
Abstract
Youth continue to show high HIV infection rates, and adolescents with mental health problems are especially at risk. We used longitudinal data to test a cognitive-behavioral model of risky sexual behavior among 175, ethnically diverse urban adolescents seeking mental health services. Path analyses of the cross-sectional data revealed that Motivation was a strong predictor of Behavioral Skills and Sexual Risk Taking. The model explained 42% of the variance in Sexual Risk Taking with age included—29% without age. In the longitudinal path analyses, Motivation had a significant negative effect on levels of Sexual Risk Taking 6 months later, controlling for Information, Behavioral Skills, age, and baseline levels of Sexual Risk Taking. These longitudinal effects explained 60% of the variance in Sexual Risk Taking. These results underscore the need to address motivational factors in HIV prevention programs designed for adolescents with mental health problems.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rates of HIV remain consistently high among youths (up to age 24) in the U.S. From 2000 to 2003, 12% of new cases of HIV/AIDS were diagnosed among young people (CDC, 2003), but many more were unknowingly infected. Some estimates suggest 50% of new HIV infections occur in youth (Fisher, Fisher, Bryan, and Misovich, 2002). The majority of infections among teenagers are acquired through sexual transmission (CDC, 2003). However, risk is not uniform across youth—race, income, and mental health factors are related to infection rates. Youths seeking psychiatric care are at especially high risk because they are more likely than other teens to be sexually active, more likely to have multiple partners, and less likely to use condoms (Brown, Danovsky, Lourie, DiClemente, and Ponton, 1997; Donenberg, Emerson, Bryant, Wilson, and Weber-Shifrin, 2001). Mental health problems exacerbate risk of exposure because of HIV-specific factors, such as lack of perceived vulnerability to HIV (Katz, Mills, Singh, and Best, 1995), negative attitudes towards prevention (Brown et al., 1997), and low self-efficacy for preventive acts (Brown, Reynolds, and Lourie, 1997). More general processes related to psychopathology may also be relevant to HIV risk taking behaviors, such as low self-esteem and pessimistic outlooks (Carey, Carey, and Kalichman, 1997), difficulty being assertive and communicating effectively (Brown et al., 1997), and negative peer influence (McFarlane, Bellissimo, and Norman, 1995).
In the absence of a vaccine, effective prevention programs are critical to curb HIV transmission. Preventive interventions have the greatest chance at success when they are tailored to the unique risk factors of the target population. Therefore, the goal of the current study is to explore the applicability of a widely-used cognitive-behavioral HIV prevention model in a sample of ethnically diverse urban youth receiving psychiatric care.
The current study extends previous research testing the utility of cognitive behavioral variables in explaining risk behavior among teens seeking mental health services (Donenberg et al., 2005). This paper examines the longitudinal value of the widely used IMB model (e.g., Carey et al., 1997; Fisher and Fisher, 1992; Fisher and Fisher, 2002; Fisher et al., 2002; Fisher, Fisher, Misovich, Kimble, and Malloy, 1996) to predict sexual risk taking in this vulnerable subgroup. According to the IMB model, two cognitive processes, Information and Motivation, and one behavioral factor, Behavioral Skills, determine HIV prevention acts. Information about transmission and prevention is considered necessary, but insufficient for enacting safe behavior (Fisher and Fisher, 1992). Motivation to initiate and maintain safe sex is considered a multidimensional construct consisting of attitudes and intentions regarding preventive behaviors (e.g., Jemmott and Jemmott, 1990) and social norms about prevention acts (e.g., DiClemente, 1990). Motivation is viewed as important in determining whether individuals with appropriate knowledge and skills will behave safely, but it is unrelated to Information (i.e., you can have knowledge but no Motivation and vice-versa). According to the model, Information and Motivation directly affect sexual risk behaviors, but their influence is largely mediated by Behavioral Skills (Fisher and Fisher, 1992). Behavioral Skills is defined as perceived self-efficacy and the actual ability to perform preventive acts like assertive communication and accurate condom use (Fisher and Fisher, 1992).
The effects of Information, Motivation, and Behavioral Skills vary as a function of the study population (e.g., age, mental health, sexual orientation, and ethnicity) and the specific HIV preventive behavior. Research has investigated components of the IMB model in adolescents or applied the model to interventions, yet far fewer studies have tested the structural components of the IMB factors in relation to sexual risk taking, especially among troubled teens. Fisher, Williams, Fisher, and Malloy (1999) examined the cross-sectional effects of the IMB factors on engagement in safer-sex behaviors among sexually active urban adolescents. Sex differences were found both in the variance explained (boys=75% girls=46%) and in the structure of the model: Information was linked to Behavioral Skills in girls but not boys, and Motivation was linked to engagement in safer-sex behaviors in boys but not girls. Interestingly, Information was not related to safer-sex behaviors in either sex, and Behavioral Skills, measured as self-efficacy, had a positive effect on engagement in safer-sex behaviors. In another study of heterosexual university students a slightly different pattern of results emerged with less variance explained (10%) and structural differences in the model; Information was related to Behavioral Skills, and Motivation did not have an effect on AIDS preventive behaviors (Fisher, Fisher, Williams, and Malloy, 1994). Lastly, in a study of teens seeking outpatient mental health services, Donenberg and colleagues (2005) reported different patterns linking the IMB factors to sexual risk taking depending on how age was tested. When age was included in the model, Information had a significant positive effect on Behavioral Skills and sexual risk taking, Motivation was positively associated with Behavioral Skills and negatively associated with sexual risk taking, and Behavioral Skills had a small negative association with sexual risk taking—in all the model explained 35% of the variance in sexual risk taking. The paths were equivalent for boys and girls. Other studies have not tested the IMB structural model in adolescents, but they have used multivariate regression analyses that included the IMB components. These studies have yielded different degrees of variance explained by the IMB factors (22% in a sample recruited from a teen clinic, Boyer et al., 2000; 3% in Zambian adolescents, Slonim-Nevo and Mukuka, 2005).
The current study builds on previous research by testing the structural components of the IMB model using longitudinal analyses, and by focusing on teens seeking mental health care. Although half of the teens whose data are included in this study also provided data for the cross sectional analyses reported by Donenberg et al. (2005), this is the first report of longitudinal effects from all teens. These longitudinal data, collected 6 months from the first assessment, allow us to prospectively test the effects of the IMB factors on sexual risk taking, controlling for baseline levels of sexual risk taking. Our report also differ from Donenberg et al. (2005) in three important ways. First, we include several additional measures of Motivation to capture the intended components of the construct more fully. Second, we use path analysis instead of structural equation modeling because of the higher number of parameters, and therefore larger sample size, required to fit a model with latent variables. Third, we use an outcome variable that combines condom use and number of sexual partners, the most direct indicators of sexual risk taking, instead of a global composite score that also includes other behaviors such as drug use. The ultimate goal of these analyses is to understand the role of cognitive and behavioral factors in sexual risk taking among teens with mental health problems over time, yielding important insight for the development of interventions tailored to this at-risk population.
Methods
Procedure
This paper includes the first and second waves of data collection from a longitudinal study of HIV-risk behavior among youths in psychiatric care (the CARES project). Details regarding baseline recruitment methods and consent rates are provided elsewhere (Donenberg et al., 2005). Briefly, adolescents and their primary caregivers were recruited from four outpatient psychiatric clinics in Chicago. At baseline and 6-month follow up, parents and youths separately completed self-report measures and interviews, which lasted approximately three to four hours. Youths were excluded from the study if they: (1) were identified as having a pervasive developmental disorder or had a cognitive impairment that would limit their ability to understand the questions or the assent process (N=58); (2) were wards of the Department of Child and Family Services, whose institutional review board denied approval for the study (N=46); (3) did not speak English, because measures and consent/assent forms were normed for English speakers (N=37); (4) did not live with a guardian or caretaker (N=3). Participants were compensated for their participation.
Participants
Participants (N=175) are a subset of the larger sample for whom complete data were available at baseline and 6-month follow-up. Subject retention at the 6-month follow-up assessment was 78% (N=257). Participants did not complete the follow-up assessment for the following reasons: refused (29% of nonresponders, N=16), did not consent to be followed (29% N=16), agreed to participate but then would not come to the assessment despite repeated attempts (24%, N=14), unable to locate or did not return calls (10%, N=6), deceased (3%, N=2), or other reasons (5%, N=3). There were no differences in age, F(1, 272)=1.05, p > .05; gender, F(1, 272)=1.84, p > .05; or ethnicity, Mann–Whitney U(N=273)=7610.50, p > .05 between participants with complete data and those who were lost at the 6-month follow-up or who provided incomplete follow-up data. Moreover, participants with complete data at the 6-month follow-up did not differ from nonresponders or incomplete-responders in Information, F(1, 271)=.07, p > .05; Motivation F(1, 256)=.93, p > .05; Behavioral Skills, F(1, 265)=.01, p > .05; or Sexual Risk Taking, F(1, 259)=.95, p > .05 as measured at baseline.
At baseline, youths ranged in age from 12 to 19 (M=14.76; SD=1.81) and 42% (N=74) were female. Teens were ethnically diverse (African American 60%, N=105; Caucasian 20%, N=35; Latino 13%, N=23; Biracial 5%, N=9) and 57% (N=100) of the families scored in the first three levels of the Hollingshead (1975) index, indicating low to middle incomes. Participants qualified for a range of psychiatric disorders based on the Computerized Diagnostic Interview Schedule for Children (CDISC; Shaffer, Fisher, Piacentini, Schwab-Stone, and Wiks, 1991). According to youth’s report, 11% (N=19) met criteria for a mood disorder, 20% (N=35) met criteria for an anxiety disorder, 15% (N=26) met criteria for conduct disorder, and 32% (N=56) met criteria for at least one disorder. According to guardian’s report, 18% (N=32) of the teens met criteria for a mood disorder, 20% (N=35) met criteria for an anxiety disorder, 43% (N=75) met criteria for a disruptive behavior disorder, and 60% (N=104) met criteria for at least one disorder. The relatively low association between rates of parent and child reported child psychopathology are consistent with previous findings (Achenbach, McConaughy, and Howell, 1987).
Measures
Demographics and psychopathology
At baseline, parents reported adolescent’s age, gender, ethnicity, and the family’s socioeconomic status (Hollingshead, 1975). Both parents and teens completed the CDISC (Shaffer et al., 1991) at the baseline assessment.
Information
AIDS knowledge was measured with a true–false self-report instrument adapted from previously published measures of modes of transmission, misconceptions about transmission, and risk-reduction strategies (Brown, DiClemente, and Beausoleil, 1992) and modified to be linguistically and developmentally appropriate for adolescents. Three scales were computed: (1) knowledge about transmission consisted of 20 items (e.g., “A person can get AIDS by touching or hugging someone with AIDS”); (2) knowledge about prevention consisted of ten items (e.g., “Condoms reduce the risk of getting the AIDS virus”); and (3) general AIDS knowledge consisted of five items (e.g., “Most people who have the AIDS virus quickly show signs of being sick”). For all scales, items were scored as “0” (incorrect) or “1” (correct) and summed together. A factor score was created to combine individual scales.
Motivation
AIDS attitudes and behavioral intentions were assessed using a self-report measure based on IMB model constructs (Fisher and Fisher, 1992) and social cognitive theory (Bandura, 1994). Items were developed for use with pre-adolescents and adolescents. We computed four scales: (1) Social norms concerning preventive acts consisted of eight items (e.g., “Friends that I respect think I should use condoms every time, if I have sex, during the next 2 months”). The items had five response options ranging from “very true” to “very untrue.” (2) Attitudes towards HIV prevention acts consisted of three items (e.g., “If I have sex during the next 2 months, using condoms every time would be:”) with response options ranging from “very bad” to “very good.” (3) Behavioral intentions to prevent AIDS infection consisted of three items (e.g., “If I have sex during the next 2 months, I’m planning to use condoms every time”) with five response options ranging from “very true” to “very untrue.” (4) Beliefs about condom use consisted of five items (e.g., “Condoms take all the fun out of sex”), with response options ranging from “strongly disagree” to “strongly agree.” For all scales, items were summed to compute a composite score. A factor score was created to combine individual scales.
Behavioral skills
AIDS Behavioral Skills (Donenberg et al., 2005; Misovich, 1998 (personal communication)) measured perceptions of self-efficacy to prevent HIV transmission and negotiate AIDS prevention with a partner. Questions were modified to use with adolescents. Two scales were computed: (1) Behavioral skills regarding self consisted of three items (e.g., “How hard or easy would it be for you to get condoms [buy them or get them free] at a place close to your home or school?”). (2) Behavioral skills regarding partner consisted of four items (e.g., “How hard or easy would it be for you to tell the person you like as more than a friend that you are not going to have sex with him/her?”). Both scales had five response options ranging from “Very hard to do” to “Very easy to do” with low scores indicating less self-efficacy to practice prevention. The scales were summed together to compute a composite score.
Sexual risk-taking
At baseline and 6 month follow-up the AIDS Risk Behavior Assessment (ARBA; Donenberg et al., 2001; Donenberg et al., 2005) was administered. The ARBA is a self-administered computerized interview designed specifically for use with adolescents to assess their HIV/AIDS risk behaviors. Youth self-administer the ARBA using a voice directed computer with an interviewer available to answer questions and ensure item comprehension. Two items were combined to develop a composite measure of sexual risk taking: number of sexual partners in the past 3 months and consistency of condom use during the last 3 months. Teens who were sexually abstinent in the past 3 months were assigned a zero; teens who always used condoms were assigned a one; teen who had one partner and used condoms inconsistently were assigned a two; teens with multiple partners and inconsistent condom use were assigned a three; teens with multiple partners who never used condoms were assigned a four. This approach to computing sexual risk behavior has several advantages. First, it is consistent with previous measurement of adolescent sexual risk taking (e.g., Dutra, Miller, and Forehand, 1999; Fisher et al., 1999; Kotchick, Dorsey, Miller, and Forehand, 1999), allowing for comparison of findings across studies. Second, it allowed us to include all participants—whether sexually active or not—in all analyses, thereby increasing power and eliminating bias against nonsexually active youth. The inclusion of nonsexually active participants is consistent with previous research (Donenberg, Bryant, Emerson, Wilson, and Pasch, 2003; Donenberg et al., 2005), allowing further comparison of our findings to other reports. Finally, this method is consistent with research showing that factors that influence initiation versus abstinence are at least partially etiologically connected to those that influence variability in other sexual health behaviors, such as number of sexual partners (Mustanski, Viken, Kaprio, and Rose, 2005).
Statistical analyses
Factor analysis was performed on each of the scales making up the Information and Motivation constructs using Principal Components (PC) extraction to compute factor scores. When scored, all scales were positively correlated; therefore, an increase in the factor score can be directly interpreted as being related to increases in each scale. Path analysis was used because the sample size was not adequate to estimate the additional parameters involved in producing latent variables for structural equations modeling. The sample size (N=175) was adequate given the 20 parameters and the general rule of having at least five subjects per parameter (Kline, 2005). Model fit was assessed using a variety of fit indices recommended by Kline (2005), including: the Root Mean Square Error of Approximation (RMSEA; Browne and Cudeck, 1993), which should be less than 0.05 for close fit, less than 0.08 for reasonable fit, and have the lower bound of the 90% confidence interval less than 0.05; The Standardized Root Mean Square Residual (SRMR), which should be less than 0.10 for favorable fit (Kline, 2005); The Comparative Fit Index, which should be greater than .90 (Hu and Bentler, 1999).
Results
Descriptive analyses
Table 1 presents the means, standard deviations, and correlations among the variables. As described above, the second wave of data collection took place approximately 6 months after baseline, which is reflected by the increase in mean age by almost exactly 6 months and the correlations between age at baseline and follow-up estimated close to unity. Note that the Information and Motivation variables were computed using regression output from a PC factor analysis, which resulted in variables that were standardized; this explains the estimated means and standard deviations close to zero and one, respectively.
Consistent with earlier studies based on a subgroup of the current sample (e.g., Donenberg et al., 2005), teens reported high rates of sexual risk taking. At baseline, 27% (N=48) of these young teens reported a sexual partner in the last 3 months. Only 15% (N=26) always used a condom with at least one partner, 7% (N=12) reported one partner with inconsistent condom use, and 6% (N=10) of teens had multiple partners with inconsistent condom use. At the 6-month follow-up assessment the rates changed slightly, with 29% (N=51) of teens reporting a sexual partner in the last 3 months, 18% (N=32) always used a condom with at least one partner, 3% (N=5) reported one partner with inconsistent condom use, 7% (N=12) of teens had multiple partners with inconsistent condom use, and 1% (N=2) of teens reported multiple partners without ever using a condom in the last 3-months. These changes are reflected in higher mean sexual risk-taking scores at the 6-month follow-up relative to the baseline assessment.
Factor analyses
For constructs with at least three scales serving as indicators (i.e., Information and Motivation), factor analysis was used to compute factors that were then used in the path analysis. For the Information construct factor analysis produced one factor with an eigenvalue over one, which explained 68% of variance. For the Motivation factor, factor analysis produced one factor with an eigenvalue over one, which explained 61% of the variance.
Testing the model
Mardia statistics revealed significant departures from univariate normality for each of the variables included in the model. Accordingly, Maximum Likelihood (ML) estimation was used to compute the Satorra-Bentler chi-square, which is the most preferred method for adjusting goodness-of-fit statistics for bias due to nonnormality (Kline, 2005).
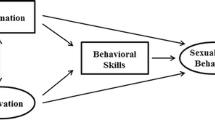
Figure 1 illustrates the model which yielded a reasonable fit to the data based on the selected fit indices (chi square=1.97, df=1, p=0.16; RMSEA=0.075 with 95% CI:0.00–0.23; SRMR=0.02; CFI=0.99). The figure contains the standardized parameter estimates from the model. For the sake of visual clarity, the correlations between Information and Age (r=0.49, p < 0.01), Motivation and Age (r=−0.24, p < 0.05), and the error variances (derivable below) were excluded from the figure.

Path model of IMB factors predicting sexual risk taking at baseline and 6-month follow-up. Parameters are standardized estimates. * p > .05.
In the cross-sectional portion of the path model, Information and Motivation did not covary. Contrary to expectations, Information did not have a significant effect on either Behavioral Skills or baseline Sexual Risk Taking. Motivation had a moderate positive effect on Behavioral Skills and a moderate negative effect on baseline Sexual Risk Taking. Behavioral Skills had a small, but significant, positive effect on baseline Sexual Risk Taking, indicating that teens who reported that it would be very easy to engage in preventive behaviors were less likely to engage in those protective behaviors. Consistent with previous research, age had a moderate effect on baseline Sexual Risk Taking, and with age included in the model we were able to explain 42% of the variance—excluding age dropped the variance explained to 29%.
Many of the findings from the cross-sectional analyses were replicated in the longitudinal portion of the path model. Again, Information did not have a significant effect on Sexual Risk Taking. Motivation had a significant negative relationship with Sexual Risk Taking assessed 6 months later, even when including Information, Behavioral Skills, age, and baseline Sexual Risk Taking as predictors. However, Behavioral Skill had a nonsignificant relationship with Sexual Risk Taking at the 6-month follow-up, controlling for other factors in the model. Finally, there was considerable stability in Sexual Risk Taking over time. In the prospective analyses, 60% of the variance in Sexual Risk Taking was explained by Information, Motivation, Behavior Skills, age, and baseline level of Sexual Risk Taking.
Supplemental analyses
Given the important role that Motivation played in predicting Sexual Risk Taking in both the cross-sectional and longitudinal analyses, and because Motivation is a multidimensional construct, supplemental regression analyses were performed to assess the individual components of Motivation in relation to sexual risk behavior at the 6-month follow-up. Table 2 shows the results of the multiple regression analysis with Peer Norms for HIV prevention, Personal Attitudes Towards HIV Prevention, Intentions to Engage in HIV Preventive Behaviors, and Attitudes Towards Condoms predicting 6-month Sexual Risk Taking. These analyses clearly indicate that Intentions to Engage in HIV Preventive Behaviors (e.g., plan to use condoms with sexual partners) underlie the relationship between Motivation and Sexual Risk Taking. Intentions is the only Motivation component that showed a significant relationship with sexual behavior, and the relationship is large and negative, indicating that teens who reported higher levels of Intentions to engage in HIV preventive behaviors were less likely to engage in risky sexual behavior 6 months later.
In the path analysis, Behavioral Skills showed a significant positive association with baseline Sexual Risk Taking. This small, but significant, positive association was in the opposite direction posited by the authors of the IMB theory (Fisher and Fisher, 1992); it was also in the opposite direction found by Donenberg et al. (2005) in a subsample of the subjects reported here, but with a different measure of sexual risk taking. To determine the source of this positive association we conducted several supplemental analyses. First, to establish if this positive association was explained by the inclusion of nonsexually active teens, we entered the IMB factors and age as independent variables and baseline Sexual Risk Taking as the dependent variable, but we only included teens who had initiated sexual behavior (N=50). As shown in Table 2, among sexually active youth, a slightly different pattern of findings emerged, relative to those produced in the path analysis of the full sample. Age was no longer significant, Information had a positive and significant relationship to risky sex, Motivation continued to significantly negatively predict baseline Sexual Risk Taking, and the small positive association with Behavioral Skills became nonsignificant. Second, we explored the relationship between the IMB factors and other sexual risk outcome variables using multiple regression to determine if the positive association was due to our choice of outcome measure. The same pattern of findings emerged when the dependent variable was consistency of condom use in the last 3 months, number of occasions of vaginal sex in the last 3 months, and number of partners in the last 3 months. Finally, we investigated if the positive association was due to one of the subcomponents of our measure of Behavioral Skill; self-efficacy for self to engage in preventive acts or self-efficacy to engage in preventive behaviors with a partner. To do this, we conducted multiple regression analyses with behavior skills regarding self and partner entered separately along with age, Information, and Motivation as predictors of Sexual Risk Taking. The results suggest that behavioral skills related to self underlie the association between Behavioral Skills and sexual risk taking (standardized beta=0.16, p < 0.05), whereas Behavioral Skills related to a partner showed a nonsignificant relationship.
Discussion
This is one of the very few studies to test the cognitive and behavioral factors of the IMB model using longitudinal data, and only the second to explore these constructs among youths seeking mental health services. The model provided an adequate fit to the data. Results support some, but not all, of the links proposed by the IMB model (Fisher and Fisher, 1992) or those found in a previous cross-sectional report of youths seeking psychiatric care (Donenberg et al., 2005). The IMB model was moderately useful as applied to this population, and the constructs explained 29% of the variance in baseline sexual risk taking (42% including age as a predictor).
Contrary to the originally proposed linkages of the IMB model, Information did not predict Behavioral Skills or Sexual Risk Taking. This is consistent with findings of urban adolescent males (Fisher et al., 1999), but not urban adolescent females (Fisher et al., 1999) or adolescents with mental health problems; the latter showed a positive association with Behavioral Skills and sexual risk behavior (Donenberg et al., 2005). The relationship between Information and other model constructs appears to be unstable across populations (Fisher and Fisher, 2002), reflecting potential differences in levels of HIV knowledge or the application of that knowledge. In this study, the lack of association was unlikely due to saturation of knowledge, since the mode percent correct on the HIV knowledge scale was 63% (mean=62%). Rather, for youths with psychiatric problems, relevant aspects of their psychopathology may make it difficult for them to apply their knowledge about HIV prevention. For example, these teens tend to be impulsive and deficient in problem solving and social negotiation skills making it difficult to use their knowledge of HIV transmission and prevention to enact safe behavior (Donenberg and Pao, 2005).
Motivation played the central role in predicting Behavioral Skills and Sexual Risk Taking in this study. In the cross-sectional analyses, Motivation had a moderate positive association with Behavioral Skills and a moderate negative association with Sexual Risk Taking, suggesting that higher motivation to prevent HIV transmission was linked to greater perceived behavioral skills and less risky sex. These effects were replicated in the longitudinal analyses, where Motivation was significantly related to Sexual Risk Taking at the 6-month follow-up assessment, controlling for Information, Behavioral Skills, age, and baseline levels of Sexual Risk Taking. The prospective nature of these analyses allow for greater inference about the potential causal nature of Motivation in sexual risk taking within this sample of urban adolescents seeking psychiatric care.
Like other research, Motivation was defined as a multidimensional construct in this study. Supplemental longitudinal analyses of the individual components revealed that Intentions to prevent HIV infection were the primary source predicting sexual risk taking. In these analyses, Behavioral Intention were reported 6 months earlier than Sexual Risk Taking, allowing us to partially disentangle potential confounding effects of reporting biases that may be related to both reports of Behavioral Intentions and past sexual behavior. The importance of Behavioral Intentions is consistent with Sikkema et al. (2004) who found that behavioral intentions, and not peer norms or expectancies, was the only variable to predict sexual risk taking among adolescents in public housing. These findings suggest that for teens seeking psychiatric care, intentions to practice safer sex is an important target for interventions. Encouraging these youth to plan ahead and be prepared to engage in preventive acts could reduce high risk behavior.
In the cross sectional analyses, Behavioral Skills had a small, but significant, positive association with Sexual Risk Taking, indicating that perceptions of self-efficacy to prevent HIV transmission were linked to more sexual risk taking. This finding is inconsistent with the IMB model (Fisher and Fisher, 1992) and with results reported by Donenberg et al. (2005) on a subsample of the subjects included here. Why the difference in these two studies of youth seeking mental health services? There are at least two possible reasons. First, Donenberg et al. (2005) used structural equations modeling rather than path analysis, and second, they defined sexual risk taking as a global composite comprised of number of sexual partners, use of alcohol/drugs during sex, having sex with a partner whose history was not well known, and sex without a condom. By contrast, we defined sexual risk taking as the number of partners and consistency of condom use during the last 90 days. Therefore, differences in both the analytic strategy and measure of sexual risk taking may account for the different patterns.
Several other reasons may explain the positive association between Behavioral Skills and baseline sexual risk. First, the explanation could be due to a number of methodological factors. We included sexual abstainers in the analyses and previous reports indicate that sexually active youths score higher on measures of self-efficacy (Faryna and Morales, 2000), the same type of behavioral skills measure used in this study. Sexually abstinent teens may be less likely to report efficacy to engage in preventive behaviors, because they do not plan to have sex at all. To test this hypothesis, we ran analyses of IMB variables and age predicting baseline Sexual Risk Taking only among sexually active adolescents (see Table 2). Indeed, the positive effect of Behavioral Skills was attenuated (0.07) relative to the path analysis with the full sample (0.13), suggesting that the inclusion of abstainers may explain part of the positive association. It also may reflect our method of measuring sexual risk as a composite of number of partners and consistency of condom use. We explored this by testing the relationship between the IMB factors and other commonly used sexual risk outcome variables; in all cases a similar patterns of results emerged. Another methodological explanation may be our measurement of Behavioral Skills, which included measurement of self-efficacy for self- and partner-related prevention behaviors. We explored if only one of the components of Behavioral Skills (regarding self or partners) caused the positive relationship with baseline Sexual Risk Taking. These analyses suggested that Behavioral Skills regarding self, not behavioral skills related to partner, was the root of the positive relationship with Sexual Risk Taking.
In addition to the potential methodological explanations for the positive association between Behavioral Skills and Sexual Risk Taking, it is also possible that the explanation is substantive and due to perceptions of self-efficacy being poor predictors of actual behavioral skills (Forsyth, Carey, and Fuqua, 1997), especially for teens with mental health problems. These youth often display poor affect regulation and significant cognitive deficits, including poor reality testing, perceived invulnerability, and inadequate problem solving. The positive association between baseline Sexual Risk Taking and perceived Behavioral Skills may underscore the difficulty these teens have enacting safe behaviors in the context of affective arousal. This may be reflected in the results of the longitudinal analyses where the relationship between Behavioral Skills and Sexual Risk Taking was nonsignificant; suggesting that this variable may have more to do with plans for the future and less to do with actual future behavior. For example, a mentally ill teen told us during an HIV prevention program, “I totally know how to use a condom, but last week, when I was in the back of the car with my girlfriend, and I wanted to have sex right then, I didn’t even think about using a condom.” In fact, this same teen exhibited good condom negotiation skills in the group and accurate condom use during a role play. His inability to apply these skills in the heat of the moment underscores the problem with cognitive-behavioral models of risk taking for these teens.
Levels of Sexual Risk Taking were high in this sample of urban adolescents seeking psychiatric care. For example, at the 6-month follow-up 29% (N=51) of these young teens reported being sexually active in the last 3 months, 60% (N=35) of sexually active teens reported using a condom at last intercourse, and 26% (N=15) reporting having four or more sexual partners in the last 6 months. These rates are riskier than data from the CDC’s Youth Risk Behavior Survey data for ninth grade (CDC, 2004). Levels of sexual risk also showed considerable stability over 6-months. Similar levels of stability in sexual risk taking have been reported for gay men, but rates in this study are higher than those reported by heterosexual college students in the only other longitudinal test of the IMB model (Fisher et al., 1994). If these levels of stability are confirmed in other longitudinal studies, they may suggest the importance of individual differences in traits, such as personality, that tend to be stable and have been found to be related to sexual risk taking (Hoyle, Fejfar, and Miller, 2000). For adolescents with mental health problems, individual differences in factors related to psychopathology may be especially relevant to risky sexual behavior, for example, differences in impulsivity, negative emotionality, and reward responsiveness. Future research should focus on teasing apart these distinctions.
Results must be interpreted in the context of study limitations. First, these findings are based on youths seeking outpatient mental health services and the results may not generalize to other populations. Nevertheless, these teens are at elevated risk of HIV infection and understanding the role of cognitive behavioral factors on their risk behavior will lead to better informed and uniquely targeted prevention programs. Second, this study relied on adolescent self-reports of the IMB constructs and sexual behavior. We attempted to minimize bias by using computer assisted technology, which has been found to increase validity regarding sensitive behaviors (Romer, Hornik, and Stanton, 1997). Third, many of our variables were skewed. For example, few participants reported multiple partners and never using condoms. We attempted to correct for this by using the Satorra-Bentler adjustment, but the standard errors and fit statistics could still show some bias. Finally, this is the first longitudinal study to use path analyses to study the relationships among multiple IMB constructs over time. Replication is essential to fully understand the cognitive-behavioral factors that influence sexual risk taking among youths in psychiatric care, particularly across time. Of particular value would be efforts to understand the relationship between perceived self-efficacy and sexual risk behavior, as this link has been inconsistent across studies. Future research should investigate the mediating and moderating role of age, gender, and symptoms of psychopathology in relation to the IMB constructs. Testing these questions will require larger samples to allow sufficient power to conduct multigroup path analysis.
This longitudinal study found the IMB model to be moderately useful in explaining variance in sexual risk taking among adolescents seeking mental health services across two waves of data collection, 6-months apart. Motivation was the most important predictor of sexual risk taking at baseline, as well as in the longitudinal analyses. Information and Behavioral Skills showed little relationship to sexual risk behavior in this population. Indeed, teens know how to use condoms and believe they can use them, but they do not, especially when they are emotionally aroused. These results highlight the importance of addressing Motivation, and specifically behavioral intentions, in interventions to reduce HIV and STI infections among youths with mental health problems. In our current prevention efforts, we work with teens to develop safety plans by anticipating risky people, places, and situations and identifying strategies and intentions for staying safe. Moreover, although we only examined the role of cognitive and behavioral factors associated with risk behavior, there is ample evidence that contextual factors influence adolescent risk taking, especially among troubled youth (Donenberg and Pao, 2005). Donenberg and Pao (2005) articulate a social-personal model of adolescent risk behavior that underscores the role of family context, peer and partner relationships, personal attributes, and the broader environmental context. Thus, the most effective prevention programs will likely require a broad contextual framework and multiple targets, including motivation, affect regulation, and psychopathology.
References
Achenbach, T. M., McConaughy, S. H., and Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213–232.
Bandura, A. (1994). Social cognitive theory and exercise control of HIV infection. In R. J. DiClemente and J. L. Peterson (Eds.), Preventing AIDS: Theories and methods of behavioral interventions. New York: Plenum Press.
Boyer, C. B., Shafer, M., Wibbelsman, C. J., Seeberg, D., Teitle, E., and Lovell, N. (2000). Associations of sociodemographic, psychosocial, and behavioral factors with sexual risk and sexually transmitted diseases in teen clinic patients. Journal of Adolescent Health, 27, 102–111.
Brown, L. K., Danovsky, M. B., Lourie, K. J., DiClemente, R. J., and Ponton, L. E. (1997). Adolescents with psychiatric disorders and the risk of HIV. Journal of American Academy of Child and Adolescent Psychiatry, 36, 1609–1617.
Brown, L. K., DiClemente, R. J., and Beausoleil, N. I. (1992). Comparison of human immunodeficiency virus related knowledge, attitudes, intentions, and behaviors among sexually active and abstinent young adolescents. Journal of Adolescent Health, 13, 140–145.
Brown, L. K., Reynolds, L. A., and Lourie, K. J. (1997). A pilot HIV prevention program for adolescents in a psychiatric hospital. Psychiatric Services, 48, 531–533.
Browne, M. W., and Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen and J. S. Long (Eds.), Testing Structural Equation Models (pp. 136–162). Newbury Park: Sage Publications.
Carey, M. P., Carey, K. B., and Kalichman, S. C. (1997). Risk for HIV infection among persons with severe mental illnesses. Clinical Psychology Review, 17, 271–291.
Carey, M. P., Maisto, S. A., Kalichman, S. C., Forsyth, A. D., Johnson, B. T., and Wright, E. (1997). Enhancing motivation to reduce the risk of HIV infection for economically disadvantaged urban women. Journal of Consulting and Clinical Psychology, 65, 531–541.
CDC. (2003). HIV/AIDS surveillance report. From http://www.cdc.gov/hiv/stats/2003surveillancereport.pdf.
CDC. (2004). Youth risk behavior surveillance. Morbidity and mortality weekly, 53, 1–96.
DiClemente, R. J. (1990). The emergence of adolescents as a risk group for human immunodeficiency virus infection. Journal of Adolescent Research, 5, 7–17.
Donenberg, G. R., Bryant, F. B., Emerson, E., Wilson, H. W., and Pasch, K. E. (2003). Tracing the roots of early sexual debut among adolescents in psychiatric care. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 594–608.
Donenberg, G. R., Emerson, E., Bryant, F. B., Wilson, H., and Weber-Shifrin, E. (2001). Understanding AIDS-risk behavior among adolescents in psychiatric care: Links to psychopathology and peer relationships. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 642–653.
Donenberg, G. R., and Pao, M. (2005). Youths and HIV/AIDS: Psychiatry’s role in a changing epidemic. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 728–747.
Donenberg, G. R., Schwartz, R. M., Emerson, E., Wilson, H. W., Bryant, F. B., and Coleman, G. (2005). Applying a cognitive-behavioral model of HIV-risk to youths in psychiatric care. AIDS Education and Prevention, in press.
Dutra, R., Miller, K. S., and Forehand, R. (1999). The process and content of sexual communication with adolescents in two-parent families: Associations with sexual risk-taking behavior. AIDS and Behavior, 3, 59–66.
Faryna, E. L., and Morales, E. (2000). Self-efficacy and HIV-related risk behaviors among multiethnic adolescents. Cultural Diversity and Ethnic Minority Psychology, 6, 42–56.
Fisher, J. D., and Fisher, W. A. (1992). Changing AIDS-risk behavior. Psychological Bulletin, 111, 455–474.
Fisher, J. D., and Fisher, W. A. (2002). The information-motivation-behavioral skills model. In R. J. DiClemente, R. A. Crosby and M. C. Kegler (Eds.), Emerging theories in health promotion practice and research: Strategies for improving public health (pp. 40–70). San Francisco: Jossey-Bass.
Fisher, J. D., Fisher, W. A., Bryan, A. D., and Misovich, S. J. (2002). Information-motivation-behavioral skills model-based HIV risk behavior change intervention for inner-city high school youth. Health Psychology, 21, 177–186.
Fisher, J. D., Fisher, W. A., Misovich, S. J., Kimble, D. L., and Malloy, T. E. (1996). Changing AIDS risk behavior: Effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychology, 15, 114–123.
Fisher, J. D., Fisher, W. A., Williams, S. S., and Malloy, T. E. (1994). Empirical tests of an information-motivation-behavioral skills model of AIDS-preventive behavior with gay men and heterosexual university students. Health Psychology, 13, 238–250.
Fisher, W. A., Williams, S. S., Fisher, J. D., and Malloy, T. E. (1999). Understanding AIDS risk behavior among sexually active urban adolescents: An empirical test of the information-motivation-behavioral skills model. AIDS and Behavior, 3, 13–23.
Forsyth, A. D., Carey, M. P., and Fuqua, R. W. (1997). Evaluation of the validity of the condom use self-efficacy scale (CUSES) in young men using two behavioral simulations. Health Psychology, 16, 175–178.
Hollingshead, A. B. (1975). Four factor index of social status. Unpublished manuscript, Yale University.
Hoyle, R. H., Fejfar, M. C., and Miller, J. D. (2000). Personality and sexual risk taking: A quantitative review. Journal of Personality, 68, 1203–1231.
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55.
Jemmott, L., and Jemmott, F. E. (1990). Sexual knowledge, attitudes, and risky sexual behavior among inner-city Black male adolescents. Journal of Adolescent Research, 5, 346–369.
Katz, R. C., Mills, K., Singh, N. N., and Best, A. M. (1995). Knowledge and attitudes about AIDS: A comparison of public high school students, incarcerated delinquents, and emotionally disturbed adolescents. Journal of Youth and Adolescence, 24, 117–131.
Kline, R. B. (2005). Principles and practice of structural equation modeling (2 edn.). New York: Guilford Press.
Kotchick, B. A., Dorsey, S., Miller, K. S., and Forehand, R. (1999). Adolescent sexual risk-taking behavior in single-parent ethnic minority families. Journal of Family Psychology, 13, 92–102.
McFarlane, A. H., Bellissimo, A., and Norman, G. R. (1995). The role of family and peers in social self-efficacy: Links to depression in adolescence. American Journal of Orthopsychiatry, 65, 402–410.
Mustanski, B. S., Viken, R. J., Kaprio, J., and Rose, R. J. (2005). Sexual experience in young adulthood: A population-based twin study. Under review.
Romer, D., Hornik, R., and Stanton, B. (1997). “Talking” computers: An efficient and private method to conduct interviews on sensitive on sensitive health topics. Journal of Sex Research, 34, 3–9.
Shaffer, D., Fisher, P., Piacentini, J. C., Schwab-Stone, M. E., and Wiks, J. (1991). Diagnostic interview for children (DISC 2.3)– Child Version. New York: Columbia University.
Slonim-Nevo, V., and Mukuka, L. (2005). AIDS-related knowledge, attitudes and behavior among adolescents in Zambia. AIDS and Behavior, 9, 223–231.
Acknowledgments
This research was supported by R01 MH58545, the Warren Wright Adolescent Center at Northwestern Memorial Hospital, and Northwestern Memorial Hospital’s Intramural Grants Program. The authors gratefully acknowledge the Healthy Youths Program staff and the families who participated. We thank the administrators and staff at Northwestern Memorial Hospital, Children’s Memorial Hospital, Cook County Bureau of Health, and the Institute for Juvenile Research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mustanski, B., Donenberg, G. & Emerson, E. I Can Use a Condom, I Just Don’t: The Importance of Motivation to Prevent HIV in Adolescent Seeking Psychiatric Care. AIDS Behav 10, 753–762 (2006). https://doi.org/10.1007/s10461-006-9098-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-006-9098-2