
Abstract
China faces a growing HIV epidemic; psychosocial needs of HIV-positive individuals remain largely unaddressed. Research is needed to consider the gap between need for mental healthcare and lack of sufficiently trained professionals, in a culturally acceptable manner. This study assessed explicit and implicit forms of social support and mental health symptoms in 120 HIV-positive Chinese. Explicit social support refers to interactions involving active disclosure and discussion of problems and request for assistance, whereas implicit social support refers to the emotional comfort one obtains from social networks without disclosing problems. We hypothesized and found using multiple linear regression, that after controlling for demographics, only implicit, but not explicit social support positively predicted mental health. Future research is warranted on the effects of utilizing implicit social support to bolster mental health, which has the potential to circumvent the issues of both high stigma and low professional resources in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
AIDS is a global pandemic, with 33 million people now living with HIV/AIDS (PLWHA) [1]. PLWHA have widely been documented to be at increased risk for mental health problems such as depression, suicidality, and substance abuse [2–5]. It is important to know which factors are helpful to PLWHA in coping with the distress of having HIV.
Within the United States, social support, as defined by the perception that one is loved and cared for, esteemed and valued, and part of a network of communication and mutual obligations [6], has been found to be helpful with coping and adjusting to stress by acting as a buffer against adverse mental and physical health effects of stress. Specifically in HIV-positive populations in the US, social support is associated with increased self-esteem [7], decreased depression [8], and decreased perceived HIV-related stigma [9].
Outside the West, however, there is less research on the psychological aspects of HIV. In China, despite the increasing HIV epidemic, mental health needs are seldom the focus of treatment and care. In 2009, an estimated 26,000 people died from AIDS in China, causing it to be the leading cause of death among infectious diseases for the first time in the country’s history [1, 10]. The government has made considerable progress in addressing the medical aspect of the epidemic (e.g., the Four Frees and One Care program has made HIV medication free and widely available [11]). However, the mental health aspects of PLWHA have received less attention and research. This is understandable, given the relative lack of mental health resources. Indeed, in China, there is approximately one certified psychologist per every 80,000 people, as estimated by the Chinese Society of Psychiatry [12]. In contrast to approximately one psychologist for every 1800 individuals in the United States for reference [13], this low availability of trained mental health professionals presents a significant challenge in the effort to consider viable options to meet the mental health needs of Chinese individuals affected by HIV.
A reliably recommended resource for addressing mental health needs of HIV-positive individuals in the West is accessing social support networks, based on studies showing that increased social support is associated with improvement in psychological wellbeing (e.g., overall quality of life and depression [14–16]). However, less is known about the effects of social support in HIV-positive populations in China. The only known quantitative study about the direct relationship between social support and mental health among PLWHA in China, by Sun et al. [17] found, paradoxically, that while participants reported moderately high levels of social support (as measured by the perceived social support scale), they continued to report high psychological distress (measured by the symptom checklist SCL-90). Literature on social support from the field of social psychology suggests a possible explanation for what may appear to be a contradiction. Many researchers have documented cultural differences in social support seeking. In the US, Asian Americans appear to utilize less social support than European Americans [18, 19]. Similarly, cross-national studies comparing samples of European American with Chinese [20], Korean [21], and Japanese [22] participants found that European Americans seek more social support. Kim et al. [23] hypothesized that a primary reason why this discrepancy exists may be an artifact of the methodology used in the studies. Specifically, the studies assessed only explicit seeking and receiving of social support, which involve active disclosure and discussion of problems as well as request for assistance, and can take the form of advice, instrumental aid, or emotional comfort recruited from social networks [24].
In contrast, other studies that include implicit social support have suggested that implicit social support use may be more beneficial for Asians and Asian Americans compared to European Americans. Implicit social support is defined as the emotional comfort one obtains from social networks without disclosing specifics of the stressful event, such as enjoying pleasant activities together or being in the company of close others without discussing problems [23]. For example, Kim et al. [21] conducted a daily diary study with college students in Korea and the US, in which participants recorded their daily stressors, social supports accessed, and mood and life satisfaction. The results demonstrated that Korean students reported using implicit social support to a greater extent than European Americans. Furthermore, among Koreans, both implicit and explicit support predicted better wellbeing while only explicit support was predictive for European Americans. In another study distinguishing between forms of social support, Taylor and colleagues [24] conducted the trier social stress task [25] with Asian American and European American participants who were provided both explicit and implicit social support, and assessed physiological stress indicators such as heart rate, blood pressure, and salivary cortisol levels. They found that Asians and Asian Americans benefited more both psychologically and biologically from implicit social support than explicit social support, while the reverse was true for European Americans. Furthermore, surprisingly, among Asians and Asian Americans, mobilizing explicit social support actually exacerbated their emotional and biological distress.
Researchers [24, 26, 27] have theorized that in cultures valuing interdependent harmony, such as China, soliciting social support may be perceived as disrupting social networks and has the potential to negatively affect relationships. In such collectivistic cultures where relationships involve social obligation [28], members may be less likely to recruit social support due to interdependent relationship concerns [21]. Indeed, these findings provide evidence for cultural differences in the utility of various forms of social support and suggest that culturally specific matching of explicit or implicit support may lead to better outcomes.
Therefore, in an effort to consider innovative strategies to address the gap between the low availability of professional mental healthcare providers and the high need for psychosocial support among Chinese PLWHA, we sought to understand how social support operates in this population. Specifically, we predict that implicit social support will be associated with better mental health outcomes, while explicit social support will not significantly predict better mental health outcomes among Chinese PLWHA.
Methods
Participants and Procedures
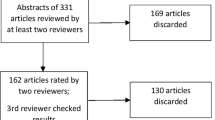
The study was conducted in China at Beijing Ditan Hospital, a premier AIDS treatment facility affiliated with Capital Medical University. The present study is a secondary data analysis of all survey data collected between December 2006 and April 2008 as part of an efficacy trial of a nurse-delivered HIV medication adherence intervention [29]. Eligible participants were HIV-positive, Mandarin-speaking adults over age 18, receiving care at Ditan Hospital; individuals who were cognitively impaired or actively psychotic were excluded. Upon providing written informed consent, participants completed an hour-long interviewer-administered survey for which they were reimbursed RMB100 (approximately $12 USD). All study procedures were approved by the Institutional Review Boards of the University of Washington, Ditan Hospital, and the China Center for Disease Control.
Demographic characteristics of the final sample are presented in Table 1. Among the total sample of 120 participants, 81.7 % were male with a mean age of 36.3 years (SD = 8.0; range 20.1–54.5). Participants’ primary methods of HIV transmission included having sex with men who have sex with men (MSM)—43.3 %, selling blood—18.3 %, having sex with commercial sex workers—16.7 %, and blood transfusions—15.0 %.
Measures
Sociodemographic Variables
Sociodemographic variables assessed were sex, age, marital status, sex of sexual partner, education, employment, and annual household income. Participants also reported their HIV transmission route and most recent CD4 count.
Social Support
Social support was assessed using a Chinese adaptation [30] of the Medical Outcome Study-Social Support Scale (MOS-SSS), a psychometrically validated multidimensional measure for perceived social support of patients with chronic disease [31]. The survey assesses perceived availability of support (“How many times in the last 3 months have the following types of support been available to you if you need it?”) with a five-point scale from 0 (none of the time) to 5 (all of the time). It includes four subscales: (1) emotional/informational support (eight items; e.g., someone to offer advice, guidance, and feedback, someone to listen to you when you need to talk); (2) tangible support (four items; e.g., someone to take you to the doctor, someone to help with daily chores if you are sick); (3) affectionate support (three items; e.g., someone to love you and make you feel wanted, someone to hug you); and (4) positive social interaction (four items; e.g., someone to have a good time with, someone to get together with for relaxation). According to Kim et al.’s [23] conceptualization of explicit and implicit social support, explicit social support characterizes the first two subscales, because in order to receive emotional/informational or tangible social support, one typically has to explicitly disclose the nature of the problem and directly ask for assistance. In other words, in the domain of emotional/informational support, to receive advice or guidance for a problem, explicit disclosure of the problem is likely necessary. Similarly, obtaining tangible support of rides to the doctor or help when one is sick, for example, requires some disclosure that one is in fact sick. In contrast, social support in the forms of physical affection or positive social interaction is termed implicit, as it is obtainable without direct disclosure of a problem. Specifically, receiving physical affection or sharing enjoyable activities together does not presuppose active disclosure of a problem.
The original English version of the MOS-SSS had internal consistency of α > .91 for each subscale in the norming sample of N = 2987 patients with chronic conditions in the US [31]. Using our sample and Chinese translation of the scale, Cronbach’s alphas were as follows: emotional/informational support subscale: α = .81, tangible support subscale: α = .79, affectionate support subscale: α = .49, and positive social interaction subscale: α = .84. Due to low reliability [32] in the affectionate support subscale, it was not used in subsequent analyses. Upon inspection of the survey instrument, translation errors were found in the affectionate support items, which explained the low reliability of the subscales. Therefore, explicit social support subscales included the original two domains of emotional/informational support and tangible support, while implicit social support was represented with only the positive social interaction subscale, leaving out the affectionate subscale. Future research using the Chinese MOS-SSS will benefit from re-translating, back-translating, and psychometric validation of the affectionate subscale in order to have an additional measure of implicit social support.
Mental Health Indicators
Depressive Symptoms
A previously validated and abbreviated Chinese version of the Center for Epidemiological Studies Depression Scale (CES-D 10-item) routinely used as a screening measure to examine prevalence of psychological distress in community samples was used to assess depressive symptoms [33]. Aggregate scores range from 0 to 30, with a threshold of 10 or above indicating presence of possible clinical depression. Cronbach’s alpha in our sample was α = .77.
Anxiety Symptoms
Anxiety symptoms were assessed using the Substance Abuse and Mental Illness Screener, a non-diagnostic screener validated in HIV-positive patients for which positive screening requires further psychiatric evaluation [34]. Anxiety symptoms assessed included those indicating presence (categorical; yes or no) of possible panic attacks, generalized anxiety disorder, and post-traumatic stress disorder. Total scores ranged from 0 (no positive screen) to 6 (all symptoms endorsed). Reliability is typically not assessed with this scale, as the separate anxiety symptoms are not necessarily expected to hang together.
Quality of Life and General Mental Health Summary Score
Quality of life and the general mental health summary score was assessed using the Medical Outcomes Study-HIV (MOS-HIV) survey [35, 36], a psychometrically validated measure to assess dimensions of health. The MOS-HIV health survey contains 35 questions and is used worldwide to assess quality of life in PLWHA. The raw item scores of each subscale are summed and transformed into a total score ranging from 0 to 100, where higher scores indicate better health. Cronbach’s alpha in our sample for quality of life was α = .72 and for general mental health was α = .74.
Results
Preliminary Analyses
Skew and kurtosis were examined for all variables of interest. Assumptions of parametric data were met, prompting no further corrections. The mean, standard deviations, and ranges of the main variables are presented in Table 2. On the brief 10-item CES-D, 54.2 % of the sample obtained a score of 10 or above, indicating the presence of “significant depressive symptomatology”. Furthermore, 30.8 % of the sample screened positive for generalized anxiety disorder, and 42.9 % screened positive for panic attacks. Participants’ mean quality of life and mental health summary scores were 48.7 and 44.2, respectively, out of a possible 100. For social support, participants most commonly endorsed that they perceived availability “some of the time” for each of the 18 items, with a normal distribution of endorsement of other answer options.
Based on independent samples t-tests, perceptions of availability of social support (all subscales) were not significantly different for married versus non-married (including single, widowed, and divorced) participants. Social support subscales were also not significantly associated with sex of sexual partners and most recent CD4 count. The only significant association present between route of transmission and social support is that participants who acquired HIV via having sex with a man who has sex with men were less likely to have perceived tangible social support (r = −.21, p < .05).
Bivariate Correlations
Bivariate correlations between variables of interest are included in Table 2. As expected, the three subscales of social support (i.e., emotional support, tangible support, and positive social interaction) were significantly inter-correlated, as were the measures of mental health (i.e., anxiety, depressive symptomatology, quality of life, and the mental health summary score); p’s < .01). Interestingly, while two items measuring socio-economic status (education and income) were significantly correlated, employment was not correlated with the others. This could possibly be due to the high unemployment rate in this Chinese sample, where compromised physical health and fear of stigma may inhibit full engagement in the workplace.
Multivariate Analyses
Four separate hierarchical multiple linear regression analyses were run, one for each of the four mental health outcomes. In each regression, the first step included age, gender, income, education, and employment, and the second step included the three social support subscales entered separately.
As seen in Table 3, all four F tests of overall fit with both levels of predictors entered were statistically significant at the p < .05 level at least. Specifically, for: (1) depressive symptomatology, F(3, 111) = 5.58, p < .001; (2) anxiety, F(3, 111) = 2.86, p < .05; (3) quality of life, F(3, 111) = 2.84, p < .05; and (4) mental health summary score, F(3, 111) = 3.97, p < .01. In terms of individual parameters, as hypothesized, the social support subscale of positive social interaction emerged as a unique predictor accounting for variance in mental health indicators. Specifically, for depressive symptomatology, the social support subscale of positive social interaction emerged as a significant predictor of less symptomatology, t(119) = −3.39, p < .001 above and beyond the variance accounted for by age, gender, income, education, and employment. Furthermore, as hypothesized, the two other social support subscales of emotional support and tangible support were not significant predictors. A similar pattern emerged for the other mental health indicators of anxiety, quality of life, and the mental health summary score, with positive social interaction accounting for more variance than the other social support subscales in the expected directions (less anxiety, better quality of life, and higher mental health), although only trending towards statistical significance: anxiety (p = .06), quality of life (p = .07), and mental health summary score (p = .08).
Discussion
In one of the few studies examining behavioral aspects of HIV in China, we found that among a sample of HIV-positive outpatients in Beijing, implicit social support (defined as emotional comfort obtained from social networks without active disclosure of problems) was more strongly related to mental health than explicit social support (which does require disclosure and discussion of problems). Specifically, a series of multiple linear regressions indicated, as hypothesized, that implicit social support in the form of positive social interaction emerged as a reliable predictor of variance in the mental health outcomes of depressive symptomatology, anxiety, quality of life, and a summary score of mental health, while the two types of explicit social support (emotional/informational and tangible support) did not. These results indicate potential for harnessing positive social interactions with others as a way to reduce stress for HIV-positive Chinese individuals.
Our findings are theoretically aligned with emerging research on social support among Asian and Asian American populations, where less social support is explicitly sought and utilized, compared to European American populations [18, 19, 21, 23]. Additionally, Asian and Asian American participants appeared to benefit more from implicit social support that does not require active disclosure, and may in fact be further distressed by activating disclosure-dependent explicit social support [24].
Our findings are encouraging and particularly relevant for implications for future intervention for Chinese HIV-positive individuals, as China is a high HIV-related stigma setting [37] with low availability of mental health resources [12]. Indeed, a 2008 survey of more than 6000 urban Chinese residents on their attitudes toward HIV found that 48 % of respondents indicated they would not eat with someone who had HIV, and 30 % thought that children with HIV should not be allowed to attend the same schools as uninfected children [38]. In this setting of high stigma, a cross-sectional secondary data analysis of HIV outpatients in Beijing found, promisingly, that perceived social support (aggregated social support not distinguished between implicit and explicit) mediated the impact of stigma on depression and quality of life, suggesting that social support may be an important target of intervention for highly stigmatized Chinese PLWHA [39].
Given the climate of HIV-relate stigma, overall rates of self-disclosure of HIV status are understandably low. While we could not find population-representative studies of disclosure rates in China, small-scale and population-specific studies, such as one by Ko et al. [40] of 105 PLWHA in Taiwan (a culturally similar country), reported a mean disclosure rate of 27 % to all identified persons. Disclosure rates reported by studies vary widely, as some query whether disclosure to anyone has ever occurred, while others ask questions that are more open-ended about whom PLWHA have disclosed to, such as partners, family members, or close friends. With our current sample, we asked, “Do any of the people in your household know your HIV status”, with 16 % of respondents answering “No”, 26 %—“Some know”, and 41 %—“All know”. Other studies have identified PLWHA’s concerns about disclosure, including anticipated and experienced negative impact of HIV disclosure, such as being ostracized by their neighbors, kicked out of their villages of residence, fired from work, and causing psychological burden [41, 42]. In summary, much fewer than half of HIV-positive individuals have fully disclosed their HIV status to their friends and family, likely due to potentially negative consequences, suggesting that seeking explicit social support for needs related to HIV may be particularly difficult, as they would have to disclose the nature of their request and distress.
Furthermore, China is a low mental health resource setting, whose HIV-positive population would greatly benefit from efforts to shift provision of psychosocial assistance from scarce professionals to more readily available peers, friends, and family. Low rates of disclosure mean that seeking explicit forms of social support to assist in HIV-related distress would be more difficult as well as potentially less rewarding due to possible ramifications of disclosure. These anticipated consequences of disclosure range from fearing stigma both from and for the disclosure recipients (e.g., due to family association to the HIV-positive individual) to causing psychological burden for the recipients [41]. This may explain the seemingly perplexing findings by Sun et al. [17] as discussed in the introduction, where a sample of HIV-positive participants in China reported both moderately high levels of social support and concurrent high psychological distress. This study used the Perceived Social Support scale, which only measures explicit and not implicit social support. Therefore, our findings suggesting that implicit social support predicts better mental health outcomes are encouraging in that a non-disclosure-dependent form of social support will be more palatable and practical in such a high stigma setting. Additionally, several studies of Chinese PWLHA have demonstrated that patients who have family/caregiver support report improved anti-retroviral medication adherence, which is associated with better quality of life and overall wellbeing [43–45]. A large proportion of participants in the studies did not have family/caregiver support however, as they had not disclosed their HIV status to their family. Given that support behaviors in the studies ranged from providing patients with financial assistance, to reminding them to take their medication, to spending quality time with them, it may be useful to consider the potential positive impact of garnering just implicit social support on medication adherence for those patients who do not currently feel able to disclose. Future research may be warranted that systematically addresses the effects of implicit social support such as increasing positive social interactions of relaxing and doing enjoyable and fun things with members in one’s social network, on improving wellbeing for HIV-positive Chinese patients.
There are several limitations to the present study. First, the small sample of N = 120 was a convenience sample, collected at Ditan Hospital in Beijing, which is a premier infectious disease hospital in the country. While a wide representation of residence was found in the sample, as HIV-positive individuals in China often have to travel to major cities in order to receive healthcare, the sample likely represents those who have the physical resources to be in the capital city. Furthermore, significant differences in mental health and social support have been found between rural and city dwellers [17]; thus it is recommended that the analyses be replicated with a more nationally representative sample of HIV-positive individuals. Additionally, as the present study involved secondary data analysis of a cross-sectional survey, we cannot infer causality. Finally, although the measures used were psychometrically validated in English, as demonstrated by the low reliability in social support subscale, more psychometric studies need to be conducted on the Mandarin versions of the scales. Given that we were unable to analyze the affectionate support subscale, another measure of implicit social support, future research is needed to seek to replicate these findings with the additional form of implicit social support.
Despite these limitations, our findings should provide an impetus to further investigate the specificity of efficacy of social support for certain populations who are in need of distress reduction. There is a long history of research on social support indicating its ability to buffer against adverse mental and physical effects of stress. However, which specific aspects of social support are useful (and not detrimental) for specific cultural groups with unique constellations of problems, warrants further investigation. Additionally, once specific modalities of support are delineated, research is necessary on how to capitalize on the pathways, for example training HIV-positive peers to provide social support [46].
Better understanding the mechanisms of social support will allow for targeted intervention recommendations when considering the specific needs of a population, which will lead to a better likelihood of success and improved outcomes, especially for those like HIV-positive Chinese individuals living in a socio-cultural context of high stigma and few mental health resources.
References
United Nations Programme on HIV/AIDS (UNAIDS). Report on the global AIDS epidemic. Geneva: UNAIDS, 2010.
Stoskopf C, Kim YK, Glover SH. Dual diagnosis: HIV and mental illness, a population-based study. Community Ment Health J. 2001;37(6):469–79.
Jin H, Hamptom-Atkinson J, Heaton R, et al. Depression and suicidality in HIV/AIDS in China. J Affect Disord. 2006;94(1–3):269–75.
Klinkenberg WD, Sacks S. Mental disorders and drug abuse in persons living with HIV/AIDS. AIDS Care. 2004;16(Suppl 1):S22–42.
Leserman J. Role of depression, stress, and trauma in HIV disease progression. Psychosom Med. 2008;70(5):539–45.
Cobb S. Social support as a moderator of life stress. Psychosom Med. 1976;38:300–14.
Zea MC, Reisen CA, Poppen PJ, Biachi FT, Echeverry JJ. Disclosure of HIV status and psychological well-being among Latino gay and bisexual men. AIDS Behav. 2005;9(1):15–26.
Remien RH, Exner T, Kertzner RM, et al. Depressive symptomatology among HIV-positive women in the era of HAART: a stress and coping model. Am J Community Psychol. 2006;38(3–4):275–85.
Galvan FH, Davis EM, Banks D, Bing EG. HIV stigma and social support among African Americans. AIDS Patient Care STDs. 2008;22(5):423–36.
McGivering J. AIDS takes deadly toll in China. BBC News. 2009. http://news.bbc.co.uk/2/hi/asia-pacific/7896133.stm. Accessed 1 May 2014.
Zhang F, Dou Z, Ma Y, et al. Five-year outcomes of the China national free antiretroviral treatment program. Ann Intern Med. 2009;151(4):241–51.
Mental health in China: And now the 50-minute hour. The Economist. 2007. http://www.economist.com/node/9657086?story_id=9657086. Accessed 1 May 2014.
United States Bureau of Labor Statistics. Occupational Outlook Handbook: Psychology. 2010. http://www.bls.gov/ooh/Life-Physical-and-Social-Science/Psychologists.htm. Accessed 1 May 2014.
Folkman S, Cheesney M, Pollack L, Coates T. Stress, coping and depressive mood in HIV-positive and negative gay men in San Francisco. J Nerv Ment Dis. 1993;181(7):409–16.
Green G. Editorial review: social support and HIV. AIDS Care. 1993;5(1):87–104.
Friedland J, Renwick R, McColl M. Coping and social support as determinants of quality of life in HIV/AIDS. AIDS Care. 1996;8(1):15–31.
Sun H, Zhang J, Fu X. Psychological status, coping, and social support of people living with HIV/AIDS in central China. Public Health Nurs. 2007;24(2):132–40.
Sasaki J and Kim HS. Cultural differences in daily effects of religious coping. Poster session presented at: Annual Meeting of the Society for Personality and Social Psychology; 2008; Albuquerque, NM.
Taylor SE, Sherman DK, Kim HS, Jarcho J, Takagi K, Dunagan MS. Culture and social support: who seeks it and why? J Pers Soc Psychol. 2004;87(3):354–62.
Chu TQ, Kim HS, and Sherman DK. Culture and the perceptions of implicit and explicit social support use. Poster session presented at: Annual Meeting of the Society for Personality and Social Psychology; 2008; Albuquerque, NM.
Kim HS, Sherman DK, Chu TQ et al. Culture and social support in daily life. Manuscript in preparation; 2008; as cited in Kim HS, Sherman DK, and Taylor SE. Culture and social support. Am Psychol 2008;63(6):518–26.
Hashimoto T, Imada T, Kitayama S. Support seeking in Japan and US: Perspective from daily support and professional help. Proceedings of the 71st conference of the Japanese Psychological Association; 2007; Tokyo: Tokyo University.
Kim HS, Sherman DK, Taylor SE. Culture and social support. Am Psychol. 2008;63(6):518–26.
Taylor SE, Welch WT, Kim HS, Sherman DK. Cultural differences in the impact of social support on psychological and biological stress responses. Psychol Sci. 2007;18(9):831–7.
Kirschbaum C, Pirke KM, Hellhammer DH. The ‘trier social stress test: a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology. 1993;28(1–2):76–81.
Wang S, Shih JH, Hu A, Louie JY, Lau AS. Cultural differences in daily support experiences. Cultur Divers Ethnic Minor Psychol. 2010;16(3):413–20.
Kim HS, Sherman DK, Ko D, Taylor SE. Pursuit of comfort and pursuit of harmony: culture, relationships, and social support seeking. Pers Soc Psychol Bull. 2006;32(12):1595–607.
Adams G, Plaut VC. The cultural grounding of personal relationship: friendship in North American and West African worlds. Pers Relatsh. 2003;10(3):333–47.
Simoni JM, Chen WT, Huh D, et al. A preliminary randomized controlled trial of a nurse-delivered medication adherence intervention among HIV-positive outpatients initiating antiretroviral therapy in Beijing, China. AIDS Behav. 2011;15(5):919–29.
Yu DSF, Lee DTF, Woo J. Psychometric testing of the Chinese version of the Medical Outcomes Study Social Support Survey (MOS-SSS-C). Res Nurs Health. 2004;27(2):135–43.
Sherbourne CD, Stewart AL. The MOS Social Support Survey. Soc Sci Med. 1991;32(6):705–14.
Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334.
Dai Y, Zhang S, Yamamoto J, et al. Cognitive behavioral therapy of minor depressive symptoms in elderly Chinese Americans: a pilot study. Comm Ment Health J. 1999;35(6):537–42.
Pence BW, Gaynes BN, Whetten K, Eron JJ Jr, Ryder RW, Miller WC. Validation of a brief screening instrument for substance abuse and mental illness in HIV-positive patients. JAIDS. 2005;40(4):434–44.
Wachtel T, Piette J, Mor V, Stein M, Fleishman J, Carpenter C. Quality of life in persons with human immunodeficiency virus infection: measurement by the Medical Outcomes Study Instrument. Ann Int Med. 1992;116(2):129–37.
Wu AW, Hays RD, Kelly S, Malitz F, Bozzette SA. Applications of the Medical Outcomes Study health-related quality of life measures in HIV/AIDS. Qual Life Res. 1997;6(6):531–54.
Burki TK. Discrimination against people with HIV persists in China. Lancet. 2011;377(9762):286–7.
China AIDS Media Partnership and UNAIDS. AIDS-related knowledge, attitudes, behavior, and practices: A survey of 6 Chinese cities. 2008. http://www.unaids.org.cn/uploadfiles/20081118143056.pdf. Accessed 1 May 2014.
Rao D, Chen WT, Pearson CR, et al. Social support mediates the relationship between HIV stigma and depression/quality of life among people living with HIV in Beijing, China. Int J STD AIDS. 2012;23(7):481–4.
Ko NY, Lee HC, Hsu ST, Wang WL, Huang MC, Ko WC. Differences in HIV disclosure by modes of transmission in Taiwanese families. AIDS Care. 2007;19(6):791–8.
Yang JP, Xie TY, Shiu CS, et al. A model of Chinese parental HIV disclosure. AIDS and Behavior; Under review.
Simoni JM, Yang JP, Shiu CS et al. A preliminary randomized controlled trial of a parental HIV disclosure support intervention in China. AIDS (in press).
Fredriksen-Goldsen K, Shiu CS, Starks H, et al. “You must take the medications for you and for me”: family caregivers promoting HIV medication adherence in China. AIDS Patient Care STDs. 2011;25(12):735–41.
Shiu CS, Chen WT, Simoni JM, Fredriksen-Goldsen K, Zhang F, Zhou H. The Chinese Life-Steps Program: a cultural adaptation of a cognitive behavioral intervention to enhance HIV medication adherence. Cogn Behav Pract. 2013;20(2):202–12.
World Heath Organization (WHO). Adherence to long term therapies—evidence for action. 2003. http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Accessed 10 Mar 2015.
Simoni JM, Nelson KM, Franks JC, et al. Are peer interventions for HIV efficacious? A systematic review. AIDS & Behav. 2011;15:1589–95.
Acknowledgments
We gratefully acknowledge the participants and providers at Ditan Hospital for their assistance with the Project. Additionally, we would like to thank Kimberly M. Nelson, Rick Cruz, Jennifer Wang, Karen Pang, Laura Brady, and Karen Chang for their revisions on earlier drafts of the manuscript. Funding for this research was provided by the National Institute of Mental Health (NIMH: 1F31MH099925-01, Yang, PI; MH074364, Simoni, PI;), and the University of Washington Center for AIDS Research (CFAR), an NIH-funded Program [P30AI27757].
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yang, J.P., Leu, J., Simoni, J.M. et al. “Please Don’t Make Me Ask for Help”: Implicit Social Support and Mental Health in Chinese Individuals Living with HIV. AIDS Behav 19, 1501–1509 (2015). https://doi.org/10.1007/s10461-015-1041-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-015-1041-y