
Abstract
In this paper, we highlighted links between personality traits and successful ageing through a systematic review of recent empirical studies. Particularly, we addressed the question of whether personality traits are related to successful ageing and, if so, why and how? Answers to this question provided, for example, arguments that supported personality’s role in planning an individual’s future based on self-knowledge, thereby contributing to a sense of identity throughout their life. Then, considering longitudinal studies, we examined whether personality is stable over one’s life course, or does it change and, if so, why and under what conditions? Answers to this question gave substance to the idea that a stable personality allows for continuous and consistent development. In addition, certain personality changes are likely to allow an individual to develop the resilience to better adapt to life’s challenges. Therefore, the arguments brought by these two questions can help clarify the modulating role of personality for successful ageing via health and well-being outcomes. These insights may contribute to the development of new prevention approaches, more focused on inter- and intraindividual differences, to promote successful ageing.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the last two decades, a considerable amount of gerontological research has sought answers about how individuals may age successfully (e.g. Jopp et al. 2016a). Although researchers are far from understanding underlying mechanisms of successful ageing (SA), there is a growing interest for the idea that specific personality traits could be involved (e.g. Kato et al. 2013). Hence, we conducted a systematic review of recent empirical studies on the relationships between personality and SA to provide support and substance to the concept of personality having a role in SA. A large number of studies have supplied considerable evidence that changes in multiple domains of functioning such as physical and psychological health, cognition, and social networking characterize old and very old age (e.g. Ihle et al. 2016). Although there has been no agreement on a universal definition for SA (e.g. Pruchno et al. 2015), many scholars have agreed that SA refers to physical, psychological, and social well-being in old age (Cosco et al. 2014; Martin et al. 2015). According to scientific approaches in conjunction with complementary lay perspectives, SA is a multidimensional construct that includes as key dimensions physical and functional health, cognitive functioning, emotional adjustment and positive affect, and social engagement (e.g. Jopp et al. 2015). Well-trained cognitive, behavioural, and affective tendencies, captured by personality traits (e.g. Kato et al. 2013), may represent factors of primary importance as they influence the individual’s thinking, acting, and feelings over the course of their lifespan, with substantial consequences for different central domains of functioning and well-being (e.g. Chan et al. 2018), which accumulate in old age (e.g. Caspi et al. 2005). For instance, being more conscientious has been associated with more positive health behaviour and better health (e.g. Pocnet et al. 2016a); at the same time, conscientiousness may influence individuals’ social networks, as they may be sought out as reliable interaction partners (e.g. Kern and Friedman 2008). High extraversion is likely to be associated with a larger social network at any point in the lifespan (e.g. Pocnet et al. 2016b). Instead, a higher level of neuroticism may come with generally experiencing more negative emotions, being less well able to adapt to difficulty, feeling less trust in others, and having fewer social relations (Lahey 2009; Sutin et al. 2011). Thus, as suggested by these examples, personality could have a considerable impact on how successfully individuals develop and age over their lifespan.
Considering the biopsychosocial model of SA, we addressed the following research questions: for the first section, we investigated whether personality traits are related to SA and, if so, how and why? Answers to this question could help clarify personality’s role for individual’s development across the lifespan. Personality may allow to better understand, for instance, how individuals acquire and treat resources such as health, as well as how they plan their futures based on their knowledge about themselves, and thus contributes to their sense of identity throughout their lives. Moreover, understanding the mechanisms of each personality trait can help people assume their responsibilities by adopting healthy or unhealthy behaviours throughout their lives, which could impact their ageing. For the second section, we examined whether personality is stable over the life course, or whether it may change and, if so, under what conditions? The answers to this question could support the idea that a stable personality allows for continuous and consistent development. In turn, certain personality changes could allow an individual to develop the resilience to better adapt to life’s challenges. Therefore, the arguments these two questions introduce could help clarify personality’s modulating role in SA via health and well-being outcomes. The final section presents possible interventions for developing a balanced and adaptable personality that is likely to contribute to health promotion and SA.
Methods
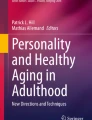
We undertook a systematic literature review, searching PubMed, PsycINFO, SocioFile, Ovid, Web of Science, Google Scholar, and Research Gate. Searches were defined by all possible keywords’ combinations of the terms and variations of “successful ageing,” “personality,” “health,” “well-being,” and “quantitative studies.” We included 178 papers presenting reviews or overviews, meta-analysis of the topic, or data from cross-sectional and longitudinal surveys. We excluded 53 studies that did not report on the associations between the mentioned keywords. Based on an abstract and title search, we assessed 125 papers for eligibility but excluded 49 after full-text reviews because they did not have a personality measure or represent qualitative but not quantitative studies. Finally, we included 76 quantitative studies in the systematic review (Fig. 1).

Inclusion flowchart: screening process for study inclusion
Results
Our search identified 76 studies that met the predefined criteria, that is, reported quantitative data from adults over age 60. Three studies included a female-only population, and the other studies included a mixed elderly population. The studies were published between 2000 and 2020. Specific details from some of these studies are presented in Table 1.
Are Personality Traits Related to Successful Ageing and, if So, Why and How?
Personality has been described with various models. Among them, the five-factor model benefits from strong empirical support (McCrae and Costa 2008) and suggests five main dimensions to accurately and succinctly describe personality traits: conscientiousness, neuroticism, extraversion, openness to experiences, and agreeableness. Each of these personality dimensions is likely to influence SA differently.
For instance, conscientiousness (C), involving competence, orderliness, dutifulness, achievement-striving, self-discipline, and deliberation, is the most likely to be implicated in various aspects that could contribute to SA such as health-promoting behaviours and cognitions (e.g. Kern and Friedman 2011). Several recent studies have suggested the effects of higher C on SA via health and well-being outcomes. For example, the C component self-discipline may facilitate positive development (Moffitt et al. 2011) because it has been linked to a variety of health-promoting activities, including maintaining a balanced diet and abstaining from smoking, alcohol, and other substance addictions (Bogg and Roberts 2004). People with high C scores are well organized and able to anticipate and prepare for the consequences of potential future adversities (Pocnet et al. 2016b) and thus may better adjust to change (Roberts et al. 2007). Moreover, as other people trust in them, conscientious people will be better able to create lasting relationships, which will contribute to their SA. These individuals also have enhanced adaptive coping strategies, which in turn could help them live better and longer (Chapman et al. 2010).
Concerning the underlying biological mechanisms, the findings of a meta-analysis of personality’s genome-wide association studies on multiple samples found one single nucleotide protein—KATNAL2—that was associated with C (de Moor et al. 2012). Nevertheless, replication is difficult to achieve due to the many intervening factors between a single nucleotide protein and a complex phenotype such as the C trait (Terracciano et al. 2010). Lower C has been linked to higher levels of the inflammatory marker interleukin (Chapman et al. 2011). Also associated with chronic stress, negative health behaviours, or diseases, interleukin could be a predictor of mortality in older persons (Gruenewald et al. 2006). While C seems, in general, to have a beneficial role, pathologically high levels of C such as perfectionism or compulsive persistence should, however, be noted as enhancing the risk of mortality (Fry and Debats 2009). Immunological studies have suggested that compulsive persistence, defined as the inability to disengage from an impossible, stressful task, induces a higher hypothalamic–pituitary–adrenal axis response (Smith and Vale 2006). Hence, it is helpful to differentiate healthy C, as a protective factor of SA, from extreme inflexibility or compulsive behaviour as a risk factor of mortality.
Neuroticism (N) is the personality trait that researchers have most often examined in conjunction with unhealthy behaviours, which are likely to have a negative impact on SA. Defined as the tendency to experience negative emotions, including hostility, anxiety, depression, self-consciousness, impulsiveness, and vulnerability (Costa and McCrae 1992), N has been suggested to be a risk factor for increasing stress levels. Also called emotional instability, N is associated with more difficulties coping with life challenges (Judge et al. 2002), poor lifestyle choices such as limited food intake control (Brummett et al. 2006) and smoking (Terracciano and Costa 2004), and general aetiologic factors, which make individuals vulnerable and could lead to a foreshortened life (Chapman et al. 2011). In line with this, N has been argued to be of public health relevance because it is associated with a host of negative outcomes and a poor quality of life (Ellenbogen et al. 2010; Pocnet et al. 2016b). Several studies have linked higher N to all-cause mortality in the general population (Chapman et al. 2010; Ploubidis and Grundy 2009) or to chronic diseases such Alzheimer’s-type dementia (Henriques-Calado and Duarte-Silva 2020; Segerstrom 2020; Terracciano and Sutin 2019), cardiovascular disease (Pelle et al. 2010; Sutin et al. 2011), and cancer (Dahl 2010). Concerning underlying biological mechanisms, some research has shown that N is linked to neuroendocrine interactions involving the hypothalamic–pituitary–adrenal and sympatho-medullary axes (Ouanes and Popp 2019). Although N has been a topic of considerable research linked to risk behaviours and unhealthy outcomes, this personality trait has rarely been considered in relation to the lifespan development and ageing.
Extraversion (E) encompasses the tendency towards assertiveness, warmth, gregariousness, activity, excitement-seeking, and positive emotions (Costa and McCrae 1992). The mechanisms by which E may improve the subjective quality of life are not clear, and the results are somewhat mixed, with findings suggesting reduced, increased, and no mortality risks. Biological research shows that E is partly a function of dopaminergic activity (Deary et al. 2010). Moreover, studies suggest associations of E with immune function. For example, optimism as a positive future attitude representing a cognitive–emotional facet of E was found to be linked to a lower level of inflammatory markers (Gawronski et al. 2016), representing an element associated with reduced all-cause mortality risk (Solberg Ness and Segerstrom 2006), yet underlying mechanisms linking E to health functioning are not clear. Some authors suggest that E may come with various benefits that reduce the experience of stress in everyday life. Compared to pessimists, optimists seem to have more effective emotional regulation, which allows them to better deal with unpleasant events. Specifically, they use more planning (Brissette et al. 2002), more reassessment (Gross and John 2003), more acceptance (Solberg Ness and Segerstrom 2006), and fewer strategies that focus on the negative aspects of the event (Scheier et al. 1994). Having an attentional bias towards positive information, optimists seem to avoid negative information, which suggests a facility for emotional disengagement, allowing thus information processing (Johnson 2009). However, optimism can also come with some downsides: more optimistic people may experience more frustration when they have no immediate success (Moffitt et al. 2011) and may persist longer in stressful situations because they expect positive results (Segerstrom 2007). Another risk is that optimists tend to overestimate the chance that their coping efforts may be successful and underestimate potential negative events, thinking all will be good (Shah et al. 2016). E comes also with various social benefits: More extraverted people like to be with other people and enjoy the company of others, which may help to more easily find social partners and create lasting social relationships. As a consequence, they may have a larger support network and profit more fully from these relationships in normal times and when confronted with difficulty. Another explanation is that compared to introverts, extroverts are more able to process verbal information supporting their sociability, which in turn may be useful for adaptation purposes (Pocnet et al. 2015a). E may be particularly protective against feelings of loneliness, general social withdrawal, and isolation, risks associated with very old age. In line with these assumptions, the role of E seems powerful even in very old individuals with little resources. Specifically, in centenarians, E was found to have an independent direct effect on well-being, while controlling for health, cognitive function, number of social partners, and even optimistic outlook (Jopp et al. 2008). Thus, E may represent a particularly important personality trait to study in the contact of psychological mechanism of SA that deserves to be studied. It is also helpful to differentiate healthy E, as a protective factor of SA, from unhealthy E—defined on the one hand by very high expectations and chances for overestimation of coping strategies and on the other hand by underestimation of some critical life events—as a possible risk factor for pathological ageing.
Openness to experiences (O) incorporates facets such as fantasy, aesthetics, feelings, actions, ideas, and values (Costa and McCrae 1992). Regarding its influence on SA, few studies exist, but results have suggested that higher levels of O are associated with a decreased risk for specific mortality types, such as cardiovascular mortality (Jonassaint et al. 2007). Other studies have found that cognitive and behavioural flexibility, curiosity, and an interest in aesthetics were particularly important predictors of SA (Turiano et al. 2012). The biological mechanisms by which O may improve well-being and therefore SA are not clear. However, it has been found that O may be related to markers of synaptic plasticity, such as insulin-like growth factor, which has been linked to cognitive function and SA (e.g. Cappola et al. 2003). Moreover, the catechol-O-methyltransferase gene, which regulates levels of dopamine in the prefrontal cortex, has also been associated with cognitive functioning in healthy older adults (e.g. Erickson et al. 2008). Individuals with high O have been found to be able to seek out environments, which enhances cognitive engagement and flexibility, contributing to the maintenance of cognitive function (i.e. Duberstein et al. 2011). Higher cognitive functioning may, in turn, have an effect on physical health, for instance, by helping to prevent avoidable health problems and increasing adaptive disclosure of health concerns, decision-making, and the capacity to manage problems that are encountered throughout people’s lives, including in old age. In contrast, a low premorbid O has been related to higher amounts of cerebral pathology (i.e. Alzheimer’s disease) and was found to predict lower cognitive performance in AD patients (Tautvydaitė et al. 2017). Although O has been a topic of several studies linking O and cognitive functions to health outcomes, this relationship has rarely been considered in relation to the lifespan.
Agreeableness (A) is a dimension combining some traits related to maintaining interpersonal harmony: trust, honesty, compliance, interpersonal deference, altruism, and compassion for others (Costa and McCrae 1992). Regarding the association between A and SA, few studies exist, and they show weak or unclear relations. For instance, one study demonstrated a protective effect for A against all-cause mortality (Weis and Costa 2005), but another study found that A was associated with higher all-cause mortality when combined with low C (Chapman et al. 2010). Regarding biological mechanisms, the link between A and serotonin level has been interpreted as a socialization factor that reflects an array of socially desirable facets or expresses personality development through socialization (De Young 2010). Given its general tendency to regulate or restrain potentially disruptive emotions and behaviours in social relationships, A is likely to contribute to a continuous developmental process (Pocnet et al. 2018). What could be the role of A in SA, as well as the associated underlying mechanisms, remains speculative, however, as little research has been carried out in this domain. Given the nature of A, its indirect effects could also be considered: for instance, people with high A could have a larger social network and more exchanges, which in turn may be linked to better health and lower mortality, but this still needs to be studied.
Having a better understanding of the mechanisms of each personality dimension and therefore a better self-knowledge, this would help to improve decisions about people’s health and their subjective well-being for as long as possible (Araújo et al. 2018). For example, knowing that a low level in N may influence effectively the management of stressful situations, this in turn could have an impact on physical and mental health, whereas a high E level may contribute to a greater subjective well-being and vitality (Givens et al. 2009; Ribeiro et al. 2014). Likewise, O and C personality traits can lead to self-selection in different environments. Thus, disadvantageous socio-economic situations can generate various responses (Donnellan et al. 2009) being interpreted as challenges to be taken up by people who are both open and conscientious, influencing their well-being and thus SA (Chapman et al. 2012; Sutin et al. 2011).
Is personality stable over the life course, or does it change and, if so, why and under what conditions?
When considering personality as a factor influencing SA, an important question includes to what extent personality remains stable or changes as a person grows older and until what point this dynamic is important for SA. Globally, research has indicated that personality traits are relatively consistent over the life course, implicating that changes are neither fast nor significant (Pocnet et al. 2011). Longitudinal studies covering long periods of the lifespan provide important evidence for the stability of individuals’ personality. Defining personality in terms of enduring dispositions, Costa and McCrae (1992) followed individuals aged between 19 and 80 years old for over 12 years and found that personality remained stable after approximately 30 years of age. Moreover, the Baltimore Longitudinal Studies of Adult Life and Ageing found that people who were cheerful and assertive when they were 30 years old would likely be the same when they were 80 years old (Tan et al. 2011). More than that, a longitudinal study over six decades (Harris et al. 2016) found that some aspects of personality in older age may even relate to personality childhood. These longitudinal studies further argued that this stability is be important for psychological well-being, as it would provide a consistent and reliable basis for adaptation to a changing world. This idea is supported by specific personality traits shared by centenarians such as low N and high E, O, and C also potentially having strong heritable genetic components (Andersen et al. 2012; Distel et al. 2009).
Beyond the concept of personality as being comprised of stable traits, personality can be understood as a developmental construct that by nature is subject to change and adaptation over the lifespan (Caspi et al. 2005). Supporting this notion, longitudinal studies of the transition from adolescence to adulthood have indicated distinct patterns of stability and change for several dimensions of personality. For instance, some authors have suggested that between the ages of 20 and 30, people’s personalities change and attain a configuration of traits that will characterize them for years to come (Costa and McCrae 2003). They argued that during this period, adaptive functions develop that are related to entry into adult life, in which individuals must adapt to a new life which balances work, family, and societal demands. People in this stage exhibit increased self-control, ability to plan, emotional regulation, altruism, trust, and warm engagement with others, all facilitating their recognition of societal expectations and their involvement in adult social roles (Roberts et al. 2006). Cross-sectional (McCrae and Costa 2008) and longitudinal (Costa and McCrae 2006) analyses have suggested that normative declines in N, E, and O continue after age 30, albeit at a modest rate of 1–2 T-score points per decade. This period seems to follow a plateau of the average level of these personality traits until people are in their mid-50s; thereafter, there is a slight decline (Morizot and Le Blanc 2005). These various changes over the lifespan indicate a pattern of increasing maturity with age, according to life’s growing responsibilities. Studies have also identified intraindividual changes in later life. Using a longitudinal study on 1944 participants (age ranged from 20 to 96 years) and hierarchical linear modelling analyses, Terracciano et al. (2005) found that personality changes gradually, indicating first stability up to age 60, and then decline in E, decline in O, increase in A and C up to age 70, as well as N declines up to age 80. Other research has shown that the mean-level changes in personality traits accelerated in very old age (e.g. Möttus et al. 2011), although there were no substantial changes in the eighth decade but rather in the second half of the 80th decade and in the ninth decade. Moreover, research on the personalities of centenarians’ offspring confirmed that distinctive characteristics might have important implications for their health benefits (Kern and Friedman 2008). Although some authors have shown that even in old age, structural stability is unaffected by ageing (Allemand et al. 2008), others have reported that moderate changes in personality features occur over an individual’s life course (Edmonds 2008), even during very old age. For example, an age-related decrease in E and C and an increase in harm avoidance have been reported for people of very old age (Lautenschlager and Förstl 2007). These changes could be part of an adaptive process for coping better with age-related morbidity and frailty in old age (Srivastava and Das 2013).
Regarding personality development, researchers have discussed different underlying mechanisms that can be grouped into biological, psychological, and social factors. As biological factors, genes may play a role, not only for the actual expression of personality traits but also for their temporal stability (or change). For instance, a prospective study on 833 twins from the Minnesota Twin Study of Adult Development and Aging asked participants to self-rate their personalities twice with a 5-year interval between measurements (Johnson et al. 2005). The results showed that the mean and standard deviation of scale scores of the personality traits remained stable between the first and the second self-rating. The authors concluded that the high stability of personality traits even in old age was based on a strong underlying genetic component in combination with stable environmental factors. Another study on twins confirmed the heritability of major personality traits in a range from 40 to 50%, with most of the remaining variation attributed to environmental influences (Roberts et al. 2006). These two studies suggested that genes not only define one’s temperament and represent the stability of their personality, but also keep influencing personality changes over their lifespan and contribute to intrinsic maturation (Caspi et al. 2005). For instance, personality changes at midlife, such as men accessing more their female sides and women more strongly expressing their male characteristics, that had been proposed in the context of Jung’s (1981) model of personality development may be due to normative hormonal changes associated with entering the post-reproductive phase of the lifespan (menopause). Other age-related biological changes may also be of importance, such as physiological ageing, which may be associated with some long-term personality changes (Roberts et al. 2006). For instance, age-related sensorimotor changes including impairments in vision (presbyopia), hearing (presbycusis), mobility were found to be linked to increases in N and decreases in E (e.g. Berg and Johansson 2013). Similarly, chronic diseases and chronic pain were found to be linked to high N and low O, E, and C (Jokela et al. 2014). The development of brain pathology also substantially contributes to personality changes (Henriques-Calado and Duarte-Silva 2020; Tautvydaitė et al. 2017). However, concerning very old age, some studies have suggested that centenarians may carry biological features of SA because, by far, they have delayed or escaped major illnesses. Therefore, centenarians are less likely to develop Alzheimer’s disease and, as a consequence, may show less brain pathology and therefore fewer strong personality changes (Motta et al. 2005). In this sense, a comparative Japanese study comparing 70 centenarians and 1812 people aged 60–84 years who were residents of Tokyo showed higher O in male and female centenarians and higher C and E in female centenarians (Masui et al. 2006). The results suggested that high scores in these specific personality traits were associated with health-related behaviour, stress reduction, and better adaptation to the challenging problems of the “oldest old” (Gondo et al. 2006; Martin et al. 2006). However, given that biological ageing processes are similar for all people while also highly variable from one individual to another due to genetics, lifestyles, and stressors, personalities may change more strongly for some individuals but stay more stable for others. Common genetic bases may lead to the joint expression of certain personality phenotypes and health behaviours (Deary et al. 2010), and these are likely to accumulate across the lifespan (Dillaway and Byrnes 2009).
Psychological factors may also play an important role in SA. For example, subjective perceptions can lead people to different interpretations of stressors or age-related changes. Emotional reactions to stressful events depend on an individual’s tendency to appraise the situation as challenging or threatening (Lazarus 1993). Specific personality traits have an impact on the subjective appraisal of stressful situations and subsequent affective reactions. For instance, high levels of O, E, and C can predict higher levels of problem-solving and cognitive restructuring, and a high level of N predicts inadequate strategies, such as wishful thinking, withdrawal, and emotion-focused coping (Connor-Smith and Flachsbart 2007). In particular, O—as a factor capturing plasticity and flexibility—helps people perceive ambiguous situations as opportunities and adapt to changes (De Young 2010). By changing the perception of life situations, facilitating adjustment to transitions, and influencing well-being (Bardi et al. 2009), O contributes to positive emotional experiences and increases life satisfaction (Jovanović and Brdarić 2012). Furthermore, being open may be associated with lower egocentrism, which may be useful for reducing vicious cycle of negative thoughts and rumination. We observe in these people a virtuous cycle between experience of positive affect and implementation on the broad-mind strategy of appreciation and distraction (Pavani et al. 2017). Otherwise, individuals who are emotionally stable, organized, and optimistic tend to use more active and functional coping strategies to deal with stressful situations and show greater task persistence when facing adversity. This manner of feeling, thinking, and acting can influence their lives and well-being. On the contrary, high N increases people’s perceptions of stressors as being worse, which has a negative impact on their life satisfaction (Oliver et al. 2010). Indeed, difficulties in regulating emotions, overestimation of threats, underestimation of personal coping, and ineffective forms of emotion-focused coping—such as self-criticism and maladaptive metacognition—that perpetuate awareness of negative self-beliefs lead to perseverative and unproductive worry. In the long term, all this can have negative consequences of ageing.
However, these psychological factors alone are not sufficient to explain well-being or adaptability to life changes. Indeed, environmental contexts such as social factors also play an essential role and represent undeniable resources and contributors to well-being, which can lead to SA. In this sense, social roles and the life experiences and responsibilities that accompany them can shape the life course (Helson et al. 2002). Moreover, the number of close social partners and the quality of relationships are important determinants of SA (Bischop et al. 2006). Social support from family members and sociocognitive interactivity appear to be significant factors in life satisfaction (Deng et al. 2009). In very old age, individuals with more regular in-person and phone contacts were found to value their lives more highly (Jopp et al. 2008), and having more family support was associated with fewer depressive symptoms (Jopp et al. 2016b). On the contrary, social changes such as retirement or partner loss can lead to giving up well-liked activities and feelings of worthlessness or isolation, which influence a person’s behavioural and cognitive preferences. These losses of persons or experiences, characterizing people’s lives in later old age, can lead to deterioration of health and cognition, narrowing of social interaction, and increasingly limited ability to function independently. Significant mood changes such as anxiety, depression, vulnerability to stress, and loss of interest and hope can accompany this stage (Pocnet et al. 2015b). However, specific personality traits can influence the environment in which the individual lives and therefore their well-being. For instance, being extroverted can influence the ways in which these people express their ideas and points of view and, in turn, the groups or associations where they participate in exchanges and discussions (Guillet et al. 2010). A larger social network and more social exchanges can be supportive during difficult situations (Pocnet et al. 2016b). Moreover, E seems to be particularly related to positive events with a strong interpersonal component that influences how happy individuals feel with their life and functioning (Lucas and Diener 2015). Other personality characteristics associated with E such as positive emotions, warmth, energy, sociability, and optimism may help people be more resilient to critical events over their lifespan. On the contrary, in the interpersonal realm, N appears linked to difficulties in regulating emotions, forming hostile appraisals, and reacting to others in ways that deteriorate the relationship quality, resulting in feelings of dissatisfaction (Pocnet et al. 2015a). Hence, to increase well-being across the lifespan, it may be possible to strengthen and stimulate social resources, by developing beneficial personality traits.
Interventions on personality changes could promote successful ageing
Given that personality traits reflect biopsychosocial mechanisms through which individuals are predisposed to engage in healthy or unhealthy patterns of behaviour across the lifespan (Eaton et al. 2012), it is an important question whether it is possible to influence personality characteristics to the better, so that they can support successful development and ageing. When patterns of personality change result in suffering or reduce a person’s quality of life, different intervention approaches could be considered, including psychotherapy (Costa and McCrae 2003) or even pharmacotherapy (Tang et al. 2009). Moreover, studies have shown that a decline in C and E over a 10-year period is associated with worse self-rated health at follow-up (Turiano et al. 2012). To prevent such health deterioration, a personality-related intervention may warrant consideration. For example, mindfulness-based stress reduction decreases N and improves C (Krasner et al. 2009), which in turn has a positive impact on health, including physical problems (especially pain), anxiety, depression, and improved quality of life for older people (Helmes and Ward 2017). Interventions may also make use of findings indicating that serotonin inhibitors in people suffering from depression tend to reduce N and improve E (Tang et al. 2009); thus, using a pharmacological approach could lead to stabilize personality patterns likely to contribute to SA. However, not only might C, N, and E be influenced by intervention programs, but O may also be a good candidate. For instance, one study showed that O improved as a result of a cognitive training in older persons, as the training might have increased their cognitive reserves and improved self-esteem. In turn, feeling competent is likely to increase O (Jackson et al. 2012). Learning to explore the inner world and develop multiple perspectives on the same life situation can lead to flexibility and resilience that, in turn, have benefits for SA.
Psychoeducative interventions regarding personality changes can focus on the relative stability of personality traits (Allemand et al. 2013). For instance, different psychotherapy approaches have been shown to be efficient to support adaptation in cognition, behaviour, and emotion to deal with challenges in old age (Petkus and Wetherell 2013), which could stabilize personality patterns likely to contribute to SA. By addressing psychological aspects such as self-reflection that could influence personality stability or changes, the aim of such an intervention would be to describe origins, mechanisms, and consequences of possible changes in the individual and develop active exercises to stabilize their personality (Allemand et al. 2008). In this sense, Johnson (2009) found that people trained to voluntarily direct their attention to the positive’s aspects of a stressful task, while avoiding the negative ones, persisted in a challenging task for a longer time and experienced less anxiety and less frustration. That way, elderly people learn to maintain a positive mood and positive traits through tumultuous periods and when facing life events related to older age. Promoting stability during these periods of change should be beneficial because it could help individuals retain a consistent and coherent picture of themselves despite external and internal changes (Allemand et al. 2013).
According to scarce research that suggests individuals are able to perceive their trait changes (Robins Wahlin and Byrn 2011), they may become aware of how their personality repertoire adapts within difficult life experiences or during the ageing process, in order to take measures to revert or stabilize. Sometimes, positive personality changes may be induced more or less intentionally (Roberts et al. 2006): Firstly, and perhaps most importantly, individuals are responsive to the rewards and punishments of a given setting, and it is possible that long-term exposure to specific contingencies may produce lasting personality changes (Laub and Sampson 2003); thus, people should learn to be less influenced by them. Secondly, self-reflection may lead to lasting positive personality changes due to a considerable amount of deliberate attention to the self. Indeed, a belief in the power of self-reflection to promote change is the essence of, for example, insight-oriented psychotherapy (Rogers 1980) or hypnotherapy (Erickson and Rossi 1989). Thirdly, observing others might serve as a model for personality changes through social learning (Bandura 1977). For instance, observing people with higher C could lead to becoming more alert to how positive outcomes could be promoted. Thus, perceptions by others or reflected appraisals may create personality changes (Jaret et al. 2005). Nevertheless, a strong motivation to change might be a necessary ingredient for the success of many of these psychosocial mechanisms which could contribute to personality change. In all cases, these experiences can have lasting effects on the development of a balanced and adaptable personality that, in turn, could have a positive impact on health and subjective well-being and consequently lead to SA (Cho et al. 2015).
Discussion
This literature review suggests personality play an important role in SA, proposing that specific personality traits are the basis for mechanisms that contribute to positive functioning in terms of health, cognition, social relations, and well-being across the lifespan. Although genetic factors may be responsible for personality and SA, our findings further suggest that the lifelong contributions of behavioural styles (e.g. health behaviours, social interaction styles), emotions (e.g. emotional stability, optimism, motivations), and cognitive tendencies (e.g. perception and interpretation, selection of environments and comparison frames) may influence how individuals develop over their lifespan and how they age. Our findings from this review suggest that the investigation of personality as a determinant of SA deserves further attention and could open new avenues of research. In this context, it is important to develop an integrative framework in which the effects of biological, psychological, and social factors as underlying mechanisms of personality development can be considered simultaneously in relation to the lifespan development. Choosing healthy behaviours in life might become from an awareness of oneself, contributing thus to a meaning of one’s own lives. Staying physically, socially, and psychologically active throughout life and marvelling at things in life are clearly related to personality profiles that are conscientious, open, and sociable (Baek et al. 2016; Chan et al. 2018; Gawronski et al. 2016). Although a causal relationship cannot be established from these findings, such personality dimensions seem likely to contribute to positive health-related behaviours, which in turn lead to higher subjective well-being and better objective health. In particular, the self-discipline facet of C can lead to a high level of functioning with maintenance, enhancement, or limited impairment of a person’s capacities, thus allowing the individual an optimal and continuous development (Moffitt et al. 2011), despite developing age-related pathologies. For example, it is well known that practising regular physical exercises has substantial effects on the prevention of cardiovascular disease (Sveaas et al. 2017), cancer (Zelek et al. 2010), and Alzheimer’s disease (Paillard et al. 2015). However, if C seems to be a protective factor against disease, it is helpful to differentiate the healthy C that promotes SA from the extreme inflexibility or compulsive behaviour that may represent personality disorder as a risk factor of mortality. Furthermore, O is associated with mechanisms of emotional reflection and metacognition and, therefore, is likely to contribute to maintaining a high quality of life (Leonard and Harvey 2007). To further explore the indirect effects of personality on SA, longitudinal studies are needed to provide answers on the relationship between O, cognitive functions, and health outcomes. Associated with a high dopamine level, E reflects a person’s behavioural tendency for exploration and engagement in possibilities, allowing adaptation to social challenges (De Young 2010). However, it would be useful to consider studies that differentiate healthy E, as a protective factor for SA, from unhealthy E—defined by very high expectations of overestimation in adaptation and the underestimation of certain critical life events (Baek et al. 2016)—as a possible risk of pathological ageing. Over time, some people may become more resilient and adapt more easily to stressful life events thanks to the development of their ability to regulate emotions in such situations (Pocnet et al. 2016b), thus contributing to a process of continuous development. Therefore, future longitudinal studies should evaluate interventions designed to enhance emotional stability as an important determinant of SA.
Conclusion
Given that every effort is needed to disentangle the complex interplay of the many factors contributing to successful development across the lifespan, investigating the impact of personality on adaptation and ageing in more detail appears to be very promising when conjointly using biological, psychological, and social approaches. In terms of methodology, multifactorial interaction designs can be used to better understand how the five personality dimensions or specific facets might influence SA. Moreover, considering the individual differences in social and economic inequalities contexts might provide more details for solving the ageing puzzle. Therefore, it is important to integrate each of these factors into interdisciplinary studies to form an ever-wider understanding. The application of such methods can offer comprehensive information to be used in psychotherapeutic or pharmacotherapeutic interventions. Improving the knowledge of personality’s complexity and changes would also empower clinicians to provide therapies that are centred more on individual differences to improve the daily lives of people who are suffering and facilitate more sustainable well-being.
References
Allemand M, Zimprich D, Hendriks AAJ (2008) Age differences in five personality domains across the life span. Dev Psychol 44:758–770
Allemand M, Steiger AE, Hill PL (2013) Stability of personality traits in adulthood: mechanisms and implications. GeroPsych 26:51–53
Andersen SL, Sebastiani P, Dworkis DA, Feldman L, Perls TT (2012) Health span approximates life span among many super centenarians: compression of morbidity at the approximate limit of life span. J Gerontol A Biol Sci Med Sci 67:633–636
Araújo L, Teixeira L, Ribeiro O, Paúl C (2018) Objective vs. subjective health in very advanced ages: looking for discordance in centenarians. Front Med. https://doi.org/10.3389/fmed.2018.00189
Baek Y, Martin P, Siegler IC, Davey A, Poon LW (2016) Personality traits and successful aging: findings from the Georgia Centenarian Study. Int J Aging Hum. https://doi.org/10.1177/0091415016652404
Bandura A (1977) Social learning theory. Prenctice-Hall, Englewood Cliffs
Bardi A, Guerra VM, Ramdeny GSD (2009) Openness and ambiguity intolerance: their differential relations to well-being in the context of an academic life transition. Pers Individ Differ. https://doi.org/10.1016/j.paid.2009.03.003
Berg AI, Johansson B (2013) Personality change in the oldest-old: is it a matter of compromised health and functioning? J Personal. https://doi.org/10.1111/jopy.12030
Bischop AJ, Martin P, Poon L (2006) Happiness and congruence in older adulthood: a structural model of life satisfaction. Aging Ment Health. https://doi.org/10.1080/13607860600638388
Bogg T, Roberts BW (2004) Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychol Bull 130:887–919. https://doi.org/10.1037/0033-2909.130.6.887
Brissette I, Scheier MF, Carver CS (2002) The role of optimism in social network development, coping, and psychological adjustment during a life transition. J Personal Soc Psychol. https://doi.org/10.1037//0022-3514.82.1.102
Brummett BH, Babyak MA, Williams RB, Barefoot JC, Costa PT Jr, Siegler IC (2006) Prediction of all- cause mortality by the Minnesota multiphasic personality inventory optimism-pessimism scale scores. Mayo Clin Proc 81:1541–1544. https://doi.org/10.4065/81.12.1541
Cappola AR, Xue QL, Ferrucci L, Guralnik JM, Volpato S, Fried LP (2003) Insulin-like growth factor I and interleukin-6 contribute synergistically to disability and mortality in older women. J Clin Endocrinol Metab 88:2019–2025. https://doi.org/10.1210/jc.2002-021694
Caspi A, Roberts BW, Shiner RL (2005) Personality development: stability and change. Annu Rev Psychol 56:453–484. https://doi.org/10.1146/annurev.psych.55.090902.141913
Chan BCL, Luciano M, Lee B (2018) Interaction of physical activity and personality in the subjective wellbeing of older adults in Hong Kong and the United Kingdom. Behav Sci. https://doi.org/10.3390/bs8080071
Chapman BP, Fiscella K, Kawachi I, Duberstein P (2010) Personality, socioeconomic status, and all-cause mortality in the United States. Am J Epidemiol 171:83–92. https://doi.org/10.1093/aje/kwp323
Chapman BP, Roberts B, Duberstein P (2011) Personality and longevity: knowns, unknowns, and implications for public health and personalized medicine. J Aging Res. https://doi.org/10.4061/2011/759170
Chapman B, Duberstein P, Tindle HA, Sink KM, Robins J et al (2012) Personality predicts cognitive function over 7 years in older persons. Am J Geriatr Psychiatry 20:612–621. https://doi.org/10.1097/JGP.0b013e31822cc9cb
Cho J, Martin P, Poon LW (2015) Successful aging and subjective well-being among oldest-old adults. Gerontologist 55:132–143. https://doi.org/10.1093/geront/gnu074
Connor-Smith JK, Flachsbart C (2007) Relations between personality and coping: a meta-analysis. J Personal Soc Psychol. https://doi.org/10.1037/0022-3514.93.6.1080
Cosco TD, Prina AM, Perales J, Stephan BCM, Brayne B (2014) Operational definitions of successful aging: a systematic review. Int Psychogeriatr. https://doi.org/10.1017/S1041610213002287
Costa PT, McCrae RR (1992) Revised NEO Personality Inventory (NEO-PI-R) and NEO-Five-Factor (NEO-FFI) professional manual. Psychological Assessment Resources, Odessa
Costa PT Jr, McCrae RR (2003) Personality in adulthood: a five factor theory perspective, 2nd edn. Guilford Press, New York
Costa PT Jr, McCrae RR (2006) Age changes in personality and their origins. Psychol Bull 132:26–28. https://doi.org/10.1037/0033-2909.132.1.26
Dahl AA (2010) Link between personality and cancer. Future Oncol. https://doi.org/10.2217/fon.10.31
de Moor MHM, Costa PT, Terracciano A, Krueger RF, de Geus EJC et al (2012) Meta-analysis of genome-wide association studies for personality. Mol Psychiatry 17(3):337–349. https://doi.org/10.1038/mp.2010.128
De Young CG (2010) Personality neuroscience and the biology of traits. Soc Personal Psychol Compass 4:1165–1180. https://doi.org/10.1111/j.1751-9004.2010.00327.x
Deary IJ, Weiss AW, Batty GD (2010) Intelligence and personality as predictors of illness and death: how researchers in differential psychology and chronic disease epidemiology are collaborating to understand and address health inequalities. Psychol Sci Public Interests 11:53–79. https://doi.org/10.1177/1529100610387081
Deng J, Hu J, Wu W, Dong B, Wu H (2009) Subjective well-being, social support, and age-related functioning among the very old in China. Int J Geriatr Psychiatry 25:697–703. https://doi.org/10.1002/gps.2410
Dillaway HE, Byrnes M (2009) Reconsidering successful aging: a call for renewed and expanded academic critiques and conceptualizations. J Appl Gerontol 28:702–722. https://doi.org/10.1177/0733464809333882
Distel MA, Trull TJ, Willemsen G, Vink JM, Derom CA, Lynskey M, Martin NG, Boomsma DI (2009) The five-factor model of personality and borderline personality disorder: a genetic analysis of comorbidity. Biol Psychiatry 66:1131–1138. https://doi.org/10.1016/j.biopsych.2009.07.017
Donnellan MB, Conger KJ, McAdams KK, Neppl TK (2009) Personal characteristics and resilience to economic hardship and its consequences: conceptual issues and empirical illustrations. J Personal 77:1645–1676. https://doi.org/10.1111/j.1467-6494.2009.00596.x
Duberstein PR, Chapman BP, Tindle HA et al (2011) Personality and risk for Alzheimer’s disease in adults 72 years of age and older: a 6-year follow-up. Psychol Aging 26:351–362. https://doi.org/10.1037/a0021377
Eaton NR, Krueger RF, South SC, Gruenewald TL, Seeman TE, Roberts BW (2012) Genes, environments, personality, and successful aging: toward a comprehensive developmental model in later life. J Gerontol A Biol Sci Med Sci. https://doi.org/10.1093/gerona/gls090
Edmonds GW (2008) Is character fate or is there hope to change my personality yet? Soc Personal Psychol Compass 2:399–413. https://doi.org/10.1111/j.1751-9004.2007.00037.x
Ellenbogen MA, Ostiguy CS, Hodgins S (2010) Intergenerational effects of high neuroticism in parents and their public health significance. Am Psychol. https://doi.org/10.1037/a0018512
Erickson MH, Rossi EL (1989) The February man: evolving consciousness and identity in hypnotherapy. Brunner, New York
Erickson KI, Kim JS, Suever BL, Voss MV, Francis M, Kramer AF (2008) Genetic contributions to age-related decline in executive function: a 10-year longitudinal study of COMT and BDNF polymorphisms. Front Hum Neurosci. https://doi.org/10.3389/neuro.09.011.2008
Fry PS, Debats DL (2009) Perfectionism ad the five-factor personality as predictors of mortality in older adults. J Health Psychol 14:513–524. https://doi.org/10.1177/1359105309103571
Gawronski KAB, Kim ES, Langa KM, Kubzansky LD (2016) Dispositional optimism and incidence of cognitive impairment in older adults. Psychosom Med 78(7):819–828. https://doi.org/10.1097/PSY.0000000000000345
Givens JL, Frederick M, Silverman L, Anderson S, Senville J et al (2009) Personality of traits of centenarians’offspring. Am Geriatr Soc 57:683–685. https://doi.org/10.1111/j.1532.5415.2009.02189
Gondo Y, Hirose N, Arai Y, Inagaki H, Masui Y, Yamamura K et al (2006) Functional status of centenarians in Tokyo, Japan: developing better phenotypes of exceptional longevity. J Gerontol A Biol Sci Med Sci 61:305–310. https://doi.org/10.1093/gerona/61.3.305
Gross JJ, John OP (2003) Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Personal Soc Psychol 85:348–362. https://doi.org/10.1037/0022-3514.85.2.348
Gruenewald TL, Seeman TE, Ryff CD, Karlamangla AS, Singer BH (2006) Combinations of biomarkers predictive of later life mortality. Proc Natl Acad Sci USA 103:14158–14163. https://doi.org/10.1073/pnas.0606215103
Guillet L, Hermand D, Mullet E (2010) The importance of social support in workers’ lay conceptualizations of stress. Swiss J Psychol. https://doi.org/10.1024/1421-0185/a000007
Harris MA, Brett CE, Johnson W, Deary IJ (2016) Personality stability from age 14 to age 77 years. Psychol Aging. https://doi.org/10.1037/pag0000133
Helmes E, Ward BG (2017) Mindfulness-based cognitive therapy for anxiety symptoms in older adults in residential care. Aging Ment Health 21:272–278. https://doi.org/10.1080/13607863.2015.1111862
Helson R, Jones C, Kwan VS (2002) Personality change over 40 years of adulthood: hierarchical linear modeling analyses of two longitudinal samples. J Personal Soc Psychol 83:752–766. https://doi.org/10.1037/0022-3514.83.3.752
Henriques-Calado J, Duarte-Silva ME (2020) The predictive power of personality through psychopathology in Alzheimer’s disease: a control study of self-report and baseline retrospective assessment. Psychol Health Med. https://doi.org/10.1080/13548506.2020.1734218
Ihle A, Jopp D, Oris M, Fagot D, Kliegel M (2016) Investigating discontinuity of age relations in cognitive functioning, general health status, activity participation, and life satisfaction between young-old and old-old age. Int J Env Res Public Health. https://doi.org/10.3390/ijerph13111092
Jackson JJ, Hill PL, Payne BR, Roberts BW, Stine-Morrow EAL (2012) Can an old dog learn (and want to experience) new tricks? Cognitive training increases openness to experience in older adults. Psychol Aging 27:286–292. https://doi.org/10.1037/a0025918
Jaret C, Reitzes DC, Shapkina N (2005) Reflected appraisals and self-esteem. Sociol Perspect 48(3):403–419. https://doi.org/10.1525/sop.2005.48.3.403
Johnson DR (2009) Goal-directed attentional deployment to emotional faces and individual differences in emotional regulation. J Res Personal 43:8–13
Johnson W, McGue M, Krueger RF (2005) Personality stability in late adulthood: a behavioural genetic analysis. J Personal 73:523–551. https://doi.org/10.1111/j.1467.6494.2005.00319.x
Jokela M, Hakulinen C, Singh-Manoux A, Kivimäki M (2014) Personality change associated with chronic diseases: pooled analysis of four prospective cohort studies. Psychol Med 44:2629–2640. https://doi.org/10.1017/S0033291714000257
Jonassaint CR, Boyle SH, Williams RB, Mark DB, Siegler IC, Barefoot JC (2007) Facets of openness predict mortality in patients with cardiac disease. Psychosom Med 69:319–322. https://doi.org/10.1097/PSY.0b013e318052e27d
Jopp DS, Rott C, Oswald F (2008) Valuation of life in old and very old age: the role of sociodemographic, social, and health resources for positive adaptation. Gerontologist 48(5):646–658. https://doi.org/10.1093/geront/48.5.646
Jopp D, Wozniak D, Damarin AK, de Feo M, Jung S, Jeswani S (2015) How could lay perspectives on successful aging complements scientific theory? Findings from a U.S. and a German Lifespan Sample. Special issue: successful aging. Gerontologist 55:91–106. https://doi.org/10.1093/geront/gnu059
Jopp D, Boerner K, Ribeiro O, Rott C (2016a) Life at age 100: an international research agenda a for centenarian studies. J Aging Soc Policy 28(3):133–147. https://doi.org/10.1080/08959420.2016.1161693
Jopp DS, Park MKS, Lehrfeld J, Paggi ME (2016b) Physical, cognitive, social and mental health in near-centenarians and centenarians living in New York City: findings from the Fordham Centenarian Study. BMC Geriatr 16(1):1–10
Jovanović V, Brdarić D (2012) Did curiosity kill the cat? Evidence from subjective wellbeing in adolescents. Personal Individ Differ 52(3):380–388
Judge TA, Erez A, Bono JE, Thoresen CJ (2002) Are measures of self-esteem, neuroticism, locus of control, and generalized self-efficacy indicators of a common core construct? J Personal Soc Psychol 83:693–710. https://doi.org/10.1037/0022-3514.83.3.693
Jung CG (1981) The structure and dynamics of the psyche, 5th edn. Princeton University Press, Princeton
Kato K, Zweig R, Schechter CB, Verghese J, Barzilai N, Atzmon G (2013) Personality, self-rated health, and cognition in centenarians: do personality and self-rated health relate to cognitive function in advanced age? Aging 5:183–191. https://doi.org/10.18632/aging.100545
Kern ML, Friedman HS (2008) Do conscientious individuals live longer? A quantitative review. Health Psychol 27:505–512. https://doi.org/10.1037/0278-6133.27.5.505
Kern ML, Friedman HS (2011) Personality and pathways of influence on physical health. Soc Personal Psychol Compass 5:76–87. https://doi.org/10.1111/j.1751-9004.2010.00331.x
Krasner MS, Epstein RM, Beckman H et al (2009) Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA 302:1284–1293. https://doi.org/10.1001/jama.2009.1384
Lahey BB (2009) Public health significance of neuroticism. Am Psychol 64:241–256. https://doi.org/10.1037/a0015309
Laub JH, Sampson RJ (2003) Shared beginnings, divergent lives: delinquent boys to age 70. Harvard University Press, Cambridge
Lautenschlager NT, Förstl H (2007) Personality change in old age. Curr Opin Psychiatry 20:62–66. https://doi.org/10.1097/yco.0b013e3280113d09
Lazarus RS (1993) From psychological stress to the emotions: a history of changing outlooks. Annu Rev Psychol 44:1–21. https://doi.org/10.1146/annurev.ps.44.020193.000245
Leonard NH, Harvey M (2007) The trait of curiosity as a predictor of emotional intelligence. J Applied Soc Psychol. https://doi.org/10.1111/j.1559-1816.2007.00226.x
Lucas RE, Diener E (2015) Personality and subjective well-being: current issues and controversies. In: Mikulincer M, Shaver PR, Cooper ML, Larsen RJ (eds) APA handbook of personality and social psychology. Personality processes and individual differences, vol 4. American Psychological Association, Washington, pp 577–599. https://doi.org/10.1037/14343-026
Martin P, da Rosa G, Siegler I, Davey A, MacDonald M, Poon LW (2006) Personality and longevity: findings from the Georgia Centenarian Study. Age 28:343–352. https://doi.org/10.1007/s11357-006-9022-8
Martin P, Kelly N, Kahana B, Kahana B, Willcox BJ, Willcox DC, Poon LW (2015) Defining successful aging: a tangible or elusive concept? Gerontologist 55:14–25. https://doi.org/10.1093/geront/gnu044
Masui Y, Gondo Y, Inagaki H, Hirose N (2006) Do personality characteristics predict longevity? Findings from Tokyo Centenarian Study. Age. https://doi.org/10.1007/s11357-006-9024-6
McCrae RR, Costa PT Jr (2008) The five-factor theory of personality. In: John OP, Robins RW, Pervin LA (eds) Handbook of personality: theory and research, 3rd edn. Guilford, New York, pp 159–181
Moffitt TE, Arseneault D, Belsky D et al (2011) A gradient of childhood self-control predicts health, wealth, and public safety. PNAS USA 108:2693–2698. https://doi.org/10.1073/pnas.1010076108
Morizot J, Le Blanc M (2005) Searching for a developmental typology of personality and its relations to antisocial behavior: a longitudinal study of a representative sample of men. J Personal 73:139–182. https://doi.org/10.1111/j.1467-6494.2004.00307.x
Motta M, Bennati E, Ferlito L, Malaguarnera M, Motta L (2005) Successful aging in centenarians: myths and reality. Arch Gerontol Geriatr. https://doi.org/10.1016/j.archger.2004.09.002
Möttus R, Johnson W, Deary IJ (2011) Personality traits in old age: measurement and rank-order stability and some mean-level change. Psychol Aging. https://doi.org/10.1037/a0023690
Oliver JE, Mansell A, Jose PE (2010) A longitudinal study of the role of negative affectivity on the work stressor–strain process. Int J Stress Manag 17:56–77. https://doi.org/10.1037/a0017696
Ouanes S, Popp J (2019) High cortisol and the risk of dementia and Alzheimer’s disease: a review of the literature. Front Aging Neurosci. https://doi.org/10.3389/fnagi.2019.00043
Paillard T, Rolland Y, de Souto Barreto P (2015) Protective effects of physical exercise in Alzheimer’s disease and Parkinson’s disease: a narrative review. J Clin Neurol. https://doi.org/10.3988/jcn.2015.11.3.212
Pavani J-B, Le Vigouroux S, Kop J-L, Congard A, Dauvier B (2017) A network approach to affect regulation dynamics and personality trait-induced variations: extraversion and neuroticism moderate reciprocal influences between affect and affect regulation strategies. Eur J Personal. https://doi.org/10.1002/per.2109
Pelle AJ, Pedersen SS, Schiffer AA, Szabo B, Widdershoven JW, Denollet J (2010) Psychological distress and mortality in systolic heart failure. Circ Heart Fail 3:261–267. https://doi.org/10.1161/CIRCHEARTFAILURE.109.871483
Petkus AJ, Wetherell JL (2013) Acceptance and commitment therapy with older adults: rationale and considerations. Cogn Behav Pract 20:47–56. https://doi.org/10.1016/j.cbpra.2011.07.004
Ploubidis GB, Grundy E (2009) Personality and all-cause mortality: evidence for indirect links. Personal Individ Differ. https://doi.org/10.1016/j.paid.2009.02.022
Pocnet C, Rossier J, Antonietti J-P, von Gunten A (2011) Personality changes in patients with beginning Alzheimer disease. Can J Psychiatry 56:408–417. https://doi.org/10.1177/070674371105600704
Pocnet C, Antonietti J-P, Massoudi K, Györkös C, Becker J, de Bruin G, Rossier J (2015a) Influence of individual characteristics on work engagement and job stress in a sample of national and foreigner workers in Switzerland. Swiss J Psychol 74(1):17–27. https://doi.org/10.1024/14210185/a000146
Pocnet C, Antonietti J-P, Rossier J, Donati A, Popp J, von Gunten A (2015b) Behavioral and psychological symptoms and cognitive decline in patients with amnestic MCI and mild AD: a two-year follow-up study. Int Psychogeriatr. https://doi.org/10.1017/s1041610214000283X
Pocnet C, Antonietti J-P, Rossier J, Strippoli M-P, Glaus J, Preisig M (2016a) Personality, tobacco consumption, physical inactivity, obesity markers, and metabolic components as risk factors for cardiovascular disease in the general population. Psychol Health Med 22(8):932–939. https://doi.org/10.1080/13548506.2016.1255767
Pocnet C, Antonietti J-P, Strippoli M-P, Glaus J, Preisig M, Rossier J (2016b) Influence of major life events, perceived social support, and personality traits on individual’s quality of life. Qual Life Res 25(11):2897–2908. https://doi.org/10.1007/s11136-016-1296-4
Pocnet C, Antonietti J-P, Handschin P, Massoudi K, Rossier J (2018) The many faces of personality: the DSM-5 dimensional and categorical models and the five-factor model. Personal Individ Differ 121:11–18. https://doi.org/10.1016/j.paid.2017.09.005
Pruchno R, Heid A, Wilson Genderson M (2015) Resilience and successful aging: aligning complementary constructs using a life course approach. Psychol Inq 26:200–207. https://doi.org/10.1080/1047840X.2015.1010422
Ribeiro O, Teixeira L, Araujo L, Afonso RM, Pachana N (2014) Predictors of anxiety in centenarians: health, economic factors, and loneliness. Int Psychogeriatr 27:1167–1176. https://doi.org/10.1017/S1041610214001628
Roberts BW, Walton KE, Viechtbauer W (2006) Patterns of mean-level change in personality traits across the life course: a meta-analysis of longitudinal studies. Psychol Bull. https://doi.org/10.1037/0033-2909.132.1.1
Roberts BW, Chernyshenko OS, Stark S, Goldberg LR (2007) The structure of conscientiousness: an empirical investigation based on seven major personality questionnaires. Pers Psychol. https://doi.org/10.1111/j.1744-6570.2005.00301.x
Robins Wahlin TB, Byrn GJ (2011) Personality changes in Alzheimer’s disease: a systematic review. Int J Geriatr Psychiatry 26:1019–1029. https://doi.org/10.1002/gps.2655
Rogers CR (1980) A way of being. Houghton Mifflin, Boston
Scheier MF, Carver CS, Bridges MW (1994) Distinguishing optimism from neuroticism, trait anxiety, self-mastery, and self-esteem: a re-evaluation of the life orientation test. J Personal Soc Psychol 67:1063–1078
Segerstrom SC (2007) Optimism and resources: effects on each other and on health over 10 years. J Res Personal. https://doi.org/10.1016/j.jrp.2006.09.004
Segerstrom SC (2020) Personality and incident Alzheimer’s disease: theory, evidence, and future directions. J Gerontol B. https://doi.org/10.1093/geronb/gby063
Shah P, Harris AJL, Bird G, Catmur C, Hahn U (2016) A pessimistic view of optimistic belief updating. Cogn Psychol 90:71–127. https://doi.org/10.1016/j.cogpsych.2016.05.004
Smith SM, Vale WW (2006) The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues Clin Neurosci 8:383–395
Solberg Ness L, Segerstrom SC (2006) Dispositional optimism and coping: a meta-analytic review. Personal Soc Psychol Rev 10:235–251
Srivastava K, Das RC (2013) Personality pathways of successful ageing. Ind Psychiatry J 22:1–3. https://doi.org/10.4103/0972-6748.123584
Sutin AR, Ferrucci L, Zonderman AB, Terracciano A (2011) Personality and obesity across the adult lifespan. J Personal Soc Psychol 101:579–592. https://doi.org/10.1037/a0024286
Sveaas SH, Smedslund G, Hagen KB, Dagfinrud H (2017) Effect of cardiorespiratory and strength exercises on disease activity in patients with inflammatory rheumatic diseases: a systematic review and meta-analysis. Br J Sports Med. https://doi.org/10.1136/bjsports-2016-097149
Tan J, Ward L, Ziaian T (2011) Comparing cultural definitions of successful ageing. J Appl Psychol 7:15–20. https://doi.org/10.7790/ejap.v7i1.227
Tang TZ, De Rubeis RJ, Hollon SD, Amsterdam J, Shelton R, Schalet B (2009) Personality change during depression treatment: a placebo-controlled trial. Arch Gen Psychiatry 66:1322–1330. https://doi.org/10.1001/archgenpsychiatry.2009.166
Tautvydaitė D, Antonietti JP, Henry H, von Gunten A, Popp J (2017) Relations between personality changes and cerebrospinal fluid biomarkers of Alzheimer’s disease pathology. J Psychiatr Res 90:12–20. https://doi.org/10.1016/j.jpsychires.2016.12.024
Terracciano A, Costa PT Jr (2004) Smoking and the five-factor model of personality. Addiction 99:427–481. https://doi.org/10.1111/j.1360-0443.2004.00687.x
Terracciano A, Sutin AR (2019) Personality and Alzheimer’s disease: an integrative review. Personal Disord. https://doi.org/10.1037/per0000268
Terracciano A, McCrae RR, Brant LJ, Costa PT Jr (2005) Hierarchical linear modelling analyses of the NEO-PI-R scales in the Baltimore longitudinal study of aging. Psychol Aging 20:493–506. https://doi.org/10.1037/0882-7974.20.3.493
Terracciano A, Sanna S, Uda M, Deiana B, Usala G, Busonero F et al (2010) Genome-wide association scan for five major dimensions of personality. Mol Psychiatry 15:647–656. https://doi.org/10.1038/mp.2008.113
Turiano NA, Spiro A, Mcroczek DK (2012) Openness to experience and mortality in men: analysis of trait and facets. J Aging Health 24:654–672. https://doi.org/10.1177/0898264311431303
Weis A, Costa PT Jr (2005) Domain and facet personality predictors of all-cause mortality among medicare patients aged 65 to 100. Psychos Med 67:724–733. https://doi.org/10.1097/01.psy.0000181272.58103.18
Zelek L, Bouillet T, Latino-Martel P, Pecollo N, Barrandon E, Czernichow S, Galan P, Hercberg S (2010) Lifestyle and breast cancer: what advice for the management of post-cancer? Oncologie. https://doi.org/10.1007/s10269-010-1878-7
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Responsible editor: Marja J. Aartsen.
Rights and permissions
About this article

Cite this article
Pocnet, C., Popp, J. & Jopp, D. The power of personality in successful ageing: a comprehensive review of larger quantitative studies. Eur J Ageing 18, 269–285 (2021). https://doi.org/10.1007/s10433-020-00575-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10433-020-00575-6