
Abstract
Knowledge of the functional role of the nucleus pulposus is critical for the development and evaluation of disc treatment strategies to restore mechanical function. While previous motion segment studies have shown that nucleotomy alters disc mechanics, disruption of the annulus fibrosus may have influenced these experiments. The objective of this study was to determine the mechanical role of the nucleus pulposus in support of axial loads via a trans-endplate nucleotomy procedure. Sheep motion segments were randomly assigned to three groups: control, limited nucleotomy, and radical nucleotomy. Mechanical testing consisted of 20 cycles of compression–tension, a 1-h creep, and a slow constant-rate compressive ramp test. Nucleotomy led to increased axial deformations, in particular an elongated neutral zone, a greater range of motion, and altered creep behavior. In general, the elastic properties exhibited a graded response with respect to the amount of nucleus material removed. This graded effect can be attributed to swelling of the nucleus pulposus in the limited nucleotomy group, whereas little swelling was observed in the radical group. The findings of the present study indicate that functional evaluation of nucleus pulposus replacements and disc implants should include range of motion measures (including neutral zone) and viscoelastic creep experiments in addition to considering compressive stiffness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Mechanical function of the intervertebral disc is maintained through the interaction between the gel-like nucleus pulposus and the surrounding annulus fibrosus. The nucleus pulposus has a large swelling pressure due to its high proteoglycan content and the associated glycosaminoglycan fixed charge density. Spine axial compressive loads are partially supported by the nucleus pulposus,31,38 where deformation decreases the disc height, increases nucleus pulposus pressure, and transfers loads radially to the annulus fibrosus. Compressive loads are also supported directly by the annulus fibrosus:17,18,50 axial compression induces circumferential hoop tension, for which the fiber orientation of the annulus is uniquely designed. Loss of proteoglycan in the nucleus pulposus, a hallmark of disc degeneration, leads to altered mechanical behaviors such as decreased swelling pressure,22,45,52 decreased compressive modulus,22 and increased shear modulus.20 These altered nucleus pulposus mechanics may affect load sharing interactions between the annulus and the nucleus and ultimately contribute to progression of disc degeneration.51 In addition, disc treatment strategies that aim to restore mechanical function through nucleus pulposus prosthetics or tissue engineered constructs2,4 need to be developed and evaluated with particular attention given to nucleus and annulus mechanical interactions.
Cadaveric motion segment studies have shown that both limited and radical nucleotomy procedures alter disc mechanics. These changes include decreased pressure, decreased disc height, increased deformation and flexibility, and increased annulus bulging.6,15,21,29,42,46,49 However, the mechanical differences between limited and radical nucleotomy are not well established. Limited nucleotomy of a healthy disc is followed by swelling and redistribution of remaining tissue, which may restore mechanical behavior.6,23 In contrast, radical nucleotomy precludes tissue redistribution, thus leaving a void in the center of the disc. It was recently demonstrated that a limited nucleotomy acutely altered stress relaxation behavior but not axial compressive stiffness.23,24 However, subsequent cyclic loading and unloaded recovery restored mechanical behavior to intact values due to swelling and redistribution of the remaining nucleus tissue. Previous studies suggest that increases in disc deformations under load are related to the amount of nucleus material removed,6,15 while others have shown that depressurization, without large amounts of nucleus pulposus removed, has minimal effect on radial bulge.49 Interpreting the differences between limited and radical nucleotomy is further complicated because most studies are performed through an annulus fibrosus incision, which has been shown to alter disc mechanics in the absence of nucleus pulposus removal.3,7,39,49 Thus, despite years of investigation, the role of the nucleus pulposus, and its interaction with the annulus fibrosus, remains somewhat elusive.
The objective of this study was to explore the mechanical role of the nucleus pulposus in support of axial loads. This was achieved by measuring the compression–tension and creep behavior of cadaveric sheep motion segments after limited or radical nucleotomy was performed through the endplate, keeping the annulus fibrosus intact. Following testing, magnetic resonance and optical images of the motion segment were obtained to examine disc structure. We hypothesized that removal of the nucleus pulposus would not alter the compressive or tensile stiffness. However, we hypothesized that nucleotomy would result in increased range of motion, neutral zone displacement, and creep deformation. We further hypothesized that the magnitude of changes in the limited nucleotomy group would be intermediate between those of the control and radical nucleotomy groups.
MATERIALS AND METHODS
Specimen Preparation
Lumbar spines were harvested from 12 skeletally mature sheep spines. All musculature and soft tissue were dissected and the facets and transverse processes were removed. Two bone-disc-bone motion segments per spine (levels L1L2 and L4L5, n = 24) were made by making parallel cuts, normal to the axis of the spine, through the lumbar vertebrae. Motion segments were potted in polymethyl methacrylate bone cement while tissue hydration was maintained by covering specimens with saline-soaked gauze. Kirschner wires were placed through the bone cement and the vertebral bodies to increase the pull-out strength.
Samples were randomly divided into three groups: control (n = 8), limited nucleotomy (n = 8), and radical nucleotomy (n = 8). The limited and radical nucleotomy were achieved by making perforations (4.0 and 9.5 mm diameter, respectively) parallel to the longitudinal axis of the spine, through the superior vertebrae, endplate, and nucleus pulposus. A surgical curette was used to ensure that nucleus pulposus tissue was adequately removed from the large perforation in the radical group; surgical tools were not used in the limited nucleotomy group. The amount of nucleus pulposus removed by the limited and radical treatments was determined by calculating the ratio of the cross-sectional area of the perforation to the total area of the nucleus pulposus—approximately 10% in the limited nucleotomy group and 50% in the radical nucleotomy group. Calculations were performed using an average disc cross-sectional area of 393 ± 94 mm2 and average nucleus pulposus area of 138.5 ± 32.7 mm2. As shown in Fig. 1, the center of the nucleus pulposus is located posterior to the disc center. In all groups the annulus fibrosus remained structurally intact and this was confirmed following testing by imaging specimens either with MRI or photographs of sagittal bisections.

Axial cross-sections from representative (A) control, (B) limited nucleotomy, and (C) radical nucleotomy discs. “X” indicates the centroid of the whole disc and “O” indicates the centroid of the nucleus pulposus. The nucleus pulposus is located posterior to the center of the disc.
Mechanical Testing
Following sample preparation and nucleotomy, all samples were hydrated in a refrigerated 4°C phosphate buffered saline solution for 18 h prior to testing, effectively allowing any remaining nucleus pulposus to swell. The samples were placed in fixtures designed for axial compression and tension loading. Mechanical testing was conducted in a room temperature phosphate buffered saline bath using an Instron 8874 servohydraulic test frame. The testing protocol (Fig. 2) consisted of 20 sinusoidal cycles from −400 N compression to 300 N tension at 1 Hz. Cyclic loading was followed by a creep test consisting of a second step load from 0 N to −200 N compression and a 1 h hold, followed by a slow 1 N/s constant-rate compressive ramp test from 0 N to −200 N. The maximum cyclic compressive load of −400 N was chosen to represent approximately twice human body weight, scaled for differences in the cross-sectional area of the human and ovine intervertebral discs. According to data compiled by Elliott and Sarver,10 average cross-sectional area of the human intervertebral disc is approximately 1560 mm2 and the average cross-sectional area of the ovine discs used in this study was 393 mm2. Thus 400 N applied to the sheep disc corresponds to 1560 N in the human, or approximately twice body weight.

Mechanical testing protocol used to measure motion segment mechanics. Twenty cycles of compression–tension were followed by a 1-h creep and a 1 N/s ramp. Note. Time axis not to scale.
Data Analysis
The first 19 cycles of compression–tension loading were used as preconditioning to eliminate super-hydration.1 The 20th cycle of loading was chosen for data analysis based on previous work in the literature indicating that, in rodent motion segments, a minimum of 10–15 preconditioning cycles is necessary to produce a repeatable force displacement hysteresis response.10 Experimental findings from the present study indicate that 20 cycles of preconditioning were necessary to approach a steady state peak displacement (Fig. 3). Cyclic compression–tension data were analyzed as follows (Fig. 4): cyclic compressive stiffness (S comp) and cyclic tensile stiffness (S tens) were calculated by a linear regression of the load-displacement data between −300 and −400 N for compression and between 200 and 300 N for tension. Neutral zone length was determined as follows:44 a third-order polynomial equation was fit to the compression–tension load-displacement data and the derivative of the equation taken. The displacement at which the minimum derivative occurred was defined as the inflection between compression and tension. A line, having a slope equal to the derivative of the polynomial model, was extended through the inflection point and extrapolated to intercept with the compressive and tensile stiffness lines. The axial displacement between the compressive and the tensile intercepts with this line was taken as the neutral zone (NZ) displacement. Range of motion (ROM) was directly measured as the total peak-to-peak displacement. The constant-rate slow ramp compressive stiffness (S slow) was calculated by a linear regression of the slow ramp load-displacement response.

Representative cyclic load-displacement data indicating that steady state is achieved in 20 cycles.

Representative force-displacement data (points) with corresponding curve fits. S com and S ten represent the stiffness in the compression and tension zone, respectively, from a linear regression. The neutral zone is calculated from a polynomial fit of all data, determining the inflection point from the minimum derivative, and intersecting a line of this slope with the compression and tension curves.
Creep data were analyzed as follows: step displacement was defined as the change in displacement during the 1-s applied step load. Creep displacement (d) was defined as the change in displacement following the step load during the 1-h hold. The creep displacement divided by the applied load (L 0 = 200 N) was curve fit (Graphpad Prism 4.0) as, \(\frac{{d(t)}}{{L_0 }} = \frac{1}{{S_1 }}( {1 - e^{ - tS_1 /\eta _1 } }) + \frac{1}{{S_2 }}( {1 - e^{ - tS_2 /\eta _2 } }),\) where S 1 and S 2 are the elastic damping coefficients (N/mm) and η 1 and η 2 are the viscous damping coefficients (Ns/mm) for a four-parameter rheological model.29 Note that the time constant, τ, can easily be calculated as τ i = η i/S i. The creep displacement rate (d′) was calculated from the derivative of the creep displacement as \(\frac{{d\prime (t)}}{{L_0 }} = \frac{1}{{\eta _1 }}e^{ - tS_1 /\eta _1 } + \frac{1}{{\eta _2 }}e^{ - tS_2 /\eta _2 } .\)
Statistical comparisons were performed using a one-way ANOVA (significance set at p < 0.05) with Dunnett's post hoc test for multiple comparisons.
Imaging
To qualitatively evaluate potential structural differences between the limited and the radical nucleotomy group, magnetic resonance images (MRI) of intact discs and optical images of sagittally sectioned discs were acquired. Three randomly selected discs from each treatment group were imaged in a standard clinical MR scanner (Signa 1.5 T, Nilwaukee, WI) using a custom surface coil. Axial and sagittal plane images were acquired using a gradient echo pulse sequence (TR/TE = 100/3.7 ms, 2 mm slice thickness). The images were evaluated for distribution of nucleus pulposus. The samples were then partially frozen and bisected sagittally through the denucleated location using a diamond-bladed band saw. Before thawing, the bisected motion segments were held in a custom fixture, with a plexiglass face to maintain the disc structure and limit swelling.35 Anterior–posterior images were captured (Canon Powershot Pro90 IS) and qualitatively evaluated for the distribution of nucleus pulposus. Finally, two samples from each treatment group were sectioned in the mid-axial plane using a microtome blade. The motion segments were kept semi-frozen to prevent swelling. Images in the axial plane were acquired with a calibrated scale such that whole disc cross-sectional area and nucleus pulposus cross-sectional area could be calculated.40
RESULTS
Treated samples exhibited an elongated load-displacement response (Fig. 5) where the control motion segments had a much smaller neutral zone displacement that became increasingly larger in the limited and radical nucleotomy groups. The effect of nucleotomy on the biomechanical behavior of the disc was, in general, a graded response with respect to the amount of nucleus pulposus tissue removed—limited nucleotomy produced effects that were intermediate between the control and the radical nucleotomy groups (Fig. 6). The total range of motion (ROM) was 0.67 ± 0.23 mm for control, 1.06 ± 0.38 mm for limited nucleotomy (not significant), and 1.14 ± 0.34 mm (70% greater than control, p < 0.05) for radical nucleotomy [Fig. (6A)]. Neutral zone length was 0.22 ± 0.20 mm for control, 0.40 ± 0.28 mm for limited nucleotomy (not significant), and 0.55 ± 0.18 mm for radical nucleotomy (150% greater than control, p < 0.05) [Fig. (6A)].

Representative force-displacement curves from 20th cycle of compression–tension loading for each treatment group. The control motion segments had a much smaller neutral zone displacement that became increasingly larger in the limited and radical nucleotomy groups.

Mean and standard deviations for range of motion and neutral zone (A), compression and tensile stiffness (B), and viscous damping coefficients, η 1 and η 2 (C). *denotes a significant difference compared to the control.
In contrast to the deformation results described above, nucleotomy did not significantly affect the cyclic compressive or tensile stiffness at 1.0 Hz [Fig. (6B)]. Cyclic compressive stiffness, S comp, for control samples was 2418 N/mm and was not different at 2272 and 2127 N/mm for limited and radical nucleotomy, respectively. Cyclic tensile stiffness, S tens, for control samples was 724 N/mm and was not different at 823 and 697 N/mm for limited and radical nucleotomy, respectively. In contrast, the slow constant-rate compressive ramp stiffness, S slow (Fig. 7), was significantly decreased with nucleotomy treatment. The S slow for control samples was 1960 ± 285 N/mm, 1846 ± 388 N/mm in the limited nucleotomy group, and only 1470 ± 403 N/mm (25% less than control, p < 0.05) in the radical nucleotomy group.

Slow ramp load-displacement response.
The viscoelastic creep behavior was well described by the four-parameter exponential model (Fig. 8, average R 2 > 0.99 for all fits). Plots of creep displacement and creep rate, generated from average curve fit parameters from each treatment group, are shown in Fig. 9. The initial step displacement is subtracted from the figures so that the viscoelastic creep response could be better observed. The step displacement followed a graded response with a significantly larger step displacement for the radical nucleotomy group (Table 1). Similarly, the radical nucleotomy group exhibited a larger total creep deformation (Fig. 9 top, Table 1) and exhibited a more rapid creep rate early in the test (Fig. 9 bottom). The parameters, S 1 and η 1, reflecting the early creep response were significantly different in both the limited and the radical groups: η 1 in the limited nucleotomy group was 38% of control and 32% of control in the radical nucleotomy group (p < 0.05) [Fig. (6C)]; S 1 decreased significantly in both limited and radical nucleotomy groups (p < 0.05, Table 1). Parameters reflecting the late creep response, S 2 and η 2, showed fewer differences. η 2 was significantly different from control in the radical group; S 2 was not significantly different from control in either treatment group (Table 1).

Representative 1-h creep experimental data (points) and corresponding four-parameter viscoelastic curve fit (solid line).

Creep (top) and creep rate (bottom) plotted from mean curve-fit parameters.
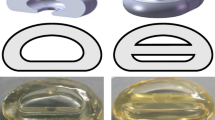
Magnetic resonance images show that the remaining tissue in the limited nucleotomy discs swelled to fill the void created by treatment (Fig. 10), whereas the remaining nucleus pulposus tissue in the radical nucleotomy group did not. MR results were confirmed by optical images taken from sagittally bisected discs (Fig. 10) and by manual palpation of the remaining nucleus pulposus in the limited nucleotomy group. Swelling of the remaining nucleus pulposus tissue was not evident in the radical nucleotomy group.

Sagittal MR images and corresponding photographs of bisected motion segments shown for control (top), limited nucleotomy (middle), and radical nucleotomy (bottom).
DISCUSSION
In this study, we found that trans-endplate nucleotomy did not alter cyclic compressive or tensile stiffness at 1.0 Hz, a finding that is consistent with previous studies.24,32,49,53 However, axial deformation and creep behavior were significantly affected by both limited and radical nucleotomy treatments. In particular, nucleotomy led to an increase in the low load neutral zone region, as demonstrated by neutral zone length and total range of motion. We showed that, in general, the effect of limited nucleotomy was intermediate between intact and radical nucleotomy. This “graded” effect (Figs. 6 and 9) can be attributed to swelling and redistribution of the remaining nucleus pulposus tissue to fill the void created by nucleotomy, as observed on MR and optical images. Although the nucleus pulposus may have been depressurized by the nucleotomy, it is likely that the remaining tissue continued to maintain an osmotic pressure that was balanced by the constraints of the collagen fiber network.
Findings from this study provide insight into the mechanisms for load support and load sharing between the nucleus pulposus and annulus fibrosus. Based on our observations that cyclic tensile and compressive stiffness do not change with nucleotomy, it seems that at high loads (after the neutral zone) and relatively high frequencies (1.0 Hz and above) compressive loads are primarily supported by the annulus fibrosus. It has been shown that direct axial compression places the annulus into circumferential hoop tension,17,18,31,50 a loading condition for which the collagen fiber reinforcement of the annulus is uniquely suited.9,11 Axial support may be further provided by fluid pressure within the annulus itself, though at fast loading rates this pressure may not be dissipated by fluid flow out of the annulus, providing a possible explanation for the difference observed between cyclic stiffness (not significant) and slow ramp compressive stiffness (decreased with nucleotomy).
At low loads (within the neutral zone) and low frequencies (1 N/s slow ramp and creep) the nucleus pulposus plays a more significant role in disc function, as demonstrated by our findings of increased neutral zone length, decreased slow ramp stiffness, and altered viscoelastic creep parameters. In the low load regime, it is thought that the nucleus pulposus acts to dissipate energy and prevent excessive axial deformations as the nucleus pulposus transfers loads to the annulus fibrosus. These loads are resisted by tension in the collagen fibers with relatively small radial and axial deformations.31,50 However, when nucleus pulposus function is compromised (i.e. due to loss of proteoglycan or by nucleotomy), larger radial and axial deformation may occur before the annulus fibers become engaged and loaded.6,33,50 Because hypermobility and excessive neutral zone deformation are key mechanical features of degeneration,36,41,43 the internal load and deformation interactions between the nucleus and the annulus fibrosus are important and further study is needed to investigate these interactions.34,47
The viscoelastic creep response was faster and larger following nucleotomy, consistent with previous in vivo and in vitro animal studies.5,13,21,27– 29 As reflected in Fig. 9, nucleotomy primarily altered the early creep response: nucleotomy resulted in significant decreases in the early elastic and viscous damping coefficients, S 1 and η 1, but fewer changes in S 2 and η 2. Thus, the nucleus may play a greater role in the early creep response, whereas the late creep response may be determined more by the annulus fibrosus. It is possible that the creep changes were due to the endplate perforation itself, rather than due to the changes in the material properties and permeability of the nucleus tissue. However, if this were the case—we would expect to see similar differences in both the limited and radical groups rather than the graded response that we found in the present study.
The mechanical and structural changes that occur with nucleotomy (e.g. increased neutral zone deformation, increased deformation under load, decreased disc height) are similar to changes that occur in early degeneration.6,15,21,29,42,46,49 It is widely accepted that a loss of nucleus pulposus pressure may accelerate disc degeneration as a result of greater stresses and strains on the annulus fibrosus and cartilaginous endplates.16,21,46,51 Whether these changes occur by interventions or by normal aging, it is thought that degeneration progresses through two potential (and overlapping) pathways: direct mechanical damage (by cyclic fatigue, increased shear stresses, delamination, and others)14,19,37 and cellular remodeling.48,51 Cadaveric studies of cyclic fatigue loading provide a model system to separate these two pathways.25,30
Nucleus pulposus implants and tissue engineered constructs are currently in development to restore mechanical function following clinical nucleotomy, herniation, or in degenerative disc disease.2,4,8,26 Such treatments require evaluation of mechanical function within the nucleus functional loading regime (neutral zone, ROM, creep). For example, human cadaver studies have shown that insertion of a prosthetic nucleus pulposus device restores the range of motion, neutral zone length, and disc height to near normal levels.12,26,54 These studies performed the elastic mechanical tests necessary to evaluate the function of a nucleus treatment. The findings of the present study indicate that while evaluations should continue to focus on the neutral zone and range of motion, they should also include the viscoelastic creep response. A compressive ramp test is not sufficient to accurately characterize the mechanical behavior of the motion segment. Even after radical nucleotomy, discs exhibited no change in cyclic compressive stiffness. Furthermore, the expediency of this experimental protocol may offer appropriate methods of in vitro testing of prototypic nucleus pulposus implants and tissue engineered constructs.
While the effects of nucleotomy on disc behavior were shown, the authors acknowledge limitations in this study. The nucleotomy was performed blindly through the superior vertebral body. Without visual guidance, it was difficult to gauge the location of the perforation. The optical and MR images, however, indicate that the annulus fibrosus was unharmed by the procedure and that the perforations were confined to the nucleus pulposus. The procedure necessarily disrupted the vertebral body and endplate but kept the annulus fibrosus structurally intact. Previous nucleotomy studies have used an incision through the annulus fibrosus, which itself alters disc mechanics.3,7,39,49 For the trans-endplate nucleotomy procedure used here, we contend that the axial motion segment mechanics were unaffected by the partial vertebral body removal because the stiffness of the ovine vertebra is orders of magnitude greater than the disc. Though a sham treatment group could potentially provide additional information about the effects of endplate perforation alone, in light of the results from the present study it is unlikely that there would be a statistically discernible sham treatment effect. Because the sham treatment would be even less disruptive than the limited nucleotomy, we would not expect the sham treatment to produce significantly different results from control. This is confirmed by our findings for no change in compression or tensile stiffness with nucleotomy, the graded response with nucleus removal, and the overall lack of statistically significant changes in the limited nucleotomy group. Still, the endplate perforation may have affected the creep behaviors and a separate control group with only a perforation (with no nucleus removal) would be required to address this. We acknowledge that the trans-endplate model does not presently represent a clinically viable surgical approach; however, the model provides a platform to study the mechanical effects of nucleotomy without an annulus fibrosus incision. A second limitation is the use of pure axial compression–tension loading. While simple axial tension is not physiologic, portions of the disc experience tensile loads during bending and torsion. Such loading was necessary to obtain the critical neutral zone behaviors which cannot be measured using pure compression, and the findings of the present study will likely translate to other loading regimes.
In summary, this study demonstrated that nucleotomy does not significantly affect cyclic axial stiffness of the disc at 1.0 Hz, however, we did observe increased range of motion, and in particular increased neutral zone length. Moreover, nucleotomy significantly altered the viscoelastic creep behavior and slow ramp compressive stiffness. These results are important toward understanding the loading mechanisms within the disc and the potential role of altered nucleus pulpous function in the degenerative cascade. Loss of nucleus pulposus function could lead to greater neutral zone deformation, subjecting the annulus fibrosus to increased stresses and strains. This may be key to understanding the progression of intervertebral disc degeneration. Further, our results suggest that functional evaluation of nucleus pulposus replacements and engineered disc constructs must focus on neutral zone and viscoelastic creep behaviors in addition to stiffness.
REFERENCES
Adams, M. A., B. J. Freeman, H. P. Morrison, I. W. Nelson, and P. Dolan, Mechanical initiation of intervertebral disc degeneration. Spine 25(13):1625–1636, 2000.
Alini, M., P. J. Roughley, J. Antoniou, T. Stoll, and M. Aebi, A biological approach to treating disc degeneration: Not for today, but maybe for tomorrow. Eur. Spine J. 11(Suppl 2):S215–S220, 2002.
Argoubi, M., and A. Shirazi-Adl. Poroelastic creep response analysis of a lumbar motion segment in compression. J. Biomech. 29(10):1331–1339, 1996.
Bao, Q. B., and H. A. Yuan. New technologies in spine: Nucleus replacement. Spine 27(11):1245–1247, 2002.
Bradford, D. S., T. R. Oegema, Jr., K. M. Cooper, K. Wakano, and E. Y. Chao, Chymopapain, chemonucleolysis, and nucleus pulposus regeneration. A biochemical and biomechanical study. Spine 9(2):135–147, 1984.
Brinckmann, P., and H. Grootenboer. Change of disc height, radial disc bulge, and intradiscal pressure from discectomy. An in vitro investigation on human lumbar discs. Spine 19(6):643–646, 1991.
Brinkmann, P. Injury of the annulus fibrosus and disc protrusions: An in vitro investigation on human lumbar discs. Spine 11(2):149–153, 1986.
Diwan, A. D., H. K. Parvataneni, S. N. Khan, H. S. Sandhu, F. P. Girardi, and F. P. Cammisa, Jr., Current concepts in intervertebral disc restoration. Orthop. Clin. North Am. 31(3):453–464, 2000.
Ebara, S., J. C. Iatridis, L. A. Setton, R. J. Foster, V. C. Mow, and M. Weidenbaum, Tensile properties of nondegenerate human lumbar anulus fibrosus. Spine 21(4):452–461, 1996.
Elliott, D. M., and J. J. Sarver. Young investigator award winner: Validation of the mouse and rat disc as mechanical models of the human lumbar disc. Spine 29(7):713–722, 2004.
Elliott, D. M., and L. A. Setton. Anisotropic and inhomogeneous tensile behavior of the human anulus fibrosus: Experimental measurement and material model predictions. J. Biomech. Eng. 123:256–263, 2001.
Eysel, P., J. Rompe, R. Schoenmayr, and J. Zoellner, Biomechanical behaviour of a prosthetic lumbar nucleus. Acta Neurochir (Wien) 141(10):1083–1087, 1999.
Furlong, D. R., and A. N. Palazotto. A finite element analysis of the influence of surgical herniation on the viscoelastic properties of the intervertebral disc. J. Biomech. 16(10):785–795, 1983.
Goel, V. K., B. T. Monroe, L. G. Gillbertson, and P. Brinckmann, Interlaminar shear stresses and laminae separation in a disc; Finite element analysis of the L3-L4 motion segment subjected to axial compressive loads. Spine 20(6):689–698, 1995.
Goel, V. K., K. Nishiyama, J. N. Weinstein, and Y. K. Liu, Mechanical properties of lumbar spinal motion segments as affected by partial disc removal. Spine 11(10):1008–1012, 1986.
Hasegawa, K., C. H. Turner, J. Chen, and D. B. Burr, Effect of disc lesion on microdamage accumulation in lumbar vertebrae under cyclic compression loading. Clin. Orthop. Relat. Res. 311:190–198, 1995.
Hickey, D. S., and D. W. L. Hukins. Relation between the structure of the annulus fibrosus and the function and failure of the intervertebral disc. Spine 5(2):106–116, 1980.
Hukins, D. W. A simple model for the function of proteoglycans and collagen in the response to compression of the intervertebral disc. Proc. R. Soc. Lond., B, Biol. Sci. 249(1326):281–285, 1992.
Iatridis, J. C., and I. ap Gwynn. Mechanisms for mechanical damage in the intervertebral disc annulus fibrosus. J. Biomech. 37(8):1165–1175, 2004.
Iatridis, J. C., L. A. Setton, M. Weidenbaum, and V. C. Mow, Alterations in the mechanical behavior of the human lumbar nucleus pulposus with degeneration and aging. J. Orthop. Res. 15:318–322, 1997.
Ishihara, H., H. Tsuji, N. Hirano, H. Ohshima, and N. Terahata, Biorheological responses of the intact and nucleotomized intervertebral discs to compressive, tensile, and vibratory stresses. Clin. Biomech. 8:250–254, 1993.
Johannessen, W. and D. M. Elliott. Effects of degeneration on the biphasic material properties of human nucleus pulposus in confined compression. Spine, in review.
Johannessen, W., E. J. Vresilovic, and D. M. Elliott, Effects of endplate nucleotomy and cyclic compressive loading on lumbar disc mechanics in vitro. Clin. Biomech., in review.
Johannessen, W., E. J. Vresilivic, A. C. Wright, and D. M. Elliott, Effects of partial nucleotomy and repetitive loading on intervertebral disc mechanics. Proceedings of the Summer Bioengineering Conference, 2003.
Johannessen, W., et al. Intervertebral disc mechanics are restored following cyclic loading and unloaded recovery. Ann. Biomed. Eng. 32:70–76, 2004.
Joshi, A., G. Fussell, J. Thomas, A. Hsuan, A. Lowman, A. Karduna, E. Vresilovic, and M. Marcolongo. Functional compressive mechanics of a PVA/PVP nucleus pulposus replacement. Biomaterials 27(2):176–184, 2006.
Kazarian, L. E. Creep characteristics of the human spinal column. Orthop. Clin. North Am. 6(1):3–18, 1975.
Keller, T. S., D. M. Spengler, and T. H. Hansson. Mechanical behavior of the human lumbar spine. I. Creep analysis during static compressive loading. J. Orthop. Res. 5(4):467–478, 1987.
Keller, T. S., D. M. Spengler, and T. H. Hansson. In vivo creep behavior of the normal and degenerated porcine intervertebral disk: A preliminary report. J. Spinal Disord.1(4):267–278, 1988.
Kuroki, H., V. K. Goel, S. A. Holekamp, N. A. Ebraheim, S. Kubo, and N. Tajima. Contributions of flexion-extension cyclic loads to the lumbar spinal segment stability following different discectomy procedures. Spine 29(3):E39–E46, 2004.
Laible, J. P., D. S. Pflaster, M. H. Krang, B. R. Simon, and L. D. Haugh. Poroelastic-swelling finite element model with application to the intervertebral disc. Spine 18(5):659–670, 1993.
Markolf, K. L., and J. M. Morris. Structural components of the intervertebral disc. J. Bone Joint Surg. 56A(4):675–687, 1974.
Meakin, J. R., T. W. Redpath, and D. W. Hukins. The effect of partial removal of the nucleus pulposus from the intervertebral disc on the response of the human annulus fibrosus to compression. Clin. Biomech. (Bristol, Avon) 16(2):121–128, 2001.
Meakin, J. R., T. W. Redpath, and D. W. Hukins. The effect of partial removal of the nucleus pulposus from the intervertebral disc on the response of the human annulus fibrosus to compression. Clin. Biomech. 16(2):121–128, 2001.
Meakin, J. R., and D. W. Hukins. Effect of removing the nucleus pulposus on the deformation of the annulus fibrosus during compression of the intervertebral disc. J. Biomech. 33(5):575–580, 2000.
Mimura, M., M. M. Panjabi, T. R. Oxland, J. J. Crisco, I. Yamamoto, and A. Vasavada. Disc degeneration affects the multidirectional flexibility of the lumbar spine. Spine 19(12):1371–1380, 1994.
Natarajan, R. N., J. H. Ke, and G. B. J. Andersson. A model to study the disc degeneration process. Spine 19(3):259–265, 1994.
Natarajan, R. N., J. R. Williams, and G. B. Andersson. Recent advances in analytical modeling of lumbar disc degeneration. Spine 29(23):2733–2741, 2004.
Natarajan, R. N., J. R. Williams, and G. B. Andersson. Effect of annular incision type on the change in biomechanical properties in a herniated lumbar intervertebral disc. J. Biomech. Eng. 124(2):229–236, 2002.
O'Connell, G. D., E. J. Vresilovic, and D. M. Elliott. Comparative intervertebral disc anatomy across several animal species. Transactions of the Orthopaedic Research Society, 52nd Annual Meeting, in review.
Oxland, T. R., and M. M. Panjabi. The onset and progression of spinal injury: A demonstration of neutral zone sensitivity. J. Biomech. 25(10):1165–1172, 1992.
Panjabi, M. M., M. H. Krag, and T. Q. Chung. Effects of disc injury on mechanical behavior of the human spine. Spine 9(7):707–713, 1984.
Panjabi, M. M., M. H. Krag, and T. Q. Chung. Effects of disc injury on mechanical behavior of the human spine. Spine 9(7):707–713, 1984.
Sarver, J. J., and D. M. Elliott. Mechanical differences between lumbar and tail discs in the mouse. J. Orthop. Res. 23(1):150–155, 2005.
Sato, K., S. Kikuchi, and T. Yonezawa. In vivo intradiscal pressure measurement in healthy individuals and in patients with ongoing back problems. Spine 24(23):2468–2474, 1999.
Seroussi, R. E., M. H. Krang, D. L. Muller, and M. H. Pope. Internal deformations of intact and denucleated human lumbar discs subjected to compression, flexion, and extension loads. J. Orthop. Res. 7:122–131, 1989.
Seroussi, R. E., M. H. Krang, D. L. Muller, and M. H. Pope. Internal deformations of intact and denucleated human lumbar discs subjected to compression, flexion, and extension loads. J. Orthop. Res. 7(1):122–131, 1989.
Setton, L. A., and J. Chen. Cell mechanics and mechanobiology in the intervertebral disc. Spine 29(23):2710–2723, 2004.
Shea, M., T. Y. Takeuchi, R. H. Wittenberg, A. A. White, and W. C. Hayes. Comparison of the effects of automated percutaneous discectomy and conventional discectomy on intradiscal pressure, disc geometry, and stiffness. J. Spinal Disord. 7(4):317–325, 1994.
Shirazi-Adl, A. Finite element simulation of changes in the fluid content of human lumbar discs. Spine 17(2):206–212, 1992.
Stokes, I. A., and J. C. Iatridis. Mechanical conditions that accelerate intervertebral disc degeneration: Overload versus immobilization. Spine 29(23):2724–2732, 2004.
Urban, J. P. G., and J. F. McMullin. Swelling pressure of the lumbar intervertebral discs: Influence of age, spinal level, composition, and degeneration. Spine 13(2):179–187, 1988.
Virgin, W. J. Experimental investigations into the physical properties of the intervertebral disc. J. Bone Joint Surg. 33B(4):607–611, 1951.
Wilke, H. J., S. Kavanagh, S. Neller, C. Haid, and L. E. Claes. Effect of a prosthetic disc nucleus on the mobility and disc height of the L4-5 intervertebral disc postnucleotomy. J. Neurosurg. 95(2 Suppl):208–214, 2001.
ACKNOWLEDGMENTS
The authors thank the National Institutes of Health AR 050052 for supporting this study. The authors also thank Justin Mills for his assistance in mechanical testing and Alexander Wright for his contribution to the MR imaging.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Johannessen, W., Cloyd, J.M., O'Connell, G.D. et al. Trans-Endplate Nucleotomy Increases Deformation and Creep Response in Axial Loading. Ann Biomed Eng 34, 687–696 (2006). https://doi.org/10.1007/s10439-005-9070-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-005-9070-8