
Abstract
In a context of increasing ageing of the population, it is crucial to better understand multimorbidity and its consequences. This study measured the prevalence of multimorbidity in a Southern Europe population and projected its evolution based on expected demographic changes. It also analysed its associated consequences on self-reported health status, functional capacity, and healthcare use. Our sample included all people aged 25–79 years (6679 men and 8517 women) who participated in the fifth Portuguese National Health Interview Survey, conducted in 2014. Multimorbidity was measured by the presence of at least two self-reported chronic conditions. Multivariable regressions were used to assess the association of multimorbidity with health status, functional capacity, and healthcare use. The projected evolution of multimorbidity was based on official demographic projections. 43.9% of the Portuguese population self-reported the multimorbidity, which was more frequent among older people, women, and low-educated people. We found an association of multimorbidity with poorer health status (OR 3.32, 95%CI 2.60–4.24) and with limited functional capacity (OR 4.44, 95%CI 3.85–5.11). Multimorbidity was also associated with higher healthcare resource use, namely a 26% increased likelihood of hospitalization in the previous 12 months per additional comorbidity. We projected a 13.1% growth in the prevalence of multimorbidity until the year 2050. Multimorbidity affects a substantial share of the population and is expected to grow in the near future related to population ageing. The co-occurrence of chronic health conditions increases sharply with age and is associated with worse health status, reduced functional capacity, and increased healthcare use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The world has continued to observe an increase in the life expectancy (Mortality Data 2013). Ageing populations are characterized by the co-occurrence of multiple chronic conditions (i.e. multimorbidity) (van den Akker et al. 1998; Walker 2007; Salisbury et al. 2011; Barnett et al. 2012). There is still a major gap in the understanding of how best to address the complex care needs of patients with multimorbidity (Navickas et al. 2016). The traditional single-disease model is insufficient, and multimorbidity should not be considered as the simple juxtaposition of independent conditions; that is, its effects on well-being and healthcare needs may exceed those one would observe by summing up single diseases’ consequences (Treadwell 2015). Thus, interest in multimorbidity is growing worldwide and has become a healthcare and research priority (Valderas et al. 2007; Ramond-Roquin and Fortin 2016).
The overall estimated prevalence of multimorbidity varies immensely across the literature (Violan et al. 2014) and can rise to as high as 95% in the elderly population (Formiga et al. 2013). It is associated with high mortality (Gijsen et al. 2001), reduced quality of life, and functional status (Walker 2007; Kadam 2007; Fortin et al. 2004), as well as with increased healthcare use (Salisbury et al. 2011; Wolff et al. 2002). In fact, most healthcare costs are spent on patients with more than one chronic condition (Anderson 2010; Ornstein et al. 2013). Therefore, not surprisingly, managing the rising prevalence of multimorbidity has been considered one of the greatest challenges faced by governments and healthcare systems worldwide (Barnett et al. 2012; WHO 2010).
Population ageing is expected to worsen this scenario, and projections regarding the forthcoming multimorbidity are essential to plan public health policies and strategies. A better understanding of the current and future epidemiology of multimorbidity and its consequences, such as self-reported health status, functional capacity, and healthcare use, is thus necessary to develop interventions to prevent them and to reduce their burden.
Portugal is at the very forefront of a general demographic concern. The rapid growth of life expectancy at birth and decline of fertility rates (11.4% and − 32.2%, respectively, over the last 30 years) (https://www.ine.pt) makes the ageing challenge in Portugal greater than in most European countries (European Commission 2015). This provides a valuable context to understand the global rise in age-related health issues. This study measured the current prevalence of multimorbidity in a Southern Europe population (Portugal) and projected its evolution based on expected demographic changes. It also analysed its consequences on self-reported health status, functional capacity, and healthcare use.
Methods
Sample
We used cross-sectional data from the fifth Portuguese National Health Interview Survey (Inquérito Nacional de Saúde, INS), conducted in 2014 (Instituto Nacional de Estatística. Inquerito Nacional de Saúde 2014). The INS is a population-based survey on a probabilistic representative sample of non-institutionalized individuals aged 15 years and over. Data collected included self-reported information on a broad range of variables related to health condition, lifestyle, and socio-economic status. The methodology of the INS has been detailed elsewhere (Instituto Nacional de Estatística. Inquerito Nacional de Saúde 2014).
In this study, all individuals aged 25–79 years were included; younger people were excluded in order to avoid as much as possible individuals who had not completed their education. In addition, older people were excluded to reduce the selective mortality bias (Kaplan et al. 1992). The final sample included 6679 men and 8517 women.
Measures
All chronic conditions collected in the INS were considered from a pre-defined list in the questionnaire: hypertension, diabetes, coronary heart disease, stroke or myocardial infarction in the previous year, arthrosis, chronic upper and low pain, chronic obstructive pulmonary disease, asthma, allergy, kidney disease, urinary incontinence, liver cirrhosis, and depression. Multimorbidity was defined by the presence of two or more of these self-reported chronic conditions (Van den Akker et al. 1996; Diederichs et al. 2011). We also considered the number of these chronic diseases.
Self-reported health was used as proxy of health status, measured as a 5-item scale from “very bad” to “very good”, as possible responses to the question “how is your health in general?”. We created a dichotomous “poor health” variable with a value one for the “bad” or “very bad” categories and zero otherwise. Self-reported health has been demonstrated to be a good predictor of morbidity and mortality (Idler and Benyamini 1997; Kawada 2003; Mossey and Shapiro 1982; Sundquist and Johansson 1997; Miilunpalo et al. 1997; DeSalvo et al. 2005). Reduction in functional capacity, categorized as limited/not limited, was measured through the global activity limitation indicator (GALI). We used the answers to the question “For at least the last 6 months have you been limited in activities people usually do, because of a health problem?” (“strongly limited”; “limited”; “not limited”) (Oyen et al. 2006; Robine and Jagger 2003; Jagger et al. 2010).
We also considered healthcare use in both primary and secondary care, including number of medical doctor visits, defined as the sum of general practitioner (GP) or specialist consultations, and whether or not the person had been hospitalized in the previous year.
The following covariates were included: age group, sex, region of residence (North, Centre, Lisbon region, Alentejo, Algarve, Azores, and Madeira), household income (categorized into five quintiles), and individual educational level, grouped into three major levels according to the highest qualification completed: None (no education), Low (primary school and basic school between primary and secondary levels), and high (secondary education/university degree).
Statistical analysis
The analysis included four steps. First, a descriptive analysis was performed to compare participants with and without multimorbidity. Second, a logistic regression model was used to assess the association of self-reported health status and functional impairment with multimorbidity, adjusting for age, sex, region, household income, and education. Third, we modelled poor self-reported health, functional impairment, and healthcare consumption, as function of age, sex, region, education, and household income, stratified by the number of chronic conditions, in order to calculate the adjusted prevalence of poor health and reduced functional capacity, and the predicted healthcare consumption in the last 12 months (i.e. hospitalizations and GP/specialist appointments). Fourth, to estimate the potential evolution of the multimorbidity in Portugal, we used the official demographic projections from the National Institute of Statistics (INE - Resident Population Projections, 2012–2060) (https://www.ine.pt). We calculated the adjusted prevalence of multimorbidity by age category. These adjusted values were obtained from a logistic regression on the risk of multimorbidity as function of sex, region, education, and household income. We also calculated the adjusted number of chronic conditions by age category. These adjusted values were obtained from a generalized linear model with a gamma distribution on the number of chronic conditions as function of sex, region, education, and household income. The gamma distribution was selected on the basis of the Akaike information criterion. (The other tested distributions were negative binomial, Gaussian, and Poisson.) We then measured how this adjusted prevalence of multimorbidity and number of conditions changed as the age distribution of the population evolved in accordance with the aforementioned official demographic projections.
All estimates used sampling weights, as previously developed by the Statistics Portugal (https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=263714091&PUBLICACOESmodo=2&xlang=en), which were computed according to design weight (i.e. the inverse of the probability of selection of each primary sampling unit and of each household in each primary sampling unit, further corrected for the effective number of participants evaluated, and taking into account the age and sex structures) in order to match the population distribution in terms of geographic region, age, and gender. Missing values were not replaced, and all statistics were calculated based on non-missing data. Missing data were very low in the INS survey (e.g. missing data on all self-reported chronic conditions were below 1%).
All statistical analyses were carried out using Stata 13 for Windows.
Results
Prevalence and characterization
Nearly half (43.9%) of the study population self-reported at least 2 chronic health conditions (Table 1). Multimorbidity was more prevalent in women and older people. On average, women had 2.2 chronic health conditions, against 1.4 among men (p < 0.01).
Multimorbidity was greater among those with lower educational level and lower household income and was more prevalent among those reporting poorer health status and limited functional capacity (89.1% and 76.6%, respectively, Table 1).
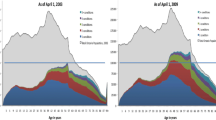
We observed a steep rise in chronic health conditions with increasing age, especially after 45 years, and in the multimorbidity prevalence (age ≥ 45 years: 58.9%; age ≥ 65 years: 75.6% Fig. 1). Almost a third of the elderly population (age ≥ 65) suffered at least five chronic health conditions.

Prevalence of multimorbidity and the number of chronic health conditions by age group
Low back pain was the most prevalent self-reported condition (34.8%), followed by hypertension (26.5%), upper back pain (25.6%), arthrosis (24.5%), allergy (19.1%), depression (13.0%), and diabetes (9.8%; “Appendix 1”). The highest re-occurrence (i.e. above 10%) was observed among chronic upper and low back pain, hypertension, and arthrosis, followed by allergy, depression, and diabetes, with co-occurring frequencies between 5% and 10% of the population (“Appendix 1”).
Health and healthcare consequences
We observed a strong association of multimorbidity with poorer health status (OR 3.32, 95% CI 2.60–4.24) and limited functional capacity (OR 4.44, 95% CI 3.85–5.11), (“Appendix 2”).
We observed a steep progression of adjusted prevalence of poor self-reported health and limited functional status according to the number of chronic health conditions (Fig. 2). The healthcare use was also higher with increasing morbidity.

Age, sex, education, income, and region-adjusted prevalence of health status, functional capacity, and healthcare use by number of chronic health conditions. HCRU healthcare resource use, GP general practitioner
Those more affected by multimorbidity reported higher healthcare use, in particular general practice appointments (86.5% vs. 67.0%; p < 0.01), specialist appointments (58.7% vs. 41.0%; p < 0.01), and hospital admissions (13.9% vs. 5.4%; p < 0.01) in the previous 12 months, compared with those without self-reported multimorbidity. We estimated a 26% increased risk of hospitalization per additional comorbidity (age, sex, education, income, and region-adjusted OR 1.26, 95% CI 1.22–1.31).
Projections
We projected from 2014 until 2050 a 5.6 percentage point and a 13.1% increase on the adjusted prevalence of multimorbidity (expected growth for 2020: 3.1%; 2030: 8.3%; 2040: 11.7%; 2050: 13.1%; compound annual growth rate, CAGR: 0.3% Figure 3). We also estimated an increase in the mean number of chronic health conditions (2014: 1.5 and 2050: 1.7), which potentially translates into at least an additional 5% increase in the hospitalizations due to multimorbidity.

Number of chronic health conditions and multimorbidity projections 2014–2050. *Baseline: based on the “central scenario” from the INE - Resident Population Projections, which in turn combines the central assumption for the fertility component, the central assumption for the mortality component, and a positive net migration. Negative outlook: based on the “low scenario”, which in turn uses the pessimistic assumption for the fertility component, the central assumption for the mortality component, and a negative net international migration. Positive outlook: based on the “high scenario”, which in turn combines the optimistic assumptions for both the fertility component and the mortality component and a positive net migration (European Commission 2015)
Discussion
In this nationwide population-based survey, multimorbidity was found to affect more than 40% of the Portuguese population, this figure being even greater among the oldest, women, and low-educated people. The multimorbidity prevalence almost doubles for those above 65 years old, a third of which have over five concomitant chronic illnesses. Also, a person with multimorbidity is approximately three and nine times more likely to report very limited physical capacity and poor health status, respectively. In addition, multimorbidity is associated with greater healthcare use, namely clinical medical appointments and hospitalizations. Ageing of the population will make this scenario worse if no public health strategy is implemented, with an expected multimorbidity increase of 13.1% until 2050.
As expected, the number of disorders increases drastically with age, confirming results from the literature (van den Akker et al. 1998; Walker 2007; Salisbury et al. 2011; Barnett et al. 2012), particularly after 45 years, which might cause absenteeism and early retirement among those still below 65 years. Women seem to be particularly vulnerable, having higher average number of chronic health conditions overall. For instance, among those aged between 65 and 69, on average, women have approximately one more illness than men. Therefore, despite the fact that women generally live longer than men (http://ec.europa.eu/eurostat/), they suffer more illnesses, which can explain their self-reported health. (Boerma et al. 2016) Although a systematic review of most previous studies indicated that women had greater prevalence of multimorbidity compared with men (Violan et al. 2014), a cross-sectional analysis in a Portuguese primary care setting did not observe any gender difference regarding the adjusted risk of multimorbidity. Differences in the setting (e.g. primary care, which will necessarily underrepresent those without multimorbidity) and study design (e.g. selection bias might occur if men tend to seek medical help less frequently and in poorer health stages than women) may explain this inconsistency. There might be several reasons underlying the gender difference regarding the multimorbidity prevalence, including the socio-economic status (e.g. women having disadvantaged access to economic resources and high social status, which are strong determinants of good health) (Charles 2011; Perelman et al. 2012) and awareness of health status itself (women’s higher use of medical appointments increases awareness and therefore higher self-reporting of morbidity compared to men) (Verbrugge 1982; Cleary et al. 1982; Bertakis et al. 2000).
The literature consistently shows that lower education is associated with greater risk of multimorbidity (Nagel et al. 2008a, b). The results of our study confirm this relationship for Portugal. Low education might increase the risk of developing the co-occurrence of multiple diseases through different routes, namely lifestyle factors, such as smoking, sedentarism, obesity, and a lower capacity to prevent and manage disease and to avoid its deterioration (Feinstein et al. 2006). It would be interesting to further explore the intermediate role of lifestyle factors and others (e.g. psychosocial and environmental factors) on the association between education and multimorbidity within the same population-based sample of INS.
Finally, our study also showed that multimorbidity is highly associated with poor health status, lower physical capacity, and healthcare use, namely hospitalizations, which is consistent with the earlier literature (Salisbury et al. 2011; Barnett et al. 2012; Treadwell 2015; Valderas et al. 2007; Richardson et al. 2017).
Limitations and strengths
This study is hampered by some limitations that need to be stated. First, the cross-sectional design of the study does not allow for an evaluation of the causal mechanism from multimorbidity to health perception and healthcare use. The causality question is, however, beyond the scope of our paper, which is more focused on showing the present and future burden of multimorbidity in an ageing society.
Secondly, the analysis is based on self-reported data, which might be subject to recall bias and misclassification bias (e.g. multimorbidity not clinically confirmed). However, evidence suggests that self-reported morbidity is a reliable predictor of morbidity, in that it does not differ largely from physician-reported data (Ferraro and Su 2000). On the other hand, participants were asked to report chronic conditions from a pre-defined list, which might have caused an underestimation of multimorbidity. Note, however, that the most prevalent diseases were included in the list so that the risk of underestimation is reduced. Furthermore, it is possible that underreporting might have taken place among those who consult less and/or are less aware of their own chronic condition. This situation is more likely to occur among low-educated groups (with lack of health literacy and awareness), thereby leading to further underestimation of self-reported morbidity.
Thirdly, our projections of multimorbidity prevalence may be biased. We considered only the population up to 79 years old. Also, all calculations were based on the demographic dynamics (i.e. changes in the proportion of age groups’ dimension) and do not reflect any other variations that might occur in future and impact multimorbidity prevalence (e.g. antibiotics resistance, economic cycles, education improvements). Furthermore, as mentioned above, age group prevalence estimates of multimorbidity were adjusted to relevant cofactors, but this adjustment was fixed throughout time (i.e. same strength of association between selected cofactors and multimorbidity from 2014 until 2050). This assumption might be incorrect, since the relationship between any current risk factor and multimorbidity may change in the coming years. Nevertheless, this limitation was impossible to overcome, given the unpredictability around the evolution of the interplay between risk factors and multimorbidity.
This study has several strengths too. It is a nationwide population-based survey that addressed a large representative sample of the Portuguese population and is very unlikely to pose any sort of selection bias.
Policy implications
Our projections for the following decades, based on the official estimates on the demographic dynamics, show that multimorbidity is high and will steadily rise, reaching by 2050 almost half of the entire population. This growth will certainly be accompanied by additional challenges at the clinical level (i.e. physicians having to deal with several concomitant diseases within a frailty context of an increasingly older patient population) and at the financial level, given the economic burden associated with multimorbidity. By the year 2050, a third of the population will be over 65 (https://www.ine.pt). If another third of this age group remains highly multimorbid (> 5 chronic conditions), as we have shown in this research, then almost a tenth of the entire population will be highly multimorbid, which will represent a serious public health concern.
It is true that the expected growth of multimorbidity until 2050 might be seen relatively low (13.1%); however, one has to bear in mind that these projections are only based on the expected evolution of age groups and that all estimates are adjusted to relevant factors, including education. In future, elderly people will be more educated, which means that the age effect on multimorbidity will decrease (e.g. educated people being more prone to health prevention and healthy habits). However, risk factors, such as sedentarism and unhealthy lifestyles, may increase because of their greater prevalence in younger cohorts (Gortmaker et al. 2011; Tackling obesities: future choices—project report 2007), further contributing to increasing morbidity.
Co-occurrence of ill health conditions is non-random, as previously reported in the literature (Formiga et al. 2013). This should trigger a system response, for instance, by promoting cooperation between specialties that deal with the frequently found concomitance. As an example, cardiologists, who have to manage hypertensive patients, and rheumatologists, who also deal with frequent diseases, such as arthritis, may cooperate with psychiatrists or psychotherapists in order to better approach the coexistence of these frequent pathologies with depression. At least for some chronic conditions, this sort of multidisciplinary integrated care approach has already shown positive results (Fann et al. 2012; Rijken and Bekkema 2011). The expected growth of multimorbidity in the coming future makes it even less reasonable to keep the current silo model of insufficient cooperation among specialties (Richardson et al. 2017). Collaboration between different healthcare professionals is indeed at the heart of integrated care for people with multimorbidity. (Richardson et al. 2017; Nuño et al. 2012).
Conclusions
In conclusion, multimorbidity is already commonly found in the Portuguese population and it is expected to grow. Society should prioritize further research on this topic and define health policies specifically targeting patients with multimorbidity as well as those at higher risk, given the potential risk factors identified in this research.
References
Anderson G (2010) Chronic care: making the case for ongoing care. http://www.rwjf.org/en/researchpublications/find-rwjf-research/2010/02/chronic-care.html. Accessed Nov 2017
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B (2012) Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet 380(9836):37–43
Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA (2000) Gender differences in the utilization of health care services. J Fam Pract 49:147–152
Boerma T, Hosseinpoor AR, Verdes E, Chatterji S (2016) A global assessment of the gender gap in self-reported health with survey data from 59 countries. BMC Public Health 30(16):675
Charles M (2011) A world of difference: international trends in women’s economic status. Annu Rev Sociol 37:355–371
Cleary PD, Mechanic D, Greenley JR (1982) Sex differences in medical care utilization: an empirical investigation. J Health Soc Behav 23:106–119
DeSalvo KB, Fan VS, McDonell MB, Fihn SD (2005) Predicting mortality and healthcare utilization with a single question. Health Serv Res 40(4):1234–1246
Diederichs C, Berger K, Bartels D (2011) The measurement of multiple chronic diseases—a systematic review on existing multimorbidity indices. J Gerontol A Biol Sci Med Sci 66:301–311
European Commission (2015) DG ECFIN, The 2015 ageing report, economic and budgetary projections for the 28 EU member states (2013–2060). In: European economy 3/2015. http://ec.europa.eu/economy_finance/publications/european_economy/2015/pdf/ee3_en.pdf. Accessed Nov 2017
EUROSTAT. http://ec.europa.eu/eurostat/. Accessed Nov 2017
Fann JR, Ell K, Sharpe M (2012) Integrating psychosocial care into cancer services. J Clin Oncol 30(11):1178–1186
Feinstein L, Sabates R, Anderson TM, Sorhaindo A, Hammond C (2006) What are the effects of education on health? In measuring the effects of education on health and civic engagement. In: Proceedings of the Copenhagen symposium. OECD, pp 117–354
Ferraro KF, Su Y (2000) Physician-evaluated and self-reported morbidity for predicting disability. Am J Public Health 90(1):103
Formiga F, Ferrer A, Sanz H, Marengoni A, Alburquerque J, Pujol RM (2013) Patterns of comorbidity and multimorbidity in the oldest old: the Octabaix study. Eur J Intern Med 24:40–44
Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu A, Maltais D (2004) Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes 2:51
Gijsen R, Hoeymans N, Schellevis F, Ruwaard D, Satariano W, Bos G (2001) Causes and consequences of comorbidity: a review. J Clin Epidemiol 54:661–674
Gortmaker SL, Swinburn BA, Levy D, Carter R, Mabry PL, Finegood DT, Huang T, Marsh T, Moodie ML (2011) Changing the future of obesity: science, policy, and action. Lancet 378(9793):838–847
Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 38:21–37
INE. https://www.ine.pt. Accessed Nov 2017
Instituto Nacional de Estatística - Resident Population Projections. https://www.ine.pt and file:///C:/Users/pedro.laires/Downloads/28ProjPopresidPort2012_2060ingles.pdf. Accessed Nov 2017
Instituto Nacional de Estatística. Inquerito Nacional de Saúde 2014. INE. Lisboa: INE; 2016. 310 p
Jagger C, Gillies C, Cambois E, Al E (2010) The Global Activity Limitation Index measured function and disability similarly across European countries. J Clin Epidemiol 63:892–899
Kadam U, Croft P, North Staffordshire GP Consortium Group (2007) Clinical multimorbidity and physical function in older adults: a record and health status linkage study in general practice. Fam Pract 24:412–419
Kaplan GA, Haan MN, Cohen RD (1992) Risk factors and the study of prevention in the elderly: methodological issues. In: Wallace RB, Woolson RF (eds) Epidemiologic study of the elderly. Oxford University Press, New York, pp 20–36
Kawada T (2003) Self-rated health and life prognosis. Arch Med Res 34:343–347
Miilunpalo S, Vuori I, Oja P, Pasanen M, Urponen H (1997) Self-rated health status as a health measure: the predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J Clin Epidemiol 50(5):517–528
Mortality Data (2013) World Health Organization, Geneva. http://www.who.int/gho/mortality_burden_disease/life_tables/en/index.html. Accessed Nov 2017
Mossey JM, Shapiro E (1982) Self-rated health: a predictor of mortality among the elderly. Am J Public Health 72:800–808
Nagel G, Peter R, Braig S, Hermann S, Rohrmann S, Linseisen J (2008a) The impact of education on risk factors and the occurrence of multimorbidity in the EPIC-Heidelberg cohort. BMC Public Health 8:384
Nagel G, Peter R, Braig S, Hermann S, Rohrmann S, Linseisen J (2008b) The impact of education on risk factors and the occurrence of multimorbidity in the EPIC-Heidelberg cohort. BMC Public Health 11(8):384. https://doi.org/10.1186/1471-2458-8-384
Navickas R, Petric V-K, Feigl AB, Seychell M (2016) Multimorbidity: what do we know? What should we do? J Comorbidity 6(1):4–11
Nuño R, Coleman K, Bengoa R, Sauto R (2012) Integrated care for chronic conditions: the contribution of the ICCC Framework. Health Policy 105(1):55–64
Ornstein SM, Nietert PJ, Jenkins RG, Litvin CB (2013) The prevalence of chronic diseases and multimorbidity in primary care practice: a PPRNet report. J Am Board Fam Med 26(5):518–524
Oyen H, Van der Heyden J, Perenboom R, Jagger C (2006) Monitoring population disability: evaluation of a new Global Activity Limitation Indicator (GALI). Soz Praventivmed 51:153–161
Perelman J, Fernandes A, Mateus C (2012) Gender disparities in health and healthcare: results from the Portuguese National Health Interview Survey. Cad Saude Publica 28(12):2339–2348
Ramond-Roquin A, Fortin M (2016) Towards increased visibility of multimorbidity research. J Comorbidity 6(2):42–45
Richardson E, Van Ginneken E, Richardson E, Figueras J, Kluge H, Lessof S, McDaid D, Mossialos E, Permanand G, North J, White C (2017) How to improve care for people with multimorbidity in Europe? Copenhagen (Denmark): European Observatory on Health Systems and Policies. European Observatory Policy Briefs
Rijken PM, Bekkema N (2011) Chronic disease management matrix 2010. Results of a survey in ten European countries. NIVEL, Utrecht
Robine JM, Jagger C, Euro-REVES Group (2003) Creating a coherent set of indicators to monitor health across Europe: the Euro-REVES 2 project. Eur J Public Health 13:6–14
Salisbury C, Johnson C, Purdy S, Valderas JM, Montgomery A (2011) Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract 582:e12–e21
Statistics Portugal: methodological details of the National Health Survey, including sampling weights. https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=263714091&PUBLICACOESmodo=2&xlang=en. Accessed Nov 2017
Sundquist J, Johansson SE (1997) Self reported poor health and low educational level predictors for mortality: a population based follow up study of 39,156 people in Sweden. J Epidemiol Community Health 51:35–40
Tackling obesities: future choices—project report. 2007 Oct 17. http://www.foresight.gov.uk/Obesity/Obesity_final/Index.html
Treadwell J (2015) Coping with complexity: working beyond the guidelines for patients with multimorbidities. J Comorbidity 5(1):11–14
Valderas JM, Starfield B, Roland M (2007) Multimorbidity’s many challenges: a research priority in the UK. BMJ 334(7604):1128
Van den Akker M, Buntix F, Knottnerus JA (1996) Comorbidity or multimorbidity: what’s in a name? A review of literature. Eur J Gen Pract 2:65–70
van den Akker M, Buntinx F, Metsemakers JFM, Roos S, Knottnerus JA (1998) Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. J Clin Epidemiol 51:367–375
Verbrugge LM (1982) Sex differentials in health. Public Health Rep 97:417–437
Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, Glynn L, Muth C, Valderas JM (2014a) Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE 9(7):e102149
Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, Glynn L, Muth C, Valderas JM (2014b) Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE 9:e102149
Walker A (2007) Multiple chronic diseases and quality of life: patterns emerging from a large national sample, Australia. Chronic Illn 3:202–218
WHO (2011) Global status report on noncommunicable diseases 2010: description of the global burden of NCDs, their risk factors and determinants. World Health Organization, Geneva. http://www.who.int/nmh/publications/ncd_report2010/en/. Accessed Nov 2017
Wolff J, Starfield B, Anderson G (2002) Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 162:2269–2276
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Pedro Laires is a Novartis employee. The current project was, however, developed during his postdoctoral internship at Nova University and was totally unrelated to any Novartis product or Grant.
Additional information
Responsible editor: Matthias Kliegel.
Appendices
Appendix 1
See Table 2.
Appendix 2
Appendix 3: Absolute numbers and percentage of sample and due projected population’s distribution according to number of chronic health conditions
NR disorders | Sample | Population | Percentage (%) |
|---|---|---|---|
0 | 5441 | 2,764,162 | 35.8 |
1 | 2568 | 1,269,005 | 16.9 |
2 | 1985 | 947,338 | 13.1 |
3 | 1625 | 733,925 | 10.7 |
4 | 1326 | 549,397 | 8.7 |
5 | 931 | 402,049 | 6.1 |
6 | 652 | 270,974 | 4.3 |
7 | 350 | 129,241 | 2.3 |
8 | 188 | 76,082 | 1.2 |
9 | 80 | 24,235 | 0.5 |
> = 10 | 50 | 17,118 | 0.3 |
Total | 15,196 | 7183,526 |
Rights and permissions
About this article

Cite this article
Laires, P.A., Perelman, J. The current and projected burden of multimorbidity: a cross-sectional study in a Southern Europe population. Eur J Ageing 16, 181–192 (2019). https://doi.org/10.1007/s10433-018-0485-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10433-018-0485-0