
Abstract
Accelerometer-based assessments can identify elderly with an increased fall risk and monitor interventions. Smart devices, like the iPod Touch, with built-in accelerometers are promising for clinical gait and posture assessments due to easy use and cost-effectiveness. The aim of the present study was to establish the validity and reliability of the iPod Touch for gait and posture assessment. Sixty healthy participants (aged 18–75 years) were measured with an iPod Touch and stand-alone accelerometer while they walked under single- and dual-task conditions, and while standing in parallel and semi-tandem stance with eyes open, eyes closed and when performing a dual task. Cross-correlation values (CCV) showed high correspondence of anterior–posterior and medio-lateral signal patterns (CCV’s ≥ 0.88). Validity of gait parameters (foot contacts, index of harmonicity, and amplitude variability) and standing posture parameters [root mean square of accelerations, median power frequency (MPF) and sway area] as indicated by intra-class correlation (ICC) was high (ICC = 0.85–0.99) and test–retest reliability was good (ICC = 0.81–0.97), except for MPF (ICC = 0.59–0.87). Overall, the iPod Touch obtained valid and reliable measures of gait and postural control in healthy adults of all ages under different conditions. Additionally, smart devices have the potential to be used for clinical gait and posture assessments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The aging population is expanding and is associated with many health problems and the additional health care costs. Falls and fall-related injuries are one of the critical problems in old adults. One out of three community-dwelling old adults falls at least once a year.28 Unfortunately, those fall incidents have often serious consequences like bruises, fractures, decreased mobility, social isolation or even early death.8 To maintain the quality of life for old adults it is important to recognize an increased fall risk in time, and to offer fall prevention intervention(s) before a (first) fall takes place.9 One of the main reasons that old adults fall are mobility impairments. Accordingly, in the geriatric clinic, analysis of gait and postural control is becoming increasingly important for diagnostic purposes. Daily practice of an outpatient geriatric department is confronted with a high rate of frail elderly patients. These patients are characterized by a combination of physical, mental and social problems, use of polypharmacy and consequently high fall risk.2,3 An instrument that could quantitatively and objectively evaluate and assess deterioration in balance and gait, and monitor the impact of mobility improving interventions is thus of great importance.
A number of clinical instruments are available to quantify fall risk in old adults, such as questionnaires, fall diaries and physical performance tests.20,23 Due to their influence on fall risk, gait and posture assessments are often included in those clinical instruments. However, the currently accepted clinical tests provide only a global assessment of balance and gait ability, and suffer from limitations including ceiling effects and limited precision to detect small changes in balance and gait ability.1,14
Instrumented recordings can provide detailed information about changes in gait and postural control due to changes in task conditions, aging and/or pathology.3,7,10 A number of sophisticated ambulant systems are available for research purposes, such as pressure sensitive soles or mats, stand-alone 3D accelerometer and gyroscope sensors. By now an extensive number of studies have shown that parameters extracted from these signals, provide insight into motor control and are sensitive to detect postural differences between patient groups, age groups and task condition and can even predict falls.5,12,13,16,27 However, main drawbacks for the clinical use of these systems is that they are quite expensive and they require specialized research staff to collect and analyze the data.
The recent rapid development of off-the-shelf mobile devices and smart phones provide an interesting alternative for motion analysis in the clinic, as these smart devices are nowadays standard equipped with inertial sensors, such as tri-axial accelerometers. Consequently, it may be possible to use the acceleration signals collected by smart devices, to calculate gait and posture parameters. At this point, if the accuracy and reliability of these smart devices is comparable to the current used stand-alone accelerometer-based research methods, this could provide new prospects of using the accelerometer embedded in smart devices in clinical motion analysis. First, smart devices are getting cheaper and many people use them on daily basis, they are lightweight and easy to handle. Second, data can be transmitted wireless over long distances and from remote locations without retrieval of the device, which provides the opportunity to send data directly to an external personal computer which clinicians or researchers can assess. Thirdly, applications for motion recording and analysis can be programmed according to the needs of the end-user, researcher and/or clinician. Finally, data of gait and posture can be combined automatically with data from questionnaires, clinical tests and drug monitoring. Using a single device allows the clinician to assess deterioration in postural control and gait and to monitor the impact of mobility improving interventions.
The validity and reliability of available stand-alone accelerometer systems for motion analysis have been determined in numerous studies, measuring gait and posture parameters.4,19,29 Although motion analysis using smart devices is an emerging and promising area, only a few studies exist that assess gait and postural control. First results show good test–retest reliability between data collected by a smart phone (Xperia S0-01B, Sony Ericsson) and by a stand-alone accelerometer unit for walking of healthy adults, (intra-class correlation between 0.75 and 0.91),21 and also when comparing data collected during standing from an iPod Touch with that of a force plate(r ≥ 0.82).22
Validity and test–retest reliability might be different for different task conditions and/or for different individual groups. Therefore, the purpose of this study was to demonstrate proof of the concept that the accelerometer embedded in the iPod Touch can be used to accurately and reliably collect signals of anterior–posterior and medio-lateral trunk acceleration for calculation of gait and posture parameters in healthy young, middle aged and older adults during the performance of different walking and balance tasks. More specifically age effects as well as task effect were studied. Participants between 18 and 75 years were instructed to walk with and without performing a cognitive dual task, and we challenged their standing posture by asking them to stand parallel as well as in semi-tandem stance with eyes open, eyes closed and while concurrently performing a dual task.
Materials and Methods
Participants
The study population consisted of 22 young healthy adults (26 ± 3.9 years; 50% male), 15 middle aged healthy adults (45 ± 6.7 years; 67% male) and 23 older healthy adults (65 ± 5.5 years; 30% male) recruited from the community. Participants between 18 and 75 years old were included if they had no orthopedic or neurological problems and used no medication that might affect gait or postural control.
The Ethical Committee of the Center of Human Movement Sciences at the University Medical Center Groningen approved the research proposal and all participants signed written informed consent.
Instrumentation
To assess trunk accelerations during walking and standing the iPod Touch G4 (iOS 6; 123 × 59 × 6 mm, 88 gram, Apple Inc.), which has a built-in tri-axial acceleration sensor, was used. To collect and store the accelerometer data, a custom made application ‘iMoveDetection’ was installed on the iPod. The raw acceleration data was recorded at a sample frequency between 88 and 92 Hz. After each measurement, the raw data was saved on the device and send to a remote server through WIFI communication, further analysis occurred offline. To investigate the validity of the data collection with the iPod, trunk accelerations were at the same time measured with a stand-alone accelerometer unit, the DynaPort®hybride unit (56 × 61 × 15 mm, 54 g; McRoberts BV, The Hague, the Netherlands), which was considered the ‘golden standard’ in the present study. The Dynaport unit consists of tri-axial accelerometers collecting data at 100 Hz and stores the data on a SD card.
Procedure
The accelerometer unit was fixed with an elastic belt near the level of lumbar segment L3 over the clothes. The iPod was firmly attached with Velcro to the stand-alone accelerometer.
To assess the validity of the iPod to quantify gait and postural control, the participant performed walking and standing tasks. In the walking task the participant walked for 3 min at a self-selected speed up and down a 10 m long course with a 1 m curve, under single and dual task condition. The dual task consisted of a letter fluency test; the participant had to name as many words starting with a predefined letter (D-A-T) as they could within 1 min.24
Participants performed two standing tasks, (1) parallel stance and (2) semi-tandem stance. Each standing task consisted of three conditions, which were performed for 1 min: eyes open, eyes closed, standing while concurrently performing a dual task. The dual task was the same as during walking but now with the letters ‘G’ and ‘P’.
To investigate the test–retest reliability of the iPod, the 3 min walking test under single task condition and the standing parallel and semi-tandem with eyes open were performed twice.
The tasks (walking, standing) were randomized, and within one task all conditions were randomized for each participant.
Data Analysis
Anterior–posterior (AP) and medio-lateral (ML) trunk acceleration signals of the iPod and of the accelerometer unit were analyzed using custom-made software in MATLAB (version 2012b, The MathWorks Inc., Natick, MA, USA). The sampling rate of the iPod was not constant; therefore the data were interpolated to get a constant sampling of 100 Hz.
First, a cross-correlation analysis was performed between the two devices, respectively for the AP and ML accelerations, for each subject and each trial. We were specifically interested in the maximal correlation between the signals and the associated time lag, to compare the similarity of the pattern of the signals of the two measurement devices. The cross-correlation value between the signals was calculated at all possible time lags (of 0.01 s) for all trials. The time lag associated with the maximal cross-correlation was used to synchronize the data.
Gait Analysis
Prior to the gait analyzes the iPod and accelerometer unit signals were detrended and filtered (4th order Butterworth; cut-off frequency 20 Hz).
Due to their relevance in clinical research the following gait parameters were obtained from accelerometer data from the walking trials: foot contacts (FC), the Index of Harmonicity (IH), and the amplitude variability (AmpVar).
From FC conventional step parameters are derived, such as step time or stride time and the variability of step or stride time. Therefore, an accurate detection of the FC is important. FC were detected based on the minima of the smoothed (Butterworth filter, 4th order; cut-off frequency 2 Hz) AP signal. Using these detected peaks as reference, the FC (nearest peaks) were determined in the unfiltered signal. To assess the agreement between the detection of the FC by the iPod and by the accelerometer unit data, the mean difference of number of samples between the detected FC was calculated for each trial.
The IH was calculated for the individual AP and ML accelerations using spectral analysis and is considered an indicator of the smoothness of the acceleration patterns.11 The power spectrum of the acceleration data of ML and AP accelerations was estimated by means of a discrete Fourier transform. The peak power of the first subsequent 10 harmonics was estimated. The IH was defined as:
where P 1 is the power spectral density of the fundamental frequency (first harmonic, stride frequency), and ΣP i the cumulative sum of power spectral density of the fundamental frequency and the first 10 super-harmonics. A power ratio of 1 indicates that accelerations are perfectly harmonic. In view of possible drift, the power spectral density of each peak was calculated within the frequency bands of +0.1 and −0.1 Hz of the peak frequency value. All power spectral densities were normalized by dividing the power by the sum of the total power spectrum, which equals the variance.
Finally, the AmpVar provides an indication of the between gait cycle variability. First all strides were time normalized to 100 data points per stride (100% gait cycle). Standard deviations across the normalized strides were calculated, representing the stride variability for each trial.
Posture Analysis
Prior to the analyzes of the AP and ML signals during the standing tasks, a high pass fourth order Butterworth filter was applied with a cut-off frequency of 0.3 Hz to correct for slow drifts during standing, Additionally, a third-order Savitsky–Golay smoothing filter with frames of 41 points to eliminate low amplitude measurement noise.
The root mean square (RMS, m/s2) indexed the variability of the accelerations of body sway in AP and ML accelerations. To assess the frequency content of the AP and ML acceleration signals, the frequency content of the time-series was determined by calculating the median of the total power of the signal (MPF, Hz). The MPF was derived from the power frequency spectrum estimated by Welch’s method, using a Hamming window without overlap. To quantify the entire acceleration path the Sway Area (SA, m2/s5) was calculated. The SA is the area enclosed by the acceleration path in the AP-ML plane during the one minute stance. To obtain a mean value for the SA, first, the AP-ML path diagram was divided into 72 segments of angles of 5° each (see Fig. 1). From the AP and ML signals the resultant vector R was calculated. In each segment the largest resultant vector (R i ) was determined. The area enclosed by two subsequent maximal R i of a segment was calculated (S i ). By summing up the 72 segment areas the SA is approximated.6

On the left side, a presentation of the total sway area (SA) is plotted for the anterior–posterior (AP) and medio-lateral (ML) accelerations. On the right side, a close-up of the upper right quadrant of the SA, illustrating the calculation of the SA. SA = sum of S i based on the largest resultant vectors (R i , R i+1) for each segment
Statistical Analysis
To get insight into the individual spread of the measurement error between the iPod Touch and the accelerometer unit the computed gait and postural parameters were analyzed using Bland–Altman tests. In Bland–Altman plots, the average value for each pair of measurement is plotted against the mean difference between the two values of the two measurement devices of individual data of all conditions within a task. In addition, the upper and lower limit of agreement as 1.96 × standard deviation, the coefficient of agreement (%) as the limit of agreement expressed as a percentage of the mean of the value of the two devices, and the coefficient of variance (%) as the standard deviation divided by the mean value of the two measurement devices were calculated.
The validity of the gait (IH, AmpVar) and posture parameters (RMS, MPF, SA) derived from the signals of the iPod and accelerometer unit, was assessed using a case 2 intra-class correlation26 as:
where, BMS is the mean squares between measurements of the two devices, EMS is the within measurements mean squares of error and k is the number of devices (k = 2).
The test–retest reliability of the gait and posture parameters obtained from the iPod accelerometer signal was examined by calculating the case 1 intra-class correlation between measurements of the same condition (e.g., walking under single task condition, parallel stance and semi-tandem stance with eyes open) as:
where, JMS is the mean squares between the devices and n is the number of measurements (n = 2).
ICCs were calculated, separately for all conditions and for age categories, using MATLAB software (version 2012b, The MathWorks, Inc., Natick, MA, USA). The following guidelines were used to interpret the ICC values: >0.80 represents excellent reliability, 0.60–0.80 good reliability 0.40–0.60 moderate reliability and <0.40 poor reliability.26 A p value of <0.05 was considered statistically significant.
Results
Gait Parameters
Averaged across participants, mean walking speed was 1.2 m/s (± 0.12 m/s) during walking without dual task and 1.1 m/s (±0.21 m/s) during walking with a cognitive dual task. Data of two trials in each condition were excluded because the data were not completely recorded by the iPod or the accelerometer unit due to technical reasons.
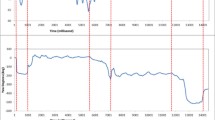
The pattern of time series of the AP and ML accelerations were very similar (see Fig. 2 for a representative example) as also indicated by the high (≥0.90) cross-correlation values between the signals of the two devices for AP as well as ML accelerations in both walking conditions. The associated mean time lags were 0.3 s (single task) and 0.4 s (dual task). Table 1 shows the cross-correlation values and corresponding time lags for both walking conditions. The FC detected based on the iPod and accelerometer unit signals differed on average 0.02 s (2 samples) for both single and dual task conditions.

Synchronised iPod (red line) and stand-alone accelerometer (blue line) acceleration signals in anterior–posterior (AP) and medio-lateral (ML) planes during walking. The cross-correlation value is displayed in the right corner of the plots
Figure 3 represents Bland–Altman plots for the IH and the VarAmp. Overall, the measurement error between the two devices was very low as indicated by mean values close to zero and the small limits of agreement. However, in two participants the difference between the devices was higher than might be expected based on the other participants’ measurements, causing the outliers in the IH and VarAmp. In line, the RPC% and CV of these participants were also low.

Bland-Altman plots of the mean of the measurements of the iPod and the stand-alone accelerometer (Acc.Unit; x-axis) against the difference of the measurement of individual participants, for the index of harmonicity (IH) value and the amplitude variability (VarAmp) during walking in anterior–posterior (AP) and medio-lateral (ML) plane. White squares represent young adults, red the middle aged adults, and gray the older adults. RPC% is the reproducibility coefficient as % of the mean. CV is the coefficient of variation
Validity and reliability were high for the IH and AmpVar for AP and ML accelerations in both walking conditions indicated by ICC values between 0.85 and 0.98. There were no differences in accuracy or reliability found for the three age categories. Table 2 shows the ICCs and confidence intervals per condition.
Posture Parameters
Fifty-seven participants completed all standing conditions. Two participants were not able to maintain the semi-tandem stance with eyes closed for one minute and one participant did not perform the semi-tandem with dual task according to protocol. Those three trials, all of participants in the older adult category, were excluded from the analysis.
The cross-correlation values between the iPod and the accelerometer unit signals were ≥0.88 for the AP and ML directions in all standing conditions. The mean time lag was between the 0.3–0.4 s (see Table 1).
As shown in Fig. 4, Bland–Altman plots showed very good levels of agreement for the RMS values between the two measurement devices. Almost all RMS values of both standing tasks are within the limits of agreement. Individual spread of measurements was larger for ML RMS than AP RMS. For tandem stance, more values of participants in the older adults’ category fell beyond the limits of agreement.

Bland-Altman plots of the mean of the measurements of the iPod and the stand-alone accelerometer (Acc.Unit; x-axis) against the difference of the measurement of individual participants, for the RMS value of anterior–posterior (AP) and medio-lateral (ML) accelerations during parallel standing and semi-tandem stance. White squares represent young adults, red the middle aged adults, and gray the older adults. RPC% is the reproducibility coefficient as % of the mean. CV is the coefficient of variation
Bland–Altman plots of the MPF (Fig. 5) showed that the majority of the values are within the limits of agreement. However, the spread of the values was larger for MPF than for RMS values, in particularly of the participants in the young adult category, as quantified by a higher reproducibility coefficient expressed as percentage of the mean percentage (RMS RPC%, <15%, and MPF RPC% between 32 and 45%).

Bland-Altman plots of the mean of the measurements of the iPod and the stand-alone accelerometer (Acc. Unit; x-axis) against the difference of the measurement of individual participants, for the median power frequency (MPF) value of anterior–posterior (AP) and medio-lateral (ML) accelerations during parallel standing and semi-tandem stance. White squares represent young adults, red the middle aged adults, and gray the older adults. RPC% is the reproducibility coefficient as % of the mean. CV is the coefficient of variation
SA measurement had small limits of agreement, however, as is shown in Fig. 6 in both conditions one subject falls far beyond the limits of agreement increasing the SD and the RPC% values.

Bland-Altman plots of the mean of the measurements of the iPod and the stand-alone accelerometer (Acc. Unit; x-axis) against the difference of the measurement of individual participants, for the sway area (SA) in anterior–posterior (AP) and medio-lateral (ML) plane during parallel standing and semi-tandem stance. White squares represent young adults, red the middle aged adults, and gray the older adults. RPC% is the reproducibility coefficient as % of the mean. CV is the coefficient of variation
Table 3 gives an overview of the ICC values and confidence intervals per condition and the reliable ICC values for the three age categories. The ICC values, to assess the validity of the iPod during standing, were ≥0.97 for the RMS and the SA. The MPF had ICC values between 0.84 and 0.97. Separate analysis for the age categories revealed no differences in validity, ICC’s for the MPF ranged from 0.85 to 0.97 and for the RMS from 0.97 to 1.00, respectively.
ICC values for the test–retest reliability of AP and ML RMS during parallel stance and semi-tandem stance were between 0.83 and 0.90. The MPF had values ≥0.78 except for the parallel stance with eyes open in AP direction for which an ICC value of 0.59 was found. The individual MPF ICC values for the age groups differed during parallel stance, the ICC values for the young, middle aged and older adults were respectively, 0.39, 0.78 and 0.62 for AP, and 0.86, 0.25 and 0.70 for ML.
Overall, the ICC for the test–retest reliability of SA was 0.81 in the parallel stance and 0.91 in the semi-tandem stance. At the group level, the young adult category had ICC values lower on the SA parameter in both parallel standing and semi-tandem stance (respectively, ICC values of 0.57 and 0.55), compared to the other two groups (Table 3).
Discussion
The aim of the present study was to establish the validity and test–retest reliability of the iPod Touch in quantifying gait and standing postural control under different conditions (eyes open, eyes closed and dual task) in healthy adults divided into three age categories (young, middle aged and older adults). We compared different acceleration signal characteristics of the iPod Touch with those of a stand-alone accelerometer unit considered as the golden standard. For the walking condition the pattern of the raw signals, the FC detection, the frequency content indexed by the IH and the VarAmp were assessed. Similarly, for the posture task, the pattern of the acceleration signals were compared using cross-correlation analysis, the variability in the signal was calculated by the RMS, the frequency content estimated by the MPF and the amplitude of the sway acceleration using a sway area measure in the AP ML plane.
The cross-correlation values indicated a very similar signal pattern of the two devices for all subjects, and task conditions. A short time delay was found, due to the fact that both devices did not start at exactly the same time.
For walking a FC detection algorithm was compared between the two devices, because many step related gait parameters such as the mean stride time, the coefficient of variation of stride time and gait symmetry indexes, rely on FC detection. In the present study, we used a validated algorithm30 with the differences that instead of the maximum peak of the AP acceleration the minima of the AP peak within a step cycle was determined. The differences between detected peaks of the iPod and the accelerometer unit was negligible small only 0.02 s (2 samples), and thus can be considered valid.
The IH and VarAmp, representing the smoothness of the acceleration pattern and the variability in gait cycles during walking respectively, were valid and reliable outcome parameters measured with the iPod during walking under both single and dual task conditions. This is in agreement with a previous study reporting good validity and reliability for gait measured under single task condition with a smart phone in a group of young healthy subjects.21 Furthermore, our study showed that the iPod has valid and reliable results in young, middle aged and older healthy adults. The outliers in the Bland–Altman plots for IH and VarAmp were originative from two participants. The two participants represented the two lowest individual cross-correlation values (respectively 0.51 and 0.57). Although it was not observed and reported during the measurements, the low cross-correlations and consequently the outliers in the Bland–Altman plots, indicated that there was a lose fixation of the iPod and stand-alone accelerometer to the participant’s lower back.
The posture parameters (RMS, MPF and SA) were valid for all six standing conditions and for the three age categories. Although the limits of agreement were small for all variables, the Bland–Altman plot showed outliers in the parallel stance and semi-tandem stance in the SA parameter. Those outliers were recorded during the dual task condition, the participants were laughing during the trial causing the aberrant values. Both the iPod and the commercial unit registered the outlier, underlining the validity of the iPod.
The test–retest reliability for the RMS and SA in the two standing conditions was good. However, the reliability on the MPF was lower. Additionally, the individual age groups showed large differences on the ICC values for the MPF in AP and ML planes during parallel stance and in AP in semi-tandem stance. This might be due to the signal/noise ratio during the postural task. The trunk movements are quite small during standing, and although we filtered the data, noise within the frequency range of the movement can influence the outcomes of the parameters, particular the outcomes in the power spectrum.17 Unfortunately, this type of noise cannot be removed by filters because accelerations related to the movement of the participant will be removed too.29 The results of the present study indicate that for the test–retest reliability more repeated measurements are needed to obtain reliable estimates for postural control parameters.
The SA parameter seemed high reliable for the middle aged and older adults, whereas young adults showed lower test-retest reliability (Table 3). A possible explanation might be the variation in the young participants balance strategy across the testing session due to the easy level of the stances and therefore performing more variable movements. In contrast, when the tasks are more challenging for instance for persons with movement pathology, the standing task might be performed with less variability. In line with this thought studies in stroke patients and low back pain patients showed a higher reliability in more challenging standing conditions (eyes-closed condition) compared to an easier condition (eyes-open condition).15,25
The iPod Touch used in the present study was fixed near the lower back around L3. Placement at the lower back is frequently used to determine gait and postural parameters due to the location near the body’s center mass.18,30 Motions of the body’s center of mass are detected and strike patterns of both feet are obtained. However, future research should investigate whether placement of smart devices on other places than the lower back obtains valid and reliable outcome parameters during gait and postural tasks.
Overall, the results showed that trunk accelerations in AP and ML planes measured with an iPod Touch during gait and postural tasks were accurately measured in young, middle aged and older healthy adults under different sensory and dual-task conditions. The gait and posture parameters derived from the iPod acceleration signals were demonstrated to be valid and reliable. Further work will include patient populations, frail elderly and old adults with an increased fall risk to assess the accuracy of smart devices in those populations.
The iPod Touch is a convenient, easy to use, cost-effective device to assess AP and ML trunk acceleration during gait and posture. To make the use of smart devices accessible for clinical practice applications need to be developed for gait and posture testing including algorithms not only for data recording and storage but also for data analysis, providing feedback to the person or clinician about gait and posture function. With the use of the tri-axis accelerometer embedded in a smart device and apps with algorithms to evaluate gait and postural control specifically developed for different end users, clinicians and researchers can accurately monitor gait and postural control to detect fall risk or evaluate the effectiveness of an intervention to improve gait and/or posture. To develop successful applications, gait and postural parameters need to be determined that are specific and sensitive to changes in aging to develop reliable and sensible applications for the clinical setting.
References
Boulgarides, L., and S. McGinty. Use of clinical and impairment-based tests to predict falls by community-dwelling older adults. Phys. Ther. 83:328–339, 2003.
De Groot, M. H., J. P. C. M. van Campen, M. A. Moek, L. R. Tulner, J. H. Beijnen, and C. J. C. Lamoth. The effects of fall-risk-increasing drugs on postural control: a literature review. Drugs Aging 30:901–920, 2013.
De Groot, M. H., H. C. van der Jagt-Willems, J. P. C. M. van Campen, W. F. Lems, J. H. Beijnen, and C. J. C. Lamoth. A flexed posture in elderly patients is associated with impairments in postural control during walking. Gait Posture 39:767–772, 2014.
Hartmann, A., K. Murer, R. A. de Bie, and E. D. de Bruin. Reproducibility of spatio-temporal gait parameters under different conditions in older adults using a trunk tri-axial accelerometer system. Gait Posture 30:351–355, 2009.
Howcroft, J., J. Kofman, and E. D. Lemaire. Review of fall risk assessment in geriatric populations using inertial sensors. J. Neuroeng. Rehabil. 10:91, 2013.
Hufschmidt, A., J. Dichgans, K. H. Mauritz, and M. Hufschmidt. Some methods and parameters of body sway quantification and their neurological applications. Arch. Psychiatr. Nervenkr. 228:135–150, 1980.
Ijmker, T., and C. J. C. Lamoth. Gait and cognition: the relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 35:126–130, 2012.
Karlsson, M. K., T. Vonschewelov, C. Karlsson, M. Cöster, and B. E. Rosengen. Prevention of falls in the elderly: a review. Scand. J. Public Health 41:442–454, 2013.
Kwok, T. M. K., and C. Y. Tong. Effects on centre-based training and home-based training on physical function, quality of life and fall incidence in community dwelling older adults. Physiother. Theory Pract. 30:243–248, 2014.
Lamoth, C. J. C., E. Ainsworth, W. Polomski, and H. Houdijk. Variability and stability analysis of walking of transfemoral amputees. Med. Eng. Phys. 32:1009–1014, 2010.
Lamoth, C. J. C., P. J. Beek, and O. G. Meijer. Pelvis-thorax coordination in the transverse plane during gait. Gait Posture 16:101–114, 2002.
Lamoth, C. J., F. J. van Deudekom, J. P. van Campen, B. A. Appels, O. J. de Vries, and M. Pijnappels. Gait stability and variability measures show effects of impaired cognition and dual tasking in frail people. J. Neuroeng. Rehabil. 8:2, 2011.
Lamoth, C. J. C., and M. J. G. van Heuvelen. Sports activities are reflected in the local stability and regularity of body sway: older ice-skaters have better postural control than inactive elderly. Gait Posture 35:489–493, 2012.
Lee, J., A. I. Geller, and D. C. Strasser. Analytical review: focus on fall screening assessments. PM R 5:609–621, 2013.
Liston, R. A., and B. J. Brouwer. Reliability and validity of measures obtained from stroke patients using the Balance Master. Arch. Phys. Med. Rehabil. 77:425–430, 1996.
Mancini, M., A. Salarian, P. Carlson-Kuhta, C. Zampieri, L. King, L. Chiari, and F. B. Horak. ISway: a sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 9:59, 2012.
Martinez-Mendez, R., M. Sekine, and T. Tamura. Postural sway parameters using a triaxial accelerometer: comparing elderly and young healthy adults. Comput. Methods Biomech. Biomed. Engin. 15:899–910, 2012.
Moe-Nilssen, R. A new method for evaluating motor control in gait under real-life environmental conditions. Part 2: gait analysis. Clin. Biomech. 13:328–335, 1998.
Moe-Nilssen, R. Test-retest reliability of trunk accelerometry during standing and walking. Arch. Phys. Med. Rehabil. 79:1377–1385, 1998.
Nguyen, U. S. D. T., D. P. Kiel, W. Li, A. M. Galica, H. G. Kang, V. A. Casey, and M. T. Hannan. Correlations of clinical and laboratory measures of balance in older men and women. Arthritis Care Res. (Hoboken) 64:1895–1902, 2012.
Nishiguchi, S., M. Yamada, K. Nagai, S. Mori, Y. Kajiwara, T. Sonoda, K. Yoshimura, H. Yoshitomi, H. Ito, K. Okamoto, T. Ito, S. Muto, T. Ishihara, and T. Aoyama. Reliability and validity of gait analysis by android-based smartphone. Telemed. J. E. Health. 18:292–296, 2012.
Patterson, J. A., R. Z. Amick, T. Thummar, and M. E. Rogers. Validation of measures from the smartphone sway balance application: a pilot study. Int. J. Sports Phys. Ther. 9:135–139, 2014.
Pluijm, S. M. F., J. H. Smit, E. A. M. Tromp, V. S. Stel, D. J. H. Deeg, L. M. Bouter, and P. Lips. A risk profile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteoporos. Int. 17:417–425, 2006.
Schmand, B., S. C. Groenink, and M. den Dungen. Letterfluency: psychometrische eigenschappen en Nederlandse normen. Tijdschr. Gerontol. Geriatr. 39:64–74, 2008.
Sherafat, S., M. Salavati, I. Ebrahimi Takamjani, B. Akhbari, S. Mohammadirad, M. Mazaheri, and H. Negahban. Intrasession and intersession reliability of postural control in participants with and without nonspecific low back pain using the Biodex Balance System. J. Manipulative Physiol. Ther. 36:111–118, 2013.
Shrout, P. E., and J. L. Fleiss. Intraclass correlations: uses in assessing rater reliability. Psychol. Bull. 86:420–428, 1979.
Spain, R. I., R. J. St George, A. Salarian, M. Mancini, J. M. Wagner, F. B. Horak, and D. Bourdette. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Posture 35:573–578, 2012.
Tromp, A. M., S. M. F. Pluijm, J. H. Smit, D. J. H. Deeg, L. M. Bouter, and P. Lips. Fall-risk screening test : a prospective study on predictors for falls in community-dwelling elderly. J. Clin. Epidemiol. 54:837–844, 2001.
Van Hees, V. T., S. M. Slootmaker, G. De Groot, W. Van Mechelen, and R. C. Van Lummel. Reproducibility of a triaxial seismic accelerometer (DynaPort). Med. Sci. Sports Exerc. 41:810–817, 2009.
Zijlstra, W., and A. L. Hof. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 18:1–10, 2003.
Acknowledgments
We thank Kees Hoogendijk for developing the data collection and storage app on the iPod, and Esther du Pre and Yvonne Dikkema for their help in collecting the data. The project was financed by the Institut Universitair de France and Investments for the Future IRT NanoElec. We certify that the studies sponsors had no involvement in the study design, in the collection, analysis and interpretation of data, in the writing of the manuscript, or in the decision to submit the manuscript for publication.
Conflict of interest
The authors declare that they have no proprietary, financial, professional, or other personal competing interests of any nature or kind.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Tingrui Pan oversaw the review of this article.
Rights and permissions
About this article

Cite this article
Kosse, N.M., Caljouw, S., Vervoort, D. et al. Validity and Reliability of Gait and Postural Control Analysis Using the Tri-axial Accelerometer of the iPod Touch. Ann Biomed Eng 43, 1935–1946 (2015). https://doi.org/10.1007/s10439-014-1232-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-014-1232-0