
Abstract
Background
The infant mortality rate was very high in Pakistan until the early 1990s, at 86 deaths/1000 live births. It has decreased 24 points and declined to 62 deaths/1000 in the last 3 decades, but Pakistan is still in the group of countries with highest infant mortality rate. The present study aimed to assess the magnitude of infant mortality in Pakistan and its causes and associated risk factors.
Methods
For this study, data from the 2018 Pakistan Demographic and Health Survey were used. Risk factors for infant mortality were first examined in bivariate analyses. Chi-square test was employed to understand the significance level of the categorical difference of independent variables. The Cox proportional hazard model was used to account for potential confounders that function as risk factors for infant deaths.
Results
Large differentials in infant survival by socioeconomic and demographic factors indicate poor coverage of social and health schemes for the public. Mothers who did not use the ANC services experienced about 1.5 times higher infant mortality than those who did (52 vs. 36/1000 LB; p = 0.007). The hazard model shows that rich households experienced about 30% (HR = 0.735; 95% CI = 0.614–0.878) less infant mortality than poor ones. The rural-urban differential in public health services and gender inequities are the underlying causes of the stagnation of infant mortality in Pakistan.
Conclusion
The low status of women’s education, poor economic conditions and low level of using public health care services are closely tied to higher infant death rates in Pakistan. Health interventions in Pakistan should be designed to reach the most under-served—women and children—especially in rural areas.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Globally, the annual infant death rate has declined from 8.8 million (65 deaths per 1000 live births) in 1990 to 4.1 million (29 deaths per 1000 live births), which contributed about three-fourth of all deaths of children < 5 years old, occurring within the first year of life in 2017. In Pakistan, the same infant death rates declined from 90 to 65/1000 live births for the same duration (The World Bank 2017; World Health Organization 2017). The number of babies in Pakistan who died before completing the first year of life was about 330,479, which is one of highest infant mortality rates (64 per 1000 live births), over eight times higher than the rate in the WHO European Region, which was 8 per 1000 live births (World Health Organization 2017).
Significant declines in infant mortality occurred in Pakistan between the 1950s and early 1960s, when large-scale public health programs were implemented. The decline in infant mortality slowed down between the early 1960s and late 1970s (Alam and Cleland 1984; Cleland and Sathar 1984; Irfan 1986; Sathar 1995; Sathar and Mallick 1991; Agha 2000). By the late 1980s and early 1990s, the decline in infant mortality appeared to have stagnated (Agha 2000): two independent national sample surveys showed that the infant mortality rate (IMR) in 1989 and 1992 was 101 per 1000 live births. These infant mortality levels are consistent with other estimates of the IMR for this period (United Nations Development Program 1994). However, the infant mortality stagnation in Pakistan appears to have occurred when the IMR was at a very high level and at a time when provincial and urban-rural differentials were large (Irfan 1986). Provincial differentials in infant mortality levels reflect distributional problems and are a source of political instability.
High infant mortality rates also have implications for rapid population growth: parents who fear that their newborns are not going to survive to older ages are likely to have more children. At 208 million (UNICEF 2018), Pakistan is already the sixth most populous country in the world. It scores poorly on all indexes of human development, and its political stability is threatened, in part, by unequal access to the limited economic resources. Socioeconomic inequalities have resulted from the concentration of political power in the powerful rural elite, poor economic and political management and the belief among the upper classes that rapid economic growth will trickle down to the poor. Lack of attention to distributional issues (Naseem 1981; Zaidi 1985) has contributed to substantial differences in access to income, nutrition, education, housing, water and sanitation within and between regions and to the slowdown in infant mortality decline.
Women’s autonomy and their social and economic status have important implications for their children’s health. Gender inequities remain an important determinant of women’s and children’s health in Pakistan. Relative to men, Pakistani women have always scored poorly on the United Nations Human Development Index. Most women in Pakistan are poor, illiterate and have low social and legal status (Patel 1991). The level of maternal mortality is among the highest in the world (Midhet et al. 1998). There were some improvements in the legal status of women in the early 1960s, but these advances were reversed because of a government-encouraged “Islamization” process that started during the late 1970s and continued through the 1980s.
Although infant mortality is extremely high, there is relatively little in the published literature about factors associated with infant survival in Pakistan. A few studies have been conducted on infant and child survival in Pakistan, but these have employed a limited range of variables in the analysis and have lacked a clearly defined conceptual framework. These studies have generally not used nationally representative data. Besides, several published studies did not use appropriate statistical methods (Agha 2000). The present study tried to access the significant risk factors of infant mortality and execute a more comprehensive analysis of factors related to infant survival in Pakistan than available in the published literature. The specific objective of this study was to investigate and assess the magnitude of infant mortality in Pakistan and its causes and associated risk factors. It utilizes the nationally representative, good-quality data of DHS Pakistan (Agha 2000), includes a spectrum of variables affecting child health and employs appropriate statistical methodology.
Data source and methodology
Data source
The Pakistan DHS (Demographic and Health Survey) was conducted in 1991, 2007, 2013 and 2018. This survey is a periodic, cross-sectional survey administered at the household level. For this study, data from the 2018 Pakistan Demographic and Health Survey were used. The survey collects information on different aspects of demographic indicators such as fertility, mortality (child and infant), fertility preferences and regulations, health status of mother and child, nutritional health status of mother and child, and awareness and attitude towards HIV/AIDS at the national level. Households in Pakistan were selected using two stages stratified using random sampling. In the first stage, 580 enumeration areas (EAs) were selected using a population proportionate to the EAs listed by the Census, and of these, 561 were successfully surveyed. In the second stage, 28 households per cluster (EAs) were selected to provide the key demographic and health variables with statistically reliable estimates for the country. For the total sample, approximately 16,240 households were selected for the survey. The target group was women aged 15–49 years. These women, who were the usual residents of the household or had stayed in the household the night before, were eligible to be interviewed for the survey. For stigmatization at the national level, all data of the survey were weighted, and interviews were conducted with 12,364 women aged 15–49 years.
Variables
In the present study, the variables were categorized as response and predictor variables.
Dependent variable
Infant mortality (1q0) is the probability of infant death before the first birthday. It was estimated as the probability of an infant dying before the first birthday.
Independent variables
The independent variables were divided into three categories: mother, child and household-related covariates.
-
1.
Mother-related variables: These variables consisted of the mother's education level (not educated; educated), occupation (not working; working), age at first birth (< 18 and ≥ 18 years), institutional delivery (no; yes) and antenatal checkups (no antenatal care; at least one) and accessed postnatal care.
-
2.
Child-related variables: These included the birth interval (< 2 years; 2 to 3 years; ≥ 3 years), birth size (average or larger; small or very small) and the child's sex (male; female).
-
3.
Household-related variables: The household variables were wealth index (poor; middle; rich), sanitation facilities (no; yes) and type of residence (rural; urban).
Statistical analysis
Bivariate and multivariate analyses were applied to estimate the association between infant mortality and its covariates. Bivariate analysis was performed to estimate the distribution of infant mortality in different groups of predictors. Multivariate analysis such as the Cox proportional hazard model was used to examine the impact of the mother, child and socioeconomic factors on the survival of infants during the first year of life. In this study, the Cox proportional hazard model was used as it is suitable for analyzing time-specific censored observations (D’agostino et al. 2008). The Cox proportional hazard regression model is useful for accessing the impact of lifetime-related factors on the hazard function. This model plays a significant role in the analysis of lifetime data.
Results
Figure 1 shows the trends of infant mortality in Pakistan for the last 3 decades. In 1990, infant mortality was recorded as 86 deaths per 1000 live births, which was close to the rate in African countries, and it decreased only 24 points over about 3 decades. The IMR was 62 for the recent round of the Pakistan DHS 2017–18. The graph shows that the highest pace of declining infant mortality was recorded during 2013–2018, although 62 infant deaths per 1000 live births (LBs) was far from the UN's Millennium Development Goals (MDGs) and Sustainable Development Goals (SDGs).

Trend of infant mortality per 1000 live births in Pakistan
Infant mortality risk factors
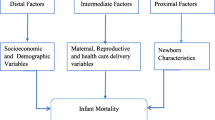
Table 1 shows the infant mortality risk factors according to the background characteristics in Pakistan. The risk factors were divided into three categories: mother-, child- and household-related factors. Of these factors, the most significant ones that influence the status of infant deaths were the occupational and educational status of the mother, the mother’s utilization of antenatal care, the birth interval and birth size and sex of the newly born baby, place of residence and wealth indices of the household.
In educated women, only 43 infant deaths were reported, while in non-educated mothers, the infant mortality was about 60/1000 live births (LB). Similarly, about 20 additional infant deaths per 1000 live births occurred in working mothers compared with mothers who were not working (68 to 49 deaths/1000 LB; p = 0.001). The results also revealed that mothers who had antenatal care during pregnancy had greater chances of survival of their respective infants. About 1.5 times more infant deaths occurred in the mothers who did not use the ANC services (52 deaths/1000 LB) compared with their counterpart women (36/1000 LB; p = 0.007).
In the child-related factors, birth interval and birth size played a significant role in controlling infant deaths. Newborns with a ≥ 2 year difference in birth interval had about 50% less probability of dying than those born in < 2 year birth intervals (35 vs. 78/1000 LB) with a high level of significance (p = 0.001). A similar pattern of infant mortality has been observed for the birth size variable. The rate was significantly higher among babies born to women who had a history of small or very small birth sizes compared with average or large birth size (77 vs. 46/1000 LB; p = 0.001).
For household risk factors, wealth index and urban place of residence were significant factors improving the infant death rate in Pakistan. The rate of infant deaths among the poor (60/1000 LB) was significantly higher than that among women who had a rich household index (42/1000 LB; p = 0.001). Similarly, in rural households, about 30% more infant deaths (57 per 1000 LB) were reported compared with their counterparts (44 infant deaths per 1000 LB) in urban resident households (p = 0.001).
Survival functions of major infant mortality controlling variables
Graph 2a, b and c represents the survival functions of infant mortality for the wealth index, birth interval and sex of the child, respectively. These survival graphs indicate that wealth indices of households, birth interval and sex of the child are the most significant social and demographic tools affecting infant mortality in Pakistan. While the gap in survival was highest for the birth interval, the lowest was recorded for the sex of child variable. These results show that infant mortality was less in the economically middle class and wealthy families than in their counterparts. Not surprisingly, the birth interval played an important role in infant deaths. The maximum birth interval that controls infant deaths in Pakistan was 2 years. Graph 2b shows that if the duration of the birth interval was ≥ 2 years, then it had a similar impact on infant mortality.

a Survival functions of infant mortality for the wealth index. b Survival functions of infant mortality for the birth interval. c Survival functions of infant mortality for sex of child
Results of survival analysis (Cox proportional hazard model)
Table 2 shows the results of the multivariate Cox model. Generally, the magnitude of effect for the factors considered here was stronger for the child- and household-related factors than mother-related factors. In terms of the hazard ratio, the important factors were the duration of the birth interval, birth size and wealth index of households. Although the working status of the mother is an important variable, it plays both positive and negative rolls. Results illustrated that educated mothers were about 30% less likely to experience infant deaths than uneducated mothers as the hazard ratio for infant mortality (IM) was 0.741 [95% confidence interval (CI) =0.545–1.006]. Working mothers also experienced increased mortality risk. The hazard ratio for IM was 1.307 (95% CI = 0.951–1.795) and about 30% less likely for non-working mothers. The utilization of antenatal care services and institutional delivery were also shown to be strongly associated with infant mortality. The mothers who had institutional delivery were less likely (HR = 0.959; 95% CI = 0.823–0.995) to experience infant deaths compared with their counterparts. Similarly, mothers who utilized antenatal care services were about 30% less likely to have infant mortality.
The time between the births of children and the birth size were strongly associated with mortality. However, because mortality within the family is correlated with birth spacing, our results must be considered with caution. Newborn babies whose birth spacing was > 3 years to their previous siblings was about 60% more likely to survive than those who had < 2 years birth spacing (HR = 0.433; 95% CI = 0.476–0.839). Both the birth size and sex of a child have a significant independent impact on mortality. These two variables are strongly correlated. Being male and having small or very small birth size of the infant were associated with increased infant mortality. Female infants were about 16% (HR = 0.844) less likely to suffer infant mortality, with 95% CI (0.723–0.984). Similarly, infants whose birth sizes were small or very small were 60% more likely to die before completion of 1 year of life than their counterparts.
Household factors had a significant effect on infant mortality, especially the wealth index and locality of residence. Urban residents had better opportunities for employment and health facilities; therefore, this could reduce the mortality rate. The hazard model shows that for the wealth index, rich households have about 30% (HR = 0.735; 95% CI = 0.614–0.878) less probability of infant mortality compared with the reference category. The households in urban regions had less probability of infant mortality compared with rural resident households (HR = 0.867; 95% CI = 0.670–0.965). Overall, we observed a highly significant reduction in mortality over the observed covariates in Pakistan.
Discussion
Available data on infant mortality in Pakistan were obtained from the Demographic Health Surveys, which collect retrospective data on infant mortality based on interviewing a sample of women of reproductive age. Infant mortality is often used as a critical indicator of the level of health care in countries. Neonatal deaths account for the majority of infant deaths (Batieha et al. 2016).
Main findings
The study found that a birth interval of < 2 years, smaller than average birth size, infants belonging to the poor household, wealth index quintile and being a rural resident were significantly associated with a higher risk of infant mortality in Pakistan. Other factors associated with infant mortality were: the mother's education level, non-utilization of antenatal care, non-institutional delivery and the sex of the infant. The findings are significant because the level of infant mortality in Pakistan is unacceptably high at 62/1000 live births. The current rate of decline is not sufficient for the country to reach its child survival MDG. Detection of these risk factors for infant deaths will help to formulate strategies and program innovations to improve infant survival.
Comparison with other studies
In agreement with a number of previous studies on infant deaths, inadequate antenatal care (Vintzileos et al. 2002), low birth size and weight (Sharma et al. 2008), male gender (Batieha et al. 2016; Sharma et al. 2008; World Health Organization 2014) and the birth interval (Batieha et al. 2016; Ronsmans 1996) were among the most prominent risk factors observed in this study. For this study, we tried to refrain from discussing the proposed mechanisms by which each of these factors contributes to infant mortality.
However, two observations in this study differ from what has been found in other studies and have implications for the potential effect of spacing programs on mortality. First, preceding birth intervals of 1–2 years did not affect neonatal or post-neonatal mortality. The latter finding merits attention since it is generally believed that children throughout the developing world experience a higher prevalence of mortality if they are born < 2 years after their mother’s previous birth (Boerma and Bicego 1992; Hobcraft et al. 1985; Preston 2013). Second, short succeeding birth intervals, in contrast, have significant adverse consequences for child survival, and the size of the effect was more substantial than those found by other authors (Boerma and Bicego 1992; Hobcraft et al. 1985; Sweemer 1984). Sufficient birth spacing has been promoted through mother-child health programs in many countries, as this is perceived to be beneficial for the health and well-being of both mother and child (Batieha et al. 2016; Binka et al. 1995; Defo 1997; Ronsmans 1996).
The current study illustrated that smaller than average birth size is an independent risk factor for infant mortality in Pakistan. The findings agree with several other studies that have identified low birth weight as a risk factor for infant mortality (Lawn et al. 2005; Richardson et al. 1993; Titaley et al. 2008; Yasmin et al. 2001). Low birth weight occurs because of either premature birth or in utero growth restriction, or both (Kramer 1987). An in-depth analysis of the PDHS data of 2006–2007 by the NIPS (National Institute of Population Studies) of Pakistan showed a strong association between small birth size and infant mortality. In a hospital-based retrospective study from Pakistan, 68% mortality in newborns was contributed by low birth weight. Furthermore, it suggested high mortality among low-birth-weight preterm infants (Tariq and Kundi 1999). Smaller birth size with complications is considered the leading cause of infant deaths in Pakistan (Khan et al. 2012; Liu et al. 2012).
For antenatal care, however, the variation depending on their level of health care was acknowledged (World Health Organization 2014). In agreement with the available literature, over three-fourths of infant deaths in our study were either preventable or possibly preventable. According to a WHO fact sheet (World Health Organization 2014), effective care can prevent three-fourths of infant deaths. The package of essential care includes antenatal care and the birth attendant’s ability to resuscitate newborns at birth. This is further supported by the findings showing that mothers who experience fewer infant deaths have received optimal medical care as ante- and postnatal care (Lau et al. 2013). Infants whose mothers had non-institutional delivery had a higher risk of infant death in our sample. The delivery needs to be managed by a skilled birth attendant in a well-equipped health facility. Studies have shown that deliveries in a health facility with a skilled birth provider reduce infant deaths (Målqvist et al. 2008).
The study illustrated that males are more prone to infant mortality in Pakistan. Similarly, many scholars have identified male gender as a risk factor for infant death (D’Souza and Chen 1980; Green 1992; Gupta 1987; Hobcraft et al. 1985; Muhuri and Preston 1991; Titaley et al. 2008). Biologically, male children have a higher risk of getting infectious diseases because of the higher prevalence of immune deficiency, respiratory illnesses and congenital malformations of the urogenital system due to late maturity, with probably all of these leading to higher neonatal mortality among males (Green 1992).
Being in the poorest household wealth index was identified as a risk factor for infant mortality in our analysis. Similar to our finding, secondary analysis in different countries and regions has also found a lower household wealth index to be a risk factor for poor infant and child health and higher infant mortality rates (Agha 2000; Batieha et al. 2016; Chauhan and Rai 2015; Knowles 1982; Nisar and Dibley 2014; Sastry 1997; Tariq and Kundi 1999; Titaley et al. 2008). Household poverty has been reported to increase infant mortality by reducing access to adequate care (Lawn et al. 2005).
In the current study infants whose mothers were not working had a lower risk of mortality in the infant period than those whose mothers were working (Agha 2000; Chauhan and Rai 2015; Curtis et al. 1993; Nisar and Dibley 2014; Sathar 1995). Others have reported increased odds of infant deaths due to lack of personal and timely care of infants born to working mothers. However, the mother’s employment status in PDHS only showed working during the last 12 months preceding the survey.
The present study attempts to analyze the infant mortality from children's file data in the Pakistan Demographic and Health Survey at the national level. Although the Pakistan Demographic and Health Survey provides accurate and detailed demographic information, this information is limited to the national level, urban and rural areas, and at most to the regional level because of the nature of sample surveys. This may cause an issue of sample size related to accurate prediction of results. On the other hand, this national-level analysis may not give the best result for small regions of the country when the sample size is representative at the national level. The other limitation of the present study is that it uses retrospective birth history information to analyze infant mortality and is likely to suffer from mothers' recall bias. The effect of memory bias can limit data quality.
Conclusion
Our study of Pakistan confirms the importance of all three major risk groups for infant mortality, that is, child-, mother- and household-related factors, including the socioeconomic status, social behavior, environmental conditions and use of health services. These findings showed the need for a broader approach to future child health programs to enable further reductions in infant mortality in Pakistan, especially in rural and poor areas. Such programs need to include improvements of accessibility to formal health services, specific attention to infants during their first year of life, emphasis on educating whole families about birth spacing and efforts to improve the accessibility of antenatal care, institutional delivery and postnatal services to mothers as well as continuing with improvements in the economic status of households. The infant mortality trends in Pakistan indicate that infant mortality declined slightly in the 28 years between 1990 and 2017. (The major contribution to this decline occurred in the extremes of the education of women, increased birth spacing and the economic status of households.) This decline may have resulted from the development programs carried out in the area during this period, specifically, the ‘Women’s Education and Home Development and Family Planning’ programs.
References
Agha S (2000) The determinants of infant mortality in Pakistan. Soc Sci Med 51(2):199–208
Alam I, Cleland J (1984) Infant and child mortality: trends and determinants. In: Alam I (ed) Fertility in Pakistan. Int Stat Inst, Voorburg, pp 187–209
Batieha AM, Khader YS, Berdzuli N, Chua-Oon C, Badran EF, Al-sheyab NA, Basha AS, Obaidat A, Ra’eda J (2016) Level, causes and risk factors of neonatal mortality, in Jordan: results of a national prospective study. Matern Child Health J 20(5):1061–1071
Binka FN, Maude GH, Gyapong M, Ross DA, Smith PG (1995) Risk factors for child mortality in northern Ghana: a case-control study. Int J Epidemiol 24(1):127–135
Boerma JT, Bicego GT (1992) Preceding birth intervals and child survival: searching for pathways of influence. Stud Fam Plan 23(4):243–256
Chauhan BG, Rai AK (2015) Factors affecting to the child health in urban India: a comparative study between two mega cities. Int Res J Soc Sci 4(5):43–51
Cleland JG, Sathar ZA (1984) The effect of birth spacing on childhood mortality in Pakistan. Popul Stud 38(3):401–418
Curtis SL, Diamond I, McDonald JW (1993) Birth interval and family effects on postneonatal mortality in Brazil. Demography 30(1):33–43
D’agostino R, Sullivan LM, Massaro J (2008) Cox proportional hazard model. Wiley Encyclopedia of Clinical Trials. Wiley-Interscience, New York
D’Souza S, Chen LC (1980) Sex differentials in mortality in rural Bangladesh. Popul Dev Rev 6(2):257–270
Defo BK (1997) Effects of infant feeding practices and birth spacing on infant and child survival: a reassessment from retrospective and prospective data. J Biosoc Sci 29(3):303–326
Green MS (1992) The male predominance in the incidence of infectious diseases in children: a postulated explanation for disparities in the literature. Int J Epidemiol 21(2):381–386
Gupta MD (1987) Selective discrimination against female children in rural Punjab, India. Popul Dev Rev 13(1):77–100
Hobcraft JN, McDonald JW, Rutstein SO (1985) Demographic determinants of infant and early child mortality: a comparative analysis. Popul Stud 39(3):363–385
Irfan M (1986) Mortality trends and patterns in Pakistan. Asian Population Studies Series No. 75, Economic and Social Commission for Asia and the Pacific Bangkok, Thailand, United Nations, New York. Available from: https://mpra.ub.uni-muenchen.de/38619/1/Mortality_Trends_and_Patterns_in_Pakistan.pdf. Retrived July 23, 2019
Khan A, Kinney MV, Hazir T, Hafeez A, Wall SN, Ali N, Lawn JE, Badar A, Khan AA, Uzma Q, Bhutta ZA (2012) Newborn survival in Pakistan: a decade of change and future implications. Health Policy Plan 27(suppl_3):iii72–iii87
Knowles JC (1982) The determinants of mortality in a low income area of Karachi. Pakistan J Appl Econ 1(1):59–91
Kramer MS (1987) Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ 65(5):663–737
Lau C, Ambalavanan N, Chakraborty H, Wingate MS, Carlo WA (2013) Extremely low birth weight and infant mortality rates in the United States. Pediatr 131(5):855–860
Lawn JE, Cousens S, Zupan J, Team LNSS (2005) 4 million neonatal deaths: when? Where? Why? Lancet 365(9462):891–900. https://doi.org/10.1016/S0140-6736(05)71048-5
Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, Cibulskis R, Li M, Mathers C (2012) Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 379(9832):2151–2161. https://doi.org/10.1016/S0140-6736(12)60560-1
Målqvist M, Nga NT, Eriksson L, Wallin L, Ewald U, Persson LAÅ (2008) Delivery care utilisation and care-seeking in the neonatal period: a population-based study in Vietnam. Ann Trop Paediatr 28(3):191–198
Midhet F, Becker S, Berendes HW (1998) Contextual determinants of maternal mortality in rural Pakistan. Soc Sci Med 46(12):1587–1598
Muhuri PK, Preston SH (1991) Effects of family composition on mortality differentials by sex among children in Matlab, Bangladesh. Popul Dev Rev 17(3):415–434
Naseem SM (1981) Underdevelopment, poverty, and inequality in Pakistan. Vanguard Publications, Lahore
Nisar YB, Dibley MJ (2014) Determinants of neonatal mortality in Pakistan: secondary analysis of Pakistan demographic and health survey 2006–07. BMC Public Health 14(1):663
Patel R (1991) Socio-economic political status and women and law in Pakistan. Faiza Publ, Karachi
Preston SH (2013) Mortality patterns in national populations: with special reference to recorded causes of death. Elsevier
Richardson DK, Phibbs CS, Gray JE, McCormick MC, Workman-Daniels K, Goldmann DA (1993) Birth weight and illness severity: independent predictors of neonatal mortality. Pediatr 91(5):969–975
Ronsmans C (1996) Birth spacing and child survival in rural Senegal. Int J Epidemiol 25(5):989–997
Sastry N (1997) What explains rural-urban differentials in child mortality in Brazil? Soc Sci Med 44(7):989–1002
Sathar ZA (1995) The relationship between poverty and infant mortality in Pakistan. Paper presented at the Annual Meeting of the Population Association of America, San Francisco, CA, pp 6–8
Sathar ZA, Mallick MD (1991) Changes in mortality in Pakistan 1960-88 [with comments]. Pak Dev Rev 30(4):669–679
Sharma V, Katz J, Mullany LC, Khatry SK, LeClerq SC, Shrestha SR, Darmstadt GL, Tielsch JM (2008) Young maternal age and the risk of neonatal mortality in rural Nepal. Arch Pediatr Adolesc Med 162(9):828–835
Sweemer CD (1984) The influence of child spacing on child survival. Popul Stud 38(1):47–72
Tariq P, Kundi Z (1999) Determinants of neonatal mortality. J Pak Med Assoc 49(3):56–59
The World Bank (2017) Estimates developed by the UN inter-agency Group for Child Mortality Estimation (UNICEF, WHO, World Bank, UN DESA Population Division). Available from: https://data.worldbank.org/indicator/SH.DTH.IMRT?end=2017&locations=PK&start=1960. Retrieved July 27, 2019
Titaley CR, Dibley MJ, Agho K, Roberts CL, Hall J (2008) Determinants of neonatal mortality in Indonesia. BMC Public Health 8(1):232
UNICEF (2018) UNICEF data: monitoring the situation of children and women. Available from: https://data.unicef.org/country/pak/#. Retrieved July 27, 2019
United Nations Development Program (1994) Human development report, New York
Vintzileos AM, Ananth CV, Smulian JC, Scorza WE, Knuppel RA (2002) The impact of prenatal care on neonatal deaths in the presence and absence of antenatal high-risk conditions. Am J Obstet Gynecol 186(5):1011–1016
World Health Organization (2014) The partnership for maternal, newborn, and child health. Avalable from: http://www.who.int/pmnch/media/press_materials/fs/fs_newborndealth_illness/en/. Retrieved June 20, 2019
World Health Organization (2017) Infant mortality: Situation and trends. Available from: https://www.who.int/gho/child_health/mortality/neonatal_infant_text/en/. Retrieved July 27, 2019
Yasmin S, Osrin D, Paul E, Costello A (2001) Neonatal mortality of low-birth-weight infants in Bangladesh. Bull World Health Organ 79:608–614
Zaidi SA (1985) The urban bias in health facilities in Pakistan. Soc Sci Med 20(5):473–482
Acknowledgments
All the authors thank all anonymous reviewers for the constructive comments for improving the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not require any ethical approval because it used the secondary data of the DHS, which is open to public.
Informed consent
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Patel, K.K., Rai, R. & Rai, A.K. Determinants of infant mortality in Pakistan: evidence from Pakistan Demographic and Health Survey 2017–18. J Public Health (Berl.) 29, 693–701 (2021). https://doi.org/10.1007/s10389-019-01175-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-019-01175-0