
Abstract
To inform the development of multilevel strategies for addressing HIV risk among labor migrants, 97 articles from the health and social science literatures were systematically reviewed. The study locations were Africa (23 %), the Americas (26 %), Europe (7 %), South East Asia (21 %), and Western Pacific (24 %). Among the studies meeting inclusion criteria, HIV risk was associated with multilevel determinants at the levels of policy, sociocultural context, health and mental health, and sexual practices. The policy determinants most often associated with HIV risk were: prolonged and/or frequent absence, financial status, and difficult working and housing conditions. The sociocultural context determinants most often associated with HIV risk were: cultural norms, family separation, and low social support. The health and mental health factors most often associated with HIV risk were: substance use, other STIs, mental health problems, no HIV testing, and needle use. The sexual practices most often associated with increased HIV risk were: limited condom use, multiple partnering, clients of sex workers, low HIV knowledge, and low perceived HIV risk. Magnitude of effects through multivariate statistics were demonstrated more for health and mental health and sexual practices, than for policy or sociocultural context. The consistency of these findings across multiple diverse global labor migration sites underlines the need for multilevel intervention strategies. However, to better inform the development, implementation, and evaluation of multilevel interventions, additional research is needed that overcomes prior methodological limitations and focuses on building new contextually tailored interventions and policies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The 2010 UNAIDS Report on the global AIDS epidemic estimated that in 2009, 33.3 million adults and 2.5 million children were living with HIV [1]. As the epidemic continues to grow, labor migrants are considered a vulnerable population for HIV infection [2]. According to the International Organization for Migration there are an estimated 214 million international migrants worldwide [3] sending around $414 billion remittance home to their families in 2009 [4]. One out of every 33 people in the world is a migrant. These numbers do not capture the tremendous heterogeneity both within and between migrant groups. Additionally, these numbers do not include all internal migrants, such as the estimated 16 million who move from rural to urban settings within their own countries, nor the additional 100 million who comprise China’s “floating population” [5].
There has been a shift from viewing HIV risk as predominantly an individual behavior to viewing it as impacted by social, economic, political, and/or cultural determinants. For example, HIV researchers have argued for understanding HIV risk through social vulnerability [6] or combined ecological models [7]. Such approaches are especially useful in understanding the complexities of labor migrants’ HIV risk and guided this review. Labor migrants are frequently separated from their spouses, nuclear and extended families as they work in mines, fields, or markets. They are forced into physically demanding and dangerous jobs, low wages, sub-par living conditions and have limited access to health care. They have limited social support networks and are forced to adapt to foreign culture, customs and languages. All these factors may contribute to increased HIV risk, though many of these factors are not necessarily specific to labor migrants and are shared with other vulnerable populations.
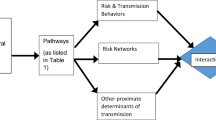
Although the pathways through which labor migration leads to the HIV transmission are not entirely understood, there is a growing body of scientific literature across the health and social sciences examining this issue in various labor migrant populations [8–10]. To date, this literature has not been reviewed as a cohesive body of knowledge. In organizing our approach to this review of the literature, we were guided by the need to look with a multidisciplinary perspective [11] for potentially modifiable determinants about which sufficient evidence exists that we should consider trying to address them and which could be used to formulate multilevel interventions (e.g., those that intervene with one or more of the following: individuals, couples, families, social and sexual networks, institutions, and entire communities). The four categories of potentially modifiable evidence-based multilevel determinants identified were: (1) policy; (2) sociocultural context; (3) health and mental health, and (4) sexual practices.
This investigation conducted a comprehensive review of the scientific literature that investigated possible associations between labor migration and HIV risk. This review summarizes prior empirical studies with a focus on examining evidence-based multilevel determinants that link labor migration and HIV risk. It also assessed for limitations and gaps in this prior research and provides recommendations for future research.
Methods
Search Methods
In order to assess the relevant literature, PubMed, and EBSCO were searched for English language articles using the following key words in various combinations: HIV, AIDS, migrant, migrants, labor migrants, mobility and migration. The reference sections of these reviewed articles were also examined to identify additional articles. Three edited volumes concerning migration and HIV/AIDS [12–14] were also reviewed and relevant articles were included. Additionally, given the first author’s extensive prior work on this topic, files from past searches were examined and relevant articles included. The authors acknowledge that despite extensive literature searches some relevant articles may have been omitted, particularly as labor migrants are sometimes classified by specific occupations (e.g., seafarers, truck drivers). A total of 216 articles or chapters were reviewed for possible inclusion.
Inclusion/Exclusion Criteria
The articles included examined labor migrants, defined as: individuals that leave their place of usual residence and move temporarily to a different locale (both in-country and abroad) to engage in remunerated activity with the intention of returning to their prior place of residence. Several mobile populations were excluded from this review for the following reasons. One, permanent immigrants were excluded as they have no intention to return to their places of origin and thus do not serve as a bridge population for transmission. Two, migrants whose income was generated by commercial sex work were excluded as their occupation is associated with distinct risk and protective behaviors. Three, border workers, those who commuted from their place of usual residence to their place of employment abroad, were excluded. Even though these individuals work across national borders, they have the ability to return home nightly and thus lack many of the characteristics shared by other labor migrants. Lastly, refugees and asylum seekers were excluded both because forced migration may produce distinct risks, and because they are not likely to return to their country of origin.
Only articles directly examining HIV/AIDS and labor migration were included. Studies that examined behavioral risk factors linked to labor migration with other conditions (e.g., substance abuse) but not HIV were not included. The articles included were published in peer- reviewed journals or books from 1989 to 2011 and were limited to original empirical research, excluding reviews of literature, editorials, newsprint, proposals, conference abstracts. Only English language literature was included. Using these criteria, two independent reviewers validated the selection of articles. Disagreement was resolved by consensus.
Multilevel Determinants
From a preliminary review of the entire database of articles, comprehensive lists of potentially modifiable determinants found to be associated with HIV risk were developed and grouped into the following four levels: (1) policy; (2) sociocultural; (3) health and mental health; (4) sexual practice (See Tables 2, 3, 4, 5). Policy determinants were those that arose from specific social policies such as those related to travel, migration, family accompaniment, employment, housing, finances and security and which were found to impact HIV risk. Sociocultural determinants were related to cultural norms, religious beliefs, acculturation, family beliefs and practices, and communities. Health and mental health determinants were defined as those factors related to individual health or mental health conditions, diagnoses, or experiences. Sexual practices determinants were those individual sexual activities, knowledge, and attitudes associated with sexual intercourse. The entire database was subsequently reviewed to code these potentially modifiable multilevel determinants. Additionally, the studies with available quantitative data summary statistics (odds ratio [95% confidence interval] and statistical significance [p value]) were recorded and documented in Table 6.
Results
Study Designs
The articles reviewed represented a variety of study designs including: quantitative (n = 46; 47 %); quantitative with biological samples (n = 25; 26 %); qualitative (n = 15; 15 %); mixed methods (n = 11; 11 %). Quantitative data was collected through written or verbal surveys [15–17]. Quantitative data with biological samples was typically gathered through population surveys with associated saliva or serum samples so as to report on HIV prevalence [18–20]. Qualitative data collected included semi-structured interviews, focus groups, participant and non-participant observations [21, 22]. Mixed methods studies combined quantitative and qualitative data sources [23, 24]. In South East Asia and the Western Pacific, the sample sizes tended to be larger, upwards of 5,000 [25, 26]. The studies in these regions were mostly surveys and some included biological samples. More qualitative and ethnographic studies were conducted in the Americas and Africa with a focus on understanding the sociocultural dimensions of HIV risk behavior [27, 28].
Given that labor migrants are highly mobile and often lack legal status, these studies faced sampling challenges. The samples studied were twice as likely to be non-probabilistic (n = 62; 64 %) as probabilistic (n = 35; 36 %). Sampling methods included convenience sampling [29], snowball sampling [30], targeted random sampling [31], and modified time space sampling [32]. One modified method of probabilistic space sampling was used in a village in Guinea where there were no population records to create a common random sample [33]. The researchers approach was to walk in randomly chosen lines and interview the nth person of the same gender that they came across, then choosing a new line and repeating the process.
Study Locations
The literature collected was sorted into geographical categories, using the WHO Regions to cluster countries (Table 1). Forty percent of the South East Asia studies arose from India (8 of 20) while countries with higher HIV/AIDS prevalence rates like Thailand [34] comprised only 20 % of regional literature (4 of 20). All but one of the Western Pacific studies were from China (22 of 23; 96 %). There were no studies from the Eastern Mediterranean region where there are known HIV/AIDS epidemics [35]. Sixty-three percent (61 of 97) of the studies collected data on labor migrants while they were away from home and 21 % (20 of 97) upon their return to their place of usual residence. Of the remaining studies, 8 % (6 of 97) studied labor migrants while they were in transit, 4 % (4 of 97) collected data in both sending and receiving places [36–38] and only one study surveyed the wives of migrants left behind at the sending place [39]. Internal migration was more heavily represented among the Western Pacific data (22 of 23; 96 %), reflecting high research interests in the large floating population in China, while studies on external migration predominated in the Americas (21 of 22; 95 %).
Policy Determinants
The studies found that labor migrants’ HIV risk was associated with a range of policy determinants (Table 2).
Prolonged and/or Frequent Absence
Some labor migrants were away more frequently and for more prolonged periods than others, and they tended to have more HIV risks. El-Bassel found that among male and female market workers in Almaty, Kazakhstan, those who reported longer trips also reported more sexual partners [40]. Kissinger found that among Latino migrant men in New Orleans, inter and intra state travel was associated with inconsistent condom use with casual partners [41]. Among Cameroon men, the prevalence of HIV infection increased with prolonged length of stay away from home [42]. Men who never left home had a prevalence of 1.4 %, those who were away for less than 31 days had a prevalence of 3.4 %, and of those who were away over 31 days, 7.6 % were infected. Similar trends were demonstrated with multi-partnering and non-spousal sexual relationships; men were more likely to participate in both the longer their absence from home. A different pattern was found among Hispanic workers in North Carolina where the likelihood of commercial sex worker use varied with time spent in North Carolina, but in a non-linear fashion [31]. Visiting commercial sex workers increased in the first years after migration, but peaked after 4 years and then slowly declined. Here, the investigators reported that initially sex worker visits increased as the migrants acquired financial resources, but then declined as they developed new social bonds.
Financial Status
Labor migration was linked with changes in socio-economic status which have been shown to be associated with elevated HIV risk [43, 44]. Among internal Chinese labor migrants exhibiting risky sexual behavior and low knowledge of HIV transmission, the majority worked long hours for little pay [45]. Among Mexican farmworkers in the U.S., poverty was associated with risk for HIV transmission [22]. These migrants came to the U.S. for economic reasons with dreams of a better life, but were often paid very low wages or cheated out of pay. In a study of Malawi men returning home from South Africa, higher financial status affected risk behaviors by attracting the attention of local women upon return home [21].
Difficult Working and Housing Conditions
Labor migrants get jobs less desired by locals that often have difficult working and housing conditions. Mine workers in South Africa described how the harsh living and working circumstances and sense of powerlessness shaped a man’s identity and risky sexual practices [28, 46]. Additionally, the risk of acquiring AIDS was dwarfed in relation to the physical dangers of daily work in the mines. Tajik migrants working in Moscow had difficulty finding safe housing due to discrimination and no legal status in Russia [47]. They must accept harsh living conditions on construction sites, in warehouses, or in parks.
Limited Access to Health Care
Limited access to health care for labor migrants made it difficult or impossible to get clinical or preventative care, including HIV/AIDS care. Without legal status, Tajik migrants in Russia were not able to access public health care institutions [47]. Private clinics that provided services charged very high rates for screening and treatment of STIs. While the majority (66 %) of migrant women working in Hong Kong had medical insurance as a condition of their employment, they reported that their ability to access quality health care was limited due to discrimination [48].
Legal Status
Labor migrants crossing political borders had limited legal status and less access to services than were afforded to citizens, including health care, social services, and government assistance programs. Some experienced outright hostility from local authorities. Tajik migrants mostly lived and work illegally in Russia. They experienced high rates of police harassment, beatings and arrests without provocation [47]. They reported feeling unprotected by law and without basic human rights.
Language Barriers
Not knowing the native language posed challenges for basic daily activities that were linked with increased HIV risk, such as increased stress. Additionally, language barriers could exclude labor migrants from healthcare and prevention initiatives in the receiving countries. In a sample of Mexican migrant laborers in the U.S. with misconceptions about modes of HIV transmission and poor knowledge of proper condom use, the overall level of local language skills was poor [49].
Sociocultural Context Determinants
Multiple studies found relationships between sociocultural context and HIV risk among labor migrants (Table 3).
Cultural Norms
HIV risk behaviors were shaped by labor migrants’ shared cultural beliefs regarding marriage, fidelity, condom use, and masculinity and the impact of migration on these norms. Often these norms differed between sending and receiving countries, such that labor migrants were somewhat freed from more traditional norms through migration. For some Malawian men, labor migration was a cultural rite of passage, a sign of maturity and masculinity [21]. Men migrated to earn money and their economic success upon return then provided an entry point to courting women. Multi-partnering was not perceived as social irresponsibility or immorality, but rather a symbol of economic and social success. A study of Mexican migrants showed that Mexican culture dictated fidelity in marriage, but greater emphasis was placed on maintaining the image of fidelity over actual abstinence from extramarital sexual relations [37]. Migrant men from Papua New Guinea demonstrated loyalty to their wives through material support [50]. Sexual fidelity was expected of the wife, since bride wealth was given for her, while the husband was the giver of bride wealth and thus fidelity was not expected of him. Furthermore, extramarital relations were not considered taboo unless they were with another man’s wife, as that was a violation of that man’s possessions. These men also reported a great sense of freedom with migration, where their extramarital relations were beyond community control.
Family Separation
While some migrant men were able to bring their wives or families with them to the labor locations, logistical or financial constraints left many men separated from their families. Away from their families, labor migrants missed their wives and children and the emotional and practical support which could help them to cope with the loneliness and stresses of migration [24]. Of men who internally migrated to Mumbai, India those who did not reside with their wives and/or families exhibited more risky sexual behaviors [25, 51]. Family separation due to migration also effected wives who were left behind by their husbands. In comparing Chinese wives of migrants to Chinese wives of non-migrant men, migrants’ wives had higher rates of multi-partnering, higher rates of HIV infection and lower rates of condom use [39].
Low Social Support
With migration comes the absence of community and psychosocial support. Labor migrants often reported that they had no one to talk to about stress and loneliness. Among Mexican migrants in New York City, 83 % of the men reported missing their families and lifestyles back home on a daily basis [24]. As levels of loneliness increased, condom use with new girlfriends decreased. In another study of Mexican migrants, farm workers in a South Carolina farm labor camp tolerated more sexual risk taking and substance abuse than those who lived in an Arizona farm camp [22]. The more conservative attitudes at the Arizona camp were thought to be a result of a larger and less ethnically isolated community as well as closer proximity to family and friends.
Health and Mental Health Determinants
Several health and mental health determinants were found to be associated with HIV risk in labor migrants (Table 4).
Substance Use
Alcohol and drug use were found to predispose labor migrants to HIV sexual risk behaviors. Latino migrants in the U.S. reported high rates of alcohol use and binge drinking before or during sex [40]. In a study of Latino day laborers solicited for sex in Los Angeles, those who screened positive for drug dependence were more likely to have sex with their solicitor [52]. A study conducted in Russia comparing labor migrants found that Eastern European migrants had higher alcohol and drug use and higher sexual risk whereas Central Asian migrants had low levels of substance use and moderate sexual risk [29]. Male Mexican migrant workers in the U.S. reported high levels of alcohol use, with 38 % drinking daily [24]. Half of the men reported not using condoms during sexual intercourse when drinking. Additionally, alcohol use was higher if there were fewer people from their hometown in their place of migration as well as if they called relatives in Mexico less frequently.
Other STIs
Several studies found an association between HIV infection and other STIs in labor migrants. Some researchers have argued that prevalence of other STIs could be a surrogate for HIV risk [53, 54]. Whether this holds true for all STIs or not is debated [55]. A study of fishermen in the Gulf of Thailand and Adaman Sea found that prior STI was significantly related to current HIV prevalence [56]. Without relying on self-reported history of STIs, another study concurrently tested seroprevalence of both HIV and syphilis and showed that between migrants who returned from India to Nepal and non-migrants in Nepal, the migrants had higher rates of both syphilis (25 % vs. 15 %) and HIV (10 % vs. 2.5 %) [57].
Mental Health Problems
Labor migrants were found to have higher levels of stress and depression. Among Puerto Rican migrants in New York and New Jersey, depression was associated with having multiple sex partners [58]. Among Central Asian migrants in Russia, those who exhibited low levels of condom usage and moderate sexual risk taking had high levels of depression [29]. In some cases, stress was experienced by migrants not only from the difficulties of relocation, lack of legal status, and absence of support but also from the difficult working conditions to which they were exposed. In particular, many African migrants working in mines witnessed accidents and fatalities of friends and coworkers [46]. These migrants had symptoms of post-traumatic stress disorder (difficulty concentrating, flashbacks, and nightmares, and social withdrawal) [59].
No HIV Testing
Several studies identified lack of prior HIV testing as a risk factor among migrants. Among long distance truck drivers in India, only 16 % of the 2,066 drivers surveyed had ever undergone HIV testing (range of 9–33 %) [60]. In China, out of 100 male migrants only one had previously been tested [61]. One study examining the feasibility and community acceptability of rapid HIV testing among Latinos in the United States showed that 66 % had never been tested for HIV [62]. In this study 75 % of participants consented to HIV testing and 97 % of participants favored using rapid HIV testing in the community.
Needle Use
While studies of injection drug use were excluded from this review, several studies highlighted needle use as a risk factor of their examined populations. A study of fishermen in the Gulf of Thailand and the Adaman Sea found an association concerning needles which was that migrants with tattoos had higher HIV prevalence [56]. The same study demonstrated that injection drug use was predictive only for the HIV-1 subtype B. Another study of Mexican migrants in California looked at a population that included 28 % injection drug users and found that they were more likely to engage in higher sexual risk than non-IDUs [63]. However, because the majority of them reported using needle exchange programs, the focus was more on risky sexual behaviors than risky needle behaviors.
Sexual Practices Determinants
The studies found a number of sexual practices associated with HIV risk among labor migrants (Table 5).
Limited Condom Use
Many studies found limited condom use among labor migrants. Cultural norms, health beliefs, impaired judgement and difficulty in obtaining condoms were identified as contributing factors. Internal migrant mine workers in South Africa reported very low rates of condom usage despite available free supplies [28, 46]. Many of the migrant miners expressed the need for flesh-to-flesh contact for sexual pleasure. Tajik migrants in Moscow reported regular unprotected sex for a variety of reasons: difficulty obtaining condoms due to their undocumented status in the city; some sex workers did not carry condoms; they didn’t use condoms when they were drunk, and sex with condoms diminished the physical pleasure [47]. Among Mexican migrant labors in the U.S., there was inadequate knowledge of proper condom use [49]. Less than half of these men always used condoms with occasional partners and about a third never used condoms with occasional partners. The female migrants’ condom usage was even lower as the migrants believed that a woman would be regarded as promiscuous if they carried condoms.
Multiple Partnering
Multiple partnering was frequently documented in the empirical literature, and through its relation to limited condom use, could become an HIV risk factor. Away from their regular partners and/or the social control of home communities, labor migrants often reported having sex with multiple female partners. In Russia, 30 % of Central Asian and Eastern European male labor migrants reported multiple female partners in the last 3 months [29]. When comparing migrants who traveled to India to non-migrants in Nepal, 49 % of migrants had multiple sex partners during the last 5 years, whereas only 25 % of non-migrants reported the same [57]. One study looked at the wives left behind by internally migrating husbands in comparison to wives of non-migrants in rural China. Wives of migrant men not surprisingly reported less frequent sexual intercourse with their husbands in the last month and also higher rates of multiple sexual partners than wives of non-migrants [39]. And among China’s migrant population 47 % of surveyed job seekers had sex outside of a monogamous relationship since leaving their place of origin [5]. In rural Tanzania, similar trends were found. The percent of non-migrants who had more than two partners in the last 12 months was 11 % whereas the percent of recent migrants was 24 % [64]. Multiple partnering is associated with a masculine identify, general physical and emotional well being, and “macho sexuality” in South African gold mines [46].
Visiting Sex Workers
The studies of labor migrants reported frequent visiting of sex workers. In a study of Tajik migrants in Moscow, all participants reported having unprotected sex with a commercial sex worker [47]. Many of these men reported doing so nearly weekly. Of Hispanic migrants surveyed in Durham, NC, 22 % reported visiting a sex worker in the past year [31]. On average, those migrants reported 6.7 sex worker visits per year. In a Bangladesh trucking industry survey, 54 % of the subjects had sex with at least one sex worker in the last year [20] and among married men 44 % had sex with at least one sex worker as well as their wife. Seafarers in Thailand reported that sex workers were easy to find. Their motivation for visiting sex workers was driven by three factors: loneliness and time out at sea, receiving a single payment for their work when arriving at a harbor, and strong peer pressure from coworkers [65].
Low HIV Knowledge
Many labor migrant populations lacked adequate knowledge about HIV/AIDS despite health education campaigns. Male migrants from Central Asia and Eastern Europe in Russia given an eight-item assessment of HIV/AIDS risk knowledge on average scored 3.6 items correctly [29]. For example, 45 % of the subjects thought that IUDs or oral contraceptives could prevent HIV infection. An assessment of migrant Mexican laborers’ knowledge of AIDS transmission showed high knowledge of major modes of transmission, but misconceptions about contracting HIV through mosquito bites, public restrooms and AIDS testing [49]. Some believed it was a disease of homosexuals and drug addicts and a person’s appearance could tell you if they were infected. Among Burmese migrants in Thailand given a knowledge assessment of HIV transmission, prevention and risk factors the overall score was 41, 36, and 82 % respectively [16]. Males scored higher than females in all categories and the level of knowledge increased with number of years of education completed. Some populations showed a much greater lack of HIV knowledge. Among internal male labor migrants in China, one study showed that only 37 % knew that condom use could prevent HIV transmission and 38 % knew that regular use of antibiotics could not prevent HIV infection [61].
Low Perceived HIV Risk
Studies documented low perception of personal HIV risk and low likelihood of HIV transmission. In South African mines the management of the mines had taken an active role in educating the migrants about AIDS through videotapes, pamphlets and posters [46]. Although the mine workers reported seeing the videos and being aware of the free condom supplies and told researchers that HIV was spread through unprotected sexual intercourse and that condoms could prevent its spread, nonetheless the majority of subjects interviewed reported unprotected sex with multiple sex partners. They were unsure about the existence of AIDS as they had never seen an infected person. They speculated that the western biomedical information was only part of the story and that traditional healers could possible cure things that hospitals could not. In a study in China, internal migrant workers had some misconceptions about modes of HIV transmission including the possibility of acquiring HIV from sharing food or swimming with an infected person or through a mosquito bite [45]. Despite these misconceptions, 71 % of migrants believed it was impossible for them to become infected. Nepalese migrants returned from India stated that despite their risky sexual behaviors, they did not feel they were at risk for HIV as they only selected healthy looking women for sex [66].
Young Age at Sexual Initiation
Few studies collected data on age at sexual initiation. One study of internal Chinese migrants demonstrated a correlation between multiple sex partners and early age at sexual initiation [67]. Another study comparing migrants and non-migrants in Kenya found there to be no universal pattern in age of first sex and risky sex behaviors [41].
Men Having Sex With Men
Few studies reported significant data on labor migrant men who had sex with men (MSM). One study of Mexican migrants in New York City reported that 4 of 50 male migrants ever had sex with a man, each reporting at least one episode of sexual contact without a condom since migration [24]. In a survey of Latino migrants seeking day labor jobs in the U.S., 38 % were solicited for sex by a male while at day labor recruitment sites, with only 9 % of those reporting sex with the solicitor [52]. In study of Mexican migrants in California, 37 % of the male migrants had sex with men in the last 90 days [63]. These men averaged 11 sexual partners in the past 2 months as compared to non-MSM who averaged three partners.
Magnitude of Effects
Table 6 reports on the summary multivariate statistics concerning HIV risk factors among labor migrants. Multiple studies demonstrated statistically significant findings within the levels of sexual practices (independent variables of multiple sex partners and paying sex workers) as well as health and mental health (independent variables of STI’s, drug use, and alcohol use). Overall, there were fewer studies with statistical findings for the levels of social policies (independent variables of prolonged and/or frequent absence) and sociocultural context (independent variables of visiting family and friends, partner’s education and employment). Multiple studies found elevations in HIV rates in migrants as compared with non-migrants.
Discussion
This systematic review showed that among labor migrants HIV risk was associated with potentially modifiable multilevel determinants in the levels of policy, sociocultural, sexual practice, and health and mental health. The policy determinants most often associated with HIV risk were: prolonged and/or frequent absence, financial status, and difficult working and housing conditions. The sociocultural determinants most often associated with HIV risk were: cultural norms, family separation, and low social support. The health and mental health determinants most often associated with HIV risk were: substance use, other STIs, mental health problems, no HIV testing, and needle use. The sexual practices determinants most often associated with increased HIV risk were: limited condom use, multiple partnering, clients of sex workers, and lack of HIV knowledge. Magnitude of effects through multivariate statistics were demonstrated more for health and mental health determinants and sexual practice, determinants than for policy or sociocultural determinants.
The consistency of these multilevel findings across multiple diverse global sites underlines the need for multilevel intervention strategies to prevent HIV transmission among labor migrants. While the determinants discussed were organized into categories for purposes of this review, it is important to point out the inter-relatedness of many of the determinants. For example, health behaviors such as HIV testing are driven by policies affecting access to health care. Mental health status can be affected by sociocultural context, such as low social support, and this can subsequently affect behaviors like substance abuse and multiple partnering. The problem of HIV risk among labor migrants requires far more than solutions at the individual behavioral level, and requires especially addressing problems in the policy and sociocultural context realms.
However, to understand in what ways labor migrants may differ from other vulnerable populations and to better inform the development, implementation, and evaluation of targeted multilevel interventions, additional research is needed. In particular, this research should address: (1) What are the social determinants of HIV risk? (2) Which HIV risk and protective factors at which levels are potentially modifiable under real world conditions? (3) Which potentially effective policies and programs are feasible, appropriate, and acceptable to the migrants, their families, and the organizations that work with them?
Future studies should further explore the complexity of labor migration and HIV risk in social contexts, particularly within the policy and sociocultural levels which have been under-investigated via quantitative methods. This would be specifically useful for those potentially modifiable policy determinants (legal status, working and housing conditions, access to health care, and prolonged and/or frequent absence) and sociocultural determinants (cultural norms, social support, and family separation) which could be modifiable through new interventions and policies, including human rights based strategies. Furthermore, instances where new policies are being introduced could serve as natural experiments, for investigation of important areas of how policies impact the structures and context of labor migration impact HIV risk and protection.
The findings of this review reveal several particular ways in which the current state of knowledge is incomplete due to methodological limitations of many existing studies and provides insight into how this can be improved upon. One, there is sometimes a lack of consistency in how investigators distinguished labor migration from other types of migration, which could be improved through more systematic attention to definitions and criteria.
Two, the study findings regarding geographical region indicate that migration and HIV have not been studied in all the necessary places. As noted earlier, there was a lack of Eastern Mediterranean studies despite the WHO noting that there are currently HIV epidemics in Djibouti, Sudan and Somalia and an underrepresentation of studies in Thailand and Myanmar, both with high HIV prevalence. Large global cities like Moscow, with over one million migrants and rising HIV prevalence, should be prioritized for investigation [68].
Three, regarding gender, HIV risk among the growing number of female labor migrants globally, is also under-investigated. We found that 48 studies (49 %) looked at both female and male migrants, whereas only 10 studies (10 %) looked exclusively at female migrants. Female labor migration needs to be investigated as a unique phenomenon, in some ways distinct from male labor migration. For example, Lin [69] reported that female migrants were at higher HIV risk because of intoxication, and Denner [63] reported that women were at higher HIV risk because of less self-efficacy. Other studies documented that in order to survive, some female labor migrants engaged in commercial sex work or transactional sex [70, 71].
Four, because many of the existing studies used non-probabilistic samples, qualitative data, or a narrow range of independent variables, many do not lend themselves to a systematic assessment of the strength of risk factors. While labor migrant populations are understandably difficult to study due to their mobility and undocumented status, research designs could be more rigorous in ways that would make cross-study comparisons possible. There is a need for more probabilistic sampling, more attention to key subgroups of migrants within samples, more attention to a broader range of factors/independent variables, and more collecting of biological samples to document HIV prevalence. Additionally, more longitudinal designs are needed that study the entire migration process, encompassing the sites of source, transit, destination and return [72].
Five, ethnographic and other qualitative data could continue to aid in better understanding the policy and sociocultural context levels, but could also contribute more to building interventions if they were more deliberately focused on intervention developmental issues such as related to service organizations and providers (including non-traditional health settings) and adaptation challenges. Mixed methods research designs could be useful in providing a more comprehensive and complex understanding of the multilevel processes involved in labor migration and HIV/AIDS, including especially the quantification and statistical analysis of a broader range of factors from the policy and sociocultural context levels [73]. Future studies should also focus on research implementation challenges such as: (1) how best to communicate with labor migrants (including perhaps through digital technology), and; (2) how to manage the constraints upon community leaders, organizations, and policymakers. The latter calls for more community collaborative approaches to research with labor migrants that increases their participation in development and implementation [74].
Six, there was a lack of investigation of protective factors for labor migrants at risk for HIV infection. Several studies [19, 33, 75] showed that when mobile populations had more risky sexual behaviors, they were also more likely to use condoms and to be tested for HIV, but protective factors could be conceived more broadly across all four levels. Kissinger’s study of Latino labor migrations in New Orleans found that membership in a social organization (e.g., a church related group) was associated with less female sex worker visits and more consistent condom use [76]. Saggurti’s study of migrants in Mumbai, India found that migrants living with their wives had lower rates of risky sexual behaviors [25]. Approaches to studying protective factors should consider a strength and resource approach [77, 78] which looks at individual, family, social, and cultural domains, and investigates what affirmative values, beliefs, and practices, are associated with HIV protective behaviors and could be a focus of preventive intervention strategies.
Lastly, with more labor migrants living with HIV/AIDS, new concerns regarding migration and HIV/AIDS are starting to be studied. These include attitudes towards HIV testing amongst migrants [79], positive HIV status as a cause for migration [80], delays in diagnosis of HIV/AIDS in migrants [81]. Other areas in need of study among labor migrants and their families include access and barriers to antiretroviral treatment, adherence, and prevention of maternal-child transmission.
References
UNAIDS Report on the Global AIDS Epidemic: UNAIDS; 2010.
HIV and International Labour Migration: UNAIDS Policy Brief. Geneva: UNAIDS; 2008.
International Migrant Stock: the 2008 Revision. United Nations; 2009 [cited 2011 Feb 4]. Available from: http://esa.un.org/migration.
World Bank’s migration and development brief 12 (April 23, 2010): outlook for remittance flows 2010–2011.
Anderson AF, Qingsi Z, Hua X, Jianfeng B. China’s floating population and the potential for HIV transmission: a social-behavioural perspective. AIDS Care. 2003;15(2):177–85.
Parker RG. Empowerment, community mobilization and social change in the face of HIV/AIDS. AIDS. 1996;10(Suppl 3):S27–31.
Waldo CR, Coates TJ. Multiple levels of analysis and intervention in HIV prevention science: exemplars and directions for new research. AIDS. 2000;14(Suppl 2):S18–26.
Decosas J, Kane F, Anarfi JK, Sodji KD, Wagner HU. Migration and AIDS. Lancet. 1995;346(8978):826–8.
Wolffers I, Fernandez I. Migration and AIDS. Lancet. 1995;346(8985):1303.
UNAIDS. Population mobility and AIDS: UNAIDS technical update. Geneva: UNAIDS; 2001.
Organista KC, Carrillo H, Ayala G. HIV prevention with Mexican migrants: review, critique, and recommendations. J Acquir Immune Defic Syndr. 2004;37(Suppl 4):S227–39.
Thomas F, Haour-Knipe M, Aggleton P. Mobility, sexuality and AIDS. Abington: Routledge; 2010.
Herdt G. Sexual cultures and migration in the era of AIDS: anthropological and demographic perspectives (International Studies in Demography). Oxford: Oxford University Press; 1997.
Hirsch J, Wardlow H, Smith DJ, Phinney H. The secret: love, marriage, and HIV. Nashville: Vanderbilt University Press; 2010.
Chen X, Stanton B, Li X, Fang X, Lin D, Xiong Q. A comparison of health-risk behaviors of rural migrants with rural residents and urban residents in China. Am J Health Behav. 2009;33(1):15–25.
Mullany LC, Maung C, Beyrer C. HIV/AIDS knowledge, attitudes, and practices among Burmese migrant factory workers in Tak Province, Thailand. AIDS Care. 2003;15(1):63–70.
Organista PB, Organista KC, Soloff PR. Exploring AIDS-related knowledge, attitudes, and behaviors of female Mexican migrant workers. Health Soc Work. 1998;23(2):96–103.
Martinez-Donate AP, Rangel MG, Hovell MF, Santibanez J, Sipan CL, Izazola JA. HIV infection in mobile populations: the case of Mexican migrants to the United States. Rev Panam Salud Publica. 2005;17(1):26–9.
Lagarde E, Schim van der Loeff M, Enel C, Holmgren B, Dray-Spira R, Pison G, et al. Mobility and the spread of human immunodeficiency virus into rural areas of West Africa. Int J Epidemiol. 2003;32(5):744–52.
Gibney L, Saquib N, Metzger J. Behavioral risk factors for STD/HIV transmission in Bangladesh’s trucking industry. Soc Sci Med. 2003;56(7):1411–24.
Chirwa WC. Migrant labour, sexual networking and multi-partnered sex in Malawi. Health Transit Rev. 1997;7(Suppl 3):5–16.
Apostolopoulos Y, Sonmez S, Kronenfeld J, Castillo E, McLendon L, Smith D. STI/HIV risks for Mexican migrant laborers: exploratory ethnographies. J Immigr Minor Health. 2006;8(3):291–302.
Hope KR. Population mobility and multi-partner sex in Botswana: implications for the spread of HIV/AIDS. Afr J Reprod Health. 2001;5(3):73–83.
Munoz-Laboy M, Hirsch JS, Quispe-Lazaro A. Loneliness as a sexual risk factor for male Mexican migrant workers. Am J Public Health. 2009;99(5):802–10.
Saggurti N, Schensul SL, Verma RK. Migration, mobility and sexual risk behavior in Mumbai, India: mobile men with non-residential wife show increased risk. AIDS Behav. 2009;13(5):921–7.
Yang X, Xia G. Gender, migration, risky sex, and HIV infection in China. Stud Fam Plan. 2006;37(4):241–50.
Kendall T, Pelcastre BE. HIV vulnerability and condom use among migrant women factory workers in Puebla, Mexico. Health Care Women Int. 2010;31(6):515–32.
Macheke C, Campbell C. Perceptions of HIV/AIDS on a Johannesburg gold mine. S Afr J Psychol. 1998;28(3):146–53.
Amirkhanian YA, Kuznetsova AV, Kelly JA, Difranceisco WJ, Musatov VB, Avsukevich NA, et al. Male labor migrants in Russia: HIV risk behavior levels, contextual factors, and prevention needs. J Immigr Minor Health. 2011;13(5):919–28.
Organista KC, Balls Organista P, Garcia de Alba JE, Castillo Moran MA, Ureta Carrillo LE. Survey of condom-related beliefs, behaviors, and perceived social norms in Mexican migrant laborers. J Community Health. 1997;22(3):185–98.
Parrado EA, Flippen C. Community attachment, neighborhood context, and sex worker use among Hispanic migrants in Durham, North Carolina, USA. Soc Sci Med. 2010;70(7):1059–69.
Kissinger P, Liddon N, Schmidt N, Curtin E, Salinas O, Narvaez A. HIV/STI risk behaviors among Latino migrant workers in New Orleans post-Hurricane Katrina disaster. Sex Transm Dis. 2008;35(11):924–9.
Kis AD. ABC for AIDS prevention in Guinea: migrant gold mining communities address their risks. AIDS Care. 2010;22(4):520–5.
WHO. HIV/AIDS in South East Asia region—situation update. Geneva: WHO; 2009.
WHO AIDS and Sexually Transmitted Diseases Regional profile [Jan 8, 2010]. Available from: http://www.emro.who.int/asd/hivsituation_regionalprofile.htm.
Coffee MP, Garnett GP, Mlilo M, Voeten HA, Chandiwana S, Gregson S. Patterns of movement and risk of HIV infection in rural Zimbabwe. J Infect Dis. 2005;191(Suppl 1):S159–67.
Hirsch JS, Higgins J, Bentley ME, Nathanson CA. The social constructions of sexuality: marital infidelity and sexually transmitted disease-HIV risk in a Mexican migrant community. Am J Public Health. 2002;92(8):1227–37.
Lurie MN, Williams BG, Zuma K, Mkaya-Mwamburi D, Garnett G, Sturm AW, et al. The impact of migration on HIV-1 transmission in South Africa: a study of migrant and nonmigrant men and their partners. Sex Transm Dis. 2003;30(2):149–56.
Qin QR, Ji GP, Xu J, Jiang QC, Hong H, Chu XY, et al. Risk of sexual HIV transmission among wives left behind and wives of nonmigrant men in rural areas of China. J Assoc Nurses AIDS Care. 2009;20(4):308–15.
Organista KC, Kubo A. Pilot survey of HIV risk and contextual problems and issues in Mexican/Latino migrant day laborers. J Immigr Health. 2005;7(4):269–81.
Brockerhoff M, Biddlecom A. Migration, sexual behavior and the risk of HIV in Kenya. Int Migr Rev. 1999;33(4):833–56.
Lydie N, Robinson NJ, Ferry B, Akam E, De Loenzien M, Abega S. Mobility, sexual behavior, and HIV infection in an urban population in Cameroon. J Acquir Immune Defic Syndr. 2004;35(1):67–74.
Booysen Fle R, Summerton J. Poverty, risky sexual behaviour, and vulnerability to HIV infection: evidence from South Africa. J Health Popul Nutr. 2002;20(4):285–8.
Krueger LE, Wood RW, Diehr PH, Maxwell CL. Poverty and HIV seropositivity: the poor are more likely to be infected. AIDS. 1990;4(8):811–4.
Li L, Morrow M, Kermode M. Vulnerable but feeling safe: HIV risk among male rural-to-urban migrant workers in Chengdu, China. AIDS Care. 2007;19(10):1288–95.
Campbell C. Migrancy, masculine identities and AIDS: the psychosocial context of HIV transmission on the South African gold mines. Soc Sci Med. 1997;45(2):273–81.
Weine S, Bahromov M, Mirzoev A. Unprotected Tajik male migrant workers in Moscow at risk for HIV/AIDS. J Immigr Minor Health. 2008;10(5):461–8.
Bandyopadhyay M, Thomas J. Women migrant workers’ vulnerability to HIV infection in Hong Kong. AIDS Care. 2002;14(4):509–21.
Organista KC, Organista PB, Garcia De Alba JE, Castillo Moran MA, Carrillo H. AIDS and condom-related knowledge, beliefs, and behaviors in Mexican migrant laborers. Hisp J Behav Sci. 1996;18(3):392–406.
Wardlow H. Men’s extramarital sexuality in rural Papua New Guinea. Am J Public Health. 2007;97(6):1006–14.
Saggurti N, Verma RK, Jain A, RamaRao S, Kumar KA, Subbiah A, et al. HIV risk behaviours among contracted and non-contracted male migrant workers in India: potential role of labour contractors and contractual systems in HIV prevention. AIDS. 2008;22(Suppl 5):S127–36.
Galvan FH, Ortiz DJ, Martinez V, Bing EG. Sexual solicitation of Latino male day laborers by other men. Salud Publica Mex. 2008;50(6):439–46.
Schachter J, Chow JM. The fallibility of diagnostic tests for sexually transmitted diseases: the impact of behavioral and epidemiologic studies. Sex Transm Dis. 1995;22(3):191–6.
Peterman TA, Lin LS, Newman DR, Kamb ML, Bolan G, Zenilman J, et al. Does measured behavior reflect STD risk? An analysis of data from a randomized controlled behavioral intervention study. Project RESPECT Study Group. Sex Transm Dis. 2000;27(8):446–51.
Pinkerton SD, Layde PM. Using sexually transmitted disease incidence as a surrogate marker for HIV incidence in prevention trials: a modeling study. Sex Transm Dis. 2002;29(5):298–307.
Entz AT, Ruffolo VP, Chinveschakitvanich V, Soskolne V, van Griensven GJ. HIV-1 prevalence, HIV-1 subtypes and risk factors among fishermen in the Gulf of Thailand and the Andaman Sea. AIDS. 2000;14(8):1027–34.
Poudel KC, Okumura J, Sherchand JB, Jimba M, Murakami I, Wakai S. Mumbai disease in far western Nepal: HIV infection and syphilis among male migrant-returnees and non-migrants. Trop Med Int Health. 2003;8(10):933–9.
Deren S, Kang SY, Mino M, Guarino H. Migrant drug users: predictors of HIV-related sexual and injection risk behaviors. J Immigr Minor Health. 2010;12(2):179–86.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed., text revision. Washington D.C.: American Psychiatric Association; 2000.
Pandey A, Benara SK, Roy N, Sahu D, Thomas M, Joshi DK, et al. Risk behaviour, sexually transmitted infections and HIV among long-distance truck drivers: a cross-sectional survey along national highways in India. AIDS. 2008;22(Suppl 5):S81–90.
He N, Wong FY, Huang ZJ, Ding Y, Fu C, Smith BD, et al. HIV risks among two types of male migrants in Shanghai, China: money boys vs. general male migrants. AIDS. 2007;21(Suppl 8):S73–9.
Sena AC, Hammer JP, Wilson K, Zeveloff A, Gamble J. Feasibility and acceptability of door-to-door rapid HIV testing among latino immigrants and their HIV risk factors in North Carolina. AIDS Patient Care STDS. 2010;24(3):165–73.
Denner J, Organista KC, Dupree JD, Thrush G. Predictors of HIV transmission among migrant and marginally housed Latinos. AIDS Behav. 2005;9(2):201–10.
Mmbaga EJ, Leyna GH, Hussain A, Mnyika KS, Sam NE, Klepp KI. The role of in-migrants in the increasing rural HIV-1 epidemic: results from a village population survey in the Kilimanjaro region of Tanzania. Int J Infect Dis. 2008;12(5):519–25.
Ford K, Chamratrithirong A. Migrant seafarers and HIV risk in Thai communities. AIDS Educ Prev. 2008;20(5):454–63.
Poudel KC, Jimba M, Okumura J, Joshi AB, Wakai S. Migrants’ risky sexual behaviours in India and at home in far western Nepal. Trop Med Int Health. 2004;9(8):897–903.
He N, Detels R, Chen Z, Jiang Q, Zhu J, Dai Y, et al. Sexual behavior among employed male rural migrants in Shanghai, China. AIDS Educ Prev. 2006;18(2):176–86.
Sassen S. The global city: New York, London and Tokyo. 2nd ed. Princeton: Princeton University Press; 2001.
Lin D, Li X, Yang H, Fang X, Stanton B, Chen X, et al. Alcohol intoxication and sexual risk behaviors among rural-to-urban migrants in China. Drug Alcohol Depend. 2005;79(1):103–12.
Chapman J, Estcourt CS, Hua Z. Saving ‘face’ and ‘othering’: getting to the root of barriers to condom use among Chinese female sex workers. Sex Health. 2008;5(3):291–8.
Munyewende P, Rispel LC, Harris B, Chersich M. Exploring perceptions of HIV risk and health service access among Zimbabwean migrant women in Johannesburg: a gap in health policy in South Africa? J Public Health Policy. 2011;32(Suppl 1):S152–61.
Deering KN, Vickerman P, Moses S, Ramesh BM, Blanchard JF, Boily MC. The impact of out-migrants and out-migration on the HIV/AIDS epidemic: a case study from south-west India. AIDS. 2008;22(Suppl 5):S165–81.
Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. Thousand Oaks: Sage Publishers; 2007.
Trickett EJ, Beehler S, Deutsch C, Green LW, Hawe P, McLeroy K, et al. Advancing the science of community-level interventions. Am J Public Health. 2011;101(8):1410–9.
Magis-Rodriguez C, Lemp G, Hernandez MT, Sanchez MA, Estrada F, Bravo-Garcia E. Going North: Mexican migrants and their vulnerability to HIV. J Acquir Immune Defic Syndr. 2009;51(Suppl 1):S21–5.
Kissinger P, Kovacs S, Anderson-Smits C, Schmidt N, Salinas O, Hembling J, et al. Patterns and predictors of HIV/STI risk among Latino migrant men in a new receiving community. AIDS Behav. 2012;16(1):199–213.
Walsh F. Traumatic loss and major disasters: strengthening family and community resilience. Fam Process. 2007;46(2):207–27.
Freudenberg N. Community capacity for environmental health promotion: determinants and implications for practice. Health Educ Behav. 2004;31(4):472–90.
Navaza B, Guionnet A, Navarro M, Estevez L, Perez-Molina JA, Lopez-Velez R. Reluctance to do blood testing limits HIV diagnosis and appropriate health care of sub-Saharan African migrants living in Spain. AIDS Behav. 2012;16(1):30–5.
Anglewicz P. Migration, marital change, and HIV infection in Malawi. Demography. 2012;49(1):239–65.
Zoufaly A, An der Heiden M, Marcus U, Hoffmann C, Stellbrink H, Voss L, et al. Late presentation for HIV diagnosis and care in Germany. HIV Med. 2012;13(3):172–81.
Lurie M, Harrison A, Wilkinson D, Abdool Karim SS. Circular migration and sexual networking in rural KwaZulu/Natal: implications for the spread of HIV and other sexually transmitted diseases. Health Transit Rev. 1997;7(Suppl 3):15–24.
Ondimu K. Labor migration and risky sexual behavior: tea plantation workers in Kericho District, Kenya. In: Thomas F, Haour-Knipe M, Aggleton P, editors. Mobility, sexuality and AIDS. Abingdon: Routledge; 2010.
Zuma K, Gouws E, Williams B, Lurie M. Risk factors for HIV infection among women in Carletonville, South Africa: migration, demography and sexually transmitted diseases. Int J STD AIDS. 2003;14(12):814–7.
Hanf M, Bousser V, Parriault MC, Van-Melle A, Nouvellet ML, Adriouch L, et al. Knowledge of free voluntary HIV testing centres and willingness to do a test among migrants in Cayenne, French Guiana. AIDS Care. 2011;23(4):476–85.
Lippman SA, Pulerwitz J, Chinaglia M, Hubbard A, Reingold A, Diaz J. Mobility and its liminal context: exploring sexual partnering among truck drivers crossing the Southern Brazilian border. Soc Sci Med. 2007;65(12):2464–73.
El-Bassel N, Gilbert L, Terlikbayeva A, West B, Bearman P, Wu E, et al. Implications of mobility patterns and HIV risks for HIV prevention among migrant market vendors in Kazakhstan. Am J Public Health. 2011;101(6):1075–81.
Evans AR, Parutis V, Hart G, Mercer CH, Gerry C, Mole R, et al. The sexual attitudes and lifestyles of London’s Eastern Europeans (SALLEE Project): design and methods. BMC Public Health. 2009;9:399.
Kramer MA, van Veen MG, de Coul EL, Geskus RB, Coutinho RA, van de Laar MJ, et al. Migrants travelling to their country of origin: a bridge population for HIV transmission? Sex Transm Infect. 2008;84(7):554–5.
Stulhofer A, Brouillard P, Nikolic N, Greiner N. HIV/AIDS and Croatian migrant workers. Coll Antropol. 2006;30(Suppl 2):105–14.
Ford K, Chamrathrithirong A. Sexual partners and condom use of migrant workers in Thailand. AIDS Behav. 2007;11(6):905–14.
Mercer A, Khanam R, Gurley E, Azim T. Sexual risk behavior of married men and women in Bangladesh associated with husbands’ work migration and living apart. Sex Transm Dis. 2007;34(5):265–73.
Li X, Fang X, Lin D, Mao R, Wang J, Cottrell L, et al. HIV/STD risk behaviors and perceptions among rural-to-urban migrants in China. AIDS Educ Prev. 2004;16(6):538–56.
Bronfman MN, Leyva R, Negroni MJ, Rueda CM. Mobile populations and HIV/AIDS in Central America and Mexico: research for action. AIDS. 2002;16(Suppl 3):S42–9.
Vaidya NK, Wu J. HIV epidemic in Far-Western Nepal: effect of seasonal labor migration to India. BMC Public Health. 2011;11:310.
Li L, Morrow M, Kermode M. Rural-to-urban male migrant workers’ vulnerability to HIV infection in Chengdu, China: qualitative findings from a mixed-method study. Work. 2010;37(4):375–86.
Song Y, Li X, Zhang L, Fang X, Lin X, Liu Y, et al. HIV-testing behavior among young migrant men who have sex with men (MSM) in Beijing, China. AIDS Care. 2011;23(2):179–86.
Hesketh T, Ye XJ, Li L, Wang HM. Health status and access to health care of migrant workers in China. Public Health Rep. 2008;123(2):189–97.
Bond V, Dover P. Men, women and the trouble with condoms: problems associated with condom use by migrant workers in rural Zambia. Health Transit Rev. 1997;7(Supplement):377–91.
Mberu BU, White MJ. Internal migration and health: premarital sexual initiation in Nigeria. Soc Sci Med. 2011;72(8):1284–93.
Smith DJ. Modern marriage, men’s extramarital sex, and HIV risk in southeastern Nigeria. Am J Public Health. 2007;97(6):997–1005.
Caballero-Hoyos R, Torres-Lopez T, Pineda-Lucatero A, Navarro-Nunez C, Fosados R, Valente TW. Between tradition and change: condom use with primary sexual partners among Mexican migrants. AIDS Behav. 2008;12(4):561–9.
Ford K, King G, Nerenberg L, Rojo C. Aids knowledge and risk behaviors among Midwest migrant farm workers. AIDS Educ Prev. 2001;13(6):551–60.
Hirsch JS, Meneses S, Thompson B, Negroni M, Pelcastre B, del Rio C. The inevitability of infidelity: sexual reputation, social geographies, and marital HIV risk in rural Mexico. Am J Public Health. 2007;97(6):986–96.
Stulhofer A. HIV related risks among Croatian migrant workers 2004–2006. AIDS Care. 2008;20(3):361–9.
Phinney HM. “Rice is essential but tiresome; you should get some noodles”: Doi Moi and the political economy of men’s extramarital sexual relations and marital HIV risk in Hanoi, Vietnam. Am J Public Health. 2008;98(4):650–60.
Puri M, Cleland J. Sexual behavior and perceived risk of HIV/AIDS among young migrant factory workers in Nepal. J Adolesc Health. 2006;38(3):237–46.
Sowell RL, Holtz CS, Velasquez G. HIV infection returning to Mexico with migrant workers: an exploratory study. J Assoc Nurses AIDS Care. 2008;19(4):267–82.
Yang X. Migration, detachment and HIV risk among rural-urban migrants in China. In: Thomas F, Haour-Knipe M, Appleton P, editors. Mobility, sexuality and AIDS. Abingdon: Routledge; 2010.
Yang X, Derlega VJ, Luo H. Migration, behaviour change and HIV/STD risks in China. AIDS Care. 2007;19(2):282–8.
Li S, Huang H, Cai Y, Ye X, Shen X, Shi R, et al. Evaluation of a school-based HIV/AIDS peer-led prevention programme: the first intervention trial for children of migrant workers in China. Int J STD AIDS. 2010;21(2):82–6.
Ehrlich SF, Organista KC, Oman D. Migrant Latino day laborers and intentions to test for HIV. AIDS Behav. 2007;11(5):743–52.
Burns FM, Evans AR, Mercer CH, Parutis V, Gerry CJ, Mole RC, et al. Sexual and HIV risk behaviour in central and eastern European migrants in London. Sex Transm Infect. 2011;87(4):318–24.
Meng X, Wang L, Chan S, Reilly KH, Peng Z, Guo W, et al. Estimation and projection of the HIV epidemic trend among the migrant population in China. Biomed Environ Sci. 2011;24(4):343–8.
Heffron R, Chao A, Mwinga A, Sinyangwe S, Sinyama A, Ginwalla R, et al. High prevalent and incident HIV-1 and herpes simplex virus 2 infection among male migrant and non-migrant sugar farm workers in Zambia. Sex Transm Infect. 2011;87(4):283–8.
Wang B, Li X, Stanton B, Fang X, Liang G, Liu H, et al. Gender differences in HIV-related perceptions, sexual risk behaviors, and history of sexually transmitted diseases among Chinese migrants visiting public sexually transmitted disease clinics. AIDS Patient Care STDS. 2007;21(1):57–68.
He N, Zhang J, Yao J, Tian X, Zhao G, Jiang Q, et al. Knowledge, attitudes, and practices of voluntary HIV counseling and testing among rural migrants in Shanghai, China. AIDS Educ Prev. 2009;21(6):570–81.
Jia Z, Wang L, Chen RY, Li D, Qin Q, Ding Z, et al. Tracking the evolution of HIV/AIDS in China from 1989–2009 to inform future prevention and control efforts. PLoS ONE. 2011;6(10):e25671.
Vissers DC, de Vlas SJ, Bakker R, Urassa M, Voeten HA, Habbema JD. The impact of mobility on HIV control: a modelling study. Epidemiol Infect. 2011;139(12):1845–53.
Fitzgerald K, Chakraborty J, Shah T, Khuder S, Duggan J. HIV/AIDS knowledge among female migrant farm workers in the midwest. J Immigr Health. 2003;5(1):29–36.
Deb AK, Deb M, Saha MK, Chakraborty S, Bhattacharya SK, Detels R. HIV transmission potential among local and migrant factory workers in Kolkata, India. AIDS Behav. 2009;13(5):928–38.
Saggurti N, Nair S, Malviya A, Decker MR, Silverman JG, Raj A. Male migration/mobility and HIV among married couples: cross-sectional analysis of nationally representative data from India. AIDS Behav. 2011 Aug 3 [Epub ahead of print].
Hu Z, Liu H, Li X, Stanton B, Chen X. HIV-related sexual behaviour among migrants and non-migrants in a rural area of China: role of rural-to-urban migration. Public Health. 2006;120(4):339–45.
Yang X, Derlega V, Luo H. Temporary migration and HIV vulnerability in China: findings from a comparative research. Exchange on HIV/AIDS, sexuality and gender. 2005(1):25–7.
Zuma K, Lurie MN, Williams BG, Mkaya-Mwamburi D, Garnett GP, Sturm AW. Risk factors of sexually transmitted infections among migrant and non-migrant sexual partnerships from rural South Africa. Epidemiol Infect. 2005;133(3):421–8.
Gupta I, Mitra A. Knowledge of HIV/AIDS among migrants in Delhi slums. J Health Popul Dev Ctries. 1999;2(1):26–32.
Islam MM, Conigrave KM, Miah MS, Kalam KA. HIV awareness of outgoing female migrant workers of Bangladesh: a pilot study. J Immigr Minor Health. 2010;12(6):940–6.
Hesketh T, Li L, Ye X, Wang H, Jiang M, Tomkins A. HIV and syphilis in migrant workers in eastern China. Sex Transm Infect. 2006;82(1):11–4.
Qu B, Guo HQ, Liu J, Zuo TM, Zhang Y, Sun G. The relationship between Chinese construction workers’ HIV/AIDS-related knowledge, attitudes and behaviour: a structural equation model. J Int Med Res. 2009;37(4):1202–10.
Yang H, Li X, Stanton B, Fang X, Lin D, Mao R, et al. Workplace and HIV-related sexual behaviours and perceptions among female migrant workers. AIDS Care. 2005;17(7):819–33.
Poudel KC, Jimba M, Okumura J, Sharma M, Poudel Tandukar K, Wakai S. Migration in far western Nepal: a time bomb for a future HIV/AIDS epidemic? Trop Doct. 2004;34(1):30–1.
Acknowledgments
This paper was completed through the support of the U.S. National Institute of Child Health and Human Development (K24 HD067095).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Weine, S.M., Kashuba, A.B. Labor Migration and HIV Risk: A Systematic Review of the Literature. AIDS Behav 16, 1605–1621 (2012). https://doi.org/10.1007/s10461-012-0183-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-012-0183-4