
Abstract
The purpose of this study was to document head and neck loading in a group of ordinary people engaged in non-injurious everyday and more vigorous physical activities. Twenty (20) volunteers that were representative of the general population were subjected to seven test scenarios: a soccer ball impact to the forehead, a self-imposed hand strike to the forehead, vigorous head shaking, plopping down in a chair, jumping off a step, a seated drop onto the buttocks, and a vertical drop while seated supine in a chair. Some scenarios involved prescribed and well-controlled stimuli, while others allowed the volunteers to perform common activities at a self-selected level of intensity. Head accelerations up to 31 g and 2888 rad/s2 and neck loads up to 268 N in posterior shear, 526 N in compression, and 36 Nm in extension were recorded. Most head and neck injury criteria predicted a low risk of injury in all activities. However, rotational head accelerations and Neck Injury Criterion (NIC) values were much higher than some proposed tolerance limits in a large number of tests, all of which were non-injurious. The data from this study help us to establish an envelope of head and neck loading that is commonly encountered and presents a minimal risk of injury.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Injuries occur along a continuum of severity, with minor injuries occurring at a rate far higher than moderate or serious injuries. At the low end of the injury severity continuum, defining what constitutes an injury is not straightforward. Diagnoses of minor head and neck injury rely on the subjective reporting of symptoms. The presence of pain or other symptoms does not necessarily indicate tissue damage.6 Furthermore, psychosocial factors play a role in how symptoms are reported and attributed to particular events.5–7 The relative importance of physical trauma vs. psychosocial factors in the etiology of symptoms can be elucidated by evaluating the biomechanical loading associated with a particular event.
The biomechanics of head and neck injury have been studied extensively. Well-accepted injury criteria, risk curves, and tolerance values exist to assess the potential for serious head and neck injury.16,17 However, the prediction of minor head and neck injury is more problematic. Widely divergent theories exist as to the biomechanical mechanisms and tolerance values for minor injury of both the head and neck. These theories are not mutually exclusive, so injury potential is often evaluated using several different injury criteria. For the purpose of this article, several more commonly used head and neck injury criteria were studied in the context of daily vigorous activities performed by ordinary people. The potential for mild traumatic brain injury (mTBI), or concussion, was predicted from the evalutions of the peak resultant acceleration of the head center of gravity, the Head Injury Criterion (HIC), the peak rotational head acceleration, and the peak rotational head velocity. The potential for whiplash injury of the neck was evaluated using the Neck Injury Criterion (NIC), upper neck loads and moments, and N ij and N km, which are based on combinations of the upper neck loads and moments.
The aim of this study was to determine the biomechanical loading of the head and neck encountered by ordinary human volunteers performing everyday and vigorous activities. These data serve three purposes. First, they establish an envelope of head and neck loading, which is commonly encountered and presents a minimal risk of injury to ordinary people. Second, the data allow a partial assessment to be made of the accuracy of the injury criteria studied. Each of the above injury criteria purports to be biomechanically based, and therefore should also be able to accurately predict the presence or absence of injury in a variety of loading scenarios. Third, the data provide a basis for comparing the injury potential of unusual or unfamiliar events to more common activities using several biomechanical parameters.
Methods
The study methodology has been described in previous articles.11,12,15 Twenty (20) human volunteer subjects participated in the study, all of whom were employees of Biodynamic Research Corporation. Volunteers were selected to obtain a representative sample of the general population, and included twelve (12) men and eight (8) women spanning a wide range of ages (26–58 years, mean 44 years), heights (150–191 cm, mean 172 cm), and weights (54–99 kg, mean 80 kg). By body mass index (BMI), six (6) subjects were normal (BMI = 20.6–24.7), ten (10) subjects were overweight (BMI = 25.0–29.6), and four (4) subjects were obese (BMI = 30.1–35.6). Plain film lateral lumbar, cervical, and head X-rays were taken of each subject to rule out substantial bony pathology. Spinal degeneration was not a cause for exclusion from the study, but the degree of spinal degeneration in each subject was assessed by a board-certified radiologist based on disc space narrowing, endplate sclerosis, facet joint arthrosis, and osteophytosis. The cervical spine films were normal in five (5) subjects and showed evidence of mild degeneration in nine (9) subjects and moderate degeneration in six (6) subjects.
Written consent was obtained from each participant, and the study protocol was approved for human use by both an internal Research Review Board and an external Institutional Review Board (IRB). The study protocol involved seven test scenarios, four of which involved progressively increasing levels of intensity. Participants were free to abstain from any test for any reason, and many did. All tests for a particular scenario were completed at one time, and different test scenarios were spaced at least 1 week apart. Subjects reported any symptoms related to testing to a physician (CEB).
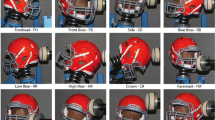
The seven test scenarios included two head impact scenarios: a soccer ball impact to the forehead and a self-imposed hand strike to the forehead (head strike). The five other test scenarios were vigorous head shaking, plopping down in a rigid chair, a vertical drop while seated supine in a chair (chair tip), a vertical drop onto the buttocks while seated upright in a swing (seated drop), and jumping off a step. All the scenarios involved loading in the sagittal plane without significant off-axis components (Fig. 1).

Video capture of a (a) soccer ball impact, (b) self-imposed hand strike to the forehead, (c) chair tip, (d) chair plop, (e) vigorous head shake, (f) seated drop, and (g) jump off a step
For the soccer ball impacts, participants stood in front of a custom-made apparatus that was aligned to shoot a regulation adult size 5 soccer ball inflated to 55 kPa horizontally such that it struck the subjects in the forehead. Up to four tests were conducted on each subject at increasing ball speeds: one low speed impact at 5 m/s, and three moderate speed impacts at 8.5, 10, and 11.5 m/s. The participants remained stationary and did not attempt to actively head the soccer ball. In fact, the ball was released and struck the subjects’ foreheads before they had a chance to react. For the self-imposed hand strikes, subjects were asked to strike themselves in the forehead with the heel of their hand as hard as they were willing to do it. Three trials were conducted for each subject.
In the voluntary head shaking scenario, subjects were asked to shake their head back and forth in the sagittal plane as vigorously as they could. One trial of 5–10 head shakes in rapid succession was conducted for each volunteer. In the chair plop scenario, subjects were asked to aggressively sit down on a rigid chair. Three trials were conducted for each subject. In the chair tip scenario, subjects were reclined almost 90° in a rigid chair that was dropped from successively increasing heights of 5, 10, and 15 cm measured to the mid-back. There was no head or upper back support, and so the subjects had to tense their neck muscles to hold their head up against gravity. A padded headrest was placed on the chair to protect against hyperextension of the neck during testing, but no contact between the head and headrest occurred in any of the tests. In the seated drop scenario, volunteers were seated upright in a swing and dropped onto a rigid platform from progressively increasing heights of 5, 7.5, and 10 cm. In the jump scenario, the test subjects jumped off steps from increasing heights of 30, 60, and 90 cm.
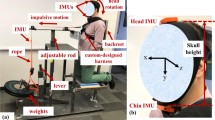
Test subjects were instrumented with tri-axial accelerometers (Endevco 7596, 30 g) attached to custom-fit mounts that were securely strapped around the lumbar and upper thoracic regions.15 Bite blocks made from dental impressions of each volunteer were instrumented with two accelerometers (Endevco 7265-HS, 20 g) and one angular rate sensor (ATA ARS-01 or DTS ARS1500k) (Fig. 2). For hygienic reasons, the instrumented bite block was wrapped in a thin plastic bag before being placed in the subjects’ mouths. Instrumentation data were collected using a TDAS-PRO 32-channel rack (DTS) at 10 kHz for the head impact scenarios, and 2 kHz for the other scenarios. All instrumentation data from human subjects were digitally filtered to 300 Hz (CFC180). High speed digital video (Phantom v7.1, Vision Research, Inc.) was recorded at 3 kHz for the head impact scenarios, and 1 kHz for the other scenarios. Image resolution for the soccer ball tests, which involved the most extensive video analysis, was 1.2 mm/pixel. Video data were analyzed by tracking various points using WINanalyze Tracking 3D Software, which is capable of subpixel accuracy (Mikromak, Inc.).

Example of X-ray and photograph overlay used to locate anatomical landmarks in the head coordinate frame in relation to the bite block instrumentation (inset)
Bite block accelerations were transformed using standard rigid body dynamics equations to determine the acceleration at the center of gravity of the head and the occipital condyles. These locations were identified from anatomical landmarks that were located precisely on scaled images in which lateral head X-rays and photographs of each volunteer were superimposed (Fig. 2). The coordinate system of the head was defined using the top of the external auditory meatus (in X-rays) or the tragus (in photographs) as the origin. The x-axis pointed anteriorly through the inferior orbital rim along the Frankfort plane. The z-axis pointed inferiorly, perpendicular to the Frankfort plane, and the y-axis pointed to the right with its origin at the midline, in accordance with the Society of Automotive Engineers sign convention. The sign of the upper neck forces was defined by the direction of the force applied below the neck. Therefore, rearward head motion relative to the torso resulted in a positive x-axis shear force, neck tension corresponded to a positive z-axis axial force, and neck flexion resulted in a positive y-axis bending moment. The location of the center of gravity of the head in all the volunteers was assumed to be 8.4 mm anterior and 31 mm superior to the origin of the head coordinate system, which is the mean value for a 50th percentile male.25 The location of the occipital condyles was identified radiographically for each volunteer, and ranged from 8 to 22 mm (mean 13 mm) posterior, and from 49 to 66 mm (mean 58 mm) inferior to the estimated location of the head center of gravity.
The effective eccentricity of the force vector applied to the head was assessed based on the ratio of the peak translational (a) and peak rotational (α) head acceleration. The peak force F was assumed to act over an effective eccentricity (e), defined as the perpendicular distance between the force vector and the center of gravity of the head. Balancing the moment about the head center of gravity yields the following relationship:
where (I) is the moment of inertia of the head, (m) is the mass of the head, and (k) is the radius of gyration of the head, which was assumed to be equal to 75 mm based on cadaver data.2,8 The effective time duration of the force pulse was estimated by dividing the peak rotational velocity of the head by the peak rotational acceleration and multiplying by two, consistent with a haversine or triangular pulse shape.
Sagittal plane loads and moments at the occipital condyles were calculated using standard inverse dynamics equations. The head mass of each volunteer was estimated using the regression equations of Clauser et al.,8 and ranged from 4.3 to 5.5 kg (mean 5.0 kg). The sagittal plane moment of inertia for the head was estimated from the head mass using the data from Beier et al.,2 and ranged from 217 to 327 kg cm2 (mean 279 kg cm2). In the case of soccer ball impacts, video analysis was used to calculate the force applied to the head by the ball. No attempt was made to calculate the force applied to the head by the hand in the voluntary hand strike tests, although the approach velocity of the hand was measured from video. The calculated occipital condyle forces and moments were digitally filtered to 50 Hz (CFC30). The entire approach was validated by performing matched soccer ball impact tests on the Hybrid III dummy and comparing calculated head accelerations and neck loads to experimental measurements.12
Several head and neck injury criteria were calculated. The Head Injury Criterion (HIC) was calculated as
where t 1 and t 2 are the initial and final times in seconds that maximize the HIC value and a(t) is the resultant acceleration at the center of gravity of the head expressed in the dimensionless unit of gravities (g).17 The maximum HIC interval (t 2 − t 1) was limited to 15 ms (HIC15). N ij was given by
where F zc is the critical axial force value equal to 6806 N in tension or 6160 N in compression, and M yc is the critical moment value equal to 310 Nm in flexion and 135 Nm in extension, in accordance with the current U.S. standard for a Hybrid III 50th percentile male dummy.17 N km was calculated according to the formula:
where F int is the intercept shear force value equal to 845 N, and M int is the intercept moment value equal to 88.1 Nm in flexion and 47.5 Nm in extension.24 For test scenarios in which the head was forced rearward with respect to the torso (all tests except the jump and seated drop scenarios), the Neck Injury Criterion (NIC) was calculated based on the relative rearward acceleration (a rel) and velocity (v rel) of the occipital condyles relative to the first thoracic vertebrae (T1) in the A–P direction (x-axis)3:
Tests in which proposed minor head and neck injury criteria were exceeded were noted. A rotational head acceleration of 1800 rad/s2 has been suggested as a tolerance value representing a 50% risk of concussion.20 In addition, a NIC of 15 has been proposed as an injury threshold.3 According to risk curves developed by Kullgren et al.,14 a NIC of 15 represents approximately an 18% risk of long-term (>1 month) minor neck injury, and an N km of 0.4 represents about a 5% risk of such an injury. The accuracy of these proposed risk curves was evaluated in two ways. First, the number of test subjects expected to sustain neck injury (E inj) was calculated by summing the probability of injury p associated with the highest NIC and N km value recorded for each subject i:
Second, the probability that no subject in the cohort would sustain a long-term (>1 month) minor neck injury was also calculated:
Results
A total of 341 human subject tests were conducted under the seven scenarios studied. The seven different test scenarios produced a wide variety of head acceleration and neck loading profiles (Tables 1 and 2). The scenarios that involved a direct head impact generated much higher head accelerations than the scenarios in which the head was loaded exclusively by the neck (Fig. 3). Peak translational head accelerations up to 18 g and 31 g were recorded in the head strike and soccer ball tests, respectively. With the exception of one data point for a chair plop test, all the subjects experienced peak resultant head acceleration less than 10 g in tests not involving a head impact. The maximum Head Injury Criterion (HIC) value calculated for any test was 10.

Peak translational and rotational head accelerations. Dotted lines represent various values for the effective eccentricity of the head force vector
Everyday activities resulted in rotational head velocities of up to 8 rad/s, with more vigorous activities producing rotational head velocities as high as 13 rad/s. The self-imposed hand strikes to the forehead delivered force vectors aimed very near the center of gravity of the head (eccentricity of only 10–15 mm), producing almost purely translational accelerations. Hand velocities ranged from 2.2 to 4.5 m/s just before striking the head in those tests. Soccer ball impacts delivered a glancing blow to the forehead (eccentricity of 50–75 mm) that created significant rotational head accelerations up to nearly 3000 rad/s2 (Fig. 4). Twelve (60%) subjects experienced peak rotational head acceleration greater than 1800 rad/s2. Assuming that 1800 rad/s2 represents a 50% risk of concussion, the odds of no concussions occurring among these 12 subjects can be conservatively estimated by raising one half to the twelfth power, which yields a probability of 1 in 4096.

Peak rotational head velocities and accelerations. Dotted lines represent various values for the effective duration of the head force pulse
The shortest effective rotational acceleration pulse durations occurred in the higher speed soccer ball tests (5–10 ms) (Fig. 4). Interestingly, the translational acceleration pulse durations were about 15–20 ms in these same tests, which was the time the soccer ball was visibly in contact with the head in the videos. The converse was observed in the head strikes, with the translational acceleration pulse durations being much shorter (5–10 ms) than the rotational acceleration pulse durations (10–50 ms). For the test scenarios with no head impact, the translational and rotational acceleration pulse durations were similar to each other and much longer than the head impact scenarios (20–100 ms).
Virtually every possible combination of sagittal plane neck loading was produced in this study (Figs. 5 and 6). The maximum upper neck loads calculated across all test scenarios were −260 N in anterior shear, 268 N in posterior shear, −526 N in compression, 29 Nm in flexion, and −36 Nm in extension (Table 2). The neck was generally loaded in compression (negative F z), posterior shear (positive F x), and extension (negative M y) in the soccer ball, head strike, chair plop, and chair tip tests. Compression, anterior shear, and flexion occurred in the jump and seated drop tests. Head shaking and some chair plops alternated between compression/anterior shear/flexion and tension/posterior shear/extension. In the soccer ball tests, only about 20% of the horizontal force applied to the head was transmitted to the neck as shear, with the remaining 80% being resisted by the inertia of the head. In contrast, the peak neck compression often exceeded the peak vertical force applied by the ball, presumably as a result of elastic rebound of the neck structures. In the remaining test scenarios without a head impact, the neck forces were directly proportional to the head accelerations in accordance with Newton’s second law.

Peak upper neck shear and axial forces in the predominant directions of loading

Average peak neck bending moments in flexion (+) and extension (−). Error bars indicate one standard deviation, and the box represents the entire range of values from minimum to maximum
Although relatively high upper neck forces and moments were generated in some tests, there was not any motion of the neck beyond its normal range. In the higher speed soccer ball tests, the head center of gravity typically moved only 10 mm during the time the ball was in contact with the head. There was likewise very little motion of the neck during the head strike tests, although voluntary neck extension sometimes occurred after the impact. The head shake tests produced the largest head displacements, which averaged only 86 mm and never exceeded 50° of flexion or extension. The chair tip tests required the subjects to actively tense their neck muscles before being dropped to hold their head up against gravity. During the drop, this active muscle tension caused the neck to flex. Upon landing, the neck remained flexed and did not extend enough even to return to a neutral orientation during any of the tests. Active muscle tension also limited the motions during the neck in the chair plop and jump tests. In the seated drop tests, the predominant loading mode was vertical, and so neck motion was minimal.
No subjects reported injury beyond minor short-term symptoms as a result of testing (Table 3). Almost all of these symptoms fell into one of two categories: head complaints related to soccer ball testing and neck complaints related to muscle soreness as a result of the head shaking or chair tip tests. The head shaking and chair tip tests were the only scenarios that required significant active neck muscle tension on the part of the study participants, and the subjects typically characterized their neck complaints after these tests as being due to muscle exertion or fatigue. No concussions, long-term neck injuries, or any other long-term injuries of any kind were reported. Injury criteria values were not significantly higher in the subjects who reported symptoms compared to the subjects who did not report symptoms in similar testing, although symptoms were more likely to be reported in activities involving higher head accelerations and neck loading. The distribution of ages, gender, and degree of spinal degeneration in the subjects reporting symptoms was nearly identical to the overall study population. A gender difference was observed only in the head strike and head shake tests, with nearly all biomechanical parameters being significantly higher (p < 0.05) in males compared to females. Age and body size had no effect on biomechanical measurements or symptom being reported in any of the test scenarios.
Nkm was highly correlated with N ij for all of the scenarios (R2 = 0.78) (Fig. 7). The Nkm value was approximately four times higher than the N ij value on average. In contrast, values for NIC, which is an acceleration-based criterion, were not at all correlated with the values of N ij (R2 = 0.08) or Nkm (R2 = 0.01) (Fig. 8). Furthermore, the relationship between NIC and Nkm varied by test scenario. In the soccer ball scenario, very high NIC values were often associated with very low values of N ij and Nkm. The head shaking scenario generated some moderately high values of Nkm, but only very low values for NIC.

Correlation between N ij and N km values (R 2 = 0.78)

Correlation between NIC and N km values (R 2 = 0.01)
The load-based neck injury criteria (N ij and N km) generally predicted a low risk of neck injury. The highest N ij value calculated for any test was 0.31 (Table 2). There was only one test in which the calculated N km exceeded 1. However, all the 20 subjects experienced an N km value greater than 0.4 at some point in the study. The highest N km values occurred in the chair tip, soccer ball, and head shake tests. According to the N km risk curves of Kullgren et al.,14 2 subjects were expected to have sustained long-term minor neck injury, and the odds of no subject sustaining any long-term neck injury was 8%.
The NIC, which is an acceleration-based injury criterion, predicted a high risk of neck injury in the soccer ball, head strike, and chair tip scenarios. The head impact and chair tip scenarios produced high NIC values in opposite ways. In the head impact scenarios, the head acceleration pulse was so short that almost no acceleration developed at T1 and very little relative velocity developed between the head and T1 before the peak head acceleration. The NIC (Eq. 5) in the head impact tests was therefore directly proportional to the rearward occipital condyle acceleration. In the chair tip tests, high NIC values developed because the x-axis T1 acceleration exceeded the lagging x-axis acceleration of the head and occipital condyles, as occurs in automotive rear impacts. NIC values greater than 15 were measured in 16 (80%) subjects during the study. The soccer ball tests generated NIC values as high as 30. The highest NIC value of 33 occurred during a self-imposed hand strike to the forehead. According to the NIC risk curves of Kullgren et al.,14 7 subjects were expected to have sustained long-term minor neck injury, and the probability of no subject sustaining any long-term neck injury was essentially zero.
Discussion
The primary purpose of this study was to establish an envelope of head and neck loading that is commonly encountered and presents a minimal risk of injury to ordinary people. Test scenarios were chosen to provide a variety of loading conditions. Some test scenarios could be classified as everyday activities, such as the head strike, head shake, chair plop, 30-cm jump, and seated drop tests. The soccer ball tests and the 60- and 90-cm jumps could be described as mildly athletic activities. The chair tip scenario is not commonly encountered in everyday life, but represented a controlled scenario with some similarities to an automotive rear impact. In the soccer ball, chair tip, jump, and seated drop tests, the loading was externally applied, and head accelerations and neck loads generally increased with increasing impact severity. In the head strike, head shake, and chair plop tests the loading was self-imposed and depended entirely on the amount of effort put forth by the subject. Perhaps unsurprisingly, men struck and shook their heads significantly harder than women. Otherwise, age, gender, body size, and degree of spinal degeneration had no effect on biomechanical parameters or symptom reporting.
The current study adds to previous research that has documented head accelerations and neck loads in various activities. Allen et al.1 measured head accelerations in a variety of everyday activities such as sneezing, coughing, hopping off a step, and plopping in a chair. Vijayakumar et al.28 and Ng et al.19 had volunteers perform mildly athletic activities, including walking, running, hopping, skipping rope, jumping jacks, falling into a chair, jumping off a step, and running with an abrupt stop. The data from the chair plop and jump tests reported here are in excellent agreement with these previous studies. Bussone et al.4 measured head accelerations of up to 26 g, 16 rad/s, and 1705 rad/s2 in children playing on playground equipment. These values are considerably higher than the head accelerations measured in this study for activities not involving a head impact, and the disparity may be related to differences in fall height and in the size between children and adults.
The highest head accelerations in this study occurred in the soccer ball tests. The purpose of these tests was not specifically to characterize the biomechanics of heading in soccer, but to biomechanically evaluate a head impact condition that is known to be non-injurious. The ball speeds utilized in this study were well within the normal range of speeds at which balls are headed in soccer games and practices.18 Subjects were able to tolerate head accelerations well over 20 g and 2000 rad/s2 without injury. These levels of rotational head acceleration greatly exceeded the value of 1800 rad/s2 proposed as a 50% risk of cerebral concussion by Ommaya and Hirsch.20 An elementary statistical analysis demonstrated that this proposed risk level cannot be accurate.
Other studies have documented far higher levels of non-injurious head acceleration in young male athletes. Football players,9,23 boxers,22 and rugby players10 routinely experience head accelerations exceeding 80 g and 6000 rad/s2 without injury. Statistical analysis of head impact data from football players13 and nonhuman primates27 suggests that head accelerations of 80 g and 6000 rad/s2 pose less than a 1% risk of concussion. This study increases the level of head acceleration that has been shown to be non-injurious to ordinary people, many of whom were decidedly non-athletic middle-aged men and women.
The other proposed injury criterion that was routinely exceeded without injury in the current study was the NIC. Sixteen subjects (80%) experienced NIC values exceeding the threshold of 15 m2/s2 proposed by Boström et al.3 in the soccer ball, head strike, or chair tip tests. Based on the NIC risk curve proposed by Kullgren et al.,14 7 subjects should have sustained long-term (>1 month) AIS 1 neck injury as a result of participating in this study. In actuality, none did. The odds of that outcome assuming an accurate risk curve were essentially zero. The logical conclusion is that the NIC risk curve presented by Kullgren et al.14 is not biomechanically accurate. This finding is bolstered by the previously referenced studies measuring head accelerations in athletes,9,22,23 which suggest that athletes in contact sports routinely experience NIC values far exceeding the values generated in this study without injury.
Interestingly, the NIC has been shown to be a good predictor of minor neck injury in the setting for which it was originally developed: automotive rear end collisions.14 However, this predictive power could be spurious, because in rear end collisions the NIC is correlated with other parameters that have been shown to be good predictors of injury independently, such as collision severity and neck loading.14 In the scenarios tested in the current study, the NIC was not correlated with neck loading, N ij , or N km (Fig. 8), and it was found that NIC did not perform well as an injury predictor independent of neck load. It is notable that there were no neck complaints at all as a result of the voluntary head strike tests in spite of the fact that the highest NIC values were recorded in that scenario. Neck complaints were more common after scenarios involving higher levels of upper neck shear force and bending moment.
The validity of the neck injury criteria studied must be evaluated in the context of their intended use. The NIC is based on the theory that long-term minor neck injury is caused by damage to cervical nerve roots due to a “water hammer” effect from hydrodynamic pressure change in the spinal canal during the retraction phase of a rear impact.3 The finding that the NIC is a poor predictor of injury in non-automotive situations casts doubt on its biomechanical validity. The N ij was developed to predict serious rather than minor neck injury, specifically injury to the anterior longitudinal ligament at the junction of the skull and upper neck due to combined tension and extension loading in out-of-position airbag testing.16 It is therefore not surprising that N ij values were low in this study. N km is meant to predict long-term minor neck injury in automotive rear impacts, which is caused by stretching of the facet joints due to shear.24 Several test scenarios in this study induced neck loading that was similar to a low speed (<10 km/h delta-V) automotive rear impact in both magnitude and direction.21,26,28 The rate of symptom reporting in the current study was also similar to the rate of symptom reporting in low speed rear impact tests with comparable neck loading. N km appeared to be a good candidate for predicting neck complaints in this study. However, the N km risk curve proposed by Kullgren et al.14 substantially overpredicted the incidence of injury. More research is needed to establish appropriate N km tolerance values. The data presented here provide a useful comparison to activities that are non-injurious to ordinary people.
References
Allen, M. E., I. Weir-Jones, D. R. Motiuk, K. R. Flewin, R. D. Goring, R. Kobetitch, and A. Broadhurst. Acceleration perturbations of daily living: a comparison to “whiplash”. Spine 19(11):1285–1290, 1994.
Beier, G., E. Schuller, M. Schuck, C. L. Ewing, E. D. Becker, and D. J. Thomas. Center of gravity and moments of inertia of human heads. In: Proc. International IRCOBI Conf., 1980, pp. 218–228.
Boström, O., M. Y. Svensson, B. Aldman, H. A. Hansson, Y. Håland, P. Lövsund, T. Seeman, A. Suneson, A. Säljö, and T. Örtengren. A new neck injury criterion candidate—based on injury findings in the cervical spinal ganglia after experimental neck extension trauma. In: Proc. International IRCOBI Conf., 1996, pp. 123–136.
Bussone, W. R., T. L. A. Moore, D. Richards, R. T. Bove, I. Scher, and M. T. Prange. Measurements of non-injurious head accelerations of a pediatric population. Society of Automotive Engineers. Paper 2009-01-0383, 2009.
Carragee, E., T. Alamin, I. Chang, T. Franklin, and E. Hurwitz. Does minor trauma cause serious low back illness? Spine 31(25):2942–2949, 2006.
Carver, A. XIV: pain. In: ACP Medicine, edited by E. G. Nabel. BC Decker, Inc., 2009, Neuro XIV Pain-1, p. 11.
Castro, W. H., S. J. Meyer, M. E. R. Becke, C. G. Nentwig, M. F. Hein, B. I. Ercan, S. Thomann, U. Wessels, and A. E. Du Chesne. No stress—no whiplash? Prevalence of “whiplash” symptoms following exposure to a placebo rear-end collision. Int. J. Legal Med. 114(6):316–322, 2001.
Clauser, C. E., J. T. McConville, and J. W. Young. Weight, volume, and center of mass of segments of the human body. Wright-patterson AFB, Air Force Systems Command, AMRL-TR-69-70, 1969, pp. 1–100.
Duma, S. M., S. J. Manoogian, W. R. Bussone, P. G. Brolinson, M. W. Goforth, J. J. Donnenworth, R. M. Greenwald, J. J. Chu, and J. J. Crisco. Analysis of real-time head accelerations in collegiate football players. Clin. J. Sports Med. 15(1):3–8, 2005.
Fréchède, B., and A. S. McIntosh. Numerical reconstructions of real-life concussive football impacts. Med. Sci. Sports Exer. 41(2):390–398, 2009.
Funk, J. R., J. M. Cormier, C. E. Bain, H. Guzman, and E. Bonugli. An evaluation of various neck injury criteria in vigorous activities. In: Proc. International IRCOBI Conf., 2007, pp. 233–248.
Funk J. R., J. M. Cormier, C. E. Bain, H. Guzman, and E. Bonugli. Validation and application of a methodology to calculate head accelerations and neck loading in soccer ball impacts. Society of Automotive Engineers. Paper 2009-01-0251, 2009.
Funk, J. R., S. M. Duma, S. J. Manoogian, and S. Rowson. Biomechanical risk estimates for mild traumatic brain injury. Proc. Assoc. Adv. Automot. Med. 51:343–361, 2007.
Kullgren, A., L. Eriksson, O. Bostrom, and M. Krafft. Validation of neck injury criteria using reconstructed real-life rear-end crashes with recorded crash pulses. In: Proc. 18th Enhanced Safety of Vehicles Conf. Paper 344, 2003.
Manoogian, S. J., J. R. Funk, J. M. Cormier, C. E. Bain, H. Guzman, and E. Bonugli. Evaluation of Thoracic and Lumbar Accelerations of Volunteers in Vertical and Horizontal Loading Scenarios. Society of Automotive Engineers, Paper 2010-01-0146, 2010.
Mertz, H. J., and P. Prasad. Improved neck injury risk curves for tension and extension moment measurements of crash dummies. In: Proc. 44th Stapp Car Crash Conf. Paper 2000-01-SC05, 2000.
National Highway Traffic Safety Administration. 49 CFR Ch. V Part 571—Federal Motor Vehicle Safety Standards (Standard No. 208 Occupant Crash Protection). §571.208, S6.6(a). Washington, DC: U.S. Government Printing Office, 2004, pp. 520.
Naunheim, R. S., J. Standeven, C. Richter, and L. M. Lewis. Comparison of impact data in hockey, football, and soccer. J. Trauma 48(5):938–941, 2000.
Ng, T. P., W. R. Bussone, and S. M. Duma. The effect of gender and body size on linear accelerations of the head observed during daily activities. Biomed. Sci. Instrum. 42:25–30, 2006.
Ommaya, A. K., and A. E. Hirsch. Tolerances for cerebral concussion from head impact and whiplash in primates. J. Biomech. 4:13–21, 1971.
Ono, K., K. Kaneoka, A. Wittek, and J. Kajzer. Cervical injury mechanism based on the analysis of human cervical vertebral motion and head-neck-torso kinematics during low speed rear impacts. In: Proc. 41st Stapp Car Crash Conf. Paper 973340, 1997, pp. 339–356.
Pincemaille, Y., X. Trosseille, P. Mack, C. Tarriere, F. Breton, and B. Renault. Some new data related to human tolerance obtained from volunteer boxers. In: Proc. 33rd Stapp Car Crash Conf. Paper 892435, 1989, pp. 177–190.
Rowson, S., G. Brolinson, M. Goforth, D. Dietter, and S. Duma. Linear and angular head acceleration measurements in collegiate football. J. Biomech. Eng. 131:061016-1-7, 2009.
Schmitt, K.-U., M. H. Muser, and P. Niederer. A new neck injury criterion candidate for rear-end collisions taking into account shear forces and bending moments. In: Proc. 17th Enhanced Safety of Vehicles Conf. Paper 124, 2001.
Schneider, L. W., D. H. Robbins, M. A. Pflug, and R. G. Snyder. Anthropometry of Motor Vehicle Occupants. Washington, DC: National Highway Traffic Safety Administration, UMTRI-83-53-1, 1983.
van den Kroonenberg, A., M. Philippens, H. Cappon, J. Wismans, W. Hell, and K. Langwieder. Human head-neck response during low-speed rear end impacts. In: Proc. 42nd Stapp Car Crash Conf. Paper 983158, 1998, pp. 207–221.
van der Vorst, M. V., K. Ono, P. Chan, and J. Stuhmiller. Correlates to traumatic brain injury in nonhuman primates. J. Trauma 62(1):199–206, 2007.
Vijayakumar, V., I. Scher, D. C. Gloeckner, J. Pierce, R. Bove, D. Young, and R. Cargill. Head kinematics and upper neck loading during simulated low-speed rear-end collisions: a comparison with vigorous activities of daily living. Society of Automotive Engineers. Paper 2006-01-0247, 2006, pp. 49–60.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Stefan Duma oversaw the review of this article.
Rights and permissions
About this article
Cite this article
Funk, J.R., Cormier, J.M., Bain, C.E. et al. Head and Neck Loading in Everyday and Vigorous Activities. Ann Biomed Eng 39, 766–776 (2011). https://doi.org/10.1007/s10439-010-0183-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-010-0183-3