
Abstract
Direct electrical stimulation of the colon offers a promising approach for the induction of propulsive colonic contractions by using an implantable device. The objective of this study was to assess the feasibility to induce colonic contractions using a commercially available battery-operated stimulator (maximum pulse width of 1 ms and maximum amplitude of 10 V). Three pairs of pacing electrodes were inserted into the cecal seromuscular layer of anesthetized pigs. During a first set of in vivo experiments conducted on six animals, a pacing protocol leading to cecum contractions was determined: stimulation bursts with 1 ms pulse width, 10 V amplitude (7–15 mA), 120 Hz frequency, and 30-s burst duration, repeated every 2–5 min. In a second testing phase, an evaluation of the pacing protocol was performed in four animals (120 stimulation bursts in total). By using the battery-operated stimulator, contractions of the cecum and movement of contents could be induced in 92% of all stimulations. A cecal shortening of about 30% and an average intraluminal pressure increase of 10.0 ± 6.0 mmHg were observed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Several acute and chronic studies of direct electrical stimulation have been performed over the last decade on different segments of the gastrointestinal tract: (1) electrical stimulation of the stomach for the treatment of gastroparesis,7,9 (2) electrical stimulation of the small intestine to induce propulsive waves6 and to initiate local contractions that could propel an endoscope,10 and (3) direct stimulation of different colonic segments to evacuate a colonic pouch4 or induce propagating waves.1–3,8,11,13 All these experimental studies performed on cats,3 dogs,2,4,6,11 and pigs1,8,10,13 showed promising results and the published stimulation parameters cover a broad range: 10–120 Hz for the frequency, 0.5–70 ms for the pulse width, 7–100 mA for the current amplitude, and 10–30 s for the duration of one stimulation burst.1–4,6,8,10,11,13
The objective of this study was to determine the feasibility and methodology to induce colonic contractions using a battery-operated device, with electrodes implanted into the colonic seromuscular layer of anesthetized pigs. Sevcencu et al. recently proposed a method of electrical stimulation using low values for stimulation amplitude (15 mA) and pulse duration (3 ms) to induce propulsive contractions on the descending colon of pigs.13 The work presented here follows a similar approach. It focuses on the determination of stimulation parameters which result in colonic contractions based on the use of an external battery-operated stimulator with a limited power and pacing electrodes which are commercially available.
Materials and Methods
Surgical Procedure
Acute experiments were performed on 10 anesthetized farm pigs (5 males and 5 females) with an average weight of 44 ± 6.1 kg. The in vivo protocol was reviewed and approved by the local Ethics Committee on animal care (Office Vétérinaire Cantonal Lausanne). All animals received care in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care and Use of Laboratory Animals” (NIH Publication No. 86-23, revised 1985).
Anesthesia and surgical procedures were applied as described recently.1 General anesthesia was induced by inhalation of isoflurane and maintained by a perfusion of alpha-chloralose. The surgery consisted of a median laparotomy and exposure of the cecum. The colonic segments were regularly moisturized with a saline solution at body temperature. Manipulations that could affect colonic motility, such as resection, ligatures, or incisions, were minimized.
Unipolar temporary myocardial pacing electrodes of stainless steel 316L with an electrode length of 3 mm and ∅ 0.8 mm (Medtronic 6500) were inserted into the cecal seromuscular layer. Three pairs of electrode were sutured every 4–5 cm, the electrodes of each pair being placed diametrically opposite to each other. A needle (length 32 mm, ∅ 0.61 mm, 3/8 curved) was employed to advance the electrode into the colonic seromuscular layer. The insulation material was fluorinated ethylene propylene. The electrodes were flexible enough to follow the anatomy of the colon without restricting its movements and were suited for their use with existing implantable neurostimulation devices.
Each experiment lasted about 4 h after which the animals were sacrificed by administrating an overdose of pentobarbitone.
Electrical Stimulation Protocol
Electrical stimulation was delivered by an external battery-operated neurological stimulator (Medtronic Model 3625 Test Stimulator) generating rectangular pulses with a width in the range of 50–1000 μs, a frequency range of 5–120 Hz, and an amplitude range of 0–10 V. The maximum output current of the stimulator was 30 mA. The stimulator output has a capacitive coupling to electrodes, meaning that the stimulating waveforms are in fact bipolar even if they are asymmetric. This capacitive coupling avoids the imbalance in charge generated by monopolar waveforms that could cause implanted electrode corrosion. This external device is used in clinical practice to test whether a particular patient might benefit from stimulation and should receive a definitive, implantable neurostimulator with the same electrical characteristics. During stimulation, the delivered current was computed as follows (Fig. 1): a series resistor of 10 Ω was placed between the stimulator and the electrodes and the voltage drop across the resistor was measured with an oscilloscope. The stimulation current was then computed using Ohm’s law and the impedance was obtained by dividing the applied voltage by the stimulation current.

Experimental setup with the three systems used to record colonic activity: (1) digital video recording, (2) intraluminal pressure measure, and (3) Magnet Tracking System. Stimulation was delivered using a Medtronic 3625 battery-operated stimulator connected sequentially to one pair of electrodes at a time using a switching module. The delivered current was measured by assessing the voltage drop with an oscilloscope through a series resistor (10 Ω)
A first development phase of in vivo experiments was performed on 6 pigs (2 males and 4 females, average weight 42.8 ± 5.6 kg) with the aim of determining the ideal combination of pulse width, frequency, amplitude, and stimulation burst duration needed to generate a cecal contraction with the battery-operated stimulator. The values needed to induce a visually assessed tonic contractions following the onset of the stimulation burst were determined. This phase was started with 90-s stimulation bursts. The different values for amplitude, pulse width, and frequency were set via the stimulator. Using the maximum pulse width (1 ms) and the maximum frequency (120 Hz), the amplitude was increased by 1 V steps until the threshold for a visible cecal contraction was reached. The threshold values for pulse width and frequency were tested in a similar way. Once the combination of amplitude, pulse width, and frequency leading to a cecal contraction was found, the stimulation burst duration was lowered from 90 s by 5-s steps to find its minimal value.
A second testing phase of in vivo experiments consisted of an evaluation of the effect and reproducibility of the electrical stimulation parameters determined in the first development phase, in 4 pigs (3 males and 1 female, average weight 44.5 ± 5.5 kg). Stimulations were distributed equally between the three pairs of electrode implanted into the cecal seromuscular layer. Each pair was stimulated independently. A switching module between the stimulator and the electrodes (Fig. 1) was used to select a specific pair of electrodes according to the following protocol: a stimulation burst was applied to the first pair, a second stimulation burst to the second pair after a 2- to 5-min stimulation pause, and the last stimulation burst to the third pair after another 2- to 5-min pause. The sequential stimulation of the three pairs was repeated for a total of 120 stimulation bursts in the four animals (23, 30, 24, and 43 stimulation bursts, respectively). The distribution of the stimulation bursts to three pairs of electrodes with different spatial locations on the cecum reduced the dependence of the testing phase on electrode location.
Data Acquisition
In the testing phase, the following data were collected to assess the colonic contractions induced by each stimulation burst on each pair of electrode (Fig. 1): (1) video imaging of cecal shortening, (2) intraluminal pressure changes, and (3) assessment of the movement of the intraluminal contents. The three measurements were taken simultaneously and continuously during the experiments.
Visual changes in cecal wall conformation resulting from contractions were assessed by circular blue markers (∅ 5 mm) and were recorded with a SONY digital camera as previously described1 and shown in Fig. 2. These markers were glued using Tissucol® fibrin glue every 1–2 cm both in the longitudinal (7–10 markers) and transverse (3 markers) directions. The camera was linked by IEEE 1394 (FireWire) to a personal computer, where periods of interest were selected and analyzed by tracking the markers on the video sequence.

Cecal conformational changes induced by a single stimulation burst with 1 ms pulse width, 10 V amplitude, and 120 Hz frequency. Markers were glued on the serosa for further image processing and placed in order to form several lines in cecal axis direction. (a) Cecum at rest. (b) Time = 20 s, the maximum strength of a deeply haustrated contraction developed at the pacing site and propagated orally and aborally about 10 cm. White arrows indicate the simulating electrode pair and gray arrows the adjacent nonstimulating pair. (c) Time = 30 s, the stimulation was stopped. (d) Time = 80 s, the cecum almost came back to its resting position. (e) Cecal morphological changes illustrated by the superposition of cecal contours when fully contracted (plain line) compared with the resting position (dashed line)
A perfusion catheter (Sedia AG, Givisiez, Switzerland) introduced via a small ileotomy into the cecal lumen was used to record the intraluminal pressure changes as described in Aellen et al. 1
The movement of the intraluminal contents was monitored noninvasively using the Magnet Tracking System (Motilis Sàrl, St-Sulpice, Switzerland).12 This system allowed us to track in real time on a laptop computer the movements (translation and rotation) of a cylindrical permanent magnet introduced into the cecal lumen.
Data Analysis
Lammers et al. presented a new technique to monitor the motility of isolated feline duodenum based on digital video recordings5: various marker dots were placed on the serosal surface, spontaneous movements of the dots were recorded, and a software was developed to process offline the video frames and track the marker movements. We followed a similar approach and developed an image processing tool under Matlab® (The MathWorks, Inc.) to track during electrical stimulation the position of the markers glued on the cecal wall. For each frame of the digital video sequence, the position of all markers was evaluated as follows: the area representing each marker was assessed based on color selection (the blue color of the markers being different from the rest of the image). Then, the marker positions were identified using the center of mass of the selected area. A ruler placed near the markers was used as reference for the marker positions (Fig. 2). The displacement of each marker was estimated by analyzing the whole frame sequence. The relative displacement between two markers representative of the observed colonic contraction provided an estimate of the tissue shortening.
The data about intraluminal pressure changes and movement of the intraluminal contents were both sampled at 10 Hz and analyzed. The time interval between the start of stimulation and the contraction maximum was computed. The magnitude of the maximal pressure obtained after stimulation was also determined and compared to baseline values. Results were documented using mean ± standard deviation and median. Statistical analysis was performed with a one-way analysis of variance (ANOVA).
Results
Determination of Stimulation Protocol
In the development phase, the minimum amplitude needed to generate in all animals an occlusive contraction with the maximum pulse width available (1 ms) was 8 V. Since the output of the stimulator was limited to 10 V, it was not possible to initiate a contraction at shorter pulse widths. Pacing frequencies in the range of 40–50 Hz were found to be sufficient to induce contractions in most cases but higher frequencies (up to the maximum output of 120 Hz) tended to generate stronger contractions. Stimulation bursts were applied for 5–90 s and the contraction peak was reached 5–25 s after the onset of the stimulation burst. Based on these observations, the following parameters were chosen for the stimulation protocol to be tested in the second phase: (1) stimulation of the colon with 1 ms pulse width, amplitude 10 V, frequency 120 Hz for a duration of 30 s and (2) break of stimulation during 2–5 min to allow the cecum to return to its initial resting state.
Electrically Induced Colonic Contractions
In the testing phase, contractions of the cecum were generated in all animals and in 110/120 stimulation bursts (92%). Current amplitude was in the range of 7–15 mA, and tissue impedance was in the range of 670–1430 Ω. An example of image analysis of a generated colonic contraction is shown in Fig. 3.

Example of morphological changes in cecal wall conformation during a 30-s stimulation burst with 1 ms pulse width, 10 V amplitude, and 120 Hz frequency. The evolution of the distance d between the two nonadjacent markers glued on the cecum is represented over time. Circles indicate the instant corresponding to the frames A–D. Stimulation started at position A and induced a local contraction reaching its maximum about 20 s later at position B, just before the end of the stimulation. During this phase, the distance between two nonadjacent markers placed along the longitudinal axis decreased from 3.7 to 2.7 cm, corresponding to a longitudinal shortening of 27%. After electrical stimulation was interrupted, a relaxation phase occurred during which several weaker contractions (such as from position C to D) or oscillations were observed. The markers returned to their initial position after 2–3 min
Contraction induced by stimulation involved a shortening in both longitudinal and radial directions. For all experiments, marker displacements were in the range of 1–3 cm. The corresponding longitudinal shortening was about 30%. All contractions exhibited a similar pattern: just following the beginning of electrical stimulation, a strong local contraction was generated. Once the electrical stimulation was stopped, a relaxation phase occurred during which oscillations of the colonic wall could be observed and were propagated in the anterograde and retrograde direction during 1–2 min, over a distance of about 10 cm (Fig. 3).
Pressure Increase
The effect of electrical stimulation on intraluminal pressure is presented in Fig. 4. The mean basal pressure before stimulation was 11 ± 4.2 mmHg (median 13 mmHg). Evoked contractions induced a pressure increase of up to 27 mmHg. Different types of pressure patterns were observed following stimulation: single contractions immediately following stimulation onset in 88% of the 110 stimulation bursts (Fig. 4a) or more complex patterns such as biphasic waves (Fig. 4b). For these biphasic waves, we observed in some cases that the second wave had a higher amplitude than the first one. Weaker contractions or oscillations were also observed in Fig. 4. These oscillations were previously described in Fig. 3 about marker displacements and were following the main contraction wave. They corresponded to the relaxation phase where the propagation of the contraction wave was observed.

Examples of pressure increase following electrical stimulation with 30-s burst, 1 ms pulse width, 10 V amplitude, and 120 Hz frequency. Vertical gray zones indicate periods of electrical stimulation: (a) examples of single pressure contraction waves (88% of stimulations) and (b) example of biphasic contractions (12% of stimulations). The period of time between stimulation bursts varied between 2 and 5 min. One exception is the example (b) where residual activity was still present 5 min after the stimulation was stopped needing a slightly longer period without stimulation
Quantitative Analysis
Quantitative analysis of intraluminal pressure changes and movement of the intraluminal contents are shown in Figs. 5 and 6. The statistical distribution of the time intervals between the start of stimulation and the maximum of the cecum contraction are presented in Fig. 5. The time interval after the onset of stimulation until detection of maximal displacement of intraluminal content by the Magnet Tracking System was 19.4 ± 11 s (median 16 s), whereas the time interval until maximal contraction detected by intraluminal pressure change was 20.5 ± 12.5 s (median 17 s). This difference was not found to be significant (p = 0.42).

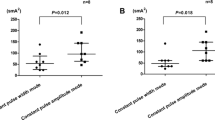
Statistical distribution of the time interval between the start of stimulation and the maximum of the cecal contraction for the N = 110 stimulation bursts performed in the four animals of the second experimental phase: (a) maximal displacement of intraluminal contents measured with the Magnet Tracking System and (b) maximum of the contraction assessed via intraluminal pressure (measured with the manometry probe)

Statistical distribution of the maximal pressure increase with respect to baseline for the N = 110 stimulation burst performed in the four animals of the second experimental phase
The mean pressure increase when compared to baseline was 9.9 ± 5.7 mmHg (median 8.5 mmHg). The percentage of pressure increase from baseline was significant (74.9 ± 39.7%, p < 0.001), without difference between animals.
Discussion
The aim of this study was to assess the feasibility and methodology of inducing reproducible contractions of the pig’s cecum with a commercialized battery-operated neurostimulator. The optimal stimulation parameters were identified to be 10 V amplitude during 30 s, with a pulse width of 1 ms and a frequency of 120 Hz, according to the recently published data.1 The current amplitude was in the range of 7–15 mA. The contraction maximum was reached after a median of 16–17 s.
Published stimulation parameters for the animal colon can be divided into three categories: (1) experiments using high current amplitude (>30 mA): (2 ms, 100 mA, 10 Hz, 120 s) in pigs8 and (1 ms, 35 mA, 40 Hz, 60 s) in cats3; (2) experiments using long pulse widths (>5 ms): (10 ms, 10 V, 50 Hz, 6–18 s) in dogs2,11; and (3) experiments using short pulse widths (<5 ms): (3 ms, 15 mA, 10 Hz, 10 s) in pigs13 and (1 ms, 15 mA, 120 Hz, 30 s) present study in pigs.
The mean value of the applied stimulation current (defined as the product of pulse width, current amplitude, and frequency) was identified as being critical for the induction of the contraction. In the first group with high current amplitude, the mean value of the applied stimulation current was in the range of 1.4–2 mA.3,8 For the second group using long pulse widths, although no information was given by Amaris et al. about impedance or injected current,2 further studies by Sanmiguel et al. using a chronic model of the same pacing scheme with stimulation trains of 6 s led to a mean impedance of 342.12 ± 26.24 Ω and an effective value of the current of 7.8–9.9 mA.11 The computed mean value of the stimulation current was in the range of 7.0–8.9 mA. In the third group with short pulse widths, the mean value of the stimulation current was 0.45 mA for Sevcencu et al. 13 and was in the range of 0.8–1.8 mA for the present study. Therefore, except for the second group using long pulse widths, the mean values of the applied stimulation current were comparable (<2 mA).
Sanmiguel et al. followed the strategy of using longer pulse widths but with short stimulation trains (6 s instead of 30 s here). Their peak current value was in the range of 11–14 mA, which is comparable to the 7–15 mA measured in the present study. A higher mean value of the stimulation current was applied in Sanmiguel et al. compared to other published colon stimulation studies.11 However, the use of short stimulation trains maintained the energy needed for one stimulation burst within a comparable range (125–201 mJ, while it was ranging from 252 to 540 mJ in the present study). It should be noted that a safety margin was taken in our study in the selection of the stimulation parameters, and that in most cases stimulations at 50 Hz during 20 s were sufficient to induce contractions, implying a reduction of the required energy by a factor of 3.6.
Sevcencu et al. followed a strategy that differed from the three categories cited above.13 They simultaneously minimized the three stimulation parameters, instead of having two low and one high value. Since our objective was to use a commercially available battery-operated stimulator with a pulse width limited to 1 ms, this requested different constraints (Sevcencu et al. used pulse widths of 3 ms that were three times longer than the maximum pulse width of the present stimulator13). Nevertheless, the contractions generated were comparable. In the present study, the evoked contractions started within 1–2 s after onset of stimulation which is consistent with the findings of Sevcencu et al. 13 Mean pressure increase, with respect to baseline, was about the double of the value reported by Sevcencu et al. 13 The differences in pressure increase in the evoked contraction are probably related to the differences in mean values of the delivered stimulation current, the values in the present study being the double of the ones observed by Sevcencu et al. 13 A much higher stimulation frequency was used here (120 Hz instead of 10 Hz). However, it was noted that pacing frequencies in the range of 40–50 Hz were sufficient in most cases to induce contractions. In this study, the decrease of the pulse width to 1 ms linked to the Medtronic 3625 battery-operated stimulator implied this increase in stimulation frequency.
In most cases (88%), the pressure patterns generated by electrical stimulation were monophasic; however, in few cases, biphasic waves were observed. The second wave could be due either to fluctuations in cell excitability or to interactions of propagation within neighboring tissue. Series of contractions were more likely to occur after repetitive stimulations. Further experiments are needed to determine the exact cause.
Our approach was based on an in vivo model without colonic obstruction or incisions and with a colon naturally filled with fecal contents. This approach is more physiological than the one presented by Amaris et al. where openings were made in the colon through which artificial mixtures were injected.2 On the other hand, the assessment of the colonic contractions and movement of its contents was rendered more difficult. Sevcencu et al. followed a similar methodology and characterized the colonic contractions with changes in the cross-sectional areas measured with impedance planimetry, luminal pressure changes, and colonic active wall tension derived from pressure recording.11 Sanmiguel et al. tested their implantable neurostimulator in chronic studies, showing that stimulation could accelerate the movement of the colon content in a canine model of delayed transit.11 A combination of three techniques was used in the present study: video recordings, intraluminal pressure recordings, and the Magnet Tracking System. No significant difference could be observed between the time distribution of the generated contraction measured with a pressure catheter and the time distribution of the movement of intraluminal contents measured with the Magnet Tracking System. Therefore, this noninvasive system, measuring the displacement of an intraluminal magnet, could be used either with an open abdomen or a closed abdomen for experiments conducted on conscious animals.
After series of repetitive stimulations, a fatigue of the colon could be observed, i.e., decrease of amplitude and extent of contractions. In addition, even though the preparation was moistured, the exposure to air led progressively to serosal fibrin secretion. For these reasons, we considered only the responses obtained before the signs of fatigue and apparition of secretions. A previous work showed, with a histological analysis, that no tissue lesions were observed after the application of the electrical stimulation protocol.1 Future experiments conducted on conscious animals are required for further validation.
Conclusions
This study showed the feasibility of direct electrical stimulation of the colon using the Medtronic 3625 battery-operated stimulator and commercial pacing electrodes. The stimulation protocol consisted of stimulation bursts of 1 ms pulse width, 10 V amplitude (7–15 mA), 120 Hz, applied during 30 s every 2–5 min. Tonic contractions could be induced in 92% of cases with a 75% increase of intraluminal pressure with respect to baseline and a colonic wall shortening of about 30%. The maximum output of the Medtronic 3625 battery-operated stimulator (1 ms, 10 V) had to be used to elicit contractions; therefore, further research should be made for a more specific and more powerful stimulation technology. The effect of the generated contractions on the global transit time still remains to be assessed in chronic animal experiments. If successful, specific motility disorders could be treated by the means of a fully implantable device.
References
Aellen, S., P. Wiesel, J.-P. Gardaz, V. Schlageter, M. Berstchi, N. Virag, and J.-C. Givel. Electrical stimulation induces propagated colonic contractions in an experimental model. Br. J. Surg. 96:214–220, 2009.
Amaris, M. A., P. Z. Rashev, M. P. Mintchev, and K. L. Bowes. Microprocessor controlled movement of solid colonic content using sequential neural electrical stimulation. Gut 50:475–479, 2002.
Bruninga, K., L. Riedy, A. Keshavarzian, and J. Walter. The effect of electrical stimulation on colonic transit following spinal cord injury in cats. Spinal Cord 36:847–853, 1998.
Hughes, S. F., S. M. Scott, M.-A. Pilot, and N. S. Williams. Electrically stimulated colonic reservoir for total anorectal reconstruction. Br. J. Surg. 82:1321–1326, 1995.
Lammers, W. J. E. P., S. Dhanasekaran, J. R. Slack, and B. Stephen. Two dimensional high-resolution motility mapping in the isolated feline duodenum: Methodology and initial results. Neurogastroenterol. Mot. 13:309–323, 2001.
Lin, X., J. Hayes, L. J. Peters, and J. D. Z. Chen. Entrainment of intestinal slow waves with electrical stimulation using intraluminal electrodes. Ann. Biomed. Eng. 28:582–587, 2000.
Lin, Z. Y., R. W. McCallum, B. D. Schirmer, and J. D. Z. Chen. Effect of pacing parameters on entrainment of gastric slow waves in patients with gastroparesis. Am. J. Physiol. 274:G186–G191, 1998.
Maw, A., M.-A. Pilot, M. R. Hutton, A. J. P. Eccersley, A. Basu, M. Scott, and N. S. Williams. The effect of direct electrical stimulation on the intact colon. Br. J. Surg. 85(Suppl 1):14, 1998.
Mintchev, M. P., C. P. Sanmiguel, M. Amaris, and K. L. Bowes. Microprocessor-controlled movement of solid gastric content using sequential neural electrical stimulation. Gastroenterology 118:258–263, 2000.
Mosse, C. A., T. N. Mills, M. N. Appleyard, S. S. Kadirkamanathan, and C. P. Swain. Electrical stimulation for propelling endoscopes. Gastrointest. Endosc. 54:79–83, 2001.
Sanmiguel, C. P., S. Casillas, A. Senagore, M. P. Mintchev, and E. E. Soffer. Neural gastrointestinal electrical stimulation enhances colonic motility in a chronic canine model of delayed colonic transit. Neurogastroenterol. Motil. 18:647–653, 2006.
Schlageter, V., P. Drljaca, R. S. Popovic, and P. Kucera. A magnetic tracking system based on highly sensitive integrated Hall sensors. JSME Int. J. Ser. C 45:967–973, 2002.
Sevcencu, C., N. J. M. Rijkhoff, H. Gregersen, and T. Sinkjaer. Electrical stimulation to induce propulsive contractions in the porcine descending colon. Artif. Organs 29:246–249, 2005.
Acknowledgments
This study was made possible by grants from the Swiss Governmental Commission of Innovative Technologies (CTI) and Medtronic Europe. Authors would like to thank Marco Burki for his participation in the animal experiments and Prof. J.-P. Gardaz for his participation in the animal experiments and his assistance in writing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Sean S. Kohles oversaw the review of this article.
Nicolas Peloponissios is deceased.
Rights and permissions
About this article
Cite this article
Bertschi, M., Schlageter, V., Vesin, JM. et al. Direct Electrical Stimulation Using a Battery-Operated Device for Induction and Modulation of Colonic Contractions in Pigs. Ann Biomed Eng 38, 2398–2405 (2010). https://doi.org/10.1007/s10439-010-9985-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-010-9985-6