
Abstract
This study examines and quantifies the linkages between population health, environmental risks, and its determinants for drinking water in New Zealand using routinely collected data. It was conducted as part of the national environmental health indicators project in New Zealand. The project is based on the World Health Organization’s (WHO) “Environmental and Health Information System” program. Drinking water quality indicators based on the Driving force–Pressure–State–Exposure–Effect–Action (DPSEEA) framework as part of this program were analyzed to validate the model by quantifying the linkages between the indicators. The results of the model suggested over the study period, the state (drinking water quality) and exposure (water access) indicators are significant independent predictors of the effect indicator (waterborne disease rate). This study suggests that routinely collected data can be structured using the DPSEEA framework and tested quantitatively using standard Poisson regression models, thus, illustrating that the model can be used routinely to provide a basis for consideration of the costs and benefits of any interventions to reduce the burden of waterborne disease. Data quality issues need to be considered if such routinely collected data linkages are to be performed for policy purposes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
This study was conducted as part of the national environmental health indicators project in New Zealand to assess the framework and linkages between population health, environmental risks, and its determinants for drinking water using routinely collected data. The aim was to empirically test the Driving force–Pressure–State–Exposure–Effect–Action (DPSEEA) framework (model) in the New Zealand context by examining and quantifying the relationship between the four indicators within the DPSEEA framework for drinking water quality, namely: the state indicator, Escherichia coli (E. coli) exceedance; the exposure indicator, water access; the effect indicator, waterborne disease; and the action indicator, monitoring intensity. All four indicators are based on the World Health Organizations’ Environmental Health Indicators project (World Health Organization, 2004).
Drinking water contamination has long been associated with gastrointestinal diseases. Approximately 4% of deaths (2.2 million) and 5.7% of disability adjusted life years (82 million) worldwide are attributable to unsafe water and poor sanitation and hygiene (Pruss et al., 2002); 99.8% of these deaths are in developing countries, of which 90% are in children (World Health Organization, 2002). However, the actual burden of waterborne disease is thought to be significantly higher than routinely collected data suggests. This is due to underreporting; attributing cases to specific risk factors is often difficult due to the ubiquitous and multifactorial nature of the hazards in the population (Ford, 1999).
The relationship between microbial drinking water quality and disease, mainly gastrointestinal illness (GI) has been widely studied with well-designed studies. A Russian cohort study (Egorov et al., 2003) suggested that higher effluent water turbidity at the treatment plant was a significant risk factor for GI. Two randomized trials (Payment et al., 1991, 1997) have suggested that drinking water meeting conventional standards may cause between 14% and 34% of GI in the community. Conversely, a number of other well-designed studies have not confirmed this observation (Strauss et al., 2001; Hellard et al., 2001). There have been a few studies examining this relationship on a national scale. However, most have focused on a smaller spatial level like a city or community, or a specific event, e.g., outbreak.
New Zealand has high rates of enteric diseases. This has led to several studies investigating the relationship between waterborne diseases and environmental and other population level risk factors. A study (Duncanson et al., 2000) examining the relationship between the incidence of human cryptosporidiosis and indicators of community drinking water quality found that the rates of notified cryptosporidiosis were highest in areas without routine water testing and which had failed fecal coliform testing. Another New Zealand study found that people living in areas of socioeconomic deprivation are at a greater risk, specifically, in urban areas. The odds of water supplies being “high risk” were 3.76 times (95% CI: 2.95–4.78) greater for the most deprived area compared with the least deprived area (Hales et al., 2003). A case control study (Hoque et al., 2002) investigated risk factors for giardia infection and identified consumption of drinking water from local supplies other than metropolitan mains’ supplies as a significant risk factor (OR = 2.11, 95% CI: 1.36–3.27).
These studies reconfirm that there is a complex relationship between environmental risk factors, and the burden of disease from drinking waterborne disease. It is useful to have a framework that can structure and analyze the relationships between these factors. The DPSEEA framework is an ideal framework for this. The framework allows the interpretation of complex environmental health issues by demonstrating clearly the links and relationships between the environment and human health. This approach has been in use for 10 years and been used by many agencies and countries to develop indicators in a wide range of environmental health issues. It has also been extensively used by the World Health Organization (WHO) and other UN agencies (World Health Organization, 2004). It is currently being used as the basis for the development of national environmental health indicator data sets in many countries worldwide, including New Zealand.
The framework covers a number of environmental health topics/areas, and derives a set of indicators, encompassed within the DPSEEA linkage framework in six stages as illustrated in Figure 1 (Corvalan and Kjellstrom, 1995; Kjellstrom and Corvalan, 1995). The DPSEEA framework is a descriptive representation of the way in which various driving forces generate pressures that affect the state of the environment and ultimately human health, through various exposure pathways by which people come into contact with the environment. The focus in this study is on those indicators, which are of closest association with population health—the “downstream” DPSEEA elements including state, exposure, and effect indicators.

DPSEEA framework illustrating the water quality indicators. This model describes the six components of the environmental health chain: Driving Forces, Pressures, State, Exposures, Effects, and Actions.
The State of the environment is often modified though pressures on the environment. In the drinking water issue, this is reflected in both the microbial and chemical contamination of the water. The deterioration in the state of the environment, however, only poses risks to human well-being when there is an interaction between people and the hazards in the environment. Exposure, therefore, is rarely an automatic consequence of the existence of a hazard: it requires that people are present both at the place and at the time that the hazard occurs. Hence, an indication of exposure to hazards from microbial contamination of water is access to safe drinking water. Exposure to environmental hazards such as microbial contamination, in turn, leads to (a range of) health Effects, such as enteric diseases. Finally, in response to the actual or potential health effects, a range of preventive or remedial Actions may be implemented (World Health Organization, 2002, 2004; Corvalan and Kjellstrom, 1995). These actions may range from regular water monitoring, water risk management plans, as well as increased protection and treatment of source water.
The various stages as outlined above form a logical causal chain. The linear nature of the framework allows a clear articulation of the connections between adjacent components. However, the reality is likely to be far more complex with many interactions between components occurring at different levels (see Fig. 1).
The New Zealand environmental health indicators project has adhered to international best practice by adopting the DPSEEA framework and the WHO–Europe environmental health indicators project as the conceptual framework and the basis of the New Zealand project. The ECOEHIS (Development of Environment and Health Indicators for European Union Countries) project is conducted by the WHO to develop methods and tools for the Environmental and Health Information System (EHIS) (European Centre for Environment and Health, 2004). The project objective was to establish a core set of environmental health (EH) indicators for the European Union (EU) countries, covering the topics related to important areas of living conditions such as air pollution, noise, housing conditions, road accidents and water pollution (World Health Organization, 2004).
Methods
This study was primarily designed to validate the association between the four drinking water quality indicators within the DPSEEA framework. The four indicators represent different stages of the framework. The indicators are based on the WHO indicator set (World Health Organization, 2000). The indicators have been adjusted to the New Zealand context mostly reflecting data availability.
The four indicators are: the state indicator, E. coli exceedance; the exposure indicator, water access; the effect indicator, waterborne disease; and the action indicator, monitoring intensity.
New Zealand has a population of 4 million people and is divided into 74 administrative districts called Territorial Local Authorities (TLAs). The data on all indicators is collected from TLA level and was collated for 5 years, 1998–2002. At the time of the study, the TLA level is the lowest spatial unit for which data for all four indicators was available.
State Indicator: E. coli Exceedance
The WHO indicator that this was based on is the “Exceedance of WHO Drinking Water Guidelines for Microbiological Parameters.” This is defined as the proportion of drinking water samples with E. coli or with fecal streptococci exceeding the guideline value of 0/100 ml water over a given time period (World Health Organization, 2000).
The indicator used in this study comprises the proportion of drinking water samples with E. coli exceeding the guideline value of 0 per 100 ml of water annually by TLA. This information is derived from the Water Information New Zealand (WINZ) database. The WINZ database is an electronic database system for handling a variety of data on drinking water quality in New Zealand. The data on WINZ is derived from local authorities, water suppliers, and local health agencies (Ministry of Health, 2003).
Exposure Indicator: Water Access
The WHO indicator that this was based on is the “Supply from Public Water Supplies.” This is defined as the percentage of the population supplied from a public water supply to the home (World Health Organization, 2000).
The indicator used in this study comprises the percentage of the population on a registered reticulated drinking water supply annually by TLA. A registered water supply means a drinking water supply serving more than 25 people for more than 60 days a year. This data was also obtained from the WINZ database. TLAs supply drinking water to approximately 95% of the population who are on a registered water supply. However, 11% of the population is supplied by a nonregistered water supplier (Ministry of Health, 2003).
Effect Indicator: Waterborne Disease
The WHO indicator that this was based on is part of the extended set of environmental health indicators, “Number of Cases of Proven Waterborne Diseases” (World Health Organization, 2000).
The indicator used in this study comprises the annual drinking waterborne disease rate per 100,000 population by TLA. The data for this indicator are from the National Notifiable Disease Surveillance System, EpiSurv (the New Zealand national communicable disease database). The rate was calculated from the following notifiable diseases where drinking water was recorded as the main mode of transmission. These included gastroenteritis, campylobacteriosis cholera, cryptosporidiosis, giardiasis, paratyphoid, salmonellosis, shigellosis, typhoid, primary amoebic meningoencephalitis, hepatitis A, legionellosis, leptospirosis, vero/shiga-toxigenic, and Escherichia coli.
Definition of the disease transmission route is the responsibility of the investigating health professional and this information is subsequently recorded in EpiSurv. Only laboratory confirmed cases have been used for these analyses. Cases with recent overseas travel have been excluded. Cases that were identified as part of a common source outbreak were also excluded.
Denominator population data were taken from the estimated census population for each year and each TLA, and the attribution of cases to geographic locale were based on the domicile of the case at the estimated time of exposure. Cases were geocoded by TLA, which are the principal loci for the monitoring and management of water quality and investigation of waterborne disease.
Action Indicator: Monitoring Intensity
The WHO indicator that this was based on is part of the extended set of environmental health indicators, “Intensity of Water Quality Monitoring.” This is defined as number of valid measurements per pollutant/capita/year (World Health Organization, 2000).
The indicator used in this study comprises the number of drinking water samples monitored annually for E. coli per capita, and reflects the intensity of drinking water monitoring by the supplier in each TLA.
Analysis
The data for each of the four indicators were plotted as histograms and mapped by TLA to illustrate the spatial distribution of the indicators across the country. A trend analyses was done to assess the temporal variation of each indicator over the 5-year period.
Poisson regression modeling was used to assess the association between the above-mentioned indicators within the DPSEEA framework. This allows the analysis of dependent variables, which follow Poisson distribution, i.e., a distribution frequently encountered when counting a number of events, or concerning the rate of occurrence with nonnegative integers. For this study, two statistical models were used. The first model assessed the relationships between the effect indicator, waterborne disease rate, and the influence on it from: a) the state indicator, E. coli exceedance; and b) the exposure indicator, water access. The hypothesis was that an increase in the waterborne disease rate would be associated with an increase in E. coli exceedance and a decrease in water access, as shown in Figure 2.

MODEL 1: Tri-Indicator Model illustrating the relationship between state indicator, E. coli exceedance, the exposure indicator, water access, and the effect indicator, waterborne disease rate.
The second model assessed the relationship between the effect indicator, waterborne disease rate, and the action indicator, monitoring intensity. The hypothesis was that an increase in the disease rate would be followed by an increase in the intensity of monitoring, as shown in Figure 3.

MODEL 2: Effect–Action Model illustrating the relationship between the effect indicator, waterborne disease rate, and the action indicator, intensity.
For both models, the Poisson regression model was used which assumes that:
where _ is (1) the waterborne disease rate or (2) the intensity of monitoring, Xi to Xn are the predictor variables, _o is the intercept, _i is the regression coefficient for predictor variable i, with i >1. Since a Poisson variable is assumed to have a mean > 0, log transformation ensures that the model-based predictions of rates are constrained to be greater than, or equal to, zero.
A P-value of less than 0.05 was considered statistically significant in this study. Statistical analyses were performed using the Statistical Analysis Software (SAS) system version 8.2. Poisson regression analyses were performed with PROC GENMOD, in SAS.
Results
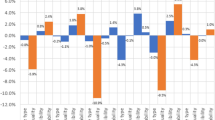
Table 1 and Figure 4 illustrate the temporal and spatial distribution nationally of the four indicators over the 5-year period, 1998–2002.

A: Distribution of drinking water quality indicator. B: Distribution of water access indicator. C: Distribution of waterborne disease rate. D: Distribution of intensity indicator.
Over the time, the state indicator, the annual E. coli exceedance, has decreased, indicating that the quality of the monitored drinking water has improved. Table 1 shows there was a nonsignificant decrease in the proportion of samples nationally that exceeded the E. coli guidelines from 3% in 1998 to 2% in 2002. The geographical distribution of E. coli exceedance is shown in Figure 4A for the period 1998–2002. The national annual mean for the period was 2.5% of samples exceeded the E. coli guideline value with a range of 0%–25.3% <suppl F4>(online appendix). There were four TLAs (5%) where the proportion of samples exceeding E. coli guideline values were significantly higher than the national average.
Water access has increased over the 5 years indicating that there are more people on a registered water supply. The percentage of the population on a registered water supply has increased nonsignificantly from 82.2% in 1998 to 83.2% in 2002. The geographical distribution of water access is shown in Figure 4B for the period 1998–2002. The national annual mean of the population on a registered drinking water supply for the period was 83.6% with a range from 44.0% to 100% <suppl F4>(online appendix). Nineteen TLAs (26%) had a significantly lower percentage of the population on a registered water supply than the national average. Twenty-nine TLAs (40%) had significantly higher percentage than the national average.
The national notifiable drinking waterborne disease rate per 100,000 remained relatively constant from 1998 to 1999 (18.0–19.7), however, from 1999 to 2001, there was a significant increase (19.7, 51.2, and 85.2, respectively), and from 2001 to 2002, a nonsignificant decrease (85.2–68.9). The geographical distribution of disease rates for the period 1998–2002 is shown in Figure 4C. The mean annual waterborne disease rate per 100,000 population for the period was 48.6 cases per 100,000 population with a range from 2.9 to 178.5 cases per 100,000 <suppl F4>(online appendix). Seventeen TLAs (23%) had a mean annual disease rate significantly higher than the national average and 16 TLAs (22%) had a significantly lower disease rate than the national average.
The intensity of monitoring increased over the period suggesting an increase in drinking water monitoring, i.e., more samples per capita monitored. The intensity of water quality monitoring has increased nonsignificantly from 1.7 samples monitored per capita in 1998 to 2.3 samples monitored per capita in 2002. Figure 4D illustrates the geographical distribution of the intensity of drinking water monitoring for the years 1998–2002. The national average was two samples monitored annually per capita with a range from 0.3 samples to 8.1 samples per capita <suppl F4>(online appendix). Only two TLAs (3%) sampled significantly more per capita than the national average.
The first model, as illustrated in Figure 2, was developed to assess the relationships between the waterborne disease rate and the “explanatory” factors, i.e., E. coli exceedance, water access, time period (year), and whether the predictor variables for E. coli exceedance vary by water access group. Table 2 presents the results of this model fit.
The Poisson regression model suggests that E. coli exceedance and water access are significant independent predictors of waterborne disease rate. Specifically the model indicates that the increase in E. coli exceedance and decrease in water access correspond to a significant annual increase in the drinking waterborne disease rate.
There is a statistically significant association between the interactions of the two parameters “E. coli exceedance” and “water access” on the waterborne disease rate. The point estimate for the E. coli exceedance in the water access, “below national average group” is 0.0257 and for the “above national average group” is 0.1557 (0.0257 + 0.1300). The higher rate ratio for water access, “above national average group,” suggests that the relationship between E. coli exceedance and drinking waterborne disease rate, is more robust for the water access “above the national average group” compared to the “below the national average group.”
Figure 3 illustrates the second model, which assesses the relationship between the action indicator “intensity,” and the effect indicator “waterborne disease rate.” The coefficients from fitting the model were _o = -4.6678, _i = 0.0067 with SE(_o) = 0.0051 and SE(_i) = 0.00001 with an associated P-value of <0.0001. This suggests that an increase in the waterborne disease rate is significantly associated with an increase in the intensity of monitoring.
The two models demonstrate a statistically significant association between the four drinking water indicators at a national level over the 5-year period, 1998–2002. More specifically, over this period, an increase in the percentage of E. coli exceedances was associated with a statistically significant increase in drinking waterborne disease at a national level. An increase in the percentage of the population on registered drinking water supply was associated with a statistically significant decrease in drinking waterborne disease. The increase in monitoring intensity was associated with an increase in the waterborne disease rate.
Both models confirm the intrinsic validity of the four indicators as well as their relationship within the DPSEEA framework. This suggests that the relationship is not a simple, linear relationship between the four indicators but rather a more complex interaction.
Discussion
This study demonstrates the potential utility of environmental health indicators as an important decision making tool. The use of the indicators within the framework provides an integrated assessment of both environmental and health information spatially and temporally, allowing comparisons across regions within the country over time. The utility of the framework and the indicators lies in their ability to connect previously disparate datasets using routinely collected data. As this study shows, this can lead to the better understanding of, as well as quantifying, the relationship between the environmental risk factors and population health. This type of study could assist in evaluating the effectiveness of policies and facilitate prioritizing resources.
This study highlights the possible application of routinely collected national datasets such as WINZ and EpiSurv for ecologic studies. This study represents the first time in New Zealand where both types of data have been collated and analyzed on a national scale. However, it should be emphasized that these observed associations apply only at a national scale and caution needs to be taken to extrapolate to a regional or local level due to small population numbers in some areas.
The linkage analyses in this study highlight some data quality issues. It has not been possible to quantify the error in key quality parameters like data quality and consistency in this study. One advantage of such an approach is that the population serves as its own control. From an epidemiological perspective, the indicators reflect endemic rather than epidemic presentations of disease.
One of the main data quality issues with ecologic studies using routinely collected data is that the data being used has been collected primarily for other purposes. One of the consequences is that the study relies heavily on the definitions applied by the organizations collecting the data. For example, individual officers investigating a case of communicable disease may apply the criteria used to define pathogen sources differently. This may result in a greater percentage of cases attributed to one source, for example, water, more than another, such as food. There is also a large margin of error, for instance, in the state indicator, E. coli exceedance, due to inconsistencies in reporting, sampling practices, and the analytical methods used.
Another data quality issue is the representativeness of the datasets. For instance, waterborne disease rates do not reflect the true rate in the community but are an underestimate due to underreporting and large numbers of gastrointestinal illness where there is no known origin.
However, one of the advantages this study has is that, in New Zealand, there is a reliable notifiable diseases surveillance system. This system has a significant waterborne disease component which records the likely mode of transmission of the communicable disease. This has enabled a more robust approach to assessing health effects related to drinking water quality.
Land use is the main driving force influencing drinking water quality in New Zealand. Land use patterns exert different pressures on source water. The main pressures in New Zealand are agricultural land use and urbanization. The urban area covers 1.9% of the land area but 87% of the population lives in towns and cities (Figure 5, <suppl F5>(online appendix)). These urban/rural differences are a factor in this study where access and quality of drinking water is heavily influenced by whether an area is urban or rural. This translates to different water quality management strategies being needed for urban and rural areas. This is because the main distinction between urban and rural land use is that urban land use is associated with point source pollution, whereas rural land use is associated with diffuse water pollution. Thus, point source pollution in urban areas can be managed through discharge permits, whereas diffuse pollution in rural areas needs other management tools. One of the recommendations from this study would be to examine the influence of driving forces like land use, as well as urban and rural pressures on the state of the environment and, subsequently, on population health.

Population distribution of the NZ population by TLA.
This study illustrates how the DPSEEA framework, the environmental health indicators, and using standard statistical methods can offer a basis for a better understanding of the linkages between environmental risk factors and population health, especially as a tool for environmental health decision making.
Abbreviations
- CI:
-
Confidence Interval
- DPSEEA:
-
Driving force – Pressure – State – Exposure – Effect – Action
- E.coli:
-
Escherichia coli
- EHI:
-
Environmental Health Indicator
- EpiSurv:
-
National Notifiable Disease Surveillance System
- GI:
-
Gastrointestinal illness
- OR:
-
Odds Ratio
- SAS:
-
Statistical Analysis Software
- TLA:
-
Territorial Local Authority
- WINZ:
-
Water Information New Zealand
- WHO:
-
World Health Organisation
References
Corvalan C, Kjellstrom T (1995) Health and environment analysis for decision making. World Health Statistical Quarterly 48:71–77
Duncanson M, Russel N, Weinstein P, Baker M, Skelly C, Hearndon M, et al. (2000) Rates of notified cryptosporidiosis and quality of drinking water supplies in Aotearoa, New Zealand. Water Research 34:3804–3812
Duncanson M, Russel N, Weinstein P, Baker M, Skelly C, Hearndon M, et al. (2000)Daily variations in effluent water turbidity and diarrhoeal illness in a Russian city. International Journal of Environmental Health Research 13:81–94
Egorov AI, Naumova EN, Tereschenko AA, Kislitsin VA, Ford TE (2003) Daily variations in effluent water turbidity and diarrhoeal illness in a Russian city. International Journal of Environmental Research 13:81–94
European Centre for Environment and Health (2004) Development of Indicators for European Union Countries—ECOHEIS, Bonn: WHO
Ford TE (1999) Microbiological safety of drinking water: United States and global perspectives. Environmental Health Perspectives 107(Suppl 1):191–206
Hales S, Black W, Skelly C, Salmond C, Weinstein P (2003) Social deprivation and the public health risks of community drinking water supplies in New Zealand. Journal of Epidemology and Community Health 57:581–583
Hellard ME, Sinclair MI, Forbes AB, Fairley CK (2001) A randomized, blinded, controlled trial investigating the gastrointestinal health effects of drinking water. Environmental Health Perspectives 109:773–778
Hoque ME, Hope VT, Kjellstrom T, Scragg R, Lay-Yee R (2002) Risk of giardiasis in Aucklanders: a case control study. International Journal of Epidemiology 6:191–197
Kjellstrom T, Corvalan C (1995) Framework for the development of environmental health indicators. World Health Statistical Quarterly 48:144–154
Ministry of Health (2003) Annual Review of the Microbiological and Chemical Quality of Drinking Water in New Zealand 2002, Wellington: Ministry of Health
Payment P, Richardson L, Siemiatycki J, Dewar R, Edwardes M, Franco E (1991) A randomised trial to evaluate the risk of gastrointestinal disease due to consumption of drinking water meeting current microbiological standards. American Journal of Public Health 81:703–708
Payment P, Siemiatycki J, Richardson L, Renaud G, Franco E, Prevost M (1997) A prospective epidemiological study of gastrointestinal health effects due to consumption of drinking water. International Journal of Environmental Health Research 7:5–31
Pruss A, Kay D, Fewtrell L, Bartram J (2002) Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environmental Health Perspectives 110:537–542
Strauss B, King W, Ley A, Hoey JR (2001) A prospective study of rural drinking water quality and acute gastrointestinal illness. Bio Medical Central Public Health 1:8. Available: http://www.biomedcentral.com/1471-2458/1/8
World Health Organization (2002) World Health Report 2002: Reducing Risks, Promoting Healthy Life, Geneva: World Health Organization. Available: http://www.who.int/whr/2002/en/Overview_E.pdf
World Health Organization, Regional Office for Europe (2000) Environmental Health Indicators: Development of Methodology for the WHO European Region. Interim Report. Available: http://www.euro.who.int/EHindicators
World Health Organization, Regional Office for Europe (2004) Environment and Health Information System. Available: http://www.euro.who.int/EHindicators
Acknowledgments
The authors thank and acknowledge the Ministry of Health (New Zealand) and the World Health Organization, European Centre for Environment and Health, Environment and Health Information Program—especially Dr. Dafina Dalbakova—for all their help and contribution to the environmental health indicators project.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplemental histograms are available in the online appendix.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Khan, R., Phillips, D., Fernando, D. et al. Environmental Health Indicators in New Zealand: Drinking Water—A Case Study. EcoHealth 4, 63–71 (2007). https://doi.org/10.1007/s10393-007-0089-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10393-007-0089-1