
Abstract
To better understand patient beliefs, which may influence adherence to HIV care and treatment, we examined three dimensions of beliefs among Ethiopian adults (n = 1177) initiating antiretroviral therapy (ART). Beliefs about benefits of ART/HIV clinical care were largely accurate, but few patients believed in the ability of ART to prevent sexual transmission and many thought Holy Water could cure HIV. Factors associated with lower odds of accurate beliefs included advanced HIV, lack of formal education, and Muslim religion (benefits of ART/clinical care); secondary or university education and more clinic visits (ART to prevent sexual transmission); and pregnancy and Orthodox Christian religion (Holy Water). Assessment of patient beliefs may help providers identify areas needing reinforcement. In this setting, counselors also need to stress the benefits of ART as prevention and that Holy Water should not be used to the exclusion of HIV care and ART.
Resumen
Para entender mejor las creencias de los pacientes que pueden influir su adherencia a los cuidados y tratamiento del VIH, examinamos tres aspectos de creencias en adultos de Etiopia (n = 1,177) al inicio del tratamiento antirretroviral. Las creencias sobre los beneficios del tratamiento y cuidado del VIH fueron en su mayoría correctas, pero muy pocos pacientes creían que el tratamiento antirretroviral puede prevenir la transmisión sexual y muchos creían que el agua bendita podría curar el VIH. Los factores asociados con menor probabilidad de creencias correctas incluyeron el estado avanzado de VIH, falta de educación formal, y la religión musulmana (para creencias sobre los beneficios de cuidado y tratamiento del VIH); educación secundaria o universitaria y más visitas clínicas (para creencias sobre tratamiento y transmisión sexual); y embarazo y religión cristiana ortodoxa (para creencias sobre el agua bendita). La evaluación de las creencias de los pacientes puede ayudar a los clínicos a identificar áreas que necesitan refuerzo. En este caso, los consejeros deben recalcar los beneficios del tratamiento como prevención, y que el agua bendita no debe remplazar el tratamiento antirretroviral.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Successful initiation of antiretroviral treatment (ART) demands acquisition and integration of knowledge, along with adoption of lifelong pill-taking behavior. After treatment initiation, sustained viral load suppression and resulting decreased risk of morbidity, mortality and onward HIV transmission largely depends on patients’ continued engagement in care and adherence to their medication regimen.
Patients’ beliefs regarding HIV can facilitate or hinder treatment. Poor understanding of HIV and effects of ART has been associated with a higher likelihood of non-adherence [1] and dropping out of care both in high-income settings [2–4] and in sub-Saharan Africa [5–8], although some studies report weak or no associations [9–11]. Traditional medicine use, a factor often closely linked to an individual’s belief system, has also emerged as a barrier to ART in the region [12–15]. In Ethiopia, many people believe in the curative potential of Holy Water, whose use has been associated with non-adherence to ART, defaulting from care, and inadequate management of side effects [16–20].
With a population of 96 million and a national HIV prevalence among adults of 1.3 %, Ethiopia has made great strides in scaling up ART since 2005, reaching approximately half of the estimated 590,000 adults living with HIV (PLWH) as of 2013 [21]. However, despite the increased HIV awareness in the country [22, 23], Ethiopians with and without HIV exhibit poorer HIV knowledge than persons in other East African countries [24], which may hinder ART scale-up in Ethiopia.
Because of the potential importance of HIV care and treatment beliefs for treatment uptake, it is important to assess the prevalence and correlates of accurate beliefs among PLWH at the time of ART initiation. Characteristics associated with HIV knowledge and favorable beliefs regarding ART among PLWH in sub-Saharan Africa include older age and higher socioeconomic status (with conflicting findings on the direction of these associations), family support, being married, and having formal education [5, 25, 26]. To date, no published studies have assessed patient beliefs at the critical time of ART initiation or examined correlates of beliefs regarding perceived benefits of HIV treatment, which lie at the core of the health belief model and social cognitive theory [27, 28].
To fill this gap, we aimed to identify sociodemographic and clinical characteristics associated with various HIV beliefs at the time of ART initiation.
Methods
Data Sources and Study Participants
We used data collected for the Multilevel Determinants of Starting ART Late (LSTART) study, where information was obtained from patients initiating ART at six HIV clinics in the Oromia region of Ethiopia. The facilities are part of the Ethiopian National ART Program and are supported by ICAP at Columbia University with funding via President’s Emergency Plan for AIDS Relief (PEPFAR). The sites are secondary health facilities in urban areas, with on-site CD4+ count testing, ART pharmacies, adherence support and peer education programs for both pre-ART and ART patients. All facilities provide HIV care services at least 5 days a week.
Patients ages 18 years and over initiating ART between April 2012 and June 2013 were eligible for the study. Exclusion criteria included overt cognitive impairment, active incarceration, and not speaking Amharic or Oromiffa. On the day of ART initiation, providers referred eligible patients to study staff, who described the study and invited patients to participate, giving them 2 weeks to complete the interview. After obtaining informed consent, study staff administered the 45–60 min structured questionnaire, which assessed HIV care history, status disclosure, HIV beliefs, stigma, and emotional health. Participants received a snack and reimbursement for transportation home from the clinic (20 birr ~1 USD). Additionally, routine clinical information from electronic medical records, dating back to patients’ enrollment in HIV care, was merged with questionnaire data. The participation rate was 95 %. The study was approved by the Institutional Review Boards of the Oromia Regional Health Bureau, Columbia University Medical Center, and the City University of New York.
Measures
HIV Care and Treatment Beliefs
HIV care and treatment beliefs were assessed through 15 questions (Cronbach’s α = 0.70) with response options on a four-point Likert scale ranging from 1, “strongly disagree,” to 4, “strongly agree.” Statements representing a negative outlook towards ART were reverse-scored so that a higher score on each question reflected beliefs favorable to HIV clinical care and ART. We identified three types of beliefs through principal component analysis: benefits of ART and HIV clinical care (α = 0.74 with ten items, e.g. “ARV medicines will not help me live longer”); ART and sexual transmission (α = 0.72 with two items, e.g. “ARV medicines can prevent HIV from being passed between partners during sex”); and the curative potential of Holy Water (α = 0.82 with three items, e.g. “Holy Water healers have cured people with HIV”).
We computed mean scores for each of the three types of beliefs, excluding respondents who had answered fewer than two-thirds of the questions in the respective belief categories. Scores were dichotomized at a mean of 3, with higher scores in each belief dimension (corresponding to “agree” or “strongly agree” on the Likert scale) defined as “accurate beliefs.”
We also examined a single question about prevention of mother-to-child transmission (PMTCT: “ARV medicines will help me/my partner have a baby without HIV”), dichotomized as described above, to provide a fuller picture of patients’ beliefs regarding HIV transmission, both to partner and to child.
Correlates of HIV Care and Treatment Beliefs
Sociodemographic characteristics considered as potential correlates of beliefs included sex, age group, education level, religion, and area of residence.
To assess potential social influences on an individual’s outlook on healthcare, we examined patients’ relationship status and having at least one close friend (as a proxy for social capital). Because parents and pregnant women may be exposed to more HIV messaging through their experiences in healthcare and social settings, having ever had children and pregnancy status at ART initiation were also examined. Pregnancy and sex were combined into a single variable with three categories: men, pregnant women, and non-pregnant women.
Health- and HIV-related factors included history of using Holy Water or traditional treatments (e.g. herbs, prayer) as a putative cure for HIV, year of HIV diagnosis (2008 and before, 2009–2011, and 2012–2013, to account for a possible cohort effect due to the evolving HIV care system), and disease stage at ART initiation (early, CD4 > 350 or WHO stage 1 or 2; moderate, 200 < CD4 ≤ 350 or WHO stage 3; and advanced, CD4 ≤ 200 or WHO stage 4). We examined the total number of clinic visits since enrollment in care as a proxy for cumulative opportunity for exposure to health messaging through counseling. This variable was analyzed instead of time since enrollment in care (r = 0.80) because each visit represents an opportunity for health education, whereas duration in care would not account for long gaps between visits experienced by many patients.
Due to a change in the questionnaire design early in the study, a group of respondents was not asked about Holy Water use for HIV. Multiple imputation was conducted to impute values for patients missing this variable (n = 147), area of residence or having had children (both n ≤ 4). Sensitivity analyses excluding these individuals were conducted.
Statistical Methods
We compared the characteristics of women and men using χ2 tests for categorical variables and Mann–Whitney U tests for continuous variables. We conducted logistic regression analyses to examine the influence of various factors on HIV care and treatment beliefs, using separate models for each of the three dichotomized composite belief variables. Bivariate associations were examined through simple logistic regression, using χ2 tests of statistical significance (p < 0.05). Multivariable models initially included all variables with bivariate p values <0.20, except the period of diagnosis, which could not be included simultaneously with the number of clinic visits due to high correlation (r = 0.66). Covariates were eliminated through backward stepwise regression until all remaining variables had p values <0.05. Finally, variables with bivariate p values >0.05 were added individually back to this model to rule out the possibility of negative confounding. Sex, age group, and number of clinic visits were retained in all multivariable models in order to produce sex- and age-adjusted odds ratios and allow for an assessment of the possible impact of repeated health education on patients’ beliefs.
Analyses were conducted in SAS 9.3 (Cary, NC) using generalized linear models with generalized estimating equations to account for clustering of observations within clinical sites.
Results
Of 1182 participants, we excluded one for a missing clinic visit history and four due to “other” religious affiliations (which we were unable to categorize), for a final analytic sample of 1177 respondents. Sixty-six participants (6 %, largely persons without education) were further excluded from analyses of ART and sexual transmission beliefs and 46 (4 %)—from Holy Water beliefs, due to not answering at least two-thirds of the questions composing these variables. Among the 1177 participants, 61 % were women, 70 % were Ethiopian Orthodox, and 78 % resided in urban areas. The median age was 34 years (interquartile range [IQR] 28–40), and participants had a median of 3 months since enrollment in HIV care (IQR 0.5–30.9 months). Women were on average younger than men (median age 30 vs. 37, p < 0.001) and more likely to have no education (39 vs. 20 %, p < 0.001). Women also had a longer median time since enrollment in care than men (5.8 vs. 1.1 months, p < 0.001) (Table 1).
HIV Care and Treatment Beliefs
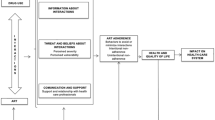
Participants showed greater accuracy in the beliefs about benefits of ART/clinical care and Holy Water than for ART and sexual transmission (mean scores of 3.3 and 3.0, respectively, vs. 2.0, p < 0.001). In comparison with other participants, pregnant women had a lower mean score on Holy Water beliefs (2.7), but scored highest of all groups on ART and sexual transmission (mean = 2.2). Overall, 90 % of respondents had accurate beliefs on benefits of ART/clinical care, 13 %—on ART and sexual transmission, and 67 %—on Holy Water (Fig. 1). Additionally, 78 % of patients endorsed the statement supporting the effectiveness of ART for PMTCT. The results of bivariate analyses of factors associated with the three main belief types are shown in Table 2.

Distribution of HIV care and treatment beliefs by sex and pregnancy status
Multivariable Analyses
Beliefs Regarding Benefits of ART/Clinical Care
Urban residence (vs. rural, aOR 1.94, 95 % CI 1.14–3.29) and university education (vs. primary/other, aOR 9.48, 95 % CI 1.45–61.84) were independently associated with higher odds of accurate beliefs. Respondents who had no education (aOR 0.64, 95 % CI 0.54–0.75), were Muslim (vs. Ethiopian Orthodox, aOR 0.48, 95 % CI 0.35–0.66) and had advanced HIV at ART initiation (vs. moderate, aOR 0.44, 95 % CI 0.22–0.86) had lower odds of accurate beliefs in this dimension (Table 3).
Beliefs Regarding ART and Sexual Transmission
Increasing level of education was associated with lower odds of accurate beliefs (aOR 0.60, 95 % CI 0.45–0.79 for secondary, and aOR 0.29, 95 % CI 0.13–0.64 for university vs. primary/other education). The odds of accurate sexual transmission beliefs decreased as the cumulative number of HIV clinic visits increased (aOR for 4–8 vs. 2–3 visits: 0.45, 95 % CI 0.28–0.71).
Beliefs Regarding Holy Water
The odds of accurate Holy Water beliefs were higher for respondents with university education (vs. primary/other, aOR 1.47, 95 % CI 1.08–2.00), those who ever had children (vs. no children, aOR 1.40, 95 % CI 1.13–1.74), and persons with only one clinic visit prior to ART initiation (vs. 2–3 visits, aOR 2.74, 95 % CI 1.60–4.67). Lower odds of accurate Holy Water beliefs were found for participants with history of Holy Water use for HIV (vs. no traditional treatment, aOR 0.28, 95 % CI 0.16–0.50), Orthodox Christians (vs. other Christians, aOR 0.23, 95 % CI 0.11–0.49), and pregnant women (vs. men, aOR 0.29, 95 % CI 0.16–0.53).
The results of sensitivity analyses excluding respondents with imputed data were consistent with the above findings (Data not shown).
Discussion
In a diverse population of patients initiating ART, most respondents held accurate beliefs regarding benefits of ART/clinical care and Holy Water, but the majority were not aware of prevention of sexual HIV transmission through ART, even though most understood that ART can prevent vertical transmission of HIV. Presence of inaccurate beliefs among many patients successfully engaged in HIV care and initiating treatment suggests that gaps may be even wider among individuals in the earlier stages of the care continuum, especially ones not yet linked to care or not diagnosed.
The direction of associations with examined correlates, especially education, varied across beliefs, underscoring the complexity of belief systems related to health. There were no consistent patterns of association between the number of clinic visits prior to ART initiation (a proxy for opportunity for exposure to health education) and HIV care and treatment beliefs. Although we found higher odds of accurate beliefs about Holy Water among those with only one clinic visit (largely those recently enrolled in HIV care), there was no evidence of a corresponding decline in odds among those with more clinic visits. The odds of accurate ART and sexual transmission beliefs were lower with increased number of clinic visits, which, combined with the bivariate association between recent HIV diagnosis and higher odds of accurate beliefs, suggests that patients enrolled in care in earlier years may not have been adequately targeted with recent messaging emphasizing treatment as prevention [29].
We were unable to assess the content or quality of clinic visits, which may be a better measure of exposure to health messaging than the proxy used in our study (number of clinic visits prior to ART initiation). In addition, HIV education may not be emphasized as much after the initial clinic visits [30]. Conversely, although moderate repetition of a message may increase its perceived validity and recall, excessive repetition may also render it tedious and less effective [31]. A Ugandan study found that additional pre-ART counseling had no impact on subsequent adherence or viremia [32], highlighting the need for better understanding of health education approaches, as well as other sources of information (e.g. mass media) and encouragement for patients starting lifelong treatment.
Although participant sex was not associated with beliefs, pregnant women were less likely to have accurate beliefs regarding Holy Water than men, even after adjusting for age and education. Previous research has found higher rates of defaulting from HIV care [33] and declines in ART adherence during the perinatal and post-delivery periods [34–36], which has been attributed to conflicting priorities of new mothers, less interaction with the healthcare system post-delivery, and postpartum depression [37]. Our finding may suggest that even before delivery, pregnant women’s belief in the need for long-term HIV care and treatment may be undercut by the belief in the curative power of Holy Water. Pursuit of such cure may detract time and resources from clinical HIV treatment, as some patients travel great distances to receive Holy Water [38]. Religious and cultural practices external to the health care system, such as blessing newborns with Holy Water and its use as a fertility aid [39–42], may contribute to the disproportionately positive attitude towards Holy Water in this subgroup. It is unclear, however, why a possible positive effect of (past) pregnancy on favorable Holy Water beliefs does not manifest itself, or is overshadowed by other factors such as trust in clinical medicine gained through greater cumulative interaction with the healthcare system, among parents in the sample.
History of past Holy Water use for HIV was associated with a lower likelihood of accurate beliefs about Holy Water. Despite failing to be cured by this method and turning to clinical medicine, some patients maintained positive views on Holy Water at ART initiation, and may turn to it again, increasing the risk of subsequent non-retention in care or poor ART adherence [17, 18]. Even accounting for the use of Holy Water, Orthodox Christians were less likely than other Christians to have accurate beliefs about Holy Water, as expected due to its common use among Orthodox Christians in Ethiopia [43]. Following the 2007 endorsement of combined ART and Holy Water use for HIV by the Ethiopian Orthodox Church [44], the benefits and use of ART should be reinforced by continued dialogue between health officials and spiritual leaders and direct interventions such as introduction of health or social workers at major Holy Water sites [38].
Muslim respondents were less likely to have accurate beliefs about benefits of ART/clinical care; a finding requiring further investigation. This result might reflect lower penetration of HIV-related information within the Muslim community or lower health-seeking behavior [45], possibly associated with concerns about ingestion of medication during the fasting month of Ramadan, when meal and sleeping times are altered [20, 46].
We found complex associations between education and beliefs, suggesting that poor literacy and knowledge of basic science may hinder understanding the benefits of biomedical HIV treatment, or that providers communicate such information more effectively to patients with higher educational attainment. In contrast, with low accuracy levels in this dimension, provider messaging about prevention of sexual transmission through ART appears to be generally inadequate and/or ineffective. Furthermore, some patients or providers may avoid discussing, or may not be adequately prepared to discuss intimate topics, possibly due to discomfort. Providers’ messages about sexual health may also be affected by their moral judgments, such as concerns about promiscuity and a desire not to encourage risky behavior [47]. Some providers may prefer to emphasize condoms as a tool for both prevention of sexual HIV transmission and family planning. Notably, a broader understanding of PMTCT and the recency of emphasis on treatment as prevention of transmission to partner, compared with prevention of vertical transmission [29], indicate that, by the time of ART initiation, many patients may not have received or internalized messages regarding the preventative effect of ART on sexual transmission of HIV.
Finally, participants in the advanced stages of HIV infection were less likely to have accurate beliefs regarding benefits of ART/clinical care. When severely ill patients arrive at the clinic in need of immediate treatment, there may not be enough time for comprehensive health messaging. Furthermore, serious symptoms may affect these patients’ ability to absorb new information. Individuals with advanced disease may have delayed testing, care seeking or ART initiation due to negative or conflicting beliefs regarding benefits of ART/clinical care or may be pessimistic about their prognosis. Such patients might benefit from additional encouragement and health education, perhaps from peer educators with similar experiences.
The study’s strengths include enhanced generalizability to other patients initiating ART in the region due to the high participation rate across multiple clinics throughout Oromia and availability of patient-reported and clinic data, allowing us to examine sociodemographic and HIV care-related factors. The analysis provides a richer perspective on potential barriers and facilitators to positive treatment outcomes through assessment of beliefs specifically at ART initiation. Importantly, in contrast to other studies [5, 25, 26], we conceptualized patient beliefs as multifaceted and assessed them in three separate dimensions, although we were constrained by pre-defined variables to construct them. Thus, these belief dimensions may not be applicable to other patient populations and should be explored further in other settings. Other weaknesses include lack of questions about combining ART with Holy Water and lack of data on exposure to other sources of information, such as mass media. Finally, the cross-sectional nature of the analysis limits our ability to make causal inferences (belief could influence a behavior such as health seeking, rather than the other way around).
Conclusions
Patients’ beliefs about ART and sexual transmission and the use of Holy Water for HIV are often inaccurate at ART initiation, which may place them at risk for delayed treatment initiation, future ART non-adherence or disengagement from HIV care. Low accuracy of beliefs about ART and sexual transmission indicates that the message of treatment as prevention needs to be emphasized among both new and existing patients. Patient subgroups including pregnant women, Orthodox Christians and Muslims, patients with advanced HIV or long delays between enrollment in care and ART initiation, should be targeted for additional or alternative health education and comprehension assessments during clinic visits. Collaboration with community and religious leaders should be expanded as a means of delivering HIV education in a sensitive and effective manner.
References
Langebeek N, Gisolf EH, Reiss P, Vervoort SC, Hafsteinsdottir TB, Richter C, et al. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: a meta-analysis. BMC Med. 2014;12:142.
Godin G, Cote J, Naccache H, Lambert LD, Trottier S. Prediction of adherence to antiretroviral therapy: a one-year longitudinal study. AIDS Care. 2005;17(4):493–504.
Grierson J, Koelmeyer RL, Smith A, Pitts M. Adherence to antiretroviral therapy: factors independently associated with reported difficulty taking antiretroviral therapy in a national sample of HIV-positive Australians. HIV Med. 2011;12(9):562–9.
Kerr T, Palepu A, Barness G, Walsh J, Hogg R, Montaner J, et al. Psychosocial determinants of adherence to highly active antiretroviral therapy among injection drug users in Vancouver. Antivir Ther. 2004;9(3):407s–14s.
Boateng D, Kwapong GD, Agyei-Baffour P. Knowledge, perception about antiretroviral therapy (ART) and prevention of mother-to-child-transmission (PMTCT) and adherence to ART among HIV positive women in the Ashanti Region, Ghana: a cross-sectional study. BMC Women’s Health. 2013;13:2.
Gourlay A, Birdthistle I, Mburu G, Iorpenda K, Wringe A. Barriers and facilitating factors to the uptake of antiretroviral drugs for prevention of mother-to-child transmission of HIV in sub-Saharan Africa: a systematic review. J Int AIDS Soc. 2013;16(1):18588.
Lifson AR, Demissie W, Tadesse A, Ketema K, May R, Yakob B, et al. Barriers to retention in care as perceived by persons living with HIV in rural Ethiopia: focus group results and recommended strategies. J Int Assoc Provid AIDS Care. 2013;12(1):32–8.
Muhamadi L, Nsabagasani X, Tumwesigye MN, Wabwire-Mangen F, Ekstrom AM, Peterson S, et al. Inadequate pre-antiretroviral care, stock-out of antiretroviral drugs and stigma: policy challenges/bottlenecks to the new WHO recommendations for earlier initiation of antiretroviral therapy (CD < 350 cells/microL) in eastern Uganda. Health Policy (Amsterdam, Netherlands). 2010;97(2–3):187–94.
Ammassari A, Trotta MP, Murri R, Castelli F, Narciso P, Noto P, et al. Correlates and predictors of adherence to highly active antiretroviral therapy: overview of published literature. J Acquir Immune Defic Syndr (1999). 2002;31(Suppl 3):S123–7.
Duff P, Kipp W, Wild TC, Rubaale T, Okech-Ojony J. Barriers to accessing highly active antiretroviral therapy by HIV-positive women attending an antenatal clinic in a regional hospital in western Uganda. J Int AIDS Soc. 2010;13:37.
Negash T, Ehlers V. Personal Factors Influencing Patients’ Adherence to ART in Addis Ababa, Ethiopia. J Assoc Nurses AIDS Care. 2013;24:530–8.
Namuddu B, Kalyango JN, Karamagi C, Mudiope P, Sumba S, Kalende H, et al. Prevalence and factors associated with traditional herbal medicine use among patients on highly active antiretroviral therapy in Uganda. BMC Public Health. 2011;11:855.
Nyika A. Ethical and regulatory issues surrounding African traditional medicine in the context of HIV/AIDS. Developing World Bioeth. 2007;7(1):25–34.
Peltzer K, Friend-du Preez N, Ramlagan S, Fomundam H, Anderson J. Traditional complementary and alternative medicine and antiretroviral treatment adherence among HIV patients in Kwazulu-Natal, South Africa. Afr J Tradit Complement Altern Med. 2010;7(2):125–37.
Peltzer K, Preez NF, Ramlagan S, Fomundam H, Anderson J, Chanetsa L. Antiretrovirals and the use of traditional, complementary and alternative medicine by HIV patients in Kwazulu-Natal, South Africa: a longitudinal study. Afr J Tradit Complement Altern Med. 2011;8(4):337–45.
Abdella SH, Wabe NT, Yesuf EA. Management of common adverse effects in the era of highly active antiretroviral therapy in south east Ethiopia. North Am J Med Sci. 2011;3(11):499–502.
Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K. Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health. 2008;8:265.
Balcha TT, Jeppsson A, Bekele A. Barriers to antiretroviral treatment in ethiopia: a qualitative study. J Int Assoc Physicians AIDS Care (Chic Ill: 2002). 2011;10(2):119–25.
Deribe K, Hailekiros F, Biadgilign S, Amberbir A, Beyene BK. Defaulters from antiretroviral treatment in Jimma University Specialized Hospital, Southwest Ethiopia. Trop Med Int Health. 2008;13(3):328–33.
Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM, Bimirew MA, Kassie DM. Barriers and facilitators of adherence to antiretroviral drug therapy and retention in care among adult HIV-positive patients: a qualitative study from Ethiopia. PLoS ONE. 2014;9(5):e97353.
Joint United Nations Programme on HIV/AIDS (UNAIDS). Global report: UNAIDS report on the global AIDS epidemic 2013. Geneva: 2013 978-92-9253-032-7.
Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International, 2012.
Suzuki C, Mishra V, Govindasamy P, Hong R, Gu Y. Recent trends in hiv-related knowledge and behavior in Ethiopia, 2000-2005: further analysis of the 2000 and 2005 Ethiopia Demographic and Health Surveys. Calverton: Macro International Inc.; 2008.
ICF International. HIV/AIDS in Ethiopia: data from the 2011 Ethiopia demographic and health survey. Calverton: ICF International; 2012.
Nachega JB, Lehman DA, Hlatshwayo D, Mothopeng R, Chaisson RE, Karstaedt AS. HIV/AIDS and antiretroviral treatment knowledge, attitudes, beliefs, and practices in HIV-infected adults in Soweto, South Africa. J Acquir Immune Defic Syndr (1990). 2005;38(2):196–201.
Nozaki I, Kuriyama M, Manyepa P, Zyambo MK, Kakimoto K, Barnighausen T. False beliefs about ART effectiveness, side effects and the consequences of non-retention and non-adherence among ART patients in Livingstone, Zambia. AIDS Behav. 2013;17(1):122–6.
Bandura A. Social foundations of thought and action. Englewood Cliffs: Prentice Hall; 1986.
Strecher VJ, Rosenstock IM. The health belief model. Cambridge handbook of psychology, health and medicine. Cambridge: Cambridge University Press; 1997.
Cohen MS, Holmes C, Padian N, Wolf M, Hirnschall G, Lo YR, et al. HIV treatment as prevention: how scientific discovery occurred and translated rapidly into policy for the global response. Health Aff (Project Hope). 2012;31(7):1439–49.
Kulkarni S, Hoffman S, Gadisa T, Melaku Z, Fantehun M, Yigzaw M, et al. Identifying perceived barriers along the HIV care continuum: findings from providers, peer educators, and observations of provider-patient interactions in Ethiopia. J Int Assoc Provid AIDS Care. 2015. doi:10.1177/2325957415593635.
Reinhard M-A, Schindler S, Raabe V, Stahlberg D, Messner M. Less is sometimes more: how repetition of an antismoking advertisement affects attitudes toward smoking and source credibility. Soc Influ. 2014;9(2):116–32.
Siedner MJ, Lankowski A, Haberer JE, Kembabazi A, Emenyonu N, Tsai AC, et al. Rethinking the “pre” in pre-therapy counseling: no benefit of additional visits prior to therapy on adherence or viremia in Ugandans initiating ARVs. PLoS ONE. 2012;7(6):e39894.
Pati R, Lahuerta M, Elul B, Okamura M, Alvim MF, Schackman B, et al. Factors associated with loss to clinic among HIV patients not yet known to be eligible for antiretroviral therapy (ART) in Mozambique. J Int AIDS Soc. 2013;16:18490.
Mirkuzie AH, Hinderaker SG, Sisay MM, Moland KM, Morkve O. Current status of medication adherence and infant follow up in the prevention of mother to child HIV transmission programme in Addis Ababa: a cohort study. J Int AIDS Soc. 2011;14:50.
Nachega JB, Uthman OA, Anderson J, Peltzer K, Wampold S, Cotton MF, et al. Adherence to antiretroviral therapy during and after pregnancy in low-income, middle-income, and high-income countries: a systematic review and meta-analysis. AIDS (London, England). 2012;26(16):2039–52.
Gwynn RC, Fawzy A, Viho I, Wu Y, Abrams EJ, Nash D. Risk factors for loss to follow-up prior to ART initiation among patients enrolling in HIV care with CD4+ cell count >/ 0 cells/muL in the multi-country MTCT-Plus initiative. BMC Health serv Res. 2015;15:247.
Boyles TH, Wilkinson LS, Leisegang R, Maartens G. Factors influencing retention in care after starting antiretroviral therapy in a rural South African programme. PLoS ONE. 2011;6(5):e19201.
Berhanu Z. Holy water as an intervention for HIV/AIDS in Ethiopia. J HIV/AIDS Soc Serv. 2010;9(3):240–60.
Anderson L. Faith as a means of healing: traditional medicine and the Ethiopian Orthodox Church in and around Lalibela. Independent Study Project (ISP) collection. Paper 128. 2007. http://digitalcollections.sit.edu/isp_collection/128.
Giel R, Gezahegn Y, van Luijk JN. Faith-healing and spirit-possession in Ghion, Ethiopia. Soc Sci Med (1967). 1988;2(1):63–79.
Sisay MM, Yirgu R, Gobezayehu AG, Sibley LM. A qualitative study of attitudes and values surrounding stillbirth and neonatal mortality among grandmothers, mothers, and unmarried girls in rural Amhara and Oromiya regions, Ethiopia: unheard souls in the backyard. J Midwifery Womens Health. 2014;59(s1):S110–S7.
Warren C. Care of the newborn: community perceptions and health seeking behavior. Ethiop J Health Dev. 2010;24(1):110–4.
Kassaye KD, Amberbir A, Getachew B, Mussema Y. A historical overview of traditional medicine practices and policy in Ethiopia. Ethiop J Health Dev. 2007;20(2):127–34.
IRIN Humanitarian News & Analysis. Ethiopia: Church endorses ‘holy water’ and ARVs as people flock to miracle mountain 2007 [07/10/2014]. http://www.irinnews.org/report/72375/ethiopia-church-endorses-holy-water-and-arvs-as-people-flock-to-miracle-mountain.
Woldemicael G, Tenkorang EY. Women’s autonomy and maternal health-seeking behavior in Ethiopia. Matern Child Health J. 2010;14(6):988–98.
Yakasai AM, Muhammad H, Babashani M, Jumare J, Abdulmumini M, Habib AG. Once-daily antiretroviral therapy among treatment-experienced Muslim patients fasting for the month of Ramadan. Trop Doct. 2011;41(4):233–5.
Both R, Samuel F. Keeping silent about emergency contraceptives in Addis Ababa: a qualitative study among young people, service providers, and key stakeholders. BMC Women’s Health. 2014;14(1):134.
Acknowledgments
This study was funded by a grant from NIH R01 (5R01MH89831) entitled “Multi-level determinants of late ART initiation in sub-Saharan Africa” (LSTART) and the President’s Emergency Plan for AIDS Relief (PEPFAR).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tymejczyk, O., Hoffman, S., Kulkarni, S.G. et al. HIV Care and Treatment Beliefs among Patients Initiating Antiretroviral Treatment (ART) in Oromia, Ethiopia. AIDS Behav 20, 998–1008 (2016). https://doi.org/10.1007/s10461-015-1184-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-015-1184-x