
Abstract
Childhood sexual and physical abuse have been linked to adolescent and adult risky sexual behaviors, including early sexual debut, an increased number of sexual partners, unprotected sex, alcohol and drug use during sex and sexual violence. This paper explores these relationships among both men and women who report histories of childhood abuse from representative samples of communities in three countries in southern and eastern Africa (South Africa, Zimbabwe and Tanzania). Data were collected as part of a 3-year randomized community trial to rapidly increase knowledge of HIV status and to promote community responses through mobilisation, mobile testing, provision of same-day HIV test results and post-test support for HIV. The results indicate that reported childhood sexual and physical abuse is high in all three settings, also among men, and shows strong relationships with a range of sexual risk behaviors, including age at first sex (OR −0.6 (CI: −0.9, −0.4, p < 0.003)—among men, OR −0.7 (CI: −0.9, −0.5, p < 0.001)—among women), alcohol (OR 1.43 (CI: 1.22, 1.68, p < 0.001)—men, OR 1.83 (CI: 1.50, 2.24, p < 0.001)—women) and drug use (OR 1.65 (CI: 1.38, 1.97, p < 0.001)—men, OR 3.14 (CI: 1.95, 5.05, p < 0.001)—women) and two forms of partner violence—recent forced sex (OR 2.22 (CI: 1.66, 2.95, p < 0.001)—men, OR 2.76 (CI: 2.09, 3.64, p < 0.001)—women) and ever being hurt by a partner (OR 3.88 (CI: 2.84, 5.29, p < 0.001)—men, OR 3.06 (CI: 2.48, 3.76, p < 0.001)—women). Individuals abused in childhood comprise between 6 and 29 % of young adult men and women living in these African settings and constitute a population at high risk of HIV infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 2010, there was an estimated 34 million people in the world living with HIV. Increasing numbers of people, some 6.65 million are now receiving treatment, and the annual number of new infections has been slowly declining since 2001. However, the total number of people living with HIV continues to increase. Sub-Saharan Africa was home to 68 % of people living with HIV in 2010. The main sources of HIV transmission vary between countries but in this region, the principal mode of infection is heterosexual intercourse. Young people, aged 15–24 years of age account for 45 % of all new HIV infections, and their vulnerability to HIV is mainly attributable to high risk sexual behaviors [1].
Risky sexual behavior includes age of sexual debut [2], being sexually active, having multiple sexual partners, practicing unprotected sex, having sex with strangers [3], sex while or after drinking alcohol [4] or using drugs [5], sexual or partner violence [6] and transactional sex [7]. While these high risk sexual behaviors have been identified, experiences in childhood and the early teens that increase the likelihood of sexual risk behavior are less studied, including sexual and physical abuse during childhood.
Childhood sexual abuse (CSA) has been suggested to play a contributory role in HIV transmission among women and men [8] through associations with earlier sexual initiation, sexual activity, having more than one recent sexual partner, unprotected sex by not using a condom at the most recent sexual experience, and using alcohol or drugs at the most recent sexual experience [3, 9, 11–14]. Reports of child physical abuse (CPA) are associated with similar high risk sexual behavior patterns [9, 12–14].
On average, about 20 % of women and 8 % of men in North America report a history of sexual abuse [15]. There is some, but limited, knowledge about rates of child physical and sexual abuse in Africa and other low and middle income countries [15–17] and relatively little has been published on the relationship between CSA, CPA and HIV-related sexual risk behavior in these settings. Much of the research from Africa is restricted to studies among small unrepresentative samples in South Africa and Zimbabwe [18–23]. Results from one large-scale analysis from Swaziland concluded that 33 % of women reported an incident of sexual violence before they reached 18 years of age, and that sexual violence was associated with reported lifetime experience of sexually transmitted infections and unwanted pregnancy [24]. A recent global meta-analysis estimated the prevalence in Africa from self-report studies of sexual abuse as close to 20 % for both males and females. These rates, for females, are comparable to Australia and the USA, but for males they are double those reported from other regions of the world [25].
Physical abuse is reportedly much more common than sexual abuse [26], and both physical and sexual abuse have been shown to have serious and long-term consequences for physical, mental and sexual health and social adjustment in high-income countries [28]. Lack of knowledge about child abuse and its consequences has been attributed to the hidden and stigmatized nature of abuse, the complexity of definitions of physical and sexual abuse, and community understandings of acceptable child rearing practices including physical punishment [28].
Childhood abuse has been linked, in both retrospective and prospective longitudinal studies, to sexuality development and sexual preoccupation, lower birth control efficacy and increased likelihood of having a teen pregnancy, [29–31] and, as indicated earlier, HIV-related sexual risk behavior. The associations between child abuse and later high risk sexual behavior are dependent on, among others, gender, ages of the victim and perpetrator, their relationship and type of sexual abuse [32].
Childhood physical abuse has been associated with a three-fold increase in high HIV risk behaviors [9], and one study reported that 40 % of female adolescents and 23 % of males who engage in high risk sexual behavior experienced physical abuse as children [33]. Children who are victims of physical abuse are also described as having low self-esteem and poor impulse control, mental health problems, and tend to anti-social behaviour; in contrast, childhood sexual abuse has been found to have an independent association with high risk sexual behavior, irrespective of psychiatric condition [34]. Social norms of violence, male dominance and legitimization of harsh physical discipline, poverty, low community cohesion, household instability and poor child supervision are associated with childhood abuse.
While the relationship between intimate partner violence and HIV sexual risk factors is reasonably well established [35], the contributory role of child abuse, sexual and/or physical, is less well documented, especially in low income, high HIV prevalence settings, as well as among men [15]. In this study we report associations between reported CSA and CPA and high risk sexual behaviors from large random household probability samples of 18–32 year-old males and females (n = 14,657) from four sites in Zimbabwe, Tanzania and South Africa.
Methods
A baseline survey was conducted in 2005 in four sites in three countries—Zimbabwe, Tanzania and South Africa (two sites)—as part of a multi-year randomized control trial to rapidly increase knowledge of HIV status and mobilise community responses to reduce HIV incidence, stigmatization and high risk sexual behavior [37]. Thirty-four communities were sampled—10 in Tanzania, 8 in Zimbabwe and 16 communities in South Africa—with households and participants 18–32 years of age, randomly selected for questionnaire completion based on interviews.
The 10 communities in Tanzania were selected from Kisarawe, located in the Pwani region in Tanzania, an agricultural area with a largely Muslim population of approximately 160,000. The eight communities in Zimbabwe were selected from Mutoko, outside Harare, a rural district with a population of approximately 130,000. In South Africa, eight communities were selected from Vulindlela, close to Pietermaritzburg in KwaZulu-Natal, a mixed rural and semi-urban, largely Zulu-speaking area with a population of approximately 553,000. The other eight communities were selected from Soweto, South Africa’s most densely populated urban area adjacent to Johannesburg, with a population of approximately 2 million people from diverse cultural and geographic backgrounds.
After demarcating communities according to social and geographic criteria, all households in each community were counted either by door-to-door visits (Zimbabwe), Global Positioning Satellite mapping (Tanzania) or aerial photography (South Africa). Each household was visited and the people in each household were included in a list of members based on whether they had lived in the house for more than 4 months of that year and, during those 4 months, had slept in the household at least two nights a week. One member per household aged 18–32 years was selected for interview with the use of the Kish Grid method.
Baseline surveys were common with setting-specific demographic sections. The 130-item questionnaire collected demographic information, alcohol and drug use, sexual risk behavior (including childhood abuse), history of HIV testing and disclosure, social norms and HIV/AIDS stigma. No incentives were given for questionnaire completion. Socioeconomic status was assessed by setting-specific questions regarding the type and number of assets and household facilities. Childhood sexual abuse was assessed by the question ‘When you were growing up (before 12 years old), did you undergo any unwanted sexual experience?’, and childhood physical abuse by ‘When you were growing up (before 12 years of age), did you ever experience serious physical violence?’. Outcome variables included age at sexual debut, number of sexual partners, relationship to sexual partner, condom use, forced or violent sexual encounters, sexually transmitted infections, HIV status and testing history. The surveys were constructed in English, translated into local languages (Shona in Zimbabwe, Swahili in Tanzania, and Zulu and Sotho in South Africa), and checked by translating the text back into English. The questionnaire was piloted in each setting among convenient samples of 25–100 respondents.
Data for this analysis is available from 11,206 individuals (2,874 from Zimbabwe, 3,073 from Tanzania, 2,596 from Vulindlela, and 2,663 from Soweto). Logistic regression analyses were undertaken for men and women separately to examine the relationship between reported sexual and/or physical abuse as a child and reported sexual risk behaviors in adulthood, controlling for marital status, education and socioeconomic status. As a result of a qualitatively and quantitatively very similar relationship between reports of CSA and CPA and the sexual risk behaviors examined, childhood physical and sexual abuse was combined into a single category of reported childhood abuse (CSA and/or CPA).
Ethical review committees for each setting provided approval of the study. These included The Johns Hopkins Bloomberg School of Public Health, Mahimbili University College of Health Sciences, The Medical College of South Carolina and The National Institute of Medical Research (Tanzania); the University of California at Los Angeles, South General Institutional Review Board, the University of the Witwatersrand and the Human Sciences Research Council (South Africa) and the University of California, San Francisco and the Medical Research Council of Zimbabwe (Zimbabwe). All research was conducted according to recognised ethical principles for protecting human participants in international research. Verbal consent was obtained from respondents.
Results
Sample Characteristics
The estimated total size of the population in each site was 76,300 in Zimbabwe, 54,900 in Tanzania, 66,100 in Vulindlela and 152,500 in Soweto. The median household size ranged from three in Soweto to five in Zimbabwe, and four in Tanzania and Vulindlela. The response rate was 93.6 % in Tanzania, 84.7 in Vulindlela, 84.5 in Soweto and 84 in Zimbabwe [37]. Denominators in the results section vary by: a) the number of people who were eligible to answer the question as pre-determined by skip patterns, and b) the number of eligible individuals who answered the question.
The gender, age, education and other demographic characteristics of the samples for this analysis from each of the four sites is shown in Table 1.
Child abuse and Sexual Risk Behavior
The rates of assessed exposure—child physical abuse (CPA) and/or child sexual abuse (CSA)—and a range of outcome variables related to HIV risk, by gender and setting, are shown in Table 2.
The average rates of reported childhood sexual abuse ranged from 1.6 % among men in Vulindlela to 4.9 % among women in Soweto. In all settings, except Zimbabwe, rates of reported childhood sexual abuse were lower among men than women. Rates of reported childhood physical abuse were much higher than reports of sexual abuse, ranging from 4.3 % among women in Tanzania to 27.4 % among men in Zimbabwe. Reported physical abuse among women in Zimbabwe was roughly 2–3 times higher than in Tanzania and South Africa.
The mean age of sexual debut of those people who reported having had sex, ranged from 16 to 19 years, with the lowest average age reported among South African males (16.5 years). Reported number of lifetime partners varied widely across the four settings, with the lowest median number of lifetime partners reported by women in Zimbabwe (1), and the highest among men in Vulindlela and Soweto (5). Few women reported more than one sexual partner during the last 6 months, but roughly a quarter of men across all four settings reported more than one sexual partner. Close to half of the participants in the South African sites reported always or frequently using condoms, with the numbers being lower in Zimbabwe and Tanzania, especially among women.
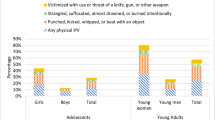
Lifetime alcohol and/or drug use varied by site, with men and women in the South African sites reporting higher use than in Zimbabwe and Tanzania. Around 10 % of women in all sites had experienced violence at the hands of a sexual partner, and close to 5 % of men (with other men). Recent forced sex (during the last 6 months) was reported by men (2.2–8 %) and women (2.5–8.1 %) in all four settings, and was almost twice as high among men as compared to women in Soweto, and also higher among men than women in Tanzania.
Participants in Zimbabwe reported low levels of HIV testing (below 10 %), as did men in Tanzania; but 40 % or more of women in Soweto, Vulindlela and Tanzania reported having had an HIV test. Up to 18 % of people indicated that they had tested HIV-positive at their last test. Most participants reputedly disclosed their HIV test results to sexual partners in all settings, close to 80 % and higher. The most common action after receiving HIV test results among men was reported to be a reduction in the number of sexual partners and, among women, to become monogamous—both were consistent across settings.
An analysis of sample characteristics and CSA and CPA indicated statistically significant effects for gender, marital status (except in Soweto), education (only in Soweto) and household SES (except Soweto). Men, in general, and both men and women who are single, were more likely to have experienced abuse as a child. In Soweto, less educated individuals were more likely to experience abuse as children, and in Tanzania, Zimbabwe and Vulindlela individuals of lower socioeconomic status reported being abused as children.
Relationships Between Child Abuse and Sexual Risk Behaviors
Table 3 shows the odds ratios depicting the relationships between reported child abuse (physical and/or sexual abuse combined) and sexual risk behaviors for men and women, adjusted for setting, education and household SES. Regressions were also conducted separately for CSA and CPA, and in the last column we report whether there was a difference in significance in the separate analyses.
Both reported sexual and physical abuse in childhood are related, in much the same way, to a range of reported sexual risk behaviors, alcohol and drug use, partner violence and HIV preventive behaviors among men and women in adulthood. Sexual debut occurs half a year younger among men and women who report childhood abuse as compared to those who don’t; men who report childhood abuse are one and a half times more likely to have had more than one sex partner during the last 6 months; and both men and women with histories of child abuse are more than twice as likely to have experienced forced sex during the last 6 months, and at least three times more likely to have a partner who ever hurt them.
Lifetime alcohol and drug use is significantly increased, especially among women, and is up to three times higher among those who reported childhood abuse as compared to those who did not. Both men and women who report childhood abuse are more likely to have taken an HIV test voluntarily. Men who report childhood abuse are more likely to report that they test HIV-positive as adults than non-abused men by a factor of three. And men with reported histories of childhood abuse are less likely to disclose their HIV status to a partner.
Discussion
The paper describes the relationships between reported childhood abuse—either sexual or physical—and reported sexual risk behaviors in adulthood in sub-Saharan Africa, a topic on which minimal research has been conducted, and certainly not among population-based samples. The results indicate significant associations between childhood abuse and the range of adult risk behaviors examined. We confirm associations between childhood abuse and adult sexual risk behaviour, and especially notable are rates of childhood abuse among African men, including sexual abuse, as well as high rates of recent forced sex and partner violence among men. The latter have not previously been reported from such sizable population-based samples in the region. In many prior studies, higher rates of childhood sexual abuse are reported among women [15]. Lower rates of reported childhood sexual abuse among men may be underestimated as a result of under-reporting, resulting from stigma and the fear of being considered ‘un-manly’ [38].
As far as we can discern, this is one of the first studies reporting a relationship between childhood abuse and sexual risk behaviors in adulthood among African men. Histories of sexual abuse have been reported in studies of HIV-positive men in the United States [39] and the EXPLORE study found that 40 % of more than 4,200 participants enrolled disclosed histories of sexual abuse. Moreover, EXPLORE found a significant association between a history of childhood sexual abuse and unprotected anal sex [40]. A recent meta-analysis of sexual risk behaviors among adolescent males in the United States reporting childhood sexual abuse found that they were more likely than boys without a history of abuse to have engaged in unprotected sex, to have had multiple sexual partners, and to report having caused a pregnancy [15].
The link between childhood abuse and adult sexual risk behavior is hypothesised to involve adverse mental health and social sequelae of childhood abuse. In the model of Finkelhor and Brown [29], this link is traumatic sexualisation leading to sexual preoccupation, aversion and/or ambivalence. Maladaptive emotional and behavioral associations with sex interfere with the development of close relationships and a sense of self-efficacy, and increase the individual’s sense of shame, isolation and stigmatization [30, 33, 41, 42]. Most child abuse is perpetrated by people who are known to a child and on whom a child depends for security and affection; the betrayal of trust and frequent denial [43] further complicate an abused child’s ability to relate to others.
While there are isolated reports of young virgins being used to ‘cleanse’ men of sexually transmitted infections and HIV [21], the so-called ‘virgin myth’ is not considered to be a major factor driving the sexual abuse of children in sub-Saharan Africa [44]. Instead, patriarchy and the obedience demanded of women and children in traditional societies, the acceptance of the view that men’s sexual urges are ‘uncontrollable’, endemic interpersonal violence, and substance abuse are believed to account for much of the abuse of children [45, 46].
The exposure to risk among young people troubled by such childhood events may be increased by their relative powerlessness to take up and implement HIV-preventive behaviors even when they have knowledge. Young people may need additional assistance beginning, for example, by screening for sexual abuse histories [47]. At the same time, greater public awareness and prevention of child abuse, both sexual and physical is needed as are services for affected children and families.
This study shares with many others the biasing effects of a cross-sectional design and retrospective reporting of childhood abuse. However, it does not have the selection bias of clinic-based or other selective samples [33, 48]. In contrast, its strength lies in large representative samples from three sub-Saharan African countries. The study adds to the emerging evidence of the carry-over of adverse effects from childhood abuse into maladaptive approaches to sexuality and relationships, including engaging in behaviors that put the individual at risk of HIV infection. At least two prospective studies, one a birth cohort [11] and the other a tracer study of adults for whom abuse reports were made before they were 12 years old—the same age reference used in this study [11]—have confirmed the association between child maltreatment and adult sexual risk behavior.
Sexual risk does not arise de novo at puberty when sexual interests and behavior usually manifest. Rather, it is moulded by social relationships and interpersonal encounters throughout child development, especially by experiences with the salience of abuse [49]. Abuse prevention is clearly important and there is evidence that both community- and family-based programmes have promise and some programs have demonstrated efficacy [50]. Abuse prevention is imperative in situations of known child vulnerability in order to prevent inter-generational cycles of sexual risk and HIV infection in high HIV prevalence environments. It is also important as a secondary prevention strategy among people living with HIV who have been abused in childhood [51].
References
World Health Organization, UNAIDS, UNICEF. Global HIV/AIDS response: Epidemic update and health sector progress towards Universal Access. Geneva: World Health Organization; 2011.
Pettifor AE, van der Straten A, Dunbar MS, Shiboski SC, Padian NS. Early age of first sex: a risk factor for HIV infection among women in Zimbabwe. AIDS. 2004;18(10):1435–42.
Senn T, Carey M, Vanable P, Coury-Doniger P, Urban M. Characteristics of sexual abuse in childhood and adolescence influence sexual risk behavior in adulthood. Arch Sex Behav. 2007;36(5):637–45.
Fisher JC, Cook PA, Kapiga SH. Alcohol use before sex and HIV risk: situational characteristics of protected and unprotected encounters among high-risk African women. Sex Transm Dis. 2010;37(9):571–8.
Lowry R, Holtzman D, Truman BI, Kann L, Collins JL, Kolbe LJ. Substance use and HIV-related behaviors among US high school students: are they related? Am J Public Health. 1994;84(7):1116–20.
Jewkes RK, Dunkle K, Nduna M, Shai M. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet. 2010;376(9734):41–8.
Maganja RK, Maman S, Groves A, Mbwambo JK. Skinning the goat and pulling the load: transactional sex among youth in Dar es Salaam, Tanzania. AIDS Care. 2007;19(8):974–81.
Kalichman SC, Gore-Felton C, Benotsch E, Cage M, Rompa D. Trauma symptoms, sexual behaviors, and substance abuse: correlates of childhood sexual abuse and HIV risks among men who have sex with men. J Child Sex Abus. 2004;13(1):1–15.
Bensley L, van Eenwyk J, Simmons K. Self-reported childhood sexual and physical abuse and adult HIV-risk behaviors and heavy drinking. Am J Prev Med. 2000;18(2):151–8.
Steel JL, Herlitz CA. The association between childhood and adolescent sexual abuse and proxies for sexual risk behavior: a random sample of the general population of Sweden. Child Abuse Negl. 2005;29(10):1141–53.
Wilson HW, Widom CS. An examination of risky sexual behavior and HIV in victims of child abuse and neglect: a 30-year follow-up. Health Psychol. 2008;27(2):149–58.
Mason WA, Zimmerman L, Evans W. Sexual and physical abuse among incarcerated youth: implications for sexual behavior, contraceptive use and teenage pregnancy. Child Abuse Negl. 1998;22(10):987–95.
Perkins DF, Jones KR. Risk behaviors and resiliency within physically abused adolescents. Child Abuse Negl. 2004;28(5):547–63.
Bornovalova MA, Gwadz MA, Kahler C, Aklin WM, Lejuez CW. Sensation seeking and risk-taking propensity as mediators in the relationship between childhood abuse and HIV-related risk behavior. Child Abuse Negl. 2008;32(1):99–109.
Homma Y, Wang N, Saewyc E, Kishor N. The relationship between sexual abuse and risky sexual behavior among adolescent boys: a meta-analysis. J Adolesc Health. 2012;51(1):18–24.
Lalor K. Child sexual abuse in sub-Saharan Africa: a literature review. Child Abuse Negl. 2004;28(4):439–60.
Finkelhor D. The international epidemiology of child sexual abuse. Child Abuse Negl. 1994;18(5):409–15.
Watts C, Zimmerman C. Violence against women: global scope and magnitude. Lancet. 2002;359(9313):1232–7.
Collings SJ. Childhood sexual abuse in a sample of South African university males: prevalence and risk factors. S Afr J Psychol. 1991;21(3):153–8.
Collings SJ. Child sexual abuse in a sample of South African women students: prevalence, characteristics and long-term effects. S Afr J Psychol. 1997;27(1):37–42.
Meursing K, Vos T, Coutinho O, et al. Child sexual abuse in Matabeleland, Zimbabwe. Soc Sci Med. 1995;41(12):1693–704.
Madu S. The prevalence and patterns of childhood sexual abuse and victim-perpetrator relationship among a sample of university students. S Afr J Psychol. 2001;31(4):32–7.
Peltzer K, Pengpid S. Sexual abuse, violence and HIV risk among adolescents in South Africa. Gender Bev. 2008;6(1):1462–78.
Reza A, Breiding MJ, Gulaid J, et al. Sexual violence and its health consequences for female children in Swaziland: a cluster survey study. Lancet. 2009;373(9679):1966–72.
Stoltenborgh M. van IJzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat. 2011;16(2):79–101.
Krug EG, Mercy JA, Dahlberg LL, Zwi AB. The world report on violence and health. Lancet. 2002;360(9339):1083–8.
Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S. Burden and consequence of child maltreatment in high-income countries. Lancet. 2009;373(9657):68–81.
Maniglio R. The impact of child sexual abuse on health: a systematic review of reviews. Clin Psychol Rev. 2009;29(7):647–57.
Finkelhor D, Browne A. The traumatic impact of child sexual abuse: a conceptualization. Am J Orthopsychiatry. 1985;55(4):530–41.
Noll JG, Trickett PK, Putnam FW. A prospective investigation of the impact of childhood sexual abuse on the development of sexuality. J Consult Clin Psychol. 2003;71(3):575–86.
Dube SR, Anda RF, Whitfield CL, et al. Long-term consequences of childhood sexual abuse by gender of victim. Am J Prev Med. 2005;28(5):430–8.
van Roode T, Dickson N, Herbison P, Paul C. Child sexual abuse and persistence of risky sexual behaviors and negative sexual outcomes over adulthood: findings from a birth cohort. Child Abuse Negl. 2009;33(3):161–72.
Senn TE, Carey MP, Vanable PA. Childhood and adolescent sexual abuse and subsequent sexual risk behavior: evidence from controlled studies, methodological critique, and suggestions for research. Clin Psychol Rev. 2008;28(5):711–35.
Luster T, Small S. Factors associated with sexual risk-taking behaviors among adolescents. J Marriage Fam. 1994;56(3):622–32.
Houck CD, Nugent NR, Lescano CM, Peters A, Brown LK. Sexual abuse and sexual risk behavior: beyond the impact of psychiatric problems. J Pediatr Psychol. 2009;35(5):473–83.
Jewkes R, Dunkle K, Nduna M, et al. Factors associated with HIV sero-status in young rural South African women: connections between intimate partner violence and HIV. Int J Epidemiol. 2006;35(6):1461–8.
Genberg B, Kulich M, Kawichai S, et al. HIV risk behaviors in sub-Saharan Africa and northern Thailand: baseline behavioral data from Project Accept. J Acquir Immune Defic Syndr. 2008;49(3):309–19.
Malkovich-Fong A, Jaffee S. Sex differences in childhood sexual abuse characteristics and victims’ emotional and behavioral problems: findings from a national sample of youth. Child Abuse Negl. 2010;34(6):429–37.
Welles S, Baker A, Miner M, Brennan D, Jacoby S, Rosser S. History of childhood sexual abuse and unsafe anal intercourse in a 6-city study of HIV-positive men who have sex with men. Am J Public Health. 2009;99(6):1079–86.
Mimiaga M, Noonan E, Donnell D, et al. Childhood sexual abuse is highly associated with HIV risk-taking behavior and infection among MSM in the EXPLORE study. J Acquir Immune Defic Syndr. 2009;51(3):340–8.
Sikkema K, Hansen N, Meade C, Kochman A, Fox A. Psychosocial predictors of sexual HIV transmission risk behavior among HIV-positive adults with a sexual abuse history in childhood. Arch Sex Behav. 2009;38(1):121–34.
Coffey P, Leitenberg H, Henning K, Turner T, Bennett RT. Mediators of the long-term impact of child sexual abuse: perceived stigma, betrayal, powerlessness and self-blame. Child Abuse Negl. 1996;20(5):447–55.
Erdmans M, Black T. What they tell you to forget: from child sexual abuse to adolescent motherhood. Qual Health Res. 2008;18(1):77–89.
Jewkes R, Martin L, Penn-Kekana L. The virgin cleansing myth: cases of child rape are not exotic. Lancet. 2002;359(9307):711.
Armstrong A. Consent and compensation: The sexual abuse of girls in Zimbabwe. In:Ncube W, ed. Law, Culture, Tradition and Children’s Rights in Eastern and Southern Africa (pp. 129-149). Dartmouth, USA: Aldershot; 1998.
LeClerc-Madlala S. Youth, HIV/AIDS and the importance of sexual culture and context. Social Dynamics. 2002;28(1):20–41.
Slonim-Nevo V, Auslander W, Ozawa M, Jung K. The long-term impact of AIDS-preventive interventions for delinquent and abused adolescents. Adolescence. 1996;31(122):409–21.
Senn T, Carey M. Child maltreatment and women’s adult sexual risk behavior: childhood sexual abuse as a unique risk factor. Child Maltreat. 2010;15(4):324–35.
Kendall-Tackett K. The health effects of childhood abuse: four pathways by which abuse can influence health. Child Abuse Negl. 2002;26(6–7):715–29.
Chen AC, Thompson EA, Morrison-Beedy D. Multi-system influences on adolescent risky sexual behavior. Res Nurs Health. 2010;33(6):512–27.
MacLeod J, Nelson G. Programs for the promotion of family wellness and the prevention of child maltreatment: a meta-analytic review. Child Abuse Negl. 2000;24(9):1127–49.
Sikkema K, Wilson P, Hansen NB, et al. Effects of a coping intervention on transmission risk behavior among people living with HIV/AIDS and a history of childhood sexual abuse. J Acquir Immune Defic Syndr. 2008; 4794):506-513.
Acknowledgments
The research was sponsored by the U.S. National Institute of Mental Health as a cooperative agreement, through contracts U01MH066687 (Johns Hopkins University), U01MH066688 (Medical University of South Carolina), U01MH066701 (University of California, Los Angeles), and U01MH066702 (University of California, San Francisco). In addition, this work was supported by the HIV Prevention Trials Network (HPTN Protocol 043) of the Division of AIDS of the U.S. National Institute of Allergy and Infectious Diseases, and by the Office of AIDS Research of the U.S. National Institutes of Health. Views expressed are those of the authors, and not necessarily those of sponsoring agencies. We thank the communities that partnered with us in conducting this research, and all study participants for their contributions. We also thank study staff and volunteers at all participating institutions for their contribution to the project.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Richter, L., Komárek, A., Desmond, C. et al. Reported Physical and Sexual Abuse in Childhood and Adult HIV Risk Behaviour in Three African Countries: Findings from Project Accept (HPTN-043). AIDS Behav 18, 381–389 (2014). https://doi.org/10.1007/s10461-013-0439-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-013-0439-7