
Abstract
Background:Patients with distant melanoma metastases have median survivals of 4 to 8 months. Previous studies have demonstrated improved survival after complete resection of pulmonary and hollow viscus gastrointestinal metastases. We hypothesized that patients with metastatic disease to intra-abdominal solid organs might also benefit from complete surgical resection.
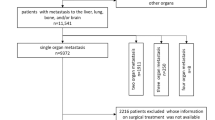
Methods:A prospectively acquired database identified patients treated for melanoma metastatic to the liver, pancreas, spleen, adrenal glands, or a combination of these from 1971 to 2010434_2001_Article_658. The primary intervention was complete or incomplete surgical resection of intra-abdominal solid-organ metastases, and the main outcome measure was postoperative overall survival (OS). Disease-free survival (DFS) was a secondary outcome measure.
Results:Sixty patients underwent adrenalectomy, hepatectomy, splenectomy, or pancreatectomy. Median OS was significantly improved after complete versus incomplete resections, but median OS after complete resection was not significantly different for single-site versus synchronous multisite metastases. The 5-year survival in the group after complete resection was 24%, whereas in the incomplete resection group, there were no 5-year survivors. Median DFS after complete resection was 15 months. Of note, the 2-year DFS after complete resection was 53% for synchronous multi-site metastases versus 26% for single-site metastases.
Conclusions:In highly selected patients with melanoma metastatic to intra-abdominal solid organs, aggressive attempts at complete surgical resection may improve OS. It is important that the number of metastatic sites does not seem to affect the OS after complete resection.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
REFERENCES
Overett TK, Shiu MH. Surgical treatment of distant metastatic melanoma. Indications and results. Cancer 1985;56:1222–1230.
Karakousis CP, Temple DF, Moore R, Ambrus JL. Prognostic parameters in recurrent malignant melanoma. Cancer 1983;52:575–579.
Sharpless SM, Das Gupta TK. Surgery for metastatic melanoma. Semin Surg Oncol 1998;14:311–318.
Fletcher WS, Pommier RF, Lum S, Wilmarth TJ. Surgical treatment of metastatic melanoma. Am J Surg 1998;175:413–417.
Leo F, Cagini L, Rocmans P, et al. Lung metastases from melanoma: when is surgical treatment warranted?. Br J Cancer 2000;83:569–572.
Ollila DW, Hsueh EC, Stern SL, Morton DL. Metastasectomy for recurrent stage IV melanoma. J Surg Oncol 1999;71:209–213.
Ollila DW, Morton DL. Surgical resection as the treatment of choice for melanoma metastatic to the lung. Chest Surg Clin N Am 1998;8:183–196.
Ollila DW, Essner R, Wanek LA, Morton DL. Surgical resection for melanoma metastatic to the gastrointestinal tract. Arch Surg 1996;131:975–979.
Ollila DW, Stern SL, Morton DL. Tumor doubling time: a selection factor for pulmonary resection of metastatic melanoma. J Surg Oncol 1998;69:206–211.
Tafra L, Dale PS, Wanek LA, Ramming KP, Morton DL. Resection and adjuvant immunotherapy for melanoma metastatic to the lung and thorax. J Thorac Cardiovasc Surg 1995;110:119–128.
Branum GD, Epstein RE, Leight GS, Seigler HF. The role of resection in the management of melanoma metastatic to the adrenal gland. Surgery 1991;109:127–131.
InstitutionalAuthorNameLong-term results of lung metastasectomy: prognostic analyses based on 5206 cases (1997) ArticleTitleThe International Registry of Lung Metastases J Thorac Cardiovasc Surg 113 37–49
Petit T, Borel C, Rixe O, et al. Complete remission seven years after treatment for metastatic malignant melanoma. Cancer 1996;77:900–902.
Meyer T, Merkel S, Goehl J, Hohenberger W. Surgical therapy for distant metastases of malignant melanoma. Cancer 2000;89:1983–1991.
Agrawal S, Yao TJ, Coit DG. Surgery for melanoma metastatic to the gastrointestinal tract. Ann Surg Oncol 1999;6:336–344.
Haigh PI, Essner R, Wardlaw JC, Stern SL, Morton DL. Long-term survival after complete resection of melanoma metastatic to the adrenal gland. Ann Surg Oncol 1999;6:633–639.
Rose DM, Essner R, Hughes TMD, et al. Surgical resection for metastatic melanoma to the liver: the John Wayne Cancer Institute and Sydney Melanoma Unit Experience. Arch Surg (in press).
Wong JH, Euhus DM, Morton DL. Surgical resection for metastatic melanoma to the lung. Arch Surg 1988;123:1091–1095.
O’Day SJ, Gammon G, Boasberg PD, et al. Advantages of concurrent biochemotherapy modified by decrescendo interleukin-2, granulocyte colony-stimulating factor, and tamoxifen for patients with metastatic melanoma. J Clin Oncol 1999;17:2752–2761.
Morton DL, Foshag LJ, Hoon DS, et al. Prolongation of survival in metastatic melanoma after active specific immunotherapy with a new polyvalent melanoma vaccine [published erratum appears in Ann Surg 1993;217:309]. Ann Surg 1992;216:463–482.
Hsueh EC, Gupta RK, Qi K, Morton DL. Correlation of specific immune responses with survival in melanoma patients with distant metastases receiving polyvalent melanoma cell vaccine. J Clin Oncol 1998;16:2913–2920.
Morton DL, Ollila DW, Hsueh EC, Essner R, Gupta RK. Cytoreductive surgery and adjuvant immunotherapy: a new management paradigm for metastatic melanoma. CA Cancer J Clin 1999;49:101–116.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the 54th Annual Meeting of the Society of Surgical Oncology, Washington, DC, March 15–18, 2001.
Rights and permissions
About this article
Cite this article
Wood, T.F., DiFronzo, L.A., Rose, D.M. et al. Does Complete Resection of Melanoma Metastatic to Solid Intra-Abdominal Organs Improve Survival?. Ann Surg Oncol 8, 658–662 (2001). https://doi.org/10.1007/s10434-001-0658-4
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s10434-001-0658-4