
Abstract
Neonatal male circumcision (NMC) is an uncommon procedure in Southern Africa, but is being scaled up in Zambia for long-term HIV prevention. We conducted a cross-sectional survey on NMC with a convenience sample of mothers of newborn boys at two public clinics in Lusaka. Following the survey, mothers received information on availability of NMC, and uptake of the service was tracked. Predictors of uptake were assessed using bivariate and multivariate logistic regression. Of the 1,249 eligible mothers approached, 1000 (80 %) agreed to participate. Although 97 % of surveyed mothers said they definitely or probably planned to have their newborn son circumcised, only 11 % of participants brought their newborn sons for NMC. Significant predictors of uptake in adjusted models included: Older maternal age (AOR 3.77, 95 % CI 1.48–9.63 for age 36 and above compared to mothers age 25 and below), having attended antenatal care at an NMC site (AOR 2.13, 95 % CI 1.32–3.44), older paternal age (AOR 4.36, 95 % CI 1.28–14.91 for age 26–35 compared to fathers age 25 and below), and the infant’s father being circumcised (AOR 2.21, 95 % CI 1.35–3.62). While acceptability studies in Southern Africa have suggested strong support for MC among parents for having their sons circumcised, this may not translate to high uptake of newly-introduced NMC services.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Three clinical trials in sub-Saharan Africa have shown a 50–60 % reduction in HIV acquisition among circumcised heterosexual men, and observational studies suggest a similar protective effect if circumcision occurs neonatally [1–4]. In 2007 WHO/UNAIDS recommended expanding access to safe medical male circumcision (MC) in countries with high HIV prevalence and low MC prevalence [5]. Although adolescents and young adults are the primary target for the scale up of MC, WHO/UNAIDS also recommend promoting neonatal MC (NMC) as a long-term HIV prevention measure [5]. NMC is considered a safer, simpler, and cheaper procedure compared to circumcision at older ages [5–8]. While the benefits of NMC for HIV prevention will take longer to be realized, a cost-effectiveness study in Rwanda concluded that infant circumcision was cost effective, likely to be cost-saving, and had better potential (as compared to circumcision of adults and adolescents) to achieve the high MC coverage required over time to reach maximal reduction of HIV incidence [6].
Modeling studies have suggested that MC could reduce HIV prevalence in southern Africa by 25–67 %, but the actual impact of MC on the epidemic will depend upon service uptake [9]. Zambia, a southern African country with an MC prevalence of only 13 % and an HIV prevalence over 14 %, is among the countries implementing MC for HIV prevention [10]. The Zambian Ministry of Health (MOH) aims to reach 50 % MC coverage and 80 % NMC uptake by 2020 [11]. Only a few of Zambia’s 70-some tribal groups currently practice routine MC, including the Lunda and Luvale of the Northwestern Province, who perform adolescent circumcision as a rite of passage to adulthood [10, 12]. There is also a small (<1 %) Muslim population, who circumcise male children for religious reasons. Although there is no prescribed age for circumcision among Muslims in Zambia, the procedure is typically been done during infancy or early childhood, at private clinics under general anesthesia [10]. Although MC is uncommon in Zambia, studies there, as in several other sub-Saharan African countries with low coverage of MC, have indicated that MC is considered acceptable, even in non-traditionally circumcising groups [12–14]. A 2007 review found that 81 % of mothers and 71 % fathers were willing to have their sons circumcised in a clinical setting [13], and in Botswana, 92 % of post-partum mothers indicated willingness to have their newborn sons circumcised after receiving information about the procedure [14]. However, it remains unclear how acceptability expressed during surveys or focus groups translates into uptake of available MC services. The purpose of this study was to assess the acceptability and uptake of newly-introduced NMC services in Lusaka, Zambia.
Methods
Study Context
In November 2008, free neonatal MC services for male babies ≤28 days old were introduced in Lusaka at the tertiary care referral hospital, and subsequently at a public primary care clinic, as part of an operational research study examining the feasibility, acceptability and safety of three common NMC techniques under local anesthesia. As part of the larger study, a cross sectional survey was administered to a convenience sample of mothers of newborn boys in the post-natal wards at these two study sites between October 2009 and July 2010. Uptake of NMC services among participants in this sample was tracked.
Study Procedures
Surveys were administered by five experienced lay counselors who were trained in NMC counseling and survey research skills. Mothers who agreed to participate provided written informed consent before completing the survey in their preferred language. Lay counselors recorded their recruitment efforts on standardized recruitment logs.
Questionnaires were developed in English, informed by a literature review on MC and NMC acceptability surveys, and were professionally translated into two common local languages (Bemba and Nyanja). Questions were primarily closed-ended, and covered the infant’s birth, demographics (of both of the infant’s parents), knowledge, attitudes, and plans regarding MC and NMC.
Knowledge and attitudes were assessed through a series of statements, such as “Circumcision reduces a man’s risk of getting HIV from sexual intercourse with a woman”, and “Circumcised penises are more hygienic than uncircumcised penises,” to which the mother could agree, or disagree (or state that she was unsure).
After completing the survey, mothers received a brochure and brief informational talk on the benefits, risks and availability of NMC. Hours and locations of the NMC clinics were also provided. Following this, mothers were asked “Do you plan to have your son who was just born circumcised?” Acceptability was defined as a mother responding that she probably or definitely planned to have her son circumcised. Women who answered favorably about plans to have their infants circumcised were also asked at what age they thought it would be best to have the procedure done.
Survey participants who later brought their newborns to the NMC clinic for circumcision were matched with their completed questionnaires and were required to complete a separate informed consent process to have the circumcision performed within the larger study. NMC uptake was defined as the percent of mothers who participated in the survey who brought their sons to one of the study clinics for circumcision within the first 28 days of life (regardless of whether or not he was found to be eligible to be circumcised). Reasons for choosing to circumcise the newborn were assessed in a separate survey at the infant’s six-week follow up visit, using the open-ended question, “Why did you decide to have your baby circumcised?” and responses were coded for analysis.
Among mothers who had indicated that they probably or definitely would have their son circumcised but did not bring their infant to the NMC clinic, a random sample of 150 (every fourth respondent recruited by each lay counselor) was selected from the 605 who had provided valid telephone numbers. Trained research assistants conducted short telephone surveys between six and 12 months after initial contact with a lay recruiter to assess reasons for not bringing the infant for NMC.
Data Analysis
Data from parental questionnaires was entered into an Access database, and analyzed using SAS version 9.1.3 (SAS Institute Inc., Cary, North Carolina). To assess the representativeness of the study population, we utilized de-identified data from the Zambian Electronic Perinatal Record System (ZEPRS), an electronic medical record system that captures data amongst pregnant women and newborns attending antenatal care in the Lusaka public sector, as a comparison group [15]. Demographics (age, marital status, religion, education, parity, type of birth) were compared between study participants and all mothers who gave birth in the two clinics during the study period using Wilcoxon rank-sum test for continuous variables and the Pearson Chi-square test for categorical variables. Chi-square tests were also used to investigate differences in NMC uptake according to study site and recruiter. Logistic regressions were used to calculate crude odds ratios of sociodemographic, clinic and recruiter factors associated with NMC uptake. Parental sociodemographic variables that predicted uptake with p < 0.20 were then considered in an adjusted multivariate logistic regression model to determine independent predictors of NMC uptake. Associations between individual knowledge and attitude items (agreement or disagreement with a particular statement) and NMC uptake were examined using logistic regression models. Each individual item was adjusted for maternal age, ethnicity, education religion and parity; location of ANC; having another circumcised son; and paternal age, ethnicity, and circumcision status. ‘Unsure’ responses were treated as missing and excluded from the logistic regression. A value of p < 0.05 was considered as statistically significant.
Ethical Considerations
This study was approved by the Institutional Review Board at the University of Alabama at Birmingham, and the Research Ethics Committee at the University of Zambia. Participants received refreshments after completing the survey.
Results
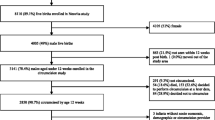
Between October 2009 and July 2010, we recruited 1,249 post-partum mothers of newborn boys in labour wards at two NMC sites, representing 8.4 % (1,249/14,759) of all women who gave birth at the two sites during the study period. Of the women approached, 1000 (80 %) agreed to complete surveys (see Fig. 1). Compared to all women who gave birth at the study sites during the same period, mothers in our sample were slightly younger (median age 26.0 years, interquartile range (IQR) 22.0–31.0, versus 26.4 years, IQR 21.8–31.4, p = 0.030), and a higher proportion were married (92 vs. 89 %, p = 0.004) and had completed at least some secondary school (74 vs. 66 %, p < 0.001), but a similar proportion were Christian (99 % in both groups) (Table 1). At the time of the survey, the median age of the participants’ infants was one day (IQR 0–1 day), and the median age of the infants’ fathers was 32 (IQR 27.0–37.0) years. One-fourth (25 %) of infants’ fathers were circumcised (according to the mothers), and 0.4 % of mothers did not know whether or not the father was circumcised.

NMC study recruitment procedure
Knowledge and Attitudes About MC
Among all respondents, 91 % (904/996) agreed with the statement that circumcision reduces a man’s risk of getting HIV through sexual intercourse with a woman, 77 % (767/995) agreed that circumcision reduces a man’s risk of acquiring certain STIs, 90 % (888/989) agreed that circumcision helps prevent urinary tract infections in baby boys, and 82 % (814/993) felt that circumcised penises were more hygienic than uncircumcised penises. Forty one percent (404/981) agreed that newborn babies were too young to be circumcised, and 23 % (228/989) agreed that circumcised men do not need to use condoms to prevent STIs and HIV.
Acceptability of MC
After receiving a short informational talk on NMC, 42 % (413/987) of mothers surveyed indicated that they were “definitely” planning to have their newly born son circumcised, 55 % (545/987) said they “probably” would have their son circumcised, and only 3 % (29/987) said either they “probably would not,” “definitely would not” or were unsure whether they would have their son circumcised. Of those who said they “definitely” or “probably” would have their sons circumcised, 90 % (851/950) said it would be best to circumcise their sons within the first month of life, 6 % (57/950) thought infancy (older than 1 month and <3 years) was the best time, 3 % (26/950) thought between four and 12 years was best, 0.3 % (3/950) thought age 13 or over was best, and 1 % (13/950) were unsure of the best age for circumcising their son.
Uptake of NMC
Eleven percent (110/1,000) of survey participants brought their sons to the NMC clinic for circumcision, a proportion which did not vary significantly by study site [11 % (77/667) at the referral hospital, and 10 % (33/333) at the primary care clinic, p = 0.44]. However, uptake did vary among individual lay counselors (recruiters), ranging from 5 % (16/298) to almost 19 % (37/195) (p < 0.0001). Combined uptake for male recruiters was 11.5 % (46/401) compared to 10.7 % (64/599) for female recruiters (p = 0.697).
Predictors of Uptake
Table 2 presents characteristics of parents who brought their infants for circumcision compared to those who did not bring their infants for circumcision. Significant maternal demographic predictors of uptake in univariate analyses included age between 26 and 35 years (OR 2.06, 95 % CI 1.33–3.21) and ≥36 years (OR 3.12, 95 % CI 1.68–5.79) compared to mothers ≤25 years, originating from a circumcising tribe (OR 2.01, 95 % CI 1.04–3.90), being Muslim (OR 8.30, 95 % CI 1.65–41.63), having completed at least some secondary education or above (OR 1.76, 95 % CI 1.05–2.95), having another son who was circumcised (OR 3.69, 95 % CI 1.77–7.70), parity of two or more (OR 1.92, 95 % CI 1.19–3.08) compared to being nuliparous, and having attended antenatal care at a clinic where NMC was offered (OR 2.43, 95 % CI 1.61–3.68). Fathers’ characteristics that predicted uptake in univariate modeling included age between 26 and 35 years (OR 4.88, 95 % CI 1.74–13.68) and ≥36 years (OR 5.26, 95 % CI 1.84–15.08) compared to fathers ≤25 years, originating from a circumcising tribe (OR 2.34, 95 % CI 1.25–4.39), and being circumcised (OR 2.67, 95 % CI 1.77–4.02). In multivariable logistic regression, the demographic variables that remained significant predictors of uptake were mother’s age (AOR 3.77, 95 % CI 1.48–9.63 for age 36 and above compared to mothers age 25 and below), having attended antenatal care at an NMC site (AOR 2.13, 95 % CI 1.32–3.44), father’s age (AOR 4.36, 95 % CI: 1.28–14.91 for age 26–35 compared to fathers age 25 and below), and the infant’s father being circumcised (AOR 2.21, 95 % CI 1.35–3.62).
Knowledge and attitude variables that significantly predicted uptake in multivariable models (adjusting for demographic variables) included: agreeing that circumcision reduces a man’s risk of getting certain STIs (AOR 3.39, 95 % CI 1.51–7.61), and disagreeing that newborns are too little to be circumcised (AOR 0.47, 95 % CI 0.28–0.78 for those who agreed with the statement compared to those who disagreed). Additionally, mothers who said they definitely planned to have their son who was just born circumcised were more likely to bring their son for circumcision than mothers who said they probably would, probably or definitely would not, or were unsure (AOR 5.12, 95 % CI 2.97–8.83) (Table 3).
Reasons for Choosing NMC
Based on responses to satisfaction surveys conducted at the infant’s six-week post-circumcision visit (n = 103), the most common reasons for parents deciding to have their newborn circumcised were for STI and HIV risk reduction (51 %), and for good hygiene or other health-related reasons, such as reduced risk of phimosis or urinary tract infections (34 %). Only 10 % of parents in this sample cited culture as an important factor in their decision. (See Fig. 2).

Reasons for choosing NMC (N = 103)
Reasons for Choosing Not to Have the Newborn Son Circumcised
In the random sample of 150 parents who had previously said they would probably or definitely have their sons circumcised but did not bring their newborns for NMC, 58 (39 %) of those called were unreachable (phone number was non-working or the mother was unavailable) and 92 completed the refusal survey. None of the mothers reached by telephone refused the survey. All mothers who completed the survey remembered speaking to a lay counselor about NMC, and 97 % said they had received a brochure on NMC. Most mothers (77 %) reported having consulted the infant’s father when deciding about NMC, 15 % consulted the infant’s grandparents, and 5 % consulted other family members, friends, or health care workers. A minority (17 %) of women did not consult anyone. In terms of who made the final decision about NMC, 46 % of mothers reported that it was the father alone, 25 % said they had made the decision together as a couple, 22 % said they alone had made the decision, and 9 % said that another family member (such as a grandparent) had made the decision. The most common reasons given for not bringing newborns for NMC were believing that the child was too young/wanting to wait until he was older (26 %), circumcision not being part of the family’s culture/tradition (12 %), fear of injury or death (10 %), wanting for the son to make the decision for himself (10 %), concerns about the infant experiencing pain (8 %), the mother being unwell following the birth or cesarean section (7 %), the mother having forgotten to bring the child (6 %), feeling that it’s not necessary (5 %), and the infant being unwell or dying soon after birth (5 %). Additional reasons mentioned by fewer participants included being too busy, not having transportation, a death in the family, and not wanting to leave the house soon after giving birth. (See Fig. 3). Most respondents (54 %) said they thought they would have the child circumcised in the future, at ages ranging from 4 months–14 years; 41 % said they did not know whether or not they would have their son circumcised, and 5 % said they would not have their son circumcised in the future.

Reasons for refusing NMC (N = 92)
Discussion
The primary aim of this study was to determine the acceptability and uptake of neonatal MC in Lusaka, Zambia, where NMC services have been introduced in public clinics as part of the country’s national MC strategy for HIV prevention [11]. While 40 % of mothers surveyed initially indicated that newborns were too small to be circumcised, after reviewing an NMC a brochure with the interviewer, 97 % said they would probably or definitely have their son circumcised, and 90 % of these specified ‘within the first month of life’ as age at which they would like to have the procedure done. This is consistent with findings from an NMC acceptability study in Botswana where 92 % of mothers surveyed expressed willingness to have their newborns circumcised in a clinical setting after reviewing a brochure about the procedure [14]. However, despite the apparent acceptability of NMC expressed by mothers during our survey, actual uptake of the procedure was only 11 %.
As in the Botswana NMC study, HIV and STI prevention were mentioned as motivating factors by parents who said they were planning to, as well as by parents who actually had their sons circumcised, and most mothers in this study believed that MC reduces the risk of being infected with HIV and STIs [14]. The majority of participants also believed that circumcision reduces an infant’s risk of urinary tract infections. However, knowledge of these health benefits clearly did not provide sufficient encouragement for most parents to have their newborns circumcised. The finding that NMC uptake was higher among women who had received antenatal care at an NMC study site was likely a result of exposure to the educational talks and messages given daily by lay counselors and health care workers at these sites during antenatal visits, providing mothers with repeated opportunities to learn about and discuss NMC with infants’ fathers before giving birth. The difference in uptake by recruiter (ranging from around 5 % to over 18 %) highlights the importance of carefully selecting the counselors to represent the program, if using this as a strategy to promote NMC. Although the male counselors appeared to be slightly more effective overall than the female counselors in this study, the difference was not significant, and the recruiter with the highest uptake (over 18 %) was a woman whose grandson had undergone NMC before she became a recruiter. Characteristics of effective recruiters were not a specific focus of this study, however, and thus it is difficult to draw conclusions about the reasons that some were more successful than others at promoting NMC.
This study is unique among circumcision acceptability studies in that it tracked service uptake following survey completion. A limitation of the study was the use of non-probabilistic sampling, which resulted in selection of a study population that was younger, had a higher level of education, was more likely to be married, and may have differed in other ways that are unknown. Thus, the findings may not accurately reflect views of all mothers who gave birth in Lusaka during the same period. Reliance on mothers’ self-reports of the fathers’ demographics and circumcision status may have affected the reliability of data. Furthermore, although interviewers were trained to remain neutral on NMC during the survey, the high percentage of mothers who reported they planned to have their sons circumcised may reflect a social desirability bias among respondents, who were asked about their plans to circumcise after reviewing a brochure on NMC with the interviewer, following the survey. It is also plausible that the findings represent true intentions and theoretical acceptance of NMC among mothers who received information on NMC, while the relatively low uptake demonstrates the strong influence of barriers that can prevent parents from having their newborns circumcised, such as lack of support from the infant’s father. Generalizability of results is also limited by the fact that the study did not directly assess acceptability among fathers, who appear to have the primary decision-making power related to NMC.
Despite its limitations, the results of this study are an important indication of the challenges that may lie ahead in reaching national NMC targets, and suggest the need for intensive communication interventions. Telephone refusal surveys indicated that among other barriers to NMC, many parents prefer to wait until their son is older to have him circumcised, and are fearful of death or injury that may result from the procedure. These findings are consistent with previous studies in Zambia, in which many parents and grandparents who supported circumcising their sons named ideal ages for circumcision that were outside of the normal window for NMC (ranging from a few of months of age to 12 years), and were concerned about infants undergoing a surgical procedure within their first couple months of life [12, 16]. NMC promotion strategies should focus on the specific benefits and safety of NMC compared to circumcision at older ages, to counter perceptions that performing the procedure soon after birth is dangerous.
In addition to other reasons cited by parents refusing NMC, it is possible that patterns of postnatal care seeking behavior may have affected the low uptake observed in this study. In Lusaka, only 64 % of women attend a postnatal visit within 6 weeks of giving birth [10]. Additionally, mothers who gave birth at the two study sites may have returned to their villages or homes outside of Lusaka following delivery, making it more difficult for them to access NMC. Compared to postnatal care coverage, antenatal coverage in Zambia is high: 99 % of pregnant women in urban areas attend at least one antenatal care visit with a skilled provider, and 59 % attend the recommended four visits [10]. Antenatal visits thus provide an opportune time to educate expecting mothers on NMC, and our results suggest that exposure to NMC information during antenatal care can help increase uptake. Messages should focus on prompting women to consider and discuss the topic with their husbands before giving birth. The finding from refusal surveys that fathers were the primary decision-makers in the majority of families who refused NMC mirrors results from our previous focus group study in Lusaka, in which both mothers and fathers were often involved in the decision-making process, but fathers, as the head of the household, tended to have the ultimate authority regarding circumcision of the newborn son [16]. It will thus be important to educate men about the benefits and availability of NMC, potentially with their partners at antenatal visits, given the current focus in Zambia on promoting male involvement. Furthermore, since parents in this study were found to be more likely to opt for NMC if the father was circumcised, it is likely that as adult circumcision prevalence increases in Zambia, uptake of NMC will also increase.
References
Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 trial. PloS Med. 2005;2:1112–222.
Bailey RC, Moses S, Parker CB, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomized controlled trial. Lancet. 2007;369:643–56.
Gray RH, Kigozi G, Serwadda D, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomized trial. Lancet. 2007;369:657–66.
Weiss HA, Quigley MA, Hayes RJ. Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. Aids. 2000;14(15):2361–70.
WHO & UNAIDS Technical Consultation. Male circumcision for HIV prevention: Research implications for policy and programming. Reprod. Health Matters. 2007;15(29):11–14.
Binagwaho A, Pegurri E, Muita J, Bertozzi S. Male circumcision at different ages in Rwanda: a cost-effectiveness study. PLoS Med. 2009;7:e1000211. doi:10.1371/journal.pmed.1000211.
Weiss H, Larke N, Halperin D, Schenker I. Complications of circumcision in male neonates, infants, and children: a systematic review. BMC Urol. 2010;10:2. doi:10.1186/1471-2490-10-2.
WHO, UNAIDS, & JHPIEGO. Manual for male circumcision under local anaesthesia. Version 2.5b. Geneva: WHO; 2007.
Nagelkerke N, Moses S, de Vlas S, Bailey R. Modelling the public health impact of male circumcision for HIV prevention in high prevalence areas in Africa. BMC Infect Dis. 2007;7:16.
Central Statistical Office, Ministry of Health, Tropical Diseases Research Centre, University of Zambia, & Macro International Inc. Zambia Demographic and Health Survey 2007. Calverton: CSO and Macro International Inc.; 2009.
Zambian Ministry of Health. National male circumcision strategy and implementation plan 2010–2020. Zambia: Lusaka; 2009.
Lukobo M, Bailey R. Acceptability of male circumcision for prevention of HIV infection in Zambia. AIDS Care. 2007;19(4):471–7.
Westercamp N, Bailey R. Acceptability of male circumcision for prevention of HIV/AIDS in sub-Saharan Africa: a review. AIDS Behav. 2007;11:341–55.
Plank R, Makhema J, Kebaabetswe P, et al. Acceptability of infant male circumcision as part of HIV prevention and male reproductive health efforts in Gaborone, Botswana, and surrounding areas. AIDS Behav. 2010;14(5):1198–202.
Chi BH, Vwalika B, Killam WP, Wamalume C, Giganti MJ, Mbewe R, et al. Implementation of the Zambia electronic perinatal record system for comprehensive prenatal and delivery care. Int J Gynaecol Obstet. 2011;113(2):131–6.
Waters E, Stringer E, Mugisa B, Temba S, Bowa K, Linyama D. Acceptability of neonatal male circumcision in Lusaka, Zambia. AIDS Care. 2011; doi:10.1080/09540121.2011.587508.
Acknowledgments
The authors would like to acknowledge the research and lay counselor team (Melissa Jaffray, Ketty Lwabila, Lucy Milambo, Salome Temba, Juliet Mphundu, Valentine Phiri, Francis Chato, Prisca Mwaba) and the staff of Matero Reference Clinic and University Teaching Hospital who supported the study. We are most grateful to the study participants. This project was supported by the Centers for Disease Control and the Elizabeth Glazer Pediatric AIDS Foundation, PHE Tracking Number: ZM.07.0183 FY Activity No.: 12525.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Waters, E., Li, M., Mugisa, B. et al. Acceptability and Uptake of Neonatal Male Circumcision in Lusaka, Zambia. AIDS Behav 17, 2114–2122 (2013). https://doi.org/10.1007/s10461-012-0297-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-012-0297-8