
Abstract
We conducted a systematic review of couple-based HIV biobehavioral (skills-building, VCT, and adherence) and biomedical (ART, circumcision) prevention and intervention studies designed to reduce sexual- and drug-risk behaviors and HIV transmission and acquisition. Of the 11,162 papers identified in the search, 93 peer-reviewed papers met the inclusion criteria and yielded a total of 33 studies conducted globally. Biobehavioral couple-based prevention and intervention studies have been efficacious in reducing sexual- and drug-risk behaviors, increasing access to HIV testing and care, and improving adherence. Biomedical couple-based studies were found to reduce HIV incidence among HIV-negative sex partners and viral load among HIV-positive partners. Despite much progress, couple-based HIV prevention and intervention studies remain limited; a number of methodological gaps exist and studies focusing on MSM, people who inject drugs, and sex workers are scarce.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The past three decades have seen significant global progress in the reduction of HIV prevalence and incidence [1]. This progress suggests that the HIV epidemic has passed its peak incidence [1, 2] and may be attributed to two major advancements: substantial increases in access to anti-retroviral therapy (ART), with ART coverage globally increasing by 63 %, and improved availability and access to combination HIV prevention services [1, 3]. Despite this progress, recent reports also describe a different scenario among subsets of the population, showing that declines in HIV incidence rates are uneven. HIV incidence rates have risen among people who inject drugs, men who have sex with men (MSM), and sex workers [1, 4]. The micro-social contexts of relationships (i.e. relationship commitment, love, trust, closeness, and interdependence in intimate relationships) in which sexual- and drug-risks occur remain drivers of HIV among couples [5–7]. Research has demonstrated that condom use and safe injection practices remain low among people in intimate relationships [8, 9]; however, these issues have not been fully addressed and integrated into biobehavioral and biomedical HIV prevention strategies [10]. HIV prevention interventions generally focus on individuals, rather than on couples as a unit of change and analysis, ignoring the important role that sex partners play in sexual- and drug-risk behaviors and HIV treatment engagement and adherence [11].
There is consensus on the need for a new generation of HIV prevention and intervention strategies such as couple-based modalities for key populations in intimate relationships [9, 12]. HIV prevention efforts where the micro-social context serves as the foundation for sexual- and drug-risk reduction strategies may be more effective in reducing risk behaviors, strengthening healthy behaviors [5–7], and increasing HIV testing and treatment adherence [13]. There are several advantages to using a couple-based approach: it allows for both members to recognize their mutual responsibility in protecting each other from HIV transmission and encourages them to work together to stay healthy; it highlights the relationship’s context (i.e. commitment, love, trust) and its connection to HIV acquisition, subsequently drawing attention to the value and power of the relationship in behavioral change; it aids in the creation of a safe environment to discuss sensitive topics such as sexual concurrency, power imbalances, and sexual coercion; it allows for couples to learn about and practice important skills such as communication and problem-solving with the support and guidance of others, such as the facilitator; and finally, it promotes accountability and increases commitment to change [9, 13]. Couple-based prevention has also been shown to increase adherence to ART and has the potential to not only improve the health of persons living with HIV, but also lowering the risk of transmission within the pair by reducing the viral load of the infected partner [9, 13]. Despite these many advantages, couple-based HIV prevention and intervention efforts remain limited, with most focusing on individual approaches.
To date, there has been only one systematic review of HIV couple-based interventions, which was conducted in 2010 and only included attention to behavioral studies [14]. Our paper addresses a gap in the literature by focusing on couple-based HIV prevention and intervention research since the beginning of the HIV epidemic, examining the current state of couple-based HIV research and focusing on both biobehavioral and biomedical HIV intervention and prevention studies. This paper includes couple-based studies that deliver interventions to couples one-on-one or to a group of couples. We include studies that define couples in various ways, including dyads, sexual partners, married or cohabiting partners, studies that allowed participants to self-define their couple status, as well as couples in long and short-term relationships. The paper describes the types of studies, intervention/prevention modalities, and core components, and examines the populations of focus, theories, inclusion and exclusion criteria, and how couples are being defined. The paper also examines advantages and gaps in the current state of couple-based HIV prevention and intervention efforts and offers recommendations for future directions.
Methods
This systematic review followed core PRISMA [15] guidelines, including pre-defining the rationale and objectives for the review, inclusion/exclusion criteria, search strategy and study selection, and data collection/extraction procedures.
Inclusion and Exclusion Criteria
In this review, we included studies explicitly targeting couples for HIV treatment, prevention, and/or intervention. Studies designed to reduce sexual- and drug-risk behaviors, HIV transmission and acquisition, as well as those focused on promotion of HIV testing, ART treatment, treatment adherence, and circumcision among couples were included. We included studies focused on serodiscordant, concordant, at-risk, and HIV status unknown couples. For any study where initial recruitment or services were directed toward an individual partner, we included the study if at least one or more intervention/prevention modality focused on the couple. We included RCTs, quasi-experimental, prospective, and observational cohort studies. As previously noted, we included studies defining couples in a myriad of ways including dyads, sexual partners, married or cohabiting partners, studies that allowed participants to define their couple-status, and studies that recruited couples who were together for any length of time. We excluded articles that had a clear lack of relevance, were modeling studies, were epidemiological/surveillance in nature, were primarily prevention of mother-to-child transmission (PMTCT)-focused studies (even if couple-based), lacked published outcomes or that were non-intervention/prevention-based.
Literature Search and Data Extraction
Electronic searches through PubMed, Biomed Central, PsycInfo, CINAHL, and Sociological Abstracts were conducted in late June 2013. We did not limit the search by year of publication. We limited our search to published papers available in English and excluded dissertations. To cast the widest net, search terms included “HIV” in conjunction with “VCT,” “CVCT,” “prevention,” “intervention,” “treatment,” or “adherence” as well as “couples,” “MSM,” “partners,” “dyad,” or “married.”
All articles were first crossed-referenced for duplication and then one author screened all remaining abstracts for relevance. A liberal approach was utilized to review abstracts; abstracts needed to indicate delivering an intervention or prevention to more than one person. In instances where abstracts were seemingly relevant or unclear (e.g. it was unclear if the intervention was delivered to an individual, couple, group, or family, or the study was intervention/prevention-focused rather than epidemiological), full-text articles were reviewed independently by both authors who then met to discuss them in accordance with the inclusion criteria. All relevant articles were reviewed by the two co-authors independently and only those that met the inclusion criteria were included in the review. When multiple papers reported data from the same dataset/project, the authors examined the articles together and reported them here accordingly. In cases where it was unclear if articles referenced the same or a different study, attempts were made to reach out to investigators for clarification. References of relevant articles were also examined for additional studies, but this strategy did not yield any additional studies. Specific information on the search terms and strategy may be obtained by request.
For studies that met the inclusion criteria, data extraction included study location, study design, type of study, sample size, aims, core components and guiding theories, definition of couple, inclusion/exclusion criteria, targeted serostatus and sexual orientation of couple, study outcomes and power, adverse events, and study quality.
Results
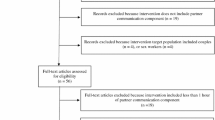
5,460 records were yielded from PubMed, 302 from BioMed Central, 2950 from PsycINFO, 1485 from CINAHL, and 965 from Sociological Abstracts. Once we removed duplicates, we screened the remaining 7,735 records for relevance using their titles and abstracts. We excluded papers lacking clear relevance, leaving 412 full-text articles for review. Of the 412 full-text articles retrieved, 93 were deemed relevant according to the inclusion criteria. Upon closer review of these articles, we identified a total of 33 studies published through late June 2013 (see Fig. 1 for more detail on the flow of the review process).

Flow diagram of systematic review search process
Description of Included Studies
We catalogued 33 HIV couple-based studies conducted globally (see Tables 1, 2). The earliest studies were conducted in the late 1980s, with many more beginning in 2000. We categorized the studies into two types: (1) biobehavioral, which includes: (a) psycho-educational and skills-building focused studies designed to reduce sexual- and drug-risks and acquisition and transmission of HIV, (b) HIV voluntary testing and counseling studies, and (c) ART adherence studies that promote medication uptake and address barriers to HIV testing and engagement in care and treatment; and (2) biomedical studies designed to evaluate the efficacy of HIV treatment options, including PrEP, combination therapies, ART, and circumcision. Twenty-seven studies were categorized as biobehavioral and six were identified as biomedical. Among the 27 biobehavioral studies, 13 were psycho-educational skills-building studies, 13 focused on VCT, and one focused on adherence. The majority of the biomedical studies focused on PrEP, combination therapies, and ART, while only one focused on male circumcision. (See Tables 1, 2 for more information on biobehavioral and biomedical studies.)
Study Regions
Ten of the 13 biobehavioral skills-building studies were conducted in the U.S., with the remaining conducted in Asia and Africa (see Table 1). Seven of the VCT studies were conducted in Africa, two in Asia, one in the Caribbean, one in the U.S., and two were multi-country studies (see Table 1). The only adherence study was implemented in the U.S. (see Table 1). All but one of the biomedical studies were conducted in Africa; the remaining study was conducted in three regions: Asia, Africa, and the U.S. (see Table 2).
Design and Sample Size
Of the 27 biobehavioral studies, roughly half were randomized control trials, with the remainder using quasi-experimental, prospective or observational study designs (see Table 1). Four of the six biomedical studies were randomized control trials; one was a prospective cohort study, and the other an observational cohort study (see Table 2). Sample sizes varied from fewer than 20 couples to more than 4,500 couples. The smallest biobehavioral study included only 12 couples [16] and the largest invited 1,995 couples to enroll [17]. The majority of the psychosocial and skills-building studies reported lack of power to detect biological endpoints where recorded. The smallest sample size among the biomedical studies was 250 couples [18] and the largest 4,758 couples [19].
Sample Size and Power Analysis
Among most of the biobehavioral studies, power analyses were not typically reported in the articles. However, among skills-building, VCT, and adherence papers that did report power analyses, studies aimed to achieve 80–90 % power [8, 20–31]. Among the biomedical studies, power analyses were consistently reported and aimed to achieve at least 80–90 % power to detect differences for major study endpoints [18, 19, 32–37].
Types of Couples
Among the 13 biobehavioral skills-building studies, 12 studies included heterosexual couples, and one included MSM couples. Four studies included people who use or inject drugs and none specifically recruited sex workers (see Table 1). The adherence study included both heterosexual and MSM couples [31]. Of the 13 VCT studies, none included MSM couples and only one specified recruiting any other high-risk group (see Table 1).
Five of the six biomedical studies recruited serodiscordant couples, and one required at least one HIV seropositive partner (see Table 2). With one exception, only heterosexual couples were recruited; Cohen et al. [34] appeared to include heterosexual and MSM couples (see Table 2). None of the six studies provided information on the inclusion of injection drug users and/or sex workers.
Inclusion and Exclusion Criteria
Among the biobehavioral skills-building studies, the most common inclusion criteria noted were: (1) age of participants (18 or older)—only two studies included couples under age 18 (these studies focused on parenting adolescents aged 14–23/25) [38, 39]; (2) engagement in sexual-risk behaviors (number of unprotected sex acts and sexual partners); (3) drug-risk (injecting and use of illicit substances, including methamphetamine); and (4) length of the relationship (being together 3–6 months and planning to stay together for a year) (see Table 1 for more information regarding inclusion criteria). Exclusion criteria for the majority of biobehavioral skills-building studies included reports of severe violence, severe mental health impairments, and pregnancy. The adherence study required participants to be a minimum of 18 years old and the HIV-positive partner to have been on ART for a minimum of 1 month [31, 40]. Among the VCT studies, several did not specify their inclusion/exclusion criteria. Where noted, major inclusion criteria included a minimum age of 18 and willingness to enroll with and disclose test results to partners (see Table 1). Five studies specifically recruited pregnant women for enrollment into their study (see Table 1).
All six biomedical studies, with one exception, reported minimum or maximum CD4 counts and confirmed serostatus of partners (see Table 2). A minimum age requirement (of 18 or older) was used in five of the six studies (see Table 2). Biomedical studies also often required no concurrent participation in any other biomedical intervention and/or adequate biological functioning to be eligible for enrollment.
Definition of a Couple
The majority of biobehavioral studies (not including VCT and adherence) defined “couple” by length of the relationship. Both members of the dyad had to independently report being together for a minimum of 3 or 6 months (sexual relationship) and intention to stay together for a minimum of 1 year. Four of the biobehavioral studies defined a couple differently: one study required the couple to be married [16], another allowed the couple to self-identify as a couple [41], and the remaining two were defined by their co-parenting status (i.e. the couple had to be parenting a child together) [38, 39].
Biomedical, VCT, and adherence studies, the majority of which were conducted in Africa and Asia, primarily defined a couple by their marital or co-habiting status or perceived definition as a couple (see Tables 1, 2). Those that did not require the couple to be married, co-habiting, or self-identified as a couple, required participants to have engaged in a minimum number of sexual acts during the prior 3–6 months (see Tables 1, 2).
Core Components of the Interventions
There is homogeneity of intervention core components among the skills-building couple-based studies: knowledge building about HIV and sexually transmitted infections, skills-building in condom use, couple communication, negotiation skills, problem-solving, and goal setting; addressing power imbalances associated with decision-making; and offering strategies to promote and maintain healthy relationships [8, 16, 22–26, 28, 38, 39, 41–49]. Studies that included people who use or inject drugs also covered content related to the micro-social context of drug use in intimate relationships, such as the meaning of sharing or refusing to share needles or drugs in intimate relationships, the relationship between refusal to share needles/syringes and partner violence, and strategies to manage negative reactions when refusing needle/syringe sharing [8, 23, 24, 42].
The adherence study’s core components included information sharing about the importance of medication and adherence, consequences of non-adherence, role of the supportive partner, discussions regarding barriers to adherence, and strategies to improve adherence, including problem-solving, communication, self-monitoring, and motivation [31, 40]. The core components of VCT studies included individual and couples HIV (rapid) testing and counseling, education and role-play (skills-building and self-efficacy), condom distribution, and information and referral for treatment, where necessary [12, 17, 20, 21, 27, 29, 30, 50–57].
Core components of the biomedical studies included distribution of medication (single or combination) and tracking adherence outcomes, including seroconversions and/or observation of outcomes to medication uptake [18, 19, 32–36]. The one circumcision study [37] focused on circumcision of male partners after enrollment of couples.
Guiding Theories of Studies
Almost all of the biobehavioral skills-building studies described the theoretical frameworks underpinning the design of their interventions. The most frequently cited theories included theory of gender and power [58], social cognitive theory [59], theory of reasoned action [60, 61], HIV risk-reduction (based on social cognitive theory), and ecological systems [23, 38, 39, 42–44, 48, 49, 62]. Other, but less frequently noted theories included the healing the wounded spirit framework and the integrated behavioral change model [38, 39, 45].
In general, the VCT study papers did not typically note the theories guiding their research. Only Jones et al. [25, 26] described their use of the theory of reasoned action and planned behavior. The adherence study employed the theory of social action [31, 40]. Among the biomedical studies, no guiding theories were noted in the articles reviewed.
Study Outcomes
A variety of behavioral endpoints were used across biobehavioral studies (see Table 1). Study endpoints included reduced unprotected sex acts [23, 24, 38, 39, 47, 49]; increased protected sex acts [8, 22–24, 26, 41, 42, 47]; fewer sexual partners [49]; increased consistent condom use with main and other sex partners [22]; decreased unsafe injection [42] and illicit drug use [49].
A number of biobehavioral studies also focused on improving the intervention mediators and found greater intention to use condoms and increased HIV/AIDS knowledge [26, 38, 39]; positive attitudes towards condoms [26]; improved mental health outcomes [16]; improved comfort levels regarding discussions with their partners about sex and condoms and ability to use learned intervention skills with their partner [46]; and increased acceptability of barrier products [25].
Couple-based VCT, when compared to individual VCT or general health promotion activities, consistently yielded reductions in risk behavior and improvements in sexual safety, HIV knowledge, willingness to get tested, and testing. More specifically, follow-up data indicated increased condom use [27, 51, 52, 54]; fewer biological markers [51, 52]; fewer unprotected sex acts [21]; fewer incidents of coerced sex [63]; increased disclosure [54]; increased HIV knowledge, willingness to get tested [56], and testing [30]; and use of formula if breast-feeding [54].
VCT acceptability and feasibility studies yielded mixed results. Becker, Mlay, Schwandt, and Lyamuya [20] found that fewer women received HIV test results in the couple-based arm, compared to those in the individual-arm, but among those who were HIV positive in the couple-based arm, more participants reported using HIV prevention measures. In contrast, Mohlala et al. [29] found that a higher number of pregnant women who were offered couple-based VCT, compared to those offered pregnancy information sessions (control), brought in their partners. Further, more of the men in the VCT arm, compared to those in the control arm, received HIV testing.
The medication adherence study found that participants in the intervention arm, compared to participants in the control arm, had higher mean medication adherence, both for doses taken and doses taken within a particular time frame [31, 40]. However, while participants in the intervention arm were more likely to have higher levels of adherence, compared with control participants, these effects were lower during follow-up periods [31, 40].
Among the six biomedical studies, ART endpoints included reductions in viral load and HIV transmissions between serodiscordant couples [18, 19, 32, 34–36]. Reynolds et al. [18] reported on additional outcomes, including greater condom use, but reported no differences in the number of sexual partners or other risk behaviors among those receiving ART and those in the control condition. However, daily acyclovir therapy did not reduce the risk of HIV-1 among those also infected with HSV-2, though it did reduce the occurrence of genital ulcers [33]. The one circumcision study proved ineffective as a sole method for the prevention of HIV transmission between couples and was terminated early due to futility [37].
Adverse Events
Among the biobehavioral skills-building studies, where noted, no adverse events occurred [8, 22, 42, 46]. Similarly, the adherence study paper reported no adverse events [31, 40]. The majority of VCT studies did not report on adverse events. Among those that did, adverse events included reactions to HIV status notification [21] and union breakups and partner violence [30].
Biomedical studies generally included a section or statement on adverse events. Adverse events included death (not related to intervention) and physical issues, including infections, psychiatric and biological disorders, among others [33–35]. Wawer et al. [37] also noted some adverse events related to circumcision (surgical).
Study Quality
Using an adapted version of the QUADAS 2 Tool [64], each study was assessed for its sample representativeness/generalizability, quality and clarity of the inclusion/exclusion criteria, sampling procedures, random assignment/randomization procedures, data analytical approach, power analysis plan and power, and reporting on attrition and loss to follow-up.
None of the reported biobehavioral or biomedical studies included representative/generalizable sample populations.
All of the biobehavioral skills-building studies utilized appropriate data analytical approaches and ten provided good/clear information about their inclusion and exclusion criteria [8, 22–25, 28, 38, 39, 42, 46, 48, 49]. Similarly, the majority of the studies also had good/clear sampling procedures [8, 22–26, 28, 38, 39, 41, 42, 46, 49]; but, five studies had small sample sizes - under 50 couples [16, 38, 42, 46, 49]. Where applicable, random assignment/ randomization procedures were clear and the majority of studies provided some information about attrition and loss to follow-up. Two studies were unclear or did not report on their attrition and loss to follow-up [26, 38]. Finally, fewer than five studies reported power analysis plans, though all 13 studies generally reported sufficient power for main outcomes of interest.
The single adherence study [31] had clear, high quality inclusion/exclusion criteria, sampling procedures, random assignment/randomization procedures, data analytical approach, power analysis plan and power, and reporting on attrition and loss to follow-up.
Among the VCT studies, several studies were unclear or lacked sufficient information about their inclusion and exclusion criteria [17, 27, 52, 54, 56, 65]. Nearly all studies had clear/good sampling procedures and reported attrition and loss to follow-up, and all used appropriate data analytical approaches. Given the nature of and ethical issues surrounding VCT, few studies randomized participants; among those that did, randomization procedures were generally clear [12, 21, 30]. Only three studies reported their power analysis plan [12, 29, 30], but all the studies seemed appropriately powered for several of their outcomes of interest.
All six biomedical studies were generally clear with respect to the inclusion and exclusion criteria with one exception, where very limited information was provided [18]. The clarity of sampling procedures, quality of data analytical approach, and random assignment/randomization procedures, where applicable, were clear in all the studies. Power analyses plans were consistently offered, though not all the studies reported sufficient power for all outcomes of interest [18].
Discussion
To our knowledge, this is the second published systematic review of couple-based HIV prevention and intervention studies since the start of the HIV epidemic. The first review targeted only behavioral prevention and intervention studies, whereas this review includes both biobehavioral and biomedical prevention and intervention studies. In our review, we found 33 couple-based studies conducted globally. Of these 33 studies, 27 were biobehavioral and six were biomedical. Nearly all of the 33 studies were conducted in the U.S., Africa, and Asia and included anywhere from 12 to nearly 5,000 couples. Most studies targeted heterosexual couples.
This review paper shows that the number of HIV couple-based studies conducted globally remains limited despite their potential to reduce sexual- and drug-risks, HIV and STI incidence rates, and improve HIV testing and adherence to ART. In the following section, we highlight a number of methodological weaknesses that characterize the state of the science of HIV couple-based research reviewed in this paper, and provide a few concrete steps that should be considered to address these drawbacks. We have focused on major methodological limitations that we believe are of high importance for advancing couple-based HIV interventions.
First, the majority of the studies we reviewed used a narrow definition of a “couple.” More specifically, the majority of studies reviewed used stringent inclusion criteria such as relationship length (for example, being together for six or more months), commitment level (for example, intention to stay together for a year), and/or relationship status (for example, being married or living together). Most studies also used a verification assessment screening prior to study participation to confirm whether the couple was “truly a couple.” Moreover, experience of severe physical or sexual abuse reported by one or both parties in the relationship was used as an exclusion criterion among many of the studies. Such criteria may have excluded couples that would have benefited from the interventions.
In order to reach out to more diverse couples who need HIV interventions and services, we advocate for the use of a flexible, broad definition of a “couple” for research studies and implementation efforts in real world settings, such as permitting participants to self-define their status (i.e. both parties in the dyadic relationship state they are a couple or sexual partners). In real-world settings, it would be unethical not to provide HIV services to couples who have been together for a short period of time, and HIV transmission risks can exist at any stage of a relationship. Thus, though we acknowledge the reasons for using relationship length or status as potentially indicative of a couple’s commitment to one another, and couple verification assessment as a method to ensure “true couples” in studies [66], we suggest using shorter verification screening assessments that include consistency across three to four questions. For example, drawing on McMahon et al.’s paper [66], one might ask each partner when the couple first met, length of time together, and living arrangement to determine if the dyad is a couple. Recognizing the immense cost of recruiting and retaining couples, as well as potential challenges in maintaining statistical power, requirements for length of relationship can vary based on the type and length of the intervention. For example, a one-time VCT session study may not need to consider the length of the relationship, whereas a multi-session couple-based intervention study may need to consider the length of relationship.
The majority of biobehavioral studies included assessment of intimate partner violence in their screening procedures and, in many cases, excluded couples that reported severe abuse. However, given research linking the relationship between violence and HIV [67, 68], we propose that couple-based studies broaden inclusion criteria to include couples that report history of severe partner abuse or whom are currently experiencing severe violence. Understanding the potential dangers and ethical concerns of including couples experiencing violence, it is critical to integrate robust screening and safeguard procedures. We advocate that intimate partner violence screenings become routinely integrated into study recruitment and enrollment procedures of HIV couple-based studies. For those couples where either active or recent abuse is present and/or risk of violence is high, for ethical and safety reasons, we suggest that the affected member of the dyad is asked separately if he/she feels safe in participating in a study where sensitive issues about sex, relationships, drugs, adherence to ART, or linkage to care are discussed. Further, we recommend that safety planning is concurrently integrated into this assessment, and that regular, ongoing check-ins and safety planning occur with the participant as to their ongoing comfort and safety in participating in the study. Suspicion or witnessing that one or both partners is verbally, physically, or sexually abusive during or outside the sessions should be taken seriously; the facilitator who delivers the intervention sessions should be appropriately trained and follow a safety plan to ensure that the abused individual has access to resources and services to deal with the situation. The sessions may be terminated if the abusive relationship continues to escalate, as it is dangerous to have the couple attend the sessions together. Some of the core components may also be delivered separately to participants—for example, to single gender groups, where female and male participants first meet separately to discuss sensitive issues in a couple-context. As an alternate recommendation to including couples with active violence, another useful approach may be to screen for active violence in the past 3 or 6 months and to subsequently follow the safety guidelines presented above as a precautionary measure. Finally, we suggest that among biobehavioral and biomedical studies, where violence remains unaddressed in the core components, integration of intimate partner violence assessment and safety planning is critical.
Second, couple-based biobehavioral and biomedical HIV intervention studies have rarely targeted MSM or drug-involved couples, and none have targeted couples in casual, short-term relationships, sex workers who have regular sexual partners, or transgender couples. For example, despite research indicating that among MSM, 33–68 % of new HIV infections are transmitted by a main partner [69, 70], HIV couple-based prevention for MSM remains low. Of the 33 studies, only one was adapted for MSM couples and an additional two specifically recruited MSM and heterosexual couples. Future research would benefit from attention to these key populations, and careful attention should be given to developing and testing couple-based HIV prevention interventions for different types of couples. Recent research focused on risk behaviors and relationship dynamics among sex workers in relationships [6, 7] and MSM couples [71–79] provide useful insight and important considerations for future studies that seek to target these groups for prevention, such as the role of avoidance in discussing sexual practices [6, 7] and sexual concurrency, as well as attachment and intimacy [73].
Third, most couple-based HIV prevention approaches are guided by individual-based theories, such as social learning and cognitive behavioral theories [80–85]. These theories assume that couples are motivated to take protective actions, and often overlook many relationship, dyadic, and structural factors. There is also a significant gap in the theoretical and conceptual models in understanding the dynamics that may influence decisions regarding sex and HIV risks, especially in short-term relationships and non-traditional relationships. It is essential to apply theoretical frameworks that allow the inclusion of multiple influences (e.g. individual, interpersonal, social, and structural) such as the ecological theory [86] that has been used to understand the dynamic among various personal, interpersonal and environmental factors. Measurement in couple-based intervention research needs to incorporate these multi-level factors.
Fourth, data analytical approaches have mainly targeted the individual, not the couple, as the unit of attention. That is, although data from existing prevention and treatment studies were collected from couples, most of the studies reviewed employed individual-data analytical approaches. We propose that more attention be given to couple-data analytical techniques. Further, a number of the psycho-educational and skills-building couple-based studies included small sample sizes and/or lacked biologically confirmed HIV and STI endpoints. Further, none have been sufficiently powered to examine new STI and HIV infections as outcomes. Future studies would benefit from including larger sample sizes and using biological endpoints.
Fifth, few studies to date have examined whether couple-level interventions are effective in reducing sexual concurrency. Sexual concurrency should be of central interest in light of evidence indicating increased HIV and STI risk among different populations in the U.S. and other countries [87]. As it stands, it is unclear whether existing couple-based HIV prevention approaches reduce HIV risk with extra-dyadic partners. A recent meta-analysis [88] suggests that behavioral couple-based approaches may be effective in reducing concurrency, however, condom use (uptake and consistency) with extra-dyadic partners remains unclear. From a measurement point of view, the literature has underscored the complexity of measuring these behaviors because they rely not only on accurate recall, but also on the start and end of the relationship [87]. However, collecting data on concurrency may be challenging given the stigma surrounding concurrency and if the members of the couple feel unsafe disclosing this behavior. To reduce these challenges, we suggest that, during the initial assessment phase when a couple comes together for research purposes, confidentiality must be secured by making sure that each individual partner is in a separate room, and that context-specific and appropriate methods are used (e.g. face-to-face interviews or technology such ACASI) to collect data on sensitive issues, such as questions about the sexual relationship and concurrency and type of couples (casual, long-term, etc.) [22, 89]. An additional strategy for addressing issues of concurrency might be to deliver select content in single-gender groups - where female and male participants first meet separately in single gender groups to discuss and assess how to best share sensitive issues in a couple-context.
Sixth, studies of couple-based HIV prevention interventions have been unable, so far, to determine the optimal intervention modality. It is unclear whether interventions are more effective when sessions are delivered individually to each couple, when sessions are delivered using a mixed format of individual and group sessions, or when content is delivered to a small, single-gender group of individuals who are in coupled relationships. A recent meta-analysis of behavioral interventions [88] suggests that delivery of material to individual couples is more effective than when delivered to a group, but it is not clear whether a mix-method approach would be more effective. The next generation of research on couple-based HIV interventions should tackle these questions using different designs that allow these scientific questions to be answered.
Finally, applying evidence-based HIV prevention and treatment approaches to real-world settings, and training clinicians to use such approaches, is an important step in making a strong public health impact on the epidemic. None of the studies reviewed in this paper focused on effectiveness or implementation research in real-world settings. We suggest that there is an urgent need for attention and resources to disseminate evidence-based couple-focused prevention and treatment research into real-world settings, as it has the potential to reduce HIV acquisition and transmission among vulnerable populations. Expanding the scope of dissemination and scaling up couple-based HIV interventions will require commitment by governments and donors to fund research on dissemination and implementation as well as training for providers in couple-based approaches. With the increased emphasis and use of a “seek, treat, and retain” HIV prevention and treatment paradigm [13, 89], a couple-based modality can be used at each stage on the continuum of this process. Engaging the couple together at each stage may lead to better outcomes where the responsibility is placed on the dyad and not simply on recruiting a partner to treatment, while also engaging them in forging linkages with support in their community, and improving retention in treatment and care. This approach requires a shift in HIV prevention where the emphasis moves from the individual to dyadic contexts. The shift also requires training service providers and increased funding to focus on the couple as unit of change rather than the individual clients.
Implementation of couple-based prevention strategies must also address a number of organizational barriers such as the service providers’ high caseloads, time constraints on engaging the couple, scarce funding for agencies to expand work with couples, health insurance and billing regulations that may not consider both individuals as a single “client,” HIPAA regulations that prevent information being shared with others, and a lack of training and technical assistance in using couple modalities (an individual-oriented approach is the norm). The next generation of couple-based research must also tackle these issues in order to make the prevention applicable to real-word settings.
In sum, the use of a couple-based modality is important for both HIV biobehavioral and biomedical prevention interventions, for all types of relationships (long-term, short- term, casual, etc.) and key populations (MSM, people who use drugs, sex workers). HIV couple-based research is in its infancy and needs to pay more attention to the methodological barriers discussed in this paper. Finally, more attention should be given to disseminating and translating couple-based modalities to real-world settings. For successful implementation of couple-based approaches in real-world settings, an ideological shift from focusing on the individual to the dyad must occur, with an emphasis on navigating existing organizational and funding barriers.
References
UNAIDS, Global Report: UNAIDS Report on the Global AIDS Epidemic 2012, Joint United Nations Programme on HIV/AIDS (UNAIDS).
Beyrer C, Abdool Karim Q. The changing epidemiology of HIV in 2013. Curr Opin HIV AIDS. 2013;8(4):306.
UNAIDS, UN World AIDS Day Report: 2012, 2012, Geneva: UNAIDS.
Baral S, et al. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(7):538–49.
Seear K, et al. Rethinking safety and fidelity: the role of love and intimacy in Hepatitis C transmission and prevention. Health Soc Rev. 2012;21(3):272–86.
Syvertsen JL, et al. ‘Where sex ends and emotions begin’: love and HIV risk among female sex workers and their intimate, non-commercial partners along the Mexico-US border. Cult Health Sex. 2013;15(5):540–54.
Syvertsen JL, et al. “Eyes that don’t see, heart that doesn’t feel”: coping with sex work in intimate relationships and its implications for HIV/STI prevention. Soc Sci Med. 2013;87:1–8.
El-Bassel N, et al. Couple-based HIV prevention for low-income drug users from New York City: a randomized controlled trial to reduce dual risks. J Acquir Immune Defic Syndr. 2011;58(2):198–206.
El-Bassel N, Wechsberg WM. Couple-based behavioral HIV interventions: placing HIV risk-reduction responsibility and agency on the female and male dyad. Couple Family Psychol. 2012;1(2):94–105.
El-Bassel N, Wechsberg WM, Shaw SA. Dual HIV risk and vulnerabilities among women who use or inject drugs: no single prevention strategy is the answer. Curr Opin HIV AIDS. 2012;7(4):326–31.
El-Bassel N, Terlikbaeva A, Pinkham S. HIV and women who use drugs: double neglect, double risk. Lancet. 2010;376(9738):312–4.
McMahon JM, et al. Effectiveness of couple-based HIV counseling and testing for women substance users and their primary male partners: a randomized trial. Adv Prev Med. 2013;2013:286207.
El-Bassel N, Remien RH. Couple-based HIV prevention and treatment: State of science, gaps, and future directions. In: Pequegnat W, editor, 2012. p. 153–172.
Burton J, Darbes LA, Operario D. Couples-focused behavioral interventions for prevention of HIV: systematic review of the state of evidence. AIDS Behav. 2010;14(1):1–10.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(7716):332–6.
Pomeroy EC, Green DL, Van Laningham L. Couples who care: the effectiveness of a psychoeducational group intervention for HIV serodiscordant couples. Res Soc Work Pract. 2002;12(2):238–52.
Kempf M-C, et al. Enrollment and retention of HIV discordant couples in Lusaka, Zambia. J Acquir Immune Defic Syndr. 2008;47(1):116–25.
Reynolds SJ, et al. HIV-1 transmission among HIV-1 discordant couples before and after the introduction of antiretroviral therapy. AIDS. 2011;25(4):473–7.
Baeten J, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367(5):399–410.
Becker S, et al. Comparing couples’ and individual voluntary counseling and testing for HIV at antenatal clinics in Tanzania: a randomized trial. AIDS Behav. 2010;14(3):558–66.
Coates TJ, et al. Efficacy of voluntary HIV-1 counselling and testing in individuals and couples in Kenya, Tanzania, and Trinidad: a randomised trial. Lancet. 2000;356(9224):103–12.
El-Bassel N, et al. National Institute of Mental Health Multisite Eban HIV/STD Prevention Intervention for African American HIV Serodiscordant Couples: a cluster randomized trial. Arch Intern Med. 2010;170(17):1594–601.
El-Bassel N, et al. The efficacy of a relationship-based HIV/STD prevention program for heterosexual couples. Am J Public Health. 2003;93(6):963–9.
El-Bassel N, et al. Long-term effects of an HIV/STI sexual risk reduction intervention for heterosexual couples. AIDS Behav. 2005;9(1):1–13.
Jones D, et al. Enhancing acceptability and use of sexual barrier products among hiv concordant and discordant couples. AIDS Behav. 2013;17(6):2185–93.
Jones DL, et al. Influence of partner participation on sexual risk behavior reduction among HIV-positive Zambian women. J Urb Health. 2005;82((3 Suppl 4)):iv92–100.
Kamenga M, et al. Evidence of marked sexual behavior change associated with low HIV-1 seroconversion in 149 married couples with discordant HIV-1 serostatus : experience at an HIV Counseling Center in Zaire. AIDS. 1991;5(1):61–7.
Kraft JM, et al. Intervening with couples—assessing contraceptive outcomes in a randomized pregnancy and HIV/STD risk reduction intervention trial. Womens Health Issues. 2007;17(1):52–60.
Mohlala BKF, Boily M-C, Gregson S. The forgotten half of the equation: randomized controlled trial of a male invitation to attend couple voluntary counselling and testing. AIDS. 2011;25(12):1535–41.
Orne-Gliemann J, et al. Increasing HIV testing among male partners. The Prenahtest ANRS 12127 multi-country randomised trial. AIDS. 2013;27(7):1167–77.
Remien RH, et al. Couple-focused support to improve HIV medication adherence: a randomized controlled trial. AIDS. 2005;19(8):807–14.
Bunnell R, et al. Changes in sexual behavior and risk of HIV transmission after antiretroviral therapy and prevention interventions in rural Uganda. AIDS. 2006;20(1):85–92.
Celum C, et al. Acyclovir and transmission of HIV-1 from persons infected with HIV-1 and HSV-2. N Engl J Med. 2010;362(5):427–39.
Cohen MS, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.
Cohen MS, McCauley M, Gamble TR. HIV treatment as prevention and HPTN 052. Curr Opin HIV AIDS. 2012;7(2):99–105.
Mujugira A, et al. Characteristics of HIV-1 serodiscordant couples enrolled in a clinical trial of antiretroviral pre-exposure prophylaxis for HIV-1 prevention. PLoS ONE. 2011;6(10):e25828.
Wawer MJ, et al. Circumcision in HIV-infected men and its effect on HIV transmission to female partners in Rakai, Uganda: a randomised controlled trial. Lancet. 2009;374(9685):229–37.
Koniak-Griffin D, et al. HIV prevention for Latino adolescent mothers and their partners. West J Nurs Res. 2008;30(6):724–42.
Koniak-Griffin D, et al. Couple-focused human immunodeficiency virus prevention for young Latino parents: randomized clinical trial of efficacy and sustainability. Arch Pediatr Adolesc Med. 2011;165(4):306–12.
Remien RH, et al. Moving from theory to research to practice. Implementing an effective dyadic intervention to improve antiretroviral adherence for clinic patients. J Acquir Immune Defic Syndr. 2006;43(Suppl 1):S69–78.
Padian NS, et al. Prevention of heterosexual transmission of human-immunodeficiency-virus through couple counseling. J Acquir Immune Defic Syndr Hum Retrovirol. 1993;6(9):1043–8.
Gilbert L, et al. Couple-based HIV prevention for injecting drug users in Kazakhstan: a pilot intervention study. J Prev Interv Community. 2010;38(2):162–76.
Group, N.M.H.S.P.T.f.A.A.C., Eban health promotion intervention: conceptual basis and procedures. J Acquir Immune Defic Syndr, 2008. 49 Suppl 1: p. S28-34.
Group, N.M.H.S.P.T.f.A.A.C., Methodological overview of an African American couple-based HIV/STD prevention trial. J Acquir Immune Defic Syndr, 2008. 49 Suppl 1: p. S3-14.
Harvey S, et al. Effects of a health behavior change model-based HIV/STI prevention intervention on condom use among heterosexual couples: a randomized trial. Health Educ Behav. 2009;36(5):878–94.
McGrath JW, et al. A group-based intervention to increase condom use among HIV serodiscordant couples in India, Thailand, and Uganda. AIDS Care. 2007;19(3):418–24.
Witte SS, et al. Promoting female condom use to heterosexual couples: findings from a randomized clinical trial. Perspect Sex Reprod Health. 2006;38(3):148–54.
Wu E, et al. Adaptation of a couple-based hiv intervention for methamphetamine-involved African American Men who have sex with men. Open AIDS J. 2010;4:123–31.
Wu E, et al. Feasibility and promise of a couple-based HIV/STI preventive intervention for methamphetamine-using, black men who have sex with men. AIDS Behav. 2011;15(8):1745–54.
Allen S, et al. Promotion of couples’ voluntary counselling and testing for HIV through influential networks in two African capital cities. BMC Public Health. 2007;7:349.
Allen S, et al. Sexual behavior of HIV discordant couples after HIV counseling and testing. AIDS. 2003;17(5):733–40.
Allen S, et al. Effect of serotesting with counselling on condom use and seroconversion among HIV discordant couples in Africa. BMJ. 1992;304(6842):1605–9.
Deschamps MM, et al. Heterosexual transmission of HIV in Haiti. Ann Intern Med. 1996;125(4):324–30.
Farquhar C, et al. Antenatal couple counseling increases uptake of interventions to prevent HIV-1 transmission. J Acquir Immune Defic Syndr. 2004;37(5):1620–6.
Katz DA, et al. Male perspectives on incorporating men into antenatal HIV counseling and testing. PLoS ONE. 2009;4(11):e7602.
Khoshnood K, et al. Assessing the efficacy of a voluntary HIV counseling and testing intervention for pregnant women and male partners in Urumqi City, China. AIDS Behav. 2006;10(6):671–81.
Mehendale SM, et al. Low HIV-1 incidence among married serodiscordant couples in Pune, India. J Acquir Immune Defic Syndr. 2006;41(3):371–3.
Connell RW. Gender and power: society, the person and sexual politics. Sydney: R.W. Connell; 1987. p. 334.
Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–84.
Ajzen I. Theory of reasoned action. Washington, DC: American Psychological Association; 2000. p. 61–3.
Fishbein M. Theory of reasoned action. London: Sage Publications; 2004.
Bronfenbrenner U. Ecological systems theory. Washington, DC: American Psychological Association; 2000. p. 129–33.
Roth DL, et al. Sexual practices of HIV discordant and concordant couples in Rwanda: effects of a testing and counselling programme for men. Int J of STD AIDS. 2001;12(3):181–8.
Whiting PF, et al. Quadas-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–36.
Mehendale SM, et al. Low HIV-1 incidence among married serodiscordant couples in Pune. India. J Acquir Immune Defic Syndr. 2006;41(3):371–3.
McMahon JM, et al. Recruitment of heterosexual couples in public health research: a study protocol. BMC Med Res Methodol. 2003;3(1):24.
Jewkes RK, et al. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet. 2010;376(9734):41–8.
Maman S, et al. The intersections of HIV and violence: directions for future research and interventions. Soc Sci Med. 2000;50(4):459–78.
Goodreau SM, et al. What drives the US and Peruvian HIV epidemics in men who have sex with men (MSM)? PLoS One. 2012;7(11):e50522.
Sullivan PS, et al. Estimating the proportion of HIV transmissions from main sex partners among men who have sex with men in five US cities. AIDS (London). 2009;23(9):1153–62.
Campbell CK, et al. Health, trust, or “Just Understood”: explicit and implicit condom decision-making processes among black, white, and interracial same-sex male couples. Arch Sex Behav. 2013;16:1–10.
Chakravarty D, et al. Rates of testing for HIV in the presence of serodiscordant UAI among HIV-negative gay men in committed relationships. AIDS Behav. 2012;16(7):1944–8.
Hoff CC, et al. Relationship characteristics associated with sexual risk behavior among MSM in committed relationships. AIDS Patient Care STDS. 2012;26(12):738–45.
Marks G, et al. Meta-analysis of high-risk sexual behavior in persons aware and unaware they are infected with HIV in the United States: implications for HIV prevention programs. J Acquir Immune Defic Syndr. 2005;39(4):446–53.
Mitchell JW. Actor–partner effects of demographic and relationship factors associated with HIV risk within gay male couples. Arch Sex Behav. 2013;42(7):1337.
Mitchell JW. Factors associated with men in HIV-negative gay couples who practiced UAI within and outside of their relationship. AIDS Behav. 2013;17(4):1329–37.
Mitchell JW. HIV-negative and HIV-discordant gay male couples’ use of HIV risk-reduction strategies: differences by partner type and couples’ HIV-status. AIDS Behav. 2013;17(4):1557–69.
Mitchell JW, Petroll AE. HIV testing rates and factors associated with recent HIV testing among male couples. Sex Transm Dis. 2012;39(5):379.
Sullivan PS. The prevalence of undiagnosed HIV serodiscordance among male couples presenting for HIV testing. Arch Sex Behav. 2014;43(1):173.
Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs: Prentice-Hall; 1980.
Bandura A, Adams NE. Analysis of self-efficacy theory of behavioral change. Cogn Therapy Res. 1977;1(4):287–310.
Bandura A. Cognitive processes mediating behavior change. J Pers Soc Psychol. 1977;35:125–39.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Beck TKH. An exploratory study of cognitive style based on perceptual mode, conceptual style and speech code. Atlanta: Emory University; 1975.
Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Behav. 1988;15(2):175.
Bronfenbrenner U. The ecology of human development: experiments by nature and design, vol. xv-330. Cambridge: Harvard University Press; 1979.
Aral SO. Partner concurrency and the STD/HIV epidemic. Curr Infect Dis Rep. 2010;12(2):134–9.
LaCroix JM. Behavioural interventions to reduce sexual risk for HIV in heterosexual couples: a meta-analysis. Sex Transmit Infect. 2013;89(8):620–7.
El-Bassel N, et al. Couple-based HIV prevention in the United States: advantages, gaps, and future directions. J Acquir Immune Defic Syndr. 2010;55(Suppl 2):S98–101.
Wall K, Karita E, Nizam A, et al. Influence network effectiveness in promoting couples’ HIV voluntary counseling and testing in Kigali, Rwanda. AIDS. 2012;26(2):217–27.
Acknowledgments
The authors acknowledge the partial support received from R01 (R01DA033168) to Dr. El-Bassel funded by the National Institute of Drug Abuse.
Conflict of interest
The authors have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jiwatram-Negrón, T., El-Bassel, N. Systematic Review of Couple-Based HIV Intervention and Prevention Studies: Advantages, Gaps, and Future Directions. AIDS Behav 18, 1864–1887 (2014). https://doi.org/10.1007/s10461-014-0827-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-014-0827-7