future follow-up study should be conducted among those who have used the HIVST-OIC to understand how the process and experience would affect their future choice regarding the mode of HIV testing, ways to reach out the community for promotion of HIVST-OIC, and interpretations of positive and negative testing results.
Conclusion
In sum, the RCT findings show that HIVST-OIC can potentially increase HIV testing rates and reduce sexual risk behaviors among MSM. Users found this new service highly acceptable. It thus has important implications on controlling the HIV epidemic among MSM. Last but not least, it can potentially be used in other key populations and other countries. Local and international dissemination and implementation research are greatly warranted.
References
WHO. Global health sector strategy on HIV/AIDS 2011-2015. 2011. http://www.hoint/hiv/en/.
World Health Organization (WHO), UNAIDS. Guidance on provider-initiated HIV testing and counselling in health facilities. Switzerland. 2007. http://www.who.int/hiv/pub/guidelines/9789241595568_en.pdf.
CfDCaP (CDC). HIV testing among men who have sex with men–21 cities, United States, 2008. MMWR. 2011;60(21):694–9.
Rotheram-Borus MJ, Newman PA, Etzel MA. Effective detection of HIV. J Acquir Immune Defic Syndr. 2000;25(Suppl 2):S105–14.
Hao C, Huan X, Yan H, Yang H, Guan W, Xu X, et al. A randomized controlled trial to evaluate the relative efficacy of enhanced versus standard voluntary counseling and testing on promoting condom use among men who have sex with men in China. AIDS Behav. 2012;16(5):1138–47.
Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410.
World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. 2015. http://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/.
UNAIDS. 90-90-90 An ambitious treatment target to help end the AIDS epidemic. 2014. http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. 2013.
Hong Kong Department of Health. Virtual AIDS office of Hong Kong: HIV surveillance and epidemiology. 2014. www.infogovhk/aids/english/surveillance/aidssurveilhtm.
Virtual AIDS Office of Hong Kong. Press meeting 27 May 2014. 2014. http://www.infogovhk/aids/english/indexhtm.
Gu J, Lau JT, Tsui H. Psychological factors in association with uptake of voluntary counselling and testing for HIV among men who have sex with men in Hong Kong. Public Health. 2011;125(5):275–82.
Wong HTH, Lee SS, Wong KH, Lee KCK. Trends and patterns of HIV prevalence and risk behaviours among MSM captured in three consecutive community-based surveys in Hong Kong. [Abstract]. Presented at 7th IAS Conference on HIV pathogenesis, treatment and prevention. 30 June–July 3, 2013. Kuala Lumpur, Malaysia. 2013. http://pag.ias2013.org/Abstracts.aspx?AID=1235.
Wang Z, Mo PK, Lau JT, Lau M, Lai CH. Acceptability of HPV vaccines and perceptions related to genital warts and penile/anal cancers among men who have sex with men in Hong Kong. Vaccine. 2013;31(41):4675–81.
Gu J, Lau JT, Tan X, Wang Z. Empathy of service providers mediates the association between perceived discrimination and willingness to take up HIV antibody testing again among men who have sex with men. PLos One. 2014.
Nuwaha F, Kabatesi D, Muganwa M, Whalen CC. Factors influencing acceptability of voluntary counselling and testing for HIV in Bushenyi district of Uganda. East Afr Med J. 2002;79(12):626–32.
UTWGoMaHAB. Enabling effective voluntary counselling and testing for men who have sex with men: Increasing the role of community based organizations in scaling up VCT services for MSM in China. Beijing, China: UNDP China and World Health Organization; November 2008. 2008.
World Health Organization, UNAIDS. A short technical update on self-testing for HIV. 2014. http://files.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2014/JC2603_self-testing_en.pdf.
World Health Organization. Guidelines on HIV self-testing and partner notification. Supplement to consolidated guidelines on HIV testing services. 2016. http://www.who.int/hiv/pub/vct/hiv-self-testing-guidelines/en/. Accessed 8 July 2017.
Gottfried TD, Mink RW, Phanuphak P. Calypte AWARE HIV-1/2 OMT antibody test using oral fluid: special challenges of rapid HIV testing in the developing world. Expert Rev Mol Diagn. 2006;6(2):139–44.
FDA. Approval letter—OraQuick In-Home HIV Test. 2012. http://www.fda.gov/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/PremarketApprovalsPMAs/ucm310592.htm.
Pebody R. Market constraints and uncertainties may limit the scale-up of HIV self-testing. 2016. http://www.aidsmap.com/Market-constraints-and-uncertainties-may-limit-the-scale-up-of-HIV-self-testing/page/3073263/.
McDaid LM, Hart GJ. Increased HIV testing and reduced undiagnosed infection among gay men in Scotland, 2005-8: support for the opt-out testing policy? Sex Transm Infect. 2011;87(3):221–4.
Torjesen I. Licensed home tests will be introduced to reduce undiagnosed HIV. BMJ. 2011;343:d7943.
Home HIV. Testing: why not in Canada? CMAJ. 2000;162(11):1545, 7.
Southern African HIV Clinicians Society, Treatment Action Campaign, SECTION27. How we can improve HIV testing and counselling. Society News 2012. http://www.sahivsoc.org/newsroom/society-news.
Figueroa C, Johnson C, Verster A, Baggaley R. Attitudes and acceptability on HIV self-testing among key populations: a literature review. AIDS Behav. 2015;19(11):1949–65.
Hurt CB, Soni K, Miller WC, Hightow-Weidman LB. Human immunodeficiency virus testing practices and interest in self-testing options among young, black men who have sex with men in North Carolina. Sex Transm Dis. 2016;43(9):587–93.
Yan H, Yang H, Raymond HF, Li J, Shi LE, Huan X, et al. Experiences and correlates of HIV self-testing among men who have sex with men in Jiangsu province, China. AIDS Behav. 2015;19(3):485–91.
Wong HT, Tam HY, Chan DP, Lee SS. Usage and acceptability of HIV self-testing in men who have sex with men in Hong Kong. AIDS Behav. 2014.
Tao J, Li MY, Qian HZ, Wang LJ, Zhang Z, Ding HF, et al. Home-based HIV testing for men who have sex with men in China: a novel community-based partnership to complement government programs. PLoS ONE. 2014;9(7):e102812.
Woods WJ, Lippman SA, Agnew E, Carroll S, Binson D. Bathhouse distribution of HIV self-testing kits reaches diverse, high-risk population. AIDS Care. 2016;28(Suppl 1):111–3.
Huang E, Marlin RW, Young SD, Medline A, Klausner JD. Using Grindr, a smartphone social-networking application, to increase hiv self-testing among black and latino men who have sex with men in Los Angeles, 2014. AIDS Educ Prev. 2016;28(4):341–50.
Maksut JL, Eaton LA, Siembida EJ, Driffin DD, Baldwin R. A test of concept study of at-home, self-administered hiv testing with web-based peer counseling via video chat for men who have sex with men. JMIR Public Health Surveill. 2016;2(2):e170.
Lippman SA, Moran L, Sevelius J, Castillo LS, Ventura A, Treves-Kagan S, et al. Acceptability and feasibility of HIV self-testing among transgender women in San Francisco: a mixed methods pilot study. AIDS Behav. 2016;20(4):928–38.
Katz D, Golden M, Hughes J, Farquhar C, Stekler J. HIV self-testing increases HIV testing frequency among high-risk men who have sex with men: a randomized controlled trial. In: IAS 2015. 8th Conference on HIV Pathogenesis, Treatment and Prevention. July 19–22, 2015. Vancouver. Abstract MOPDC0103. 2015.
Pant Pai N, Sharma J, Shivkumar S, Pillay S, Vadnais C, Joseph L, et al. Supervised and unsupervised self-testing for HIV in high- and low-risk populations: a systematic review. PLoS Med. 2013;10(4):e1001414.
Kao E. 96% of Hongkongers use their smartphone to go online everyday. 2013. http://www.scmp.com/news/hong-kong/article/1298330/hong-kong-smartphone-use-doubles-two-years.
Sweat M, O’Donnell C, O’Donnell L. Cost-effectiveness of a brief video-based HIV intervention for African American and Latino sexually transmitted disease clinic clients. AIDS. 2001;15(6):781–7.
Chiasson MA, Shaw FS, Humberstone M, Hirshfield S, Hartel D. Increased HIV disclosure three months after an online video intervention for men who have sex with men (MSM). AIDS Care. 2009;21(9):1081–9.
Janz NK, Becker MH. The Health Belief Model: a decade later. Health Educ Q. 1984;11(1):1–47. http://heb.sagepub.com/content/11/1/1.short.
Miller WR, Rollnick SR. Motivational interviewing: preparing people for change. 2nd ed. New York: The Guilford Press; 2000.
D’Amico EJ, Miles JN, Stern SA, Meredith LS. Brief motivational interviewing for teens at risk of substance use consequences: a randomized pilot study in a primary care clinic. J Subst Abuse Treat. 2008;35(1):53–61.
Bernstein J, Heeren T, Edward E, Dorfman D, Bliss C, Winter M, et al. A brief motivational interview in a pediatric emergency department, plus 10-day telephone follow-up, increases attempts to quit drinking among youth and young adults who screen positive for problematic drinking. Acad Emerg Med. 2010;17(8):890–902.
Macdonell K, Brogan K, Naar-King S, Ellis D, Marshall S. A pilot study of motivational interviewing targeting weight-related behaviors in overweight or obese African American adolescents. J Adolesc Health. 2012;50(2):201–3.
Hettema J, Steele J, Miller WR. Motivational interviewing. Ann Rev Clin Psychol. 2005;1:91–111.
Narrative approaches. http://www.narrativeapproaches.com/?page_id=16.
Lau JT, Lee AL, Tse WS, Mo PK, Fong F, Wang Z, et al. A randomized control trial for evaluating efficacies of two online cognitive interventions with and without fear-appeal imagery approaches in preventing unprotected anal sex among Chinese men who have sex with men. AIDS Behav. 2016.
Lau JT, Wang Z, Lau M, Lai CH. Perceptions of HPV, genital warts, and penile/anal cancer and high-risk sexual behaviors among men who have sex with men in Hong Kong. Arch Sex Behav. 2014;43(4):789–800.
Wong HT, Tam HY, Chan DP, Lee SS. Usage and acceptability of HIV self-testing in men who have sex with men in Hong Kong. AIDS Behav. 2015;19(3):505–15.
Bilardi JE, Walker S, Read T, Prestage G, Chen MY, Guy R, et al. Gay and bisexual men’s views on rapid self-testing for HIV. AIDS Behav. 2013;17(6):2093–9.
Thirumurthy H, Masters S, Obonyo B, Napierala Mavedzenge S, Maman S, Omanga E, Agot K. Promoting male partner and couples HIV testing through secondary distribution HIV self-tests: a randomized trial. Oral presented in AIDS 2016 conference, Durban, South Africa, July 22, 2016. 2016.
Yeo TE, Fung TH. Between ‘0’ and ‘1’: safer sex and condom use among young gay men in Hong Kong. Cult Health Sex. 2016;18(3):294–307.
Lau JT, Mo PK, Gu J, Hao C, Lai CH. Association of situational and environmental factors with last episode of unprotected anal intercourse among MSM in Hong Kong: a case-crossover analysis. AIDS Educ Prev. 2016;28(1):26–42.
Cartwright N. Are RCTs the gold standard? BioSocieties. 2007;2(1):11–20.
Funding
This study was funded by the Health and Medical Research Fund, Food and Health Bureau, Hong Kong Special Administrative Region (Project Ref: #11120791).
Author information
Authors and Affiliations
Contributions
ZW participated in designing the protocol, questionnaires and health promotion materials, managing the data collection, analyzing and interpreting the data, reviewing literature, drafting and revising the manuscript. JTFL participated in conceptualizing the study, designing the protocol and questionnaires, provide scientific and management leadership, interpreting the data, drafting and revising the manuscript critically. MI participated in designing of the health promotion materials, managing the data collection. SH participated in conceptualizing the study, providing comments on the study protocol and health promotion materials, and coordinating the data collection. PM, CL and YM participated in conceptualizing the study and providing comments on the study protocol. YK revised the manuscript critically.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Research Involving Human Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Survey and Behavioural Research Ethics Committee, the Chinese University of Hong Kong and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Wang, Z., Lau, J.T.F., Ip, M. et al. A Randomized Controlled Trial Evaluating Efficacy of Promoting a Home-Based HIV Self-Testing with Online Counseling on Increasing HIV Testing Among Men Who Have Sex with Men. AIDS Behav 22, 190–201 (2018). https://doi.org/10.1007/s10461-017-1887-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-017-1887-2