
Abstract
In this paper we used high-resolution thermal imaging to visualize the human whole body anterior cutaneous temperature (T c) variations in well-trained runners during graded exercise. Fifteen male volunteers underwent a graded treadmill test until reaching their individual maximal heart rate. Total body T c decreased as the subjects started the exercise. Thighs and forearms exhibited the earliest response. A further T c diminution occurred with the progress of the exercise. At the exercise interruption, T c values were in average 3–5 °C lower than at baseline. T c increased during recovery from exercise. Forearms and thighs exhibited the earliest increase, followed by total body T c increase. Thermal imaging documented the presence of hyperthermal spots (occasionally tree-shaped) due to the presence of muscle perforator vessels during baseline and recovery, but not during exercise. The results we report indicate that thermal infrared imaging permits the quantitative evaluation of specific cutaneous whole body thermal adaptations which occur during and after graded physical activity. Thus providing the basis for evaluating local and systemic cutaneous blood flow adaptation as a function of specific type, intensity and duration of exercise, and helping to determine the ideal conditions (in terms of environment and apparel) in which physical activities should be conducted in order to favor thermal regulatory processes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The thermo-regulatory system of the human body maintains a constant temperature against a wide range of environmental and/or physical work conditions. The control of heat transfer with the environment plays a fundamental role for body temperature regulation. At the human/environment interface (skin), heat is carried away from the body by conduction, convection, radiation and evaporation. A general energy-balance equation determines the thermal state of the body2:
where S is the rate of energy level of the body, H the rate of internal energy production, W the rate of mechanical work produced during exercise, E the rate of energy loss by evaporation, R the rate of energy exchanged by radiation, and C the rate of energy exchanged by conduction and convection.
Intense exercise activates body compensatory vasoregulation through reduction of blood flow in the splancnic region and tegumentary apparatus.9,10 During intense physical activity, core structures and muscle mass produce heat. Peripheral vasodilatation enables massive transfer of “warmer” blood from the body core to the surface, where the above-cited processes regulate heat exchange. Muscular blood flow increases, while the total volume of muscular blood remains almost unvaried because of the reduced vascular compliance in this district. The blood volume within the core region and cutaneous layers decreases, thus increasing the venous return and the cardiac output.9,10
Johnson9 and Kenney and Johnson10 found that the modification of cutaneous blood flow during exercise depends on the individual grade of vasodilatation and vasoconstriction. The cutaneous blood flow also influences the cutaneous temperature (T c). Therefore, T c variations depending on exercise-induced modification of cutaneous blood flow may occur as well.18
Moreover, both C and R directly depend on T c.2 Therefore, monitoring T c provides useful information concerning thermolysis modalities and peripheral vasoregulation during exercise. Usually, T c is estimated by averaging values of the cutaneous temperature recorded in predetermined regions of interest (ROI) through contact temperature probes.14 A more accurate method for estimating the overall T c distribution and its variation during exercise would provide important information for improving athletic performance. This can be achieved by using modern touch-less high-resolution thermal imaging devices, which quantitatively and precisely map the cutaneous temperature distribution and its time evolution.6,7,11–13,17,18 These digital devices are capable of precisely measuring and storing real-time thermal images with a resolution of up to 512 × 512 pixels. The major characteristics of these Focal Plane Array based thermal cameras are high temperature sensitivity (i.e., the capability of discriminating in ideal conditions temperature differences as low as 0.01 °C), high sampling frequency (up to 100 non-interlaced images per second), and high spatial resolution (up to 1 mrad per sensor). Although extensively used for diagnostic purposes, these devices have been rarely used to investigate the variation of T c during exercise.7,17,18 We investigated T c distribution and variations associated with graded exercise in well-trained athletes using high-resolution thermal imaging.
Materials and Methods
Fifteen male runners (who regularly trained for at least four sessions per week, 2 h per session) were randomly selected from a list of volunteers of the Sport Center of the University of Chieti-Pescara. Their mean age, weight, and height were 25.2 ± 3.1 years, 71.4 ± 4.2 kg, and 1.75 ± 0.15 m, respectively. All participants were non-smokers, with no overt history of cardiovascular or pulmonary disease. They presented normal ECG and arterial blood pressure at rest. Subjects had not assumed drugs or medications with a potential impact on cardiovascular or thermo-regulatory functions during the two months prior to enrolment.
The Ethical Committee of the University of Chieti-Pescara School of Medicine approved this study. After having received a thorough explanation of the protocol, the subjects provided their informed written consent prior to their participation.
Subjects observed the standard preparatory protocol for thermal imaging measurements.12 That is, subjects shaved or otherwise removed body hair 5–6 days before the measurements in order to obtain the most accurate thermal imaging. They cleaned their skin from lotions and other cosmetic products before initiating the measurements. They abstained from smoking and assuming alcoholic or caffeine-containing beverages for a 4-h period prior to the evaluation. Upon arrival they undressed and electrodes were placed for heart rate (HR) monitoring.
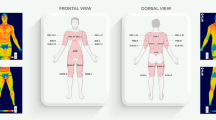
The physical locations for the user defined ROIs were based on the classical definition of body regions. The anterior body regions of the antebrachial (forearm) region, the trunk [included the pectoral, mammary, sternal and abdominal (abdomen) regions] and the thigh. Subject preparation involved positioning thermal-neutral indicators (adhesive paper markers) on specific points on the body (reperee points or landmarks of surface anatomy) in order to more easily identify these regions. These landmarks included acromion, lesser supra-clavicular fossa, xiphoid notch, umbilicus, and anterior superior iliac spin for the trunk, medial and lateral epicondyles, radial styloid and overlap of the radial styloid with proximal wrist crease for the forearm and anterior superior iliac spine, inguinal ligament, and band of Rocher for the thigh.
The subjects acclimated to the climate-controlled thermal imaging room (temperature: 23–24 °C; relative humidity: 50 ± 5%; and no direct ventilation) during a 20-min waiting period. They were then positioned on a treadmill (TecaFitness, Ortona, Italy) and initiated the standardized graded exercise program (scheme reported on Table 1). All measurements were performed in the late morning in order to minimize possible effects due to circadian variations.1
Exercise interruption criteria were: subjects having reached their age-predicted maximal HR or voluntary interruption by the subject. At that end of the exercise program or immediately after the presentation of exercise interruption criteria, the treadmill speed was reduced to Stage 1 speed and maintained for a further two minutes “cool down”. Then the treadmill was completely stopped.
Heart rate was continuously monitored by means of a standard ECG device (PowerLab AD Instruments, Sidney, Australia). Heart rate recording started 1 min prior to initiation (baseline period) and continued until the complete restoration of baseline HR.
Thermal image series of the anterior surface of each subject’s entire body were obtained during exercise via a 14-bit digital infrared camera (FLIR SC3000 QWIP, Flir Systems, Danderyd, Sweden; 320 × 240 Focal Plane Array; 8–9 μm spectral range; 0.02 K Noise Equivalent Temperature Differences (NETD); 50 Hz sampling rate; and germanium lens f 20–f/1.5). The camera was set 4 m from the subject thus permitting the simultaneous acquisition of the three regions of interest (trunk, forearms, and thighs).
Digital thermal images were acquired every second. The regions of interest were identified in the first image of each series. This process was facilitated by the use of thermally neutral markers placed on surface anatomy landmarks. The image series was then corrected for movement and re-aligned using an edge-detection based algorithm.15 Specifically, a correlation-based method (CBM) was used which required the user to define a rectangular ROI containing the marker on the first image of a series. Within this larger ROI the user defines a second, smaller ROI (sub-ROI), which circumscribes the marker. The pixels of the ROI are scanned in a step-wise manner in order to calculate the correlation between the actual mask and the chosen one onto the template image. The actual mask position associated with the best correlation value is assumed to be the correct position, that is, the assumed position of the marker in a given image. The estimated actual positions of the markers provide the parameters for the affine transformation of the images. This method was reported to yield more accurate results, both in terms of Localization Error and Test Point Error, compared to other methods particularly when tracking over large thermal variations (up to 10× improvement), large motion (4× improvement) and larger ROIs (4× improvement). The affine transformed image series were used to determine T c variations for each ROI as a function of time. Then a 5-point mobile average algorithm was applied to the T c vs. time series in order to eliminate residual effects due to motion.
Results
None of the subjects voluntarily interrupted the exercise program and all reached their maximal HR: 5 during stage 6 and 10 during stage 7 (Table 2). Figure 1 reports a representative example of T c modifications during the different phases of exercise. In particular, thermal imaging documented the following features and modifications of the T c distribution:

Anterior view of the upper and lower body of a representative subject taken during a duplicate run without markers. Total body T c changes during graded exercise: (a, d) baseline T c distribution; (b, e) immediately after reaching the age-predicted maximal HR value; and (c, f) during recovery from exercise. The color bars report pseudo-colors associated with T c. The superior and inferior views are presented with different thermal scales in order to highlight regional contrast
-
1.
Overall, T c decreased in all three regions of interest after the start the exercise (stage 1; that is, warm-up phase). This reduction was faster and more pronounced in the most peripheral region (forearms) and far less pronounced in the central region (trunk).
-
2.
As the exercise progressed (from stage 2 to stage 6–7), a further T c diminution occurred. Total body T c values were 3–5 °C lower than at baseline. In addition, T c decreased on the cutaneous projection of muscle mass directly involved in running (see Fig. 1e). Total body T c presented hyperthermal spots on the baseline images which remained visible on the abdomen and trunk during exercise, but disappeared almost completely on the legs (Fig. 1).
-
3.
Tc increased during recovery. Peripheral regions (forearms and fingertips) exhibited the earliest Tc increases, while the other regions of interest exhibited a longer recovery time. The total body Tc distribution showed at first the presence of hyperthermal spots (occasionally tree-shaped) most likely due to the presence of muscle perforator vessels. Then, the distribution smoothed toward a uniform pattern (see Figs. 1c and 1f).
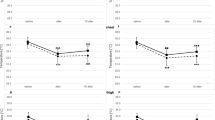
Thermal imaging and adequate data processing permitted quantitative evaluation of anterior whole body T c time-variation for defined regions of interest. For each region of interest, the mean absolute and percentage variation from baseline of T c time-profile were calculated for all subjects (Figs. 2 and 3, respectively).

Average T c values of regions of interest and total body vs. time for all subjects. The curves exhibit an initial descending phase with a minimum in correspondence to graded exercise interruption (approximately the 12th minute of exercise). Then, T c increases toward baseline values. All 15 subjects exhibited the same time-pattern. Note: the graph does not report the standard deviation (ranging from 0.1 to 0.2 °C) for each single measurement, in order to improve readability

Percentage variation from baseline of T c time-profile. The variations of the regions of interest are phase locked, but differ in amplitude
Discussion
Exercise is associated with large hemodynamic changes involving multiple regulatory processes. Since exercise causes heat generation within the body and invokes cutaneous thermo-regulatory processes, marked alterations in cutaneous temperature are expected during exercise. Blood circulation is fundamental for heat removal from deep regions of the body and heat transportation to cutaneous layers. During this compensatory mechanism, cutaneous blood flow can vary widely to provide heat dissipation or conservation, thus resulting in marked variations of T c.
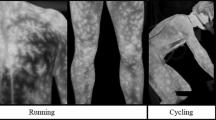
In the present study, we used high-resolution thermal imaging to monitor T c distribution variation during graded exercise in well-trained runners. In a previous study, Zontak et al.18 used dynamic infrared thermography to characterize the effect of exercise and recovery on the fingertip cutaneous temperature response. They showed that the dynamics of the cutaneous temperature response depended on the type of exercise (graded vs. constant load). During graded exercise, where the load on the body was constantly increasing, the temperature of the fingers continuously decreased throughout the exercise period. Thermal image series acquired in our study document that total body T c decreased in a similar manner throughout the exercise period. This indicated a continuous cutaneous vasoconstrictor response, attributable to an increase in catecholamine and other vasoconstrictor hormones released as the exercise intensity increases.4,17
Tc variation during exercise followed a specific pattern which was most likely due to the differences in the distribution of innervation and cutaneous/tissue vascularization between peripheral and central regions.16 In fact, the Tc of the most peripheral region of interest (forearms) decreased and recovered faster than the more central ones (thighs and trunk).
Prolonged intense exercise causes metabolic heat production, which if not re-distributed and eliminated will induce an excessive increase of muscular and core temperature. Heat removal is effectively performed shifting the blood from these districts to the cutaneous layer by activating vasoconstriction/vasodilatation mechanisms.9
Thermal images recorded during recovery from exercise showed that the cutaneous temperature at first increased in fingertips, forearms and face, a consequence of peripheral vasodilatation. Then, we observed an inhomogeneous cutaneous temperature increase for the entire body, the pattern of which highlights the presence of hyperthermal spots, which were often tree-shaped. These spots are indicative of the presence of muscle perforator vessels,3,14,17 the shape and density of which depends on the existence of different types of perforator vessels5,8; that is, Type I runs to the cutaneous surface, Type II is linked at the base and runs to the cutaneous surface, and Type III runs straight to the dermal surface and disperse parallel to the skin. The diffusion of heat from the hyperthermal spots to the surrounding cutaneous tissue suggests a possible hemodynamic and thermo-regulatory role for the perforator vessels during/after exercise.16
Heat transfer from the core to cutaneous tissue associated with blood flow causes an increment of the cutaneous temperature and, eventually, the onset of thermal dissipation processes, such as sweating. Thermal imaging can easily detect this onset.16 Therefore, the effects of sweating on the dynamics of cutaneous temperature throughout an exercise program can be studied as well.
Monitoring the topography and dynamics of anterior whole body cutaneous temperature changes during exercise provides useful information concerning temporal modifications of various thermolytic processes. Total body thermal imaging is currently the only method available for real time, touch-less non-invasive quantitative monitoring of cutaneous temperature, which can also be used during a wide range of exercise programs. The major limitation of this method is that the acquisitions are two-dimensional representation of a three-dimensional surface of a three-dimensional structure. Methodological improvements will be required to overcome this technical limitation. Ideally, acquisitions would provide a three-dimensional representation of the surface temperature of the entire three-dimensional structure using a single or a multiple camera system. This will require further improvements in both hardware and post-processing techniques.
In conclusion, the temperature of the entire anterior cutaneous surface of the body was monitored using thermal infrared imaging during graded exercise yielding a specific time evolution of cutaneous temperature modifications. The results of this study indicate that when performing graded exercise as a warm-up, the subject should not wear heavy clothing, thus favoring vasoconstriction of the cutaneous vessels increasing the blood flow to muscles.
Attempts to break world records in various disciplines has led to advances in various areas of research concerning the identification of specific environmental conditions and the development of hi-tech clothing, footwear and equipment in order to maximize performance or to guarantee the maximal comfort. The results we report provide the basis upon which subsequent studies can be designed and conducted to evaluate local and systemic cutaneous blood flow adaptation as a function of specific type, intensity and duration of exercise, thus determining the ideal conditions (in terms of environment and apparel) in which physical activities should be conducted in order to favor thermal regulatory processes. These subsequent studies should evaluate the role of direct ventilation, muscular warm-up and modifications of ambient temperature.
References
Aldemir, H., G. Atkinson, T. Cable, B. Edwards, J. Waterhouse, and T. Reilly. A comparison of the immediate effects of moderate exercise in the late morning and late afternoon on core temperature and cutaneous thermo-regulatory mechanisms. Chronobiol. Int. 17:197–207, 2000.
American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE). Handbook Fundamentals. Atlanta, GA: ASHRAE, 1985, pp. 1–24.
Binzoni, T., T. Leung, D. T. Delpy, M. A. Fauci, and D. Rufenacht. Mapping human skeletal muscle perforator vessels using a quantum well infrared photodetector (QWIP) might explain the variability of NIRS and LDF measurements. Phys. Med. Biol. 49(12):165–173, 2004.
Brengelmann, G. L., J. M. Johnson, L. Hermansen, and L. B. Rowell. Altered control of skin blood flow during exercise at high internal temperatures. J. Appl. Physiol. 43:790–794, 1977.
Chijiwa, T., K. Arai, N. Miyazaki, S. Igota, and N. Yamamoto. Making of a facial perforator map by thermography. Ann. Plast. Surg. 44(6):596–600, 2000.
Fauci, M. A., R. Breiter, W. Cski, W. Fick, R. Koch, J. Ziegler, and S. D. Gunapala. Medical Infrared Imaging—differentiating facts from fiction, and the impact of high precision quantum well infrared photodetectors camera systems, and other factors, in its reemergence. Infrared Phys. Technol. 42:337–344, 2001.
Ferreira, J. J. A., L. C. S. Mendonc, A. L. A. O. Nunes, A. C. C. Andrade Filho, J. R. Rebelatto, and T. F. Salvini. Exercise-associated thermographic changes in young and elderly subjects. Ann. Biomed. Eng. 36:1420–1427, 2008.
Itoh, Y., and K. Arai. Use of recovery-enhanced thermography to localize cutaneous perforators. Ann. Plast. Surg. 34(5):507–511, 1995.
Johnson, J. M. Exercise and the cutaneous circulation. Exercise Sport Sci. Rev. 20:59–97, 1992.
Kenney, W. L., and J. M. Johnson. Control of skin blood flow during exercise. Med. Sci. Sports Exerc. 24(3):303–312, 1992.
Merla, A., L. Di Donato, and G. L. Romani. Quantifying the relevance and stage of disease with the tau image technique. IEEE Eng. Med. Biol. 21:86–91, 2002.
Merla, A., and G. L. Romani. Functional infrared imaging in clinical applications. In: The Biomedical Engineering Handbook, edited by J. D. Bronzino. New York, NY: CRC Press, 2005, pp. 32.1–32.13.
Roganski, A. Infrared detectors: an overview. Infrared Phys. Technol. 43:187–210, 2002.
Rowell, L. B. Human cardiovascular adjustments to exercise and thermal stress. Physiol. Rev. 54:75–179, 1974.
Tangherlini, A., A. Merla, and G. L. Romani. Field-warp registration for biomedical high-resolution thermal infrared images. Conf. Proc. IEEE Eng. Med. Biol. Soc. 1:961–964, 2006.
Taylor, G. I., M. P. Gianoutsos, and S. F. Morris. The neurovascular territories of the skin and muscles: anatomic study and clinical implications. Plast. Reconstr. 94:1–36, 1994.
Vainer, B. G. FPA-based infrared thermography as applied to the study of cutaneous and stimulated vascular response in humans. Phys. Med. Biol. 50:R63–R94, 2005.
Zontak, A., S. Sideman, O. Verbitsky, and R. Beyar. Dynamic thermography: analysis of hand temperature during exercise. Ann. Biomed. Eng. 26:988–993, 1998.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Merla, A., Mattei, P.A., Di Donato, L. et al. Thermal Imaging of Cutaneous Temperature Modifications in Runners During Graded Exercise. Ann Biomed Eng 38, 158–163 (2010). https://doi.org/10.1007/s10439-009-9809-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-009-9809-8