
Abstract
Highly active antiretroviral therapy (HAART) requires strict adherence to achieve optimal clinical and survival benefits. A study was done to explore the factors affecting HAART adherence among HIV positive adults by reviewing routinely collected patient information in the Centre for the AIDS Programme of Research in South Africa’s (CAPRISA) AIDS Treatment Programme. Records of 688 patients enrolled between 2004 and 2006 were analysed. Patients were considered adherent if they had taken at least 95% of their prescribed drugs. Generalized estimating equations were used to analyse the data. The results showed that HAART adherence increased over time, however, the rate of increase differed by some of the socio-demographic and behavioural characteristics of the patients. For instance, HAART adherence increased in both urban and rural treatment sites over time, but the rate of increase was higher in the rural site. This helped identify sub-populations, such as the urban population, that required ongoing adherence counseling.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Highly active antiretroviral therapy (HAART) has dramatically reduced morbidity and mortality among HIV-infected individuals [1–3], and requires strict adherence to attain optimal clinical and survival benefits [4–6]. Patients who take 95% or more of their prescribed medication benefit more from treatment than those who take less than 95% [4]. Identifying and overcoming factors that reduce adherence to HAART is therefore critical if optimal clinical and survival benefits are to be attained. Optimal adherence to HAART is often influenced by a variety of factors, including social, demographic, economic and behavioural [7, 8]. There have, however, been inconsistent findings regarding the association between adherence, demographic and economic factors. For instance, some studies have shown an association between adherence and age [9, 10], while others did not find such a relationship [11]. Income has also been associated with HAART adherence in some studies [12, 13], while others have concluded that there was no link between the two [14]. Social factors that include family support have been consistently associated with adherence [15]. The fact that associations between adherence and demographic and economic factors are observed inconsistently highlights the need for an evaluation and understanding of how these factors interact among themselves, and how they interact with other social, clinical and behavioural factors.
In Sub-Saharan African, studies have been conducted in countries such as Ethiopia [16], Uganda [17, 18], Uganda and Zimbabwe [19], South Africa [3, 20], Senegal [12, 21, 22], Nigeria [23] and Botswana [24], to identify factors affecting adherence to HAART. Some studies were cross-sectional and did not assess adherence over time. A limitation in some studies was the lack of multivariate analyses that included an evaluation of interaction terms between demographic, social and economic factors to control for potential confounding variables.
The cross-sectional work on the analysis of social, demographic, behavioural, economic and clinical factors influencing initial adherence for this cohort revealed that two-way interaction terms between age and cell phone ownership, gender and reason for taking an HIV test, as well as treatment site and income were important [25]. Although factors associated with optimal adherence at the initial stages of therapy give important information, factors that affect long-term optimal adherence may be more relevant, as lifetime adherence to HAART is required. It is therefore important to identify factors influencing adherence over time, as well as the relationships (interactions) between these factors. Studies that evaluate relationships between factors influencing adherence are limited in the literature, hence the motivation for this study. The aim of this study was to determine the predictors of optimal long-term adherence, and whether factors affecting initial adherence also influence long-term HAART adherence.
Methods
Study Design
The Centre for the AIDS Programme of Research in South Africa (CAPRISA) started a HAART rollout program in 2004. The CAPRISA AIDS Treatment (CAT) Programme offers HIV care services at two sites in KwaZulu-Natal, South Africa, namely the eThekwini Clinical Research site located adjacent to the Prince Cyril Zulu Communicable Disease Clinic in the center of Durban, and the Vulindlela Clinical Research site, located in a rural area outside the town of Howick, approximately 95 km from Durban. The programme started providing free HAART through a President’s Emergency Plan for AIDS Relief (PEPfAR) grant at a time when access to HAART in the public sector was limited. Adult patients with a CD4+ count below 200 cells/μl, or patients with World Health Organisation (WHO) stage 4 of HIV disease, were eligible for HAART initiation.
During the first month, patients visited the clinic once a week for the first 2 weeks and again 2 weeks later for intensive clinical monitoring. Thereafter, patients visited the treatment sites monthly to collect their treatment and to undergo a clinical examination. Prior to HAART initiation, all patients received three sessions of adherence education, motivation and preparedness training. All patients were on regimens containing two nucleoside reverse transcriptase inhibitors and one non-nucleoside reverse transcriptase inhibitor. Patients in the urban clinic received Efavirenz (EFV), Lamivudine (3TC) and Didanosine (ddI or ddI-EC). This regimen was chosen as it can be co-administered with anti-tuberculosis (TB) medication. The regimen in the rural clinic consisted of EFV, 3TC and Stavudine (d4T), which is recommended according to the South African HIV treatment guidelines [26]. A few pregnant patients (3.8%) received Nevirapine (NVP) rather than EFV.
Patient information was recorded on data collection sheets at the clinics; it underwent two levels of quality control, and was faxed to a central data management centre. The data analysed in this study consisted of a retrospective review of patients’ records in the CAT programme between June 2004 and September 2006. Only patients with pill count data for the initial visit, and at least one other clinic visit for the defined study period, were included in the analysis. The number of follow-up visits differed per patient, as some patients started treatment earlier and therefore had more visits, while some patients dropped out of the treatment programme prematurely. Approval for the data collection and analysis was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee.
Model Variables and Measurements
The data routinely collected at the treatment sites included the patients’ demographic details, medical history, CD4+ cell count and viral load, pill count, clinical status and a laboratory safety assessment. For this analysis, the outcome was measured using the pill counts data, and time-independent and time-varying covariates were chosen from the collected data. Measurement and coding of the outcome and covariates is described below.
Adherence Measurement
Adherence to HAART was measured using pill counts conducted by pharmacists at the treatment sites. Patients were provided with more medication than required, i.e. tablets were usually dispensed in multiples of 30, whereas visits were booked in multiples of 28 days. Patients were asked to bring all medication bottles and unused pills to each clinic visit, but were not told that the returns were to be counted. Adherence at every visit (monthly, i.e. 28 days) for all the drugs was calculated as the total number of drugs dispensed, minus the total number of drugs returned, divided by the total number of days between clinic visits, times the daily dose. This method takes into account the date of the clinic visits and adjusts for late return to the clinic (meaning pills would have been missed) and early return to clinic (meaning pills would still be available for return).
Outcome Variable
The outcome was optimal adherence to HAART, and patients were classified as optimally adherent if they took at least 95% of the prescribed drugs in a given regimen [4], otherwise, they were considered non-adherent. At each visit, the response variable was binary, indicating whether a patient was optimally adherent or not (1 = adherence score of 95% and above, i.e. the patient was optimally adherent; 0 = adherence score less than 95%, i.e. the patient was not optimally adherent).
Time Independent Covariates
As adherence was monitored very closely for the first month after initiation of HAART (three visits), compared to subsequent visits, the adherence for the first month (initial adherence) was treated as a covariate in the analysis. It has been argued that the use of a baseline response as a covariate in a longitudinal study permits the use of each subject as their own control to assess the effect of treatment over time [27, 28]. Initial adherence was calculated as the sum of drugs dispensed in the first month, minus the sum of drugs returned in the first month (over the three visits), divided by the number of days between the first and fourth visit multiplied by the daily dose. Those who took 95% of the prescribed dose were considered adherent (1 = optimal initial adherence; 0 = not optimal initial adherence).
Baseline demographic and socio-economic variables included in this analysis were age (in years); gender (1 = female, 0 = male); educational status (2 = no schooling, 1 = primary and 0 = secondary and higher); treatment site (1 = urban, 0 = rural); whether or not a patient lived with a partner (1 = living with a partner, 0 = not living with a partner); whether or not the patient was the source of household income (1 = source of household income, 0 = not a source of household income); access to tap water (1 = yes, 0 = no) and electricity (1 = yes, 0 = no), and whether a patient owned a cell phone (1 = yes, 0 = no). Other variables recorded at baseline and included were WHO HIV stage (3 = stage 1, 2 = stage 2, 1 = stage 3 and 0 = stage 4), CD4+ cell count (cells/μl), weight (in kilograms). Patients were asked why they did an HIV test and their responses included being unwell, testing for no specific reason, testing because a partner died of HIV, being ill and unfaithfulness. Reason for testing was therefore classified as follows: (2 = possible exposure to HIV, 1 = no specific reason and 0 = unwell).
Time Varying Covariates
Time was measured as a continuous variable representing monthly follow-up visits to the treatment site. The variable time starts with the value 1 for the first follow-up visit, 2 for the second visit, up to 17 for the seventeenth follow-up visit. Weight was measured at every follow-up visit and was modeled as a time-varying covariate.
Data Analysis
Differences in the baseline characteristics of CAT patients excluded and included in the analysis were compared using the chi-squared test for categorical variables, and the t-test for continuous variables. Socio-demographic and clinical characteristics of the study population were summarised using the median and inter-quartile range (IQR) for continuous variables and proportions for categorical variables. The trend of optimal adherence over time was tested using the Cochran-Armitage test for trend [29].
To account for multiple measurements of each patient (correlated data), and to allow all patients, regardless of the number of visits, to be included in the analysis, generalized estimating equations (GEEs) [30] were used to assess factors associated with optimal adherence over time. Quasi-likelihood function value obtained under the independence model criterion (QIC) [31] was used to select the model with the best fitting correlation structure. Model selection was done by first including all predictor variables in the model and then evaluating whether any interaction terms needed to be incorporated into the model. This was determined by fitting each of the product terms formed from the predictor variables, one at a time, and keeping the significant terms in the model. As GEE parameters are estimated using quasi-likelihood procedures, there is no associated likelihood underlying the model. Therefore, the usual likelihood ratio tests could not be applied to compare models. However, the generalized Wald test was used for model comparison [32].
The GEE method accommodates missing data, however, it yields valid estimates if missing data can be assumed to be ‘missing completely at random’ (MCAR). This means that missing values do not depend on the observed (previous) or unobserved outcomes [33, 34]. A logistic regression model was used to assess whether dropout in this study is independent of the previous outcome, i.e. whether the missing data mechanism is MCAR. All statistical tests were conducted at a 5% level of significance and analyses were done using SAS (version 9.1.3).
Results
Study Population
Between June 2004 and September 2006, 1,184 patients were enrolled in the CAT programme, 411 (35%) at the urban site, and 773 (65%) at the rural site. A total of 688 patients, 369 (54%) from the urban site and 319 (46%) from the rural site were included in the analysis. Only patients with pill count data for the initial and at least one other clinic visit were included in the analysis. There were no differences between those included in the study and those excluded with regard to age (mean: included = 34.1 years, excluded = 34.0 years; t-value = 0.13, P = 0.90), gender (males: included = 30.0%, excluded = 31.8%; chi-square-value = 0.43, P=0.51) and baseline CD4+ cell count (mean: included = 107.6 cells/μl, excluded = 111.5 cells/μl; t-value = 0.72, P = 0.47). Furthermore, power calculations were performed for the available sample size (688 patients) to detect a difference in proportion of adherent patients between the first follow-up visit and the final follow-up visit of 0.27. With a sample size of 600, this gave more than 90% power when a test of proportions was done.
Baseline Socio-Demographic and Clinical Characteristics of Patients
The baseline socio-demographic and clinical characteristics of patients included in the analysis are presented in Table 1. The median age of patients was 32.5 years (IQR: 28–38 years), 70% were male and 75% were not living with a partner. Over two-thirds of the patients had attained secondary or higher level of education (69%), and 28% of patients were classified as breadwinners. Over 90% of the patients stayed in households that had access to tap water and electricity, while 42% of the households had cell phones. At enrolment, the median weight was 60 kg (IQR: 53–69 kg), median CD4+ cell count was 108 cells/μl (IQR: 52–159 cells/μl) and 64% of patients were classified as WHO stage 3. Over half of the patients (56%) reported to have taken an HIV test as they were not well, while 26% reported no specific reason for testing and 18% took an HIV test as they were concerned that they had been exposed to HIV. In the initial month of treatment, 79% of the patients were at least 95% adherent to HAART.
Overall Optimal Adherence and Follow-up Visits
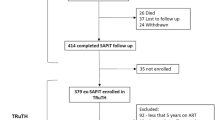
The number of follow-up visits ranged between 2 and 17 per patient, with the median of 8 (IQR: 5–12). Figure 1 presents the total number of patients expected at each visit, the number of patients who actually attended the visit and those who dropped out at each visit. The proportion of patients who dropped out gradually increased over the follow-up period.

Total number of patients expected at every visit classified by the number of patients who actually attended the clinic (non-dropouts) and those who dropped out
The proportion of patients who were at least 95% adherent (optimally adherent) to HAART increased from 58% at the first follow-up visit to 86% at the last follow-up visit (Fig. 2). The Cochran-Armitage statistic [29] (Z = 17.52 and P < 0.0001) provides strong evidence of an increasing adherence rate over time.

Optimal adherence and non-adherence rates over the follow-up visits
Selection of the Multivariate Model
Using the QIC [31], the correlation structure that fitted the data well was First-Order Autoregressive (AR1) structure, which reinforces the assumption of equally spaced measurement occasions.
Cross sectional analysis of predictors of initial optimal adherence showed that two-way interaction terms between age and cell phone ownership, gender and reason for taking an HIV test, and treatment site and income were significant [25]. Using the same data set, we evaluated whether these predictors of initial adherence also predicted long-term adherence using the GEE method. The results were not significant (Wald statistic = 4.78 with four degrees of freedom, P = 0.31), indicating no association between long-term optimal adherence and the interaction terms associated with initial adherence.
To further examine the relationship between long-term optimal adherence and other variables, a model was built by fitting all the predictor variables (listed in Table 1), followed by an assessment of whether any interaction terms need to be incorporated into the model. Consequently, the final model contained five two-way interaction terms and all the predictor variables. The two-way interactions were between gender and time, treatment site and time, reported reason for taking an HIV test and time, age and gender, as well as age and educational attainment (Table 2).
Predictors of Optimal Adherence
After controlling for other variables in the model, optimal adherence was significantly higher when patients had cell phones than when they did not have cell phones [adjusted odds ratio (aOR) = 1.260, 95% confidence interval (CI): (1.056, 1.503), P = 0.010] and when they lived with a partner compared to when they did not live with a partner [aOR = 1.335, 95% CI: (1.097, 1.625), P = 0.004] (Table 2).
Optimal HAART adherence increased on average over time, however, since interactions with time were significant, the rate at which optimal adherence increased differed by treatment site, gender and the patient’s reported reason for taking an HIV test. Age interacted significantly with gender and education. The interaction effects are presented below.
Interaction Between Gender and Time
Optimal HAART adherence increased over time for both males and females. However, since there was a significant interaction between gender and time, the rate of increase was not the same for males and females after controlling for other covariates in the model. The rate of increase was 7.4% higher for females than for males [aOR = 1.074, 95% CI: (1.034, 1.116); P < 0.001] (Table 2). Estimated probabilities of optimal adherence were higher for males at the beginning of the follow-up visits, but by the end of the study period (17th follow-up visit), they were similar for both groups (Fig. 3a).

All the two-way interaction terms in the final model of optimal adherence
Interaction Between Treatment Site and Time
The rate at which optimal adherence increased over time differed in the urban and rural treatment sites. After controlling for other variables in the model, the rate of increase in optimal adherence was 6% higher in the rural treatment site than in the urban treatment site [aOR = 1.06, 95% CI: (1.002, 1.100); P = 0.004] (Table 2). The estimated probability of optimal adherence at the first follow-up visit was 66% at the rural site and 86% at the urban site (Fig. 3b). Since the rate of increase was higher in the rural site relative to the rate of increase in the urban site, the gap in adherence between the treatment sites gradually decreased over time until, by the end of the study, the estimated optimal adherence probabilities were similar (at 91 and 92%, respectively).
Interaction Between Reason for Taking an HIV Test and Time
Optimal adherence increased over time, but the rate at which it increased differed with the patient’s reported reason for taking an HIV test. The rate of increase in optimal adherence was 5.8% higher over the study period for patients who tested due to possible exposure to HIV, than for patients who tested because they were unwell [aOR = 1.058, 95% CI: (1.010, 1.108); P = 0.016] (Table 2). There was, however, no significant difference in the rate of change of optimal adherence between patients who tested because they were unwell and those who reported no specific reason for taking an HIV test [Z = −0.43, P = 0.666] (Table 2). Further analysis revealed that the rate of increase in optimal adherence over the study period was 7% higher for patients who tested due to possible exposure to HIV, than for those who reported no specific reason for taking an HIV test [aOR = 1.069, 95% CI: (1.016, 1.126), P = 0.0107).
Figure 3c indicates that the estimated probabilities of optimal adherence for patients who tested because they were unwell, and those who reported no specific reason for taking an HIV test, were similar throughout the study.
It is again shown in Fig. 3c that at the beginning of the follow-up period, estimated probabilities of optimal adherence for patients who tested due to possible exposure to HIV were less than the estimated probabilities of patients who reported no specific reason for taking an HIV test, as well as those who tested because they were unwell. However, during the middle of the follow-up visits, estimated probabilities were similar for all the reported reasons. Towards the end of the study, the probabilities of optimal adherence were higher for patients who tested due to possible exposure to HIV than those who reported no specific reason for testing for HIV, or those who tested because they were unwell.
Interaction Between Age and Gender
Optimal HAART adherence differed by age for males and females. As the age of patients increased, females tend to adhere better to HAART than males [aOR: 1.024; 95% CI: (1.006, 1.043), P = 0.010]. It is shown in Fig. 3d that the estimated probabilities of optimal adherence were higher with younger males than with younger females, whereas with older patients, estimated probabilities were higher with females than males.
Interaction Between Age and Education
Optimal HAART adherence differed by age at different education levels. Among older patients, those with no schooling were less likely to achieve optimal HAART adherence than those with secondary and higher education [OR = 0.97; 95% CI: (0.94, 0.99); P = 0.012] (Table 2). There was, however, no significant difference in optimal HAART adherence between patients with secondary education and patients with primary education, regardless of age [Z = −0.16, P = 0.875)] (Table 2). Further analysis revealed that as patients got older, those with primary education were more likely to achieve optimal adherence than those with no schooling [aOR = 1.03, 95% CI: (1.002, 1.070); P = 0.048]. Figure 3e indicates that the estimated probabilities of optimal adherence by patients decreased with age. More specifically, the probability of optimal adherence for patients with secondary and primary education was similar for all ages, whereas probabilities of optimal adherence for those with no schooling were higher for younger ages and lower for older ages, relative to those with primary and secondary schooling.
Impact of Dropout on the Analysis
The analysis revealed that dropout did not depend on previous outcome (Chi-squared-value = 0.103 with one degree of freedom; P = 0.748). It can therefore be concluded that MCAR holds and as a result, GEE method yielded valid estimates.
Discussion
Consistent with results from recent longitudinal studies in Sub-Saharan Africa [16, 19], the findings showed that optimal HAART adherence increased with time, indicating that programmatic interventions conducted during the CAT programme may have had a positive impact on adherence. These interventions included patients being exposed to on-going peer education when queuing for services within the clinic, and through one-on-one session with a peer educator at the end of the clinic visit after the pills were collected. Every 6 months, patients received individual education on adherence maintenance. This highlights the importance of prioritising adherence counseling when setting up new HAART clinics. These results reinforce the message that it is possible to achieve and sustain high levels of HAART adherence in Sub-Saharan Africa, given strong support measures.
Studies have consistently shown that demographic characteristics are generally poor predictors of HAART adherence [35, 36]. However, the results from this study demonstrate that demographic factors predict HAART adherence through interactions among themselves or with other variables. For instance, an interaction between age and educational attainment predict HAART adherence. More specifically, as patients get older, adherence decreases over time, and the decrease is more pronounced with patients who have no schooling and in male patients.
HAART adherence increased over time but at different rates in males and females. Males had higher adherence at the beginning of the follow-up period but by the end of the study period, adherence was similar between males and females. This might be explained by social and behavioural factors associated with HAART adherence being different in males and females [37]. For instance, women are generally responsible for care-giving duties which might hamper adherence at the beginning of treatment, until they get used to the new routine of taking their own medication [37, 38].
HAART adherence has been higher in urban clinics than in rural clinics, which has been attributed to the latter being less well resourced [39]. However, the rate at which adherence increases with time is higher in the rural clinic than in the urban clinic. Studies have shown that in rural settings, optimal adherence tends to increase over time [40]. Since rural populations live in a more communal setting, the positive impact of HAART on HIV positive-patients might be more visible, which may positively influence optimal adherence to HAART.
Patients who lived with a partner adhered better to HAART than those who lived with no partner. Lack of social support has been associated with a decrease in adherence [41] and living with a partner has been associated with increased social support and optimal adherence [42]. Furthermore, cell phone ownership enhanced long-term optimal HAART adherence. This reinforces proposed interventions of providing memory aids for dosing times that include the use of new technologies such as reminders through cell phones [43–47], and verbal or text messaging for check-up reminders and general adherence messages [48].
Three shortcomings are acknowledged in our research. Firstly, adherence was assessed only through pill counts. Pill counts method is attractive due to its simplicity and empirical nature; however, it has disadvantages that include patients switching medicines between bottles or discarding pills before visits [47]. Despite these problems, it has been shown that pill counts method has a strong linear relationship with viral load [49].
Secondly, interactions between variables were identified using the data and model fit techniques. The interactions were not pre-specified or expected during data collection. Detailed information on why these interactions influenced adherence was therefore not collected, and the reasons for some of these findings cannot be explained.
Thirdly, an equal interval (monthly) between successive follow-up visits by all patients was assumed. In reality, some patients visited the clinic a number of days earlier or later than scheduled appointments. However, the impact of this assumption on the analysis is negligible for a number of reasons. The patients in the CAT programme have shown excellent clinic attendance with scheduled appointment. In addition, patients were given 2-day buffer stock with each supply to cover appointment delays and this was accounted for in calculating the adherence rate. Generally, when we say monthly data, we do not expect an equal number of days in every month. Furthermore, the effect of unequally spaced interval correlation structures was tested using QIC and was found to be insignificant, which reinforces the assumption of equal interval between clinic visits.
The study showed that HAART adherence increased over time on average, however, the rate at which it increased differed by treatment site, gender and the patient’s reported reason for taking an HIV test. Consequently, due attention should be paid to address the specific needs of each group of patients, specifically with respect to urban–rural and gender differentials. HAART adherence over time increased for patients with cell phones and patients living with a partner, and decreased as age of patients’ with no schooling increased. HAART programs need to take these factors into account in the design and implementation of long-term adherence strategies. Specific groups of patients at risk for less than optimal adherence should be targeted with long-term adherence boosting sessions tailored to their specific needs.
References
Hogg RS, Heath KV, Yip B, et al. Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA. 1998;279(6):450–4.
Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet. 2003;362(9377):22–9.
Nachega JB, Stein DM, Lehman DA, et al. Adherence to antiretroviral therapy in HIV-infected adults in Soweto, South Africa. AIDS Res Hum Retroviruses. 2004;20(10):1053–6.
Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30.
Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–3.
Knobel H, Guelar A, Valldecillo G, et al. Response to highly active antiretroviral therapy in HIV-infected patients aged 60 years or older after 24 months follow-up. AIDS. 2001;15(12):1591–3.
Chesney MA. Factors affecting adherence to antiretroviral therapy. Clin Infect Dis. 2000;30(Suppl 2):S171–6.
Ferguson TF, Stewart KE, Funkhouser E, Tolson J, Westfall AO, Saag MS. Patient-perceived barriers to antiretroviral adherence: associations with race. AIDS Care. 2002;14(5):607–17.
Murphy DA, Marelich WD, Hoffman D, Steers WN. Predictors of antiretroviral adherence. AIDS Care. 2004;16(4):471–84.
Penedo FJ, Gonzalez JS, Dahn JR, et al. Personality, quality of life and HAART adherence among men and women living with HIV/AIDS. J Psychosom Res. 2003;54(3):271–8.
Roca B, Lapuebla C, Vidal-Tegedor B. HAART with didanosine once versus twice daily: adherence and efficacy. Int J Infect Dis. 2005;9(4):195–200.
Laniece I, Ciss M, Desclaux A, et al. Adherence to HAART and its principal determinants in a cohort of Senegalese adults. AIDS. 2003;17(Suppl 3):S103–8.
Kleeberger CA, Phair JP, Strathdee SA, Detels R, Kingsley L, Jacobson LP. Determinants of heterogeneous adherence to HIV-antiretroviral therapies in the Multicenter AIDS Cohort Study. J Acquir Immune Defic Syndr. 2001;26(1):82–92.
Mohammed H, Kieltyka L, Richardson-Alston G, et al. Adherence to HAART among HIV-infected persons in rural Louisiana. AIDS Patient Care STDS. 2004;18(5):289–96.
Ammassari A, Trotta MP, Murri R, et al. Correlates and predictors of adherence to highly active antiretroviral therapy: overview of published literature. J Acquir Immune Defic Syndr. 2002;31(Suppl 3):S123–7.
Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K. Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health. 2008;8:265.
Bangsberg D, Emenyonu N, Andia I, et al. No decline in high levels of electronic pill cap, unannounced home pill count, and patient-reported adherence to free ARV therapy over 12 months in rural Uganda. In: 15th conference on retroviruses and opportunistic infections. Boston, Massachusetts, 3–6 Feb 2008 [abstract no. 801]. http://www.retroconference.org/2008/index.asp. Accessed 4 Feb 2010.
Byakika-Tusiime J, Oyugi JH, Tumwikirize WA, Katabira ET, Mugyenyi PN, Bangsberg DR. Adherence to HIV antiretroviral therapy in HIV+ Ugandan patients purchasing therapy. Int J STD AIDS. 2005;16(1):38–41.
Muyingo SK, Walker AS, Reid A, et al. Patterns of individual and population-level adherence to antiretroviral therapy and risk factors for poor adherence in the first year of the DART trial in Uganda and Zimbabwe. J Acquir Immune Defic Syndr. 2008;48(4):468–75.
Orrell C, Bangsberg DR, Badri M, Wood R. Adherence is not a barrier to successful antiretroviral therapy in South Africa. AIDS. 2003;17(9):1369–75.
Etard JF, Laniece I, Fall MB, et al. A 84-month follow up of adherence to HAART in a cohort of adult Senegalese patients. Trop Med Int Health. 2007;12(10):1191–8.
Laurent C, Diakhate N, Gueye NF, et al. The Senegalese government’s highly active antiretroviral therapy initiative: an 18-month follow-up study. AIDS. 2002;16(10):1363–70.
Iliyasu Z, Kabir M, Abubakar IS, Babashani M, Zubair ZA. Compliance to antiretroviral therapy among AIDS patients in Aminu Kano Teaching Hospital, Kano, Nigeria. Niger J Med. 2005;14(3):290–4.
Weiser S, Wolfe W, Bangsberg D, et al. Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. J Acquir Immune Defic Syndr. 2003;34(3):281–8.
Maqutu D, Zewotir T, North D, Naidoo K, Grobler A. Factors affecting early adherence to antiretroviral therapy amongst the HIV positive adults in South Africa. In: 50th annual conference of the South African statistical association, 29 Oct–2 Nov 2007. Johannesburg, South Africa.
South African National Department of Health. National antiretroviral treatment guidelines. 1st ed. (2004). http://www.hst.org.za/uploads/files/sa_ART_gudelines1.pdf/. Accessed 7 May 2009.
Littell RC, Milliken GA, Stroup WW, Wolfinger DR, Schabenberger O. SAS system for mixed models. 2nd ed. Cary, NC: SAS Institute Inc; 1999.
Milliken GA, Johnson E. Analysis of messy data. New York: Chapman & Hall/CRC; 2002.
Agresti A. Categorical data analysis. 2nd ed. New York: Wiley; 2002.
Liang K-Y, Zeger S. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13–22.
Pan W. Akaike’s information criterion in generalized estimating equations. Biometrics. 2001;57:120–5.
Hedeker D, Gibbons R. Longitudinal data analysis. New York: Wiley; 2006.
Rubin DB. Inference and missing data. Biometrika. 1976;63:581–92.
Little RJA, Rubin DB. Statistical analysis with missing data. 2nd ed. New York: Wiley; 2002.
Fong OW, Ho CF, Fung LY, et al. Determinants of adherence to highly active antiretroviral therapy (HAART) in Chinese HIV/AIDS patients. HIV Med. 2003;4(2):133–8.
Haubrich RH, Little SJ, Currier JS, et al. The value of patient-reported adherence to antiretroviral therapy in predicting virologic and immunologic response California Collaborative Treatment Group. AIDS. 1999;13(9):1099–107.
Berg KM, Demas PA, Howard AA, Schoenbaum EE, Gourevitch MN, Arnsten JH. Gender differences in factors associated with adherence to antiretroviral therapy. J Gen Intern Med. 2004;19(11):1111–7.
Skhosana N, Struthers H, Gray G, McIntyre J. HIV disclosure and other factors that impact on adherence to antiretroviral therapy: the case of Soweto, South Africa. AJAR. 2006;5(1):17–26.
Harvey KM, Carrington D, Duncan J, et al. Evaluation of adherence to highly active antiretroviral therapy in adults in Jamaica. West Indian Med J. 2008;57(3):293–7.
Birbeck GL, Chomba E, Kvalsund M, et al. Antiretroviral adherence in rural Zambia: the first year of treatment availability. Am J Trop Med Hyg. 2009;80(4):669–74.
Williams A, Friedland G. Adherence, compliance, and HAART. AIDS Clin Care. 1997;9(7):51–4, 8.
Godin G, Cote J, Naccache H, Lambert LD, Trottier S. Prediction of adherence to antiretroviral therapy: a one-year longitudinal study. AIDS Care. 2005;17(4):493–504.
Bartlett JA. Addressing the challenges of adherence. J Acquir Immune Defic Syndr. 2002;29(Suppl 1):S2–10.
Ickovics JR, Meade CS. Adherence to HAART among patients with HIV: breakthroughs and barriers. AIDS Care. 2002;14(3):309–18.
Abel E, Painter L. Factors that influence adherence to HIV medications: perceptions of women and health care providers. J Assoc Nurses AIDS Care. 2003;14(4):61–9.
Nachega JB, Hislop M, Dowdy DW, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann Intern Med. 2007;146(8):564–73.
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–97.
Chang LW, Kagaayi J, Nakigozi G, et al. Telecommunications and health Care: an HIV/AIDS warmline for communication and consultation in Rakai, Uganda. J Int Assoc Physicians AIDS Care (Chic Ill). 2008;7(3):130–2.
Bangsberg DR, Hecht FM, Charlebois ED, et al. Adherence to protease inhibitors, HIV-1 viral load, and development of drug resistance in an indigent population. AIDS. 2000;14(4):357–66.
Acknowledgments
CAPRISA was established in 2002 through a Comprehensive International Program of Research on AIDS (CIPRA) grant (AI51794) from the US National Institutes of Health (NIH), as a multi-institutional collaboration, incorporated as an independent non-profit AIDS Research Organization. The NIH funded the development of the research infrastructure, including the data management, laboratory and pharmacy cores established through the CIPRA grant. The US President’s Emergency Plan for AIDS Relief (PEPfAR) grant (1U2GPS001350) funded the care of all the patients in the CAT Programme. Dikokole Maqutu was supported by and Anneke Grobler received career development support from the Columbia University-Southern African Fogarty AIDS International Training and Research Programme (AITRP) funded by the Fogarty International Center, National Institutes of Health (Grant # D43TW00231). We gratefully acknowledge the patients in the CAT Programme. We also thank all the staff who worked on the CAT Programme, treating patients and helped in the data collection. Special thanks to the pharmacists for collection of pill count data.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maqutu, D., Zewotir, T., North, D. et al. Determinants of Optimal Adherence Over Time to Antiretroviral Therapy Amongst HIV Positive Adults in South Africa: A Longitudinal Study. AIDS Behav 15, 1465–1474 (2011). https://doi.org/10.1007/s10461-010-9688-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-010-9688-x