
Abstract
The study aimed to investigate the role of social activities, social networks as well as socioeconomic status (SES) in influencing some aspects of cognitive functioning (immediate and delayed verbal recall tests and semantic verbal fluency) in elderly people over time. This analysis was conducted on a sample of 31,954 healthy elderly people (58% female, mean age 65.54 ± 9.74) interviewed in both the fourth and sixth waves of the Survey on Health, Aging and Retirement in Europe (SHARE), in 2011 and 2015. A structural equation model with measurement component was used to assess the relationship between cognitive function, social life and SES over time. Multilevel ordinal logistic regression was applied to explain satisfaction with social network in relation to different types of social network across countries. Being equipped with good cognitive skills did not seem to be predictive of their maintenance over time (latent coefficient = 0.24, p value = 0.34). On the contrary, the subject’s social and participatory life, understood as satisfying one’s social network and engaging in diversified non-professional social activities, seemed to play a crucial role in the maintenance of cognitive functions in the elderly (latent coefficient = 3.5, p value = 0.03). This research suggests that a socially active and participatory lifestyle mitigates the effects of the physiological process of brain aging.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The progressive aging of the population requires the implementation of appropriate and innovative strategies for mitigating the adverse effects of this process on both the individual and the social and economic system. Although one of the main effects of aging is undoubtedly linked to the decline in cognitive functions, it should be stressed that this decline, which concerns both functional and neurological aspects, even if cannot be avoided, can be significantly postponed (Fillit et al. 2002; Park et al. 2003; Adam et al. 2013; Boots et al. 2015; Miceli and Gangemi 2011, Misuraca et al. 2017; Smart et al.2014). Nowadays, there is a wide consensus among researchers that cognitive functions can be enhanced and maintained through protective factors, which are linked to lifestyle (Adam et al. 2013; Andel et al. 2015; Bourassa et al. 2017; Hertzog et al. 2008; Vásquez-Amézquita 2016).
In this context, the concept of “cognitive reserve,” developed by Stern (2003, 2007, 2009) plays an important role. It states that some aspects of experience, such as education, professional status, social networking, and lifestyle and leisure activities, provide a reserve that can explain the resilience of elderly people when facing neuropathological changes. In this way, it acts as a cognitive protective factor associated with normal aging processes (La Rue 2010; Vásquez-Amézquita 2016; Singh-Manoux et al. 2011; Jefferson et al. 2011).
Among the factors that foster the reserve accumulation, an active and participatory lifestyle is of primary importance. In this vein, social participation is defined as the involvement of the individual in various social activities (Berkman et al. 2000), such as religious groups, volunteer groups, social or sports clubs. Positive correlations have been found between participation in social activities and mental health (Croezen et al. 2015), physical health (Lindström et al. 2004) and well-being (Vozikaki et al. 2017). On the contrary, the perceived social isolation (deep sense of solitude) has been associated with a greater risk of cognitive dysfunction (Cacioppo and Hawkley 2009). Some longitudinal studies have highlighted how loneliness, i.e., the absence of social bonds, significantly increased the risk of cognitive decline (Gow et al. 2007; Tilvis et al. 2004; Wilson et al. 2007). Other longitudinal studies have shown that an active lifestyle was positively associated with the maintenance of various cognitive abilities (Hultsch et al. 1999; Bourassa et al. 2017). Of note, James et al. (2011) found that socially active people had a global cognitive decline 70% lower than that of socially inactive people, on average, in 5 years. Analogously, Brown et al. (2016), using data from the Victoria Longitudinal Study, found that the engagement in social activities for older adults was related to participation in everyday cognitive activities and in turn to better cognitive performance. Conversely, lack of association between social activity and cognitive functioning along time was found in other studies (McGue and Christensen 2007; Aartsen et al. 2002; Green et al. 2008), which used a global measure of cognitive functioning and a variety of specific cognitive tasks.
Through engagement in social activities, individuals can develop and broaden their own social ties by providing an additional cognitive resource that may reduce the effects of age on cognitive abilities. Social networks including both family members and friends are a further psychosocial factor capable of preserving cognitive functions (Miller and Lachman 2000; Seeman et al. 2001; Colcombe and Kramer 2003; Béland et al. 2005), of influencing the elderly’s life satisfaction (Chan and Lee 2006; Groot et al. 2007; Litwin and Stoeckel 2013; Rafnsson et al. 2015) and of promoting virtuous and healthy behaviors at all ages (Matranga et al. 2017).
Indeed, the intensity and quality of social relationships have been demonstrated to be significantly associated with better health (Pinquart and Sörensen 2000; Dominguez and Arford 2010; Garcia et al. 2005; McLaughlin et al. 2010), greater use of health and social services (Bowling et al. 1991; Litwin 2004), and greater longevity (Brown et al. 2005; Eriksson et al. 1999). In particular, the “size” (number of family members and friends in the network) and the “composition” (the percentage of friends within the total number of people) of the social network seem to have an effect on life satisfaction of the elderly (Tomini et al. 2016). For example, Van der Horst and Coffé (2012) showed that a higher frequency of contacts and a greater percentage of friends in the network are associated with less stress and better health. Thus, by analyzing the different types of networks on the basis of the composition (for example, social networks composed exclusively of family members or friends), Fiori et al. (2006) found that elderly people in the networks that did not include the presence of friends had depressive symptoms. Socially deprived elderly people are more likely to develop disabilities and at a greater risk of mortality (Andrew et al. 2008). The underlying mechanisms involved include physiological factors, such as stress hormones, immune function, and inflammatory processes that may be more developed in those individuals with low social support or living in a condition of social isolation (Berkman et al. 2000).
Litwin and Stoeckel (2015) have investigated whether and to what extent social network and activity participation are associated with cognitive functions. Activity participation was found to be positively associated with word recall and self-rated memory more than social network and activity participation interacted significantly with social networking.
There are a few open questions in the literature. Firstly, findings from longitudinal studies concerning the relationship between social participation and cognitive functioning are not consistent. Secondly, even if protective factors related to the lifestyle can be considered modifiable for the whole population, they cannot be easily changed for elderly. In fact, it often happens that the partner has died, children may live far away and physical constraints may highly limit social participation. However, it is possible that different welfare systems can promote a participating lifestyle in different ways. Therefore, the contribution of this paper to this debate regards the following points:
-
(a)
Does higher sociality, expressed through social network and the involvement in social activities, predict higher cognitive functioning of an individual?
-
(b)
Does the socioeconomic status of an individual contribute to define his/her own cognitive functioning not only in the concurrent time but also in the prospective?
-
(c)
Are family-type networks associated with higher satisfaction of social network?
-
d)
Does the welfare system of the living country contribute to the individual’s sociality?
To respond to these queries, we will examine three cognitive tasks, two memory and one executive, as specific aspects of cognition. In fact, these tasks are among those suffering more from the effects of age, showing a constant decline both in healthy subjects and in subjects affected by Alzheimer’s disease (Henry and Crawford 2004; Laws et al. 2010; Haugrud et al. 2011). Secondly, numerous studies highlight how these cognitive tasks are strongly related to the quality of life of the elderly, to their well-being and to the participation in social activities (James et al. 2011; Bourassa et al. 2017; Fu et al. 2018). We will define the structure of relationships between social activities and networks, socioeconomic status (SES) and the examined cognitive functions through a structural equation modeling approach. As a secondary aim, we will outline types of social networks across countries and will establish different satisfaction levels related with these types.
Methods and data
The sample
Data from the fourth (year = 2011) and sixth (year = 2015) waves of the Survey on Health, Aging and Retirement in Europe (SHARE) are used for this study. The SHARE survey is a pan-European interdisciplinary dataset of microdata on health, socioeconomic status and social and family networks of people aged 50 years and over, covering most of the European Union (Börsch-Supan et al. 2013). Data collection for this survey is executed through computer-assisted personal interviews, which are conducted face-to-face with the target respondent and willing partners or spouses. For people affected by cognitive limitations, including Alzheimer’s disease, dementia and senility, information is obtained through a proxy interview. Some interviews are supplemented with the participant’s completion of a written questionnaire, which includes additional questions on subjects such as mental and physical health, health care and social networks. Complete information is gathered about social network, cognitive functioning, social activities, behavioral risks, mental health, household demography, education, working status, quality of life and the usual socioeconomic and health indicators. The dataset from the fifth wave (year = 2013) is not included because it does not contain information about social network.
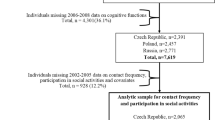
For the purposes of the current investigation, only the information concerning people from twelve European countries included in both surveys, i.e., Austria, Germany, Sweden, Spain, Italy, France, Denmark, Switzerland, Belgium, Czech Republic, Slovenia and Estonia, has been extracted. Datasets from two waves have been merged in order to include only respondents present in both. Therefore, of the 48,450 people and the 56,699 people interviewed, respectively, in 2011 and 2015, only 31,954 interviewed in both surveys were included in the present analysis. Specifically, since only normal aging was considered, people with Alzheimer’s disease, dementia and senility were excluded.
Data are available free of charge for registered users at http://www.share-project.org and are distributed through twenty-five regular and four special module files. To assure data harmonization for cross-national analyses, there are several further generated variables that enhance working with the SHARE data including several indices and scales like the quality of life CASP-12 index for elderly people.
Outcome and covariates
The outcome for the analysis was the cognitive function. We examined two memory tests and one executive function as specific aspects of cognition. Specifically, we have used the immediate (ITest) and delayed (DTest) verbal recall tests from the Ten-Word Delayed Recall Test, both ranging between 0 and 10. Ten common words are presented and participants are asked to recall the words immediately and then again 5 min later. We have also used the score of a semantic verbal fluency (FTest) test consisting of asking the participant to name as many animals as possible correctly during a 1-min period. This score ranges between 0 and 100.
The covariates used for the analysis relate to demographic and socioeconomic information, health status and quality of life, family network and social activity. More specifically, gender, age and living country were included as demographic variables, while years of education and wealth were chosen as socioeconomic status (SES) variables. Wealth was obtained as the sum of household income plus total assets (also referred to as net worth). Total assets are the sum value of the primary residence net of mortgage, value of the real estate, owned share of own business, owned cars, and the value of financial assets (bank accounts, government and corporate bonds, stocks, mutual funds, individual retirement accounts, and contractual savings for housing and life insurance policies owned by the household) minus financial liabilities. In this study, wealth instead of income was chosen as an economic indicator for elderly people in line with other literature (Tsimbos 2010; Allin et al. 2009; Bono and Matranga 2018).
With the aim of capturing the healthcare context, it was included a variable indicating the welfare system of the country in which the interview takes place, with Social-democratic/Scandinavian as reference, and Conservative/Bismarckian, Mediterranean/Southern, Post-communist/Eastern as categories. To summarize, the Social-democratic/Scandinavian system is strongly interventionist, founded on accessing benefits and services based on citizenship and on the promotion of social equality through a redistributive social security system, with generous social transfers and commitment to full employment and income protection; the Conservative/Bismarckian system is based on the principle of subsidiarity, with dominance of social insurance schemes where the redistributive impact is minimal; the Mediterranean/Southern system is characterized by a fragmented system of welfare provision, with a high percentage of social expenditure financed through contributions and strong reliance on family and on the charitable sector; finally, the Post-communist/Eastern system is an undeveloped welfare state with limited health service provision (Alvarez-Galvez 2016).
In order to measure the health status of each respondent, it was considered the variable self-perceived health, which is obtained answering the question “Would you say your health is…” with response categories being “excellent”, “very good”, “good”, “fair” and “poor.” Furthermore, to measure quality of life, it was included the 12-item version of the CASP scale (CASP-12), the reduced version of the 19-items CASP scale, which measures the four dimensions of needs Control, Autonomy, Self-realization, and Pleasure. The questions concern a list of statements used to describe people’s life or how people feel and what people think, with answers coded on a 4-point Likert scale indicating how often (1. Often, 2. Sometimes, 3. Rarely and 4. Never), if at all, the interviewed person has experienced these feelings and thoughts. All items are recoded in such a way that higher scores indicate a higher level of QoL. CASP-12 ranges between 12 and 48 (Borrat-Besson et al. 2015, Hyde et al. 2003).
In order to assess sociality of each individual, there were variables related to social network as well as the number of social activities. The “size”, “composition”, “satisfaction”, “proximity” and “closeness” were included as social network characteristics. The “size” is the number of people that are part of respondent’s network and it ranges between 0 and 7. The “composition” is composed by three modalities: “family network”, if at least one person in the first three network levels is a relative; “external network” if all persons in the first three network levels are one of the following: friend, ex-colleague/coworker, neighborhood, ex-spouse/partner, minister/priest or other clergy; “for-a-fee network” if all persons in the first three network levels are one of the following: therapist or other professional helper, housekeeper/home healthcare provider. An ordinal score expresses the “satisfaction” with the network with a range going from 0 to 10. Proximity concerns the geographical proximity expressed by the following categories: in the same household, in the same building, less than 1 km away, between 1 and 5 km, between 5 and 25 km, between 25 and 100 km, between 100 and 500 km, more than 500 km away. “Proximity” was the discrete variable counting the number of people in the network living within a distance not more than 5 km away, with a range going from 0 to 7. Closeness concerns the emotional closeness with the people that belong to the network of the respondents. It is measured by answering to the question “How close do you feel to…” and response categories are not very close, somewhat close, very close, extremely close. “Closeness” was the discrete variable counting the number of people in the network the respondent feels at least somewhat close, with a range going from 0 to 7.
Finally, the variable “number of activities” was included as the sum of the activities the respondent has done in the last 12 months among: voluntary or charity work, attending an educational or training course, going to a sport, social or other kind of club, taking part in a political or community-related organization, reading books, magazines or newspapers, doing word or number games such as crossword puzzles or Sudoku and playing cards or games such as chess. The resulting discrete variable ranges between 0 and 8.
Variables with missing data were extracted from the imputation dataset available in release 6.0.0 of the SHARE data. They are gender, age, years of education, household net worth, total household net income, number of activities, self-perceived health and semantic verbal fluency. Missing values were imputed using the univariate hot-deck method for various types of variables affected by negligible shares of missing data. Alternatively, a more sophisticated multivariate conditional specification method was used for monetary variables affected by more relevant fractions of missing data. To take into account the additional variability induced by the imputation process, the imputation database of each wave included five imputations (or implicates) of the missing values (De Luca et al. 2015).
Statistical methods
Categorical variables were summarized as counts and percentages, discrete and continuous variables as mean and standard deviation. In the presence of asymmetric distribution, variables were synthesized as median and interquartile range. Pearson’s correlations between pairs of variables were calculated. All quantitative variables were standardized before beginning statistical analysis.
Structural equation modeling was applied to assess the relationship between cognitive function, social life and socioeconomic status (SES) over time. More specifically, for this analysis a structural equation model with measurement component was used (Wheaton et al. 1977). In both 2011 (Wave 4) and 2015 (Wave 6), ITest, DTest and FTest were included to measure endogenous latent variables representing the cognitive function (CF) for the same 2 years. Years of education and household net worth were used to measure the exogenous latent variable SES. Satisfaction with social network and number of social activities were included to measure the exogenous latent variable SOCIALITY. In order to improve the SEM model, residuals between observed and estimated covariances were considered. In the presence of high residuals, some links between random errors for variables with high residuals were introduced.
To better understand the relations between social activities and cognitive functioning, it was investigated whether there was a mediation effect of years of education and if this mediation was moderated by satisfaction with social network (Hayes 2013; Preacher et al. 2007).
Multilevel ordinal logistic regression was applied to explain satisfaction with social network in relation to different types of social network across countries, net of demographic, quality of life and self-perceived health variables. The people interviewed (level 1 units) were nested within their living countries (level 2 units). Demographic information, network characteristics including size, composition, proximity and closeness, as well as health and quality of life information were included as level 1 covariates. The welfare system of the country of residence was included as level 2 covariate.
Data were analyzed using STATA software (version 14.2) with a 5% level of significance.
Results
Of 31,954 sampled people, 58% was female, the mean age was 65.54 ± 9.74 and the years of education were, on average, 10.81 ± 4.42. Of the whole, 13,496 (42%) lived in a country with a Conservative welfare system, 10,297 (32%) lived in a Post-communist country, while 5,051 (16%) and 3,110 (10%) lived in a Mediterranean and a Scandinavian country, respectively (Table 1).
Most of the interviewed people declared very good or excellent self-perceived health and a satisfactory quality of life. They were shown to be very satisfied with their own social network, which was mostly a family-type network (more than 89% in both years), small sized, with two people on average felt to be at least somewhat close and only one person on average living within a distance not more than 5 km away. Social activity was found generally scarce with slightly more than two social activities per person and a low–medium cognitive level, with verbal recall ranging between 4 and 5 on average in both years and verbal fluency around 20 (Table 2). All correlations between pair of variables were statistically significant, except for wealth and satisfaction with social network.
The estimated model suggested that CF in 2011 was positively associated with CF after 4 years, even if not significantly (latent coefficient = 0.24, p value = 0.34) and that SES in 2011 promoted CF in the same time and after 4 years (latent coefficient = 0.08, p value < 0.001 for both). Analogously, SOCIALITY in 2011 supported CF in the same year (latent coefficient = 3.7, p value < 0.001) and in successive 4 years (latent coefficient = 3.5, p value = 0.03). In both years, CF was mostly measured through ITest (coeff = 3.9 in 2011 and coeff = 3.5 in 2015, both p < 0.001) and DTest (coeff = 4.8 in 2011 and coeff = 4.2 in 2015, both p < 0.001) rather than through FTest. SOCIALITY was measured more by means of the number of social activities than by means of satisfaction with social network (coeff = 18.17, p < 0.001) and SES less by wealth than by years of education (coeff = 0.029, p < 0.001). The model suggested the positive covariance between FTest (0.18) and DTest (0.25) over 2 years and between years of education and FTest in 2011 (0.50) and in 2015 (0.44) (Fig. 1, Table S1 in Supplement materials).

Structural equation model graph for cognitive function, sociality and SES, years 2011 and 2015. Note Latent variables are represented by ovals and measurement variables by rectangles. Each arrow shows the standardized coefficient for each parameter in the model that represents the strength of the relationships
Years of education acted as a mediator of the relation between number of social activities and ITest, with estimated direct effect 0.265 (p < 0.001) and indirect effect 0.063 (p < 0.001). The mediation role of years of education was stronger for DTest, with estimated direct effect 0.337 (p < 0.001) and indirect effect 0.074 (p < 0.001). Satisfaction with social network did not moderate this mediation neither for ITest (p = 0.484) nor for DTest (p = 0.680).
Increasing levels of satisfaction with social network were observed more for females than males (adjOR = 1.27, 95%CI = [1.24; 1.30]) and were associated with higher levels of quality of life (adjOR = 1.06, 95%CI = [1.05; 1.06]), with having a social network characterized by high emotional closeness (adjOR = 1.73, 95%CI = [1.71; 1.76]) and high proximity (adjOR = 1.03, 95%CI = [1.02; 1.05]). Lower satisfaction was associated with larger networks (adjOR = 0.63, 95%CI = [0.62; 0.64]) and poor self-perceived health (adjOR = 0.93, 95%CI = [0.9; 0.95]). Finally, people living in Conservative countries showed lower levels of satisfaction with social network compared to Social-democratic/Scandinavian (Table 3). The unobserved heterogeneity at country level was statistically significant (among-countries variance = 0.09, 95%CI = [0.05; 0.16]), and all countries, except France, Czech Republic and Italy, showed a significant geographical effect (Fig. 2).

Multilevel ordinal logistic regression model for satisfaction with social network: country-level residuals and 95% CIs
Discussions
The aim of this study was to investigate the relationship between cognitive functions (immediate and delayed verbal recall tests and semantic verbal fluency), sociality and SES, among European healthy elderly, and to assess whether different types of social network are associated with different satisfaction levels. Furthermore, another scope was to know if sociality (evaluated through the “social network” variables and number of activities performed), and SES (evaluated through the variable “years of education” and “wealth”) take an explanatory role of cognitive function, both in the concurrent and in the prospective time.
In response to the first of the debated issues in the literature, our paper contributed to explain the relationship between sociality and the examined cognitive functioning through SEM. The results indicated that being equipped with good cognitive skills does not seem to be predictive of their maintenance over time. On the contrary, the subject’s social and participatory life, understood as satisfaction in one’s social network and engaging in diversified non-professional social activities (going to a social/sports club, participating in a political or community organization, helping family/friends/neighbors and volunteering), seemed to play a crucial role to affect cognitive functions of elderly in the prospective time (Barnes et al. 2004).
Numerous studies have shown that old adults without any kind of social support offered by a network present a reduced risk of cognitive impairment if engaged in the performance of non-professional activities. In contrast, social disengagement is a risk factor for cognitive functioning in elderly subjects (Adam et al. 2013; Litwin and Stoeckel 2015; Kelly et al. 2017).
This affects every aspect of health and well-being, from mental health, to the risk of emergency hospital admissions due to avoidable diseases, such as severe conditions of dehydration or malnutrition. Wealth is a significant predictor of perceived health and of the use of healthcare services. Furthermore, even if income and wealth are positively related, income reflects a flow of resources, which are available over a period, while wealth reflects a stock of resources, which are accumulated over a person’s lifetime. Among the elderly, levels of income vary much less than levels of wealth, so wealth allows more accurate measurements of SES differences in health and healthcare utilization in this population (Tsimbos 2010; Allin et al. 2009; Bono and Matranga 2018). However, this study showed that wealth played a minor role in affecting the examined cognitive tasks of individuals, while education was a significant protective factor to prevent cognitive decline in aging. This result is in line with other studies (Le Carret et al. 2003; Zhang et al. 2008; Adam et al. 2013) which suggest that education represents one of the most important factors that contribute to the development of cognitive reserve.
To assess if family-type networks with greater social capital are associated with better cognitive tasks, results of logistic regression showed that there is an inverse relation between network size and satisfaction with social network. A high level of satisfaction is in fact associated with a reduced dimension, probably due to more significant relational experiences. This result is in line with the socio-emotion selectivity theory, formulated by Carstensen (1992), which stated that social interactions assume a different role and meaning from adulthood and decrease significantly in old age, in which high-quality relationships are preferred. This finding is further confirmed by the role of emotional and geographical proximity. Having a family-like network with only one friend over external or for-a-fee networks increases the satisfaction with the network.
Another result of the study was the positive association between both quality of life and self-perceived health with satisfaction with social network. Indeed, a direct relationship of these outcomes with social engagement is consistent with other literature. The prevalence of people who do not participate in any productive and/or social activities and report either high quality of life or good self-perceived health has been found to be significantly lower compared to those who are frequently involved in activities (Vozikaki et al. 2017). This finding is supportive of the notion that sociality in old age, expressed as an individual who enjoys a satisfactory social network, is significantly associated with the quality of life, meant as the fulfillment of oneself and one’s own human needs.
In response to the second open question, our paper contributed to assess if the welfare system explains differences in satisfaction with social network among countries. It was found that people living in Conservative systems are less socially active and most inclined to be less satisfied with their own social network than people living in Socio-democratic/Scandinavian welfare systems. This finding is not surprising because Scandinavian countries enjoy a state-of-the-art welfare system that has put the Nordic countries at the forefront of rankings for quality of life, well-being and health. This system is based on the principle of Universal provision system, meaning a high level of public responsibility and comprehensive social rights for everybody. The Nordic welfare model is characterized by generalized access to benefits and services based on citizenship, the promotion of social equity through a generous redistributive social security system and the widespread use of welfare technology (Eikemo et al. 2008). In addition, in order to explain the geographic heterogeneity of individuals’ network satisfaction, we can hypothesize the existence of some country-specific characteristics, in agreement with the study of Alvarez-Galvez (2016), where the occupational status was found for Scandinavians, income for the Conservative countries, education for Mediterranean and demographic characteristics for Post-communist countries.
There are some limits of the present study. Firstly, it did not take into consideration the different types of activities and the different roles they can play on cognitive function. For example, the study conducted by Adam et al. (2013) highlights how some activities are more related to cognitive functioning than others, for example, participation in a religious organization seems to have the least impact on cognitive performance, while activities involving the acquisition and development of new skills have a greater impact.
Secondly, only three cognitive tasks were considered in this study and all of them were investigated through a single question. Moreover, we have not taken into consideration the various changes in participatory life and in social relations that may derive from exceptional events (loss of work, mourning, divorce, etc.).
Another limitation is that the analysis was not stratified by age and sex, and this could be a source of bias in estimating the weight of variables based on the life cycle. However, just 1% of the sample was not more than 50 years old and 75% was more than 65 years old. Therefore, the major part of the sample is made of economically inactive people. Furthermore, since data of the two SHARE waves were not examined as panel data, there are no results about the cognitive change at individual level. To end, in the assessment of the relationship between cognitive function, social life and SES over time, the living country of the respondent or the welfare system was not considered. This is another limitation of the study, since it would be important to determine if the same results (relationships among the different constructs) could be obtained in the different countries. We propose to investigate the geographic variability of these constructs in the future research.
Conclusion and implications
In the last decade, knowledge of the protective role played by some psychosocial factors on cognitive functioning has increased. This research seems to support the idea that a socially active and participatory lifestyle can mitigate the effects of aging. Such experimental evidence undoubtedly opens new perspectives for the development of social policy interventions to favor an “active and healthy aging,” facilitating the participation of the elderly in a wide range of activities, especially targeted at those who seem to be more socially isolated. Furthermore, it is advisable to promote prevention programs aimed at adults in order to keep their cognitive functions unaltered and prevent deterioration, with a remarkable impact in terms of containment of healthcare expenditure.
While the research in the field of biological and neurological factors involved in the processes of brain aging, continues to progress with great vigor, the study of psychosocial factors has not always evoked the same interest. This is especially true in some geographical areas, where the recognition of the importance of participation social life of the elderly is still far from being fully achieved and stimulated by welfare policies. Therefore, further research is necessary to clarify the process that underlies the causal relationship between cognitive functioning and forms of social participation and eventually to explore other measures of cognition, different from memory and executive functions.
References
Aartsen MJ, Smits CHM, Van Tilburg T, Knipscheer KCPM, Deeg DJH (2002) Activity in older adults: cause or consequence of cognitive functioning? A longitudinal study on everyday activities and cognitive performance in older adults. J Gerontol 57:153–162
Adam S, Bonsang E, Grotz C, Perelman S (2013) Occupational activity and cognitive reserve: implications in terms of prevention of cognitive aging and Alzheimer’s disease. Clin Interv Aging 8:377–39
Allin S, Masseria C, Mossialos E (2009) Measuring socioeconomic differences in use of health care services by wealth versus by income. Am J Public Health 99(10):1849–1855
Alvarez-Galvez J (2016) Discovering complex interrelationships between socioeconomic status and health in Europe: a case study applying Bayesian networks. Soc Sci Res 56:133–143
Andel R, Silverstein M, Kareholt I (2015) The role of midlife occupational complexity and leisure activity in late-life cognition. J Gerontol B Psychol Sci Soc Sci 70:314–3218
Andrew MK, Mitnitski AB, Rockwood K (2008) Social vulnerability, frailty and mortality in elderly people. PLoS ONE 3(5):e2232. https://doi.org/10.1371/journal.pone.0002232
Barnes LL, Mendes de Leon CF, Wilson RS, Bienias JL, Evans DA (2004) Social resources and cognitive decline in a population of older African Americans and whites. Neurology 63:2322–2326
Béland F, Zunzunegui MV, Alvarado B, Otero A, del Ser T (2005) Trajectories of Cognitive Decline and Social Relations. J Gerontol B Psychol Sci Soc Sci 60:320–330
Berkman LF, Glass T, Brissette I, Seeman TE (2000) From social integration to health: Durkheim in the new millennium. Soc Sci Med 51:843–857
Bono F, Matranga D (2018) Socioeconomic inequality in non-communicable diseases in Europe between 2004 and 2015: evidence from the SHARE survey. Eur J Public Health. https://doi.org/10.1093/eurpub/cky165
Boots EA, Schultz SA, Almeida RP, Oh JM, Koscik RL, Dowling MN, Gallagher CL, Carlsson CM, Rowley HA, Bendlin BB, Asthana S, Sager MA, Hermann BP, Johnson SC, Okonkwo OC (2015) Occupational complexity and cognitive reserve in a middle-aged cohort at risk for Alzheimer’s disease. Arch Clin Neuropsychol 30:634–642
Borrat-Besson C, Ryser V.-A, Gonçalves J (2015) An evaluation of the CASP-12 scale used in the Survey of Ageing and Retirement in Europe (SHARE) to measure Quality of Life among people aged 50 + . FORS Working Paper Series, paper 2015-4. Lausanne: FORS
Börsch-Supan A, Brandt M, Hunkler C, Kneip T, Korbmacher J, Malter F, Schaan B, Stuck S, Zuber S (2013) SHARE central coordination team. data resource profile: the Survey of Health, Ageing and Retirement in Europe (SHARE). Int J Epidemiol 42:992–1001
Bourassa KJ, Memel M, Woolverton C, Sbarra D (2017) Social participation predicts cognitive functioning in aging adults over time: comparisons with physical health, depression, and physical activity. Aging Ment Health 21:133–146
Bowling A, Farquhar M, Browne P (1991) Use of services in old-age: data from 3 surveys of elderly people. Soc Sci Med 33:689–700
Brown WM, Concedine NS, Magai C (2005) Altruism relates to health in an ethnically diverse sample of older adults. J Gerontol B Psychol Sci Soc Sci 60:143–152
Brown CL, Robitaille A, Zelinski EM, Dixon RA, Hofer SM, Piccinin AM (2016) Cognitive activity mediates the association between social activity and cognitive performance: a longitudinal study. Psychol Aging 31:831–846
Cacioppo JT, Hawkley LC (2009) Perceived social isolation and cognition. Trends Cogn Sci 13:447–454
Carstensen LL (1992) Social and emotional patterns in adulthood: support for socioemotional selectivity theory. Psychol Aging 7:331–338
Chan Y, Lee RP (2006) Network size, social support and happiness in later life: a comparative study of Beijing and Hong Kong. J Happiness Stud 7:87–112
Colcombe S, Kramer AF (2003) Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci 14:125–130
Croezen S, Avendano M, Burdorf A, van Lenthe FJ (2015) Social participation and depression in old age: a fixed-effects analysis in 10 European countries. Am J Epidemiol 182:168–176
De Luca G, Celidoni M, Trevisan E (2015) Item nonresponse and imputation strategies in SHARE wave 5. In: Malter F, Börsch-Supan A (eds) SHARE Wave 5: innovations & methodology, max planck institute for social law and social policy. MEA, Munich
Dominguez S, Arford T (2010) It is all about who you know: social capital and health in low-income communities. Health Sociol Rev 19:114–129
Eikemo TA, Bambra C, Judge K, Ringdal K (2008) Welfare state regimes and differences in self-perceived health in Europe: a multilevel analysis. Soc Sci Med 66(11):2281–2295
Eriksson BG, Hessler RM, Sundh J, Steen B (1999) Cross-cultural analysis of longevity among Swedish and American elders: the role of social networks in the Gothenburg and Missouri longitudinal studies compared. Arch Gerontol Geriatr 28:131–148
Fillit HM, Butler RN, O’Connell AW et al (2002) Achieving and maintaining cognitive vitality with aging. Mayo Clin Proc 77:681–696
Fiori KL, Antonucci TC, Cortina KS (2006) Social network typologies and mental health among older adults. J Gerontol B Psychol Sci Soc Sci 61:25–32
Fu C, Li Z, Mao Z (2018) Association between social activities and cognitive function among the elderly in China: a cross-sectional study. Int J Environ Res Public Health 15:231
Garcia EL, Banegas JR, Perez-Regadera AG, Cabrera RH, Rodriguez-Artalejo F (2005) Social network and health-related quality of life in older adults: a population-based study in Spain. Qual Life Res 14:511–520
Gow AJ, Pattie A, Whiteman MC, Whalley LJ, Deary IJ (2007) Social support and successful aging: investigating the relationships between lifetime cognitive change and life satisfaction. J Individ Differ 28:103–115
Green AF, Rebok G, Lyketsos CG (2008) Influence of social network characteristics on cognition and functional status with aging. Int J Geriatr Psychiatr 23:972–978
Groot W, van Den Brink HM, van Praag B (2007) The compensating income variation of social capital. Soc Indic Res 82:189–207
Haugrud N, Crossley M, Vrbancic M (2011) Clustering and switching strategies during verbal fluency performance differentiate Alzheimer’s disease and healthy aging. J Soc Particip Cognit. Int Neuropsychol Soc 17(6):1153–1157
Hayes AF (2013) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. Guilford Press, New York
Henry JD, Crawford JR (2004) A meta-analytic review of verbal fluency performance following focal cortical lesions. Neuropsychology 18(2):284–295
Hertzog C, Kramer AF, Wilson RS (2008) Enrichment effects on adult cognitive development: can the functional capacity of older adults be preserved and enhanced? Psychol Sci Public Interest. 9:1–65
Hultsch DF, Hertzog C, Small BJ, Dixon RA (1999) Use it or lose it: engaged lifestyle as a buffer of cognitive decline in aging? Psychol Aging 14:245–263
Hyde M, Wiggins R, Higgs P, Blane D (2003) A measure of quality of life in early old age: the theory, development and properties of needs satisfaction model. Aging Ment Health 7(3):186–194
James BDR, Wilson S, Barnes LL, Bennett DA (2011) Late-life social activity and cognitive decline in old age. J Int Neuropsychol Soc 17(6):998–1005
Jefferson AL, Gibbons LE, Rentz DM, Carvalho JO, Manly J, Bennett DA, Jones RN (2011) A life course model of cognitive activities, socioeconomic status, education, reading ability, and cognition. J Am Geriatr Soc 59(8):1403–1411
Kelly ME, Duff H, Kelly S, McHugh Power JE, Brennan S, Lawlor BA, Loughrey DG (2017) The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: a systematic review. Syst Rev 6(1):259
La Rue A (2010) Healthy brain aging: role of cognitive reserve, cognitive stimulation, and cognitive exercises. Clin Geriatr Med 26(1):99–111
Laws KR, Duncan A, Gale TM (2010) Normal semantic-phonemic fluency discrepancy in Alzheimer’s disease? A meta-analytic study. Cortex 46(5):595–601
Le Carret N, Lafont S, Letenneur L, Dartigues F, Mayo W, Fabrigoule C (2003) The effect of education on cognitive performances and its implication for the constitution of the cognitive reserve. Dev Neuropsychol. 23:317–337
Lindström M, Moghaddassi M, Merlo J (2004) Individual self-reported health, social participation and neighbourhood: a multilevel analysis in Malmö, Sweden. Prev Med 39:135–141
Litwin H (2004) Social networks, ethnicity and public home-care utilisation. Ageing Soc 24:921–939
Litwin H, Stoeckel KJ (2013) Social networks and subjective wellbeing among older Europeans: Does age make a difference? Ageing Soc 33:1263–1281
Litwin H, Stoeckel KJ (2015) Social network, activity participation, and cognition. A Complex Relationsh. Res Aging 38:76–97
Matranga D, Tabacchi G, Cangialosi D (2018) Sedentariness and weight status related to SES and family characteristics in Italian adults: exploring geographic variability through multilevel models. Scand J Public Health 46(5): 548–556
McGue M, Christensen K (2007) Social activity and healthy aging: a study of aging Danish twins”. Twin Res Hum Genet 10:255–265
McLaughlin D, Vagenas D, Pachana NA, Begum N, Dobson A (2010) Gender differences in social network size and satisfaction in adults in their 70s. J Health Psychol 15:671–679
Miceli S, Gangemi A (2011) Psicologia dell’intelligenza. Laterza, Bari
Miller LMS, Lachman ME (2000) Cognitive performance and the role of control beliefs in midlife. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 7:69–85
Misuraca R, Miceli S, Teuscher U (2017) Three effective ways to nurture our brain physical activity, healthy nutrition, and music. A Review. Eur Psychol 22(2):101–120
Park HL, O’Connell JE, Thomson RG (2003) A systematic review of cognitive decline in the general elderly population. Int J Geriatr Psychiatry 18(12):1121–1134
Pinquart M, Sörensen S (2000) Influences of socioeconomic status, social network, and competence on subjective well-being in later life: a meta-analysis. Psychol Aging 15(2):187–224
Preacher KJ, Rucker DD, Hayes AF (2007) Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivar Behav Res 42(1):185–227
Rafnsson SB, Shankar A, Steptoe A (2015) Longitudinal influences of social network characteristics on subjective well-being of older adults: findings from the ELSA study. J Aging Health 27(5):919–934
Seeman TE, Lusignolo TM, Albert M, Berkman L (2001) Social relationships, social support, and patterns of cognitive aging in healthy, high-functioning older adults: macArthur studies of successful aging. Health Psychol 20:243–255
Singh-Manoux A, Marmot MG, Glymour M, Sabia S, Kivimäki M, Dugravot A (2011) Does cognitive reserve shape cognitive decline? Ann Neurol 70(2):296–304
Smart EL, Gow AJ, Deary I (2014) Occupational complexity and lifetime cognitive abilities. Neurology 9(83):2285–2291
Stern Y (2003) The concept of cognitive reserve: a catalyst for research. J Clin Exp Neuropsychol 25:589–593
Stern Y (2007) Cognitive reserve: theory and application. Taylor & Francis, Philadelphia
Stern Y (2009) Cognitive reserve. Neuropsychologia 47:2015–2028
Tilvis RS, Kähönen-Väre MH, Jolkkonen J, Valvanne J, Pitkala KH, Strandberg TE (2004) Predictors of cognitive decline and mortality of aged people over a 10-year period. J Gerontol A Biol Sci Med Sci 59:268–274
Tomini F, Tomini S, Groot W (2016) Understanding the value of social networks in life satisfaction of elderly people: a comparative study of 16 European countries using SHARE data. BMC Geriatr 16(1):203
Tsimbos C (2010) An assessment of socio-economic inequalities in health among elderly in Greece, Italy and Spain. Int J Public Health 55:5–15
van der Horst M, Coffé H (2012) How friendship network characteristics influence subjective well-being. Soc Ind Res 107(3):509–529
Vásquez-Amézquita M (2016) Factores predictores de la reserva cognitiva en un grupo de adultos mayores. Predictors of cognitive reserve in a group of elderly. Rev Chil Neuropsicol 11(1):5–11
Vozikaki M, Linardakis M, Micheli K, Philalithis A (2017) Activity Participation and Well-Being Among European Adults Aged 65 years and Older. Soc Ind Res 131(2):769–795
Wheaton B, Muthen B, Alwin DF, Summers G (1977) Assessing reliability and stability in panel models. Sociol Methodol 8(1):84–136
Wilson RS, Scherr PA, Schneider JA, Tang Y, Bennett DA (2007) Relation of cognitive activity to risk of developing Alzheimer disease. Neurology 69(20):1911–1920
Zhang Z, Gu D, Hayward MD (2008) Early life influences on cognitive impairment among oldest old Chinese. J Gerontol B Psychol Sci Soc Sci 63:S25–S33
Acknowledgements
This paper uses data from release 6 of SHARE 2011 and SHARE 2015. The SHARE data collection has been primarily funded by the European Commission through the 5th Framework Programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life). Additional funding came from the US National Institute on Aging (U01 AG09740-13S2, P01 AG005842, P01 AG08291, P30 AG12815, Y1-AG-4553-01 and OGHA 04-064). Data collection in Austria (through the Austrian Science Foundation, FWF), Belgium (through the Belgian Science Policy Office) and Switzerland (through BBW/OFES/UFES) was nationally funded. The SHARE data collection in Israel was funded by the US National Institute on Aging (R21 AG025169), by the German–Israeli Foundation for Scientific Research and Development (GIF), and by the National Insurance Institute of Israel. Further support by the European Commission through the 6th Framework Programme (Projects SHARE-I3, RII-CT-2006-062193, and COMPARE, CIT5-CT-2005-028857) is gratefully acknowledged. For methodological details see [Börsch-Supan, A. and H. Jürges (Eds.) (2005). The Survey of Health, Ageing and Retirement in Europe—Methodology. Mannheim: Mannheim Research Institute for the Economics of Aging (MEA)].
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Matthias Kliegel.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Miceli, S., Maniscalco, L. & Matranga, D. Social networks and social activities promote cognitive functioning in both concurrent and prospective time: evidence from the SHARE survey. Eur J Ageing 16, 145–154 (2019). https://doi.org/10.1007/s10433-018-0486-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10433-018-0486-z